

A Systematic Review and Meta-Analysis of the Efficacy of Physical Activity Interventions among University Students


Abstract
:1. Introduction
2. Material and Methods
2.1. Protocol and Registration Details
2.2. Searching Strategies
2.3. Eligibility Criteria
2.4. Study Selection
2.5. Data Extraction
2.6. Quality Assessment
2.7. Statistical Analysis
3. Results
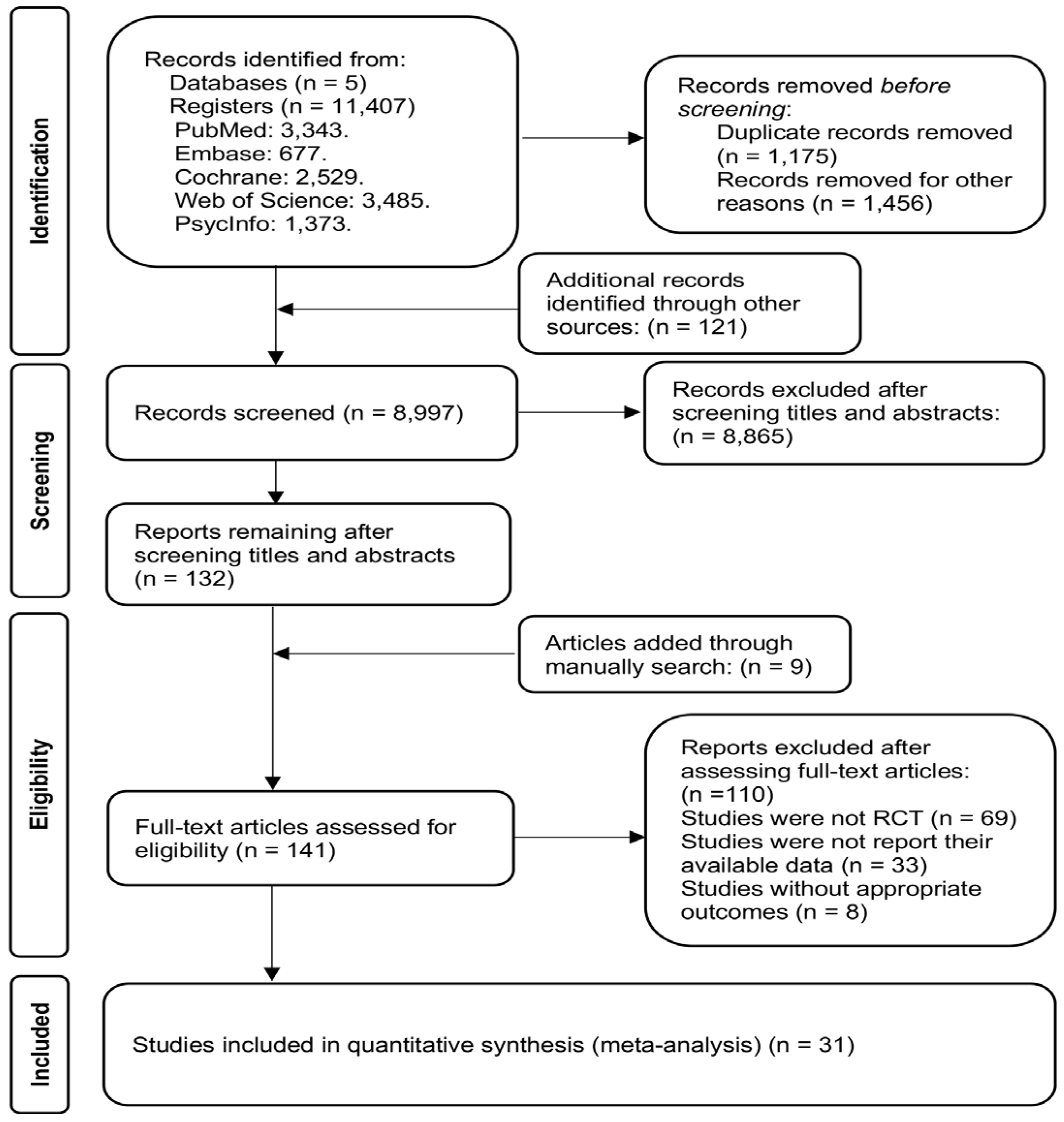
3.1. Study Selection
3.2. Studies’ Characteristics
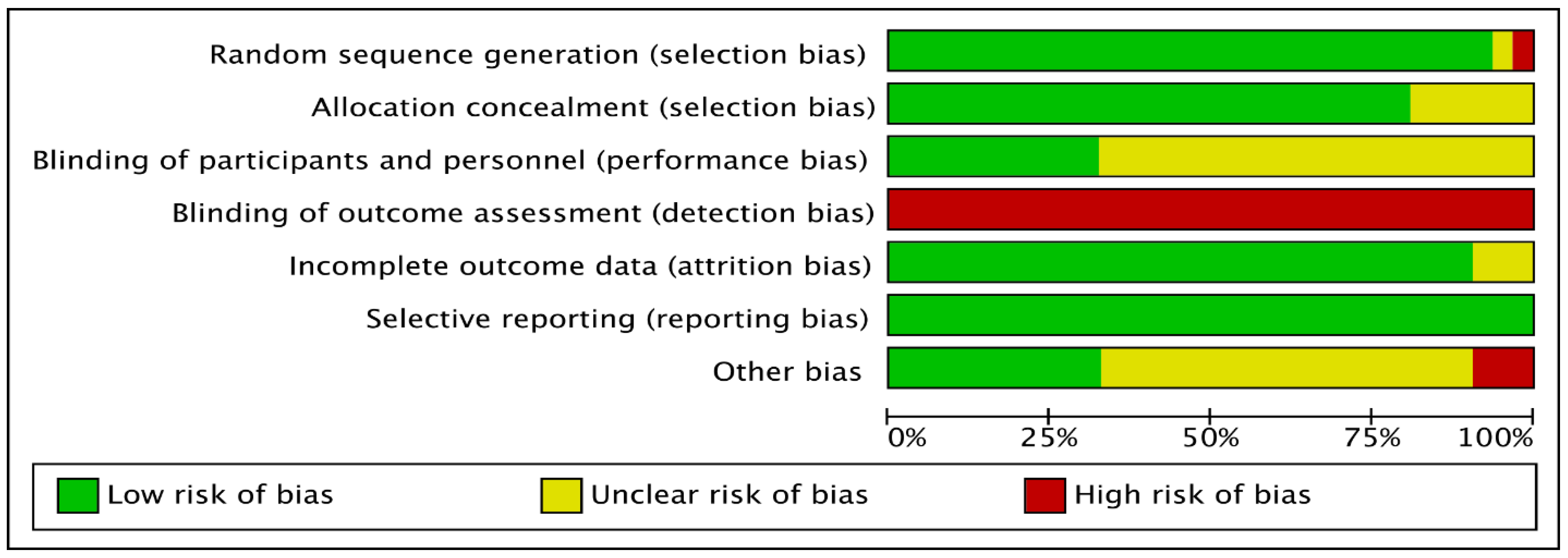
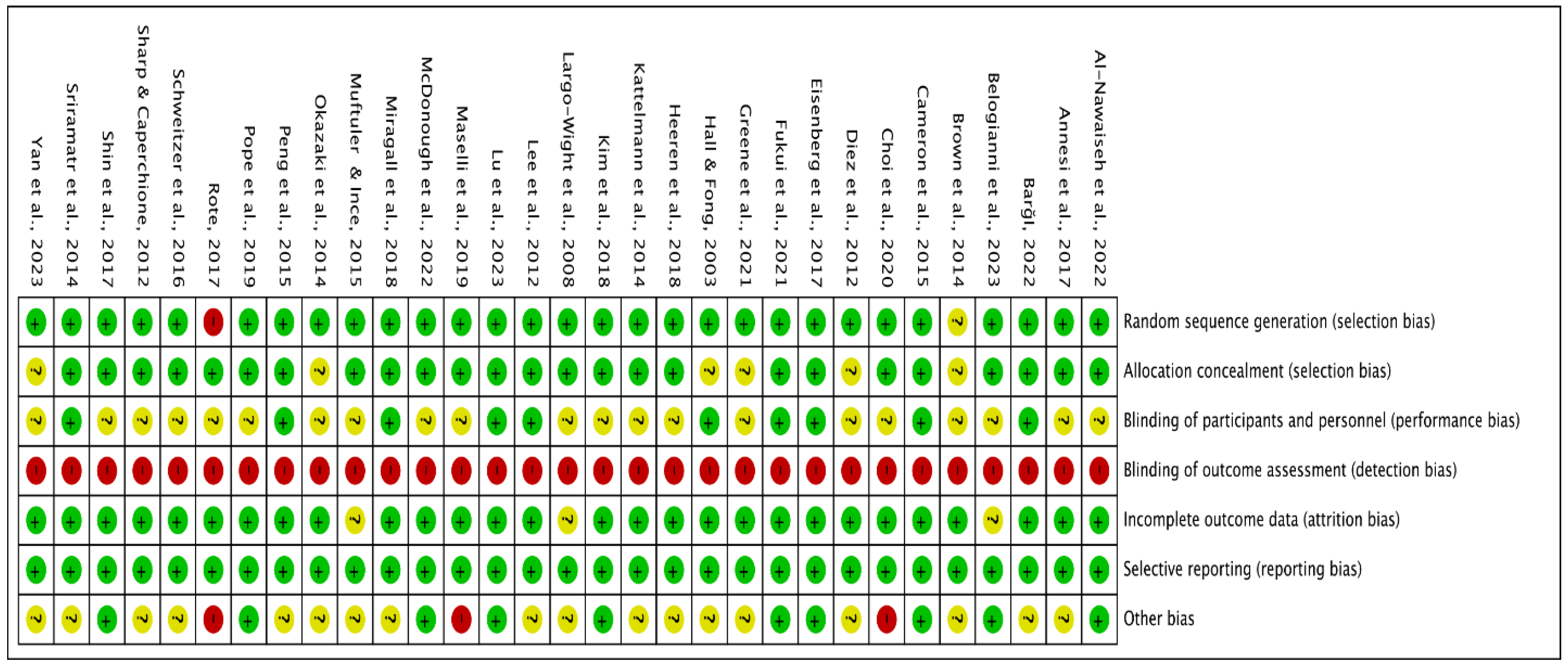
3.3. Quality of Included Studies
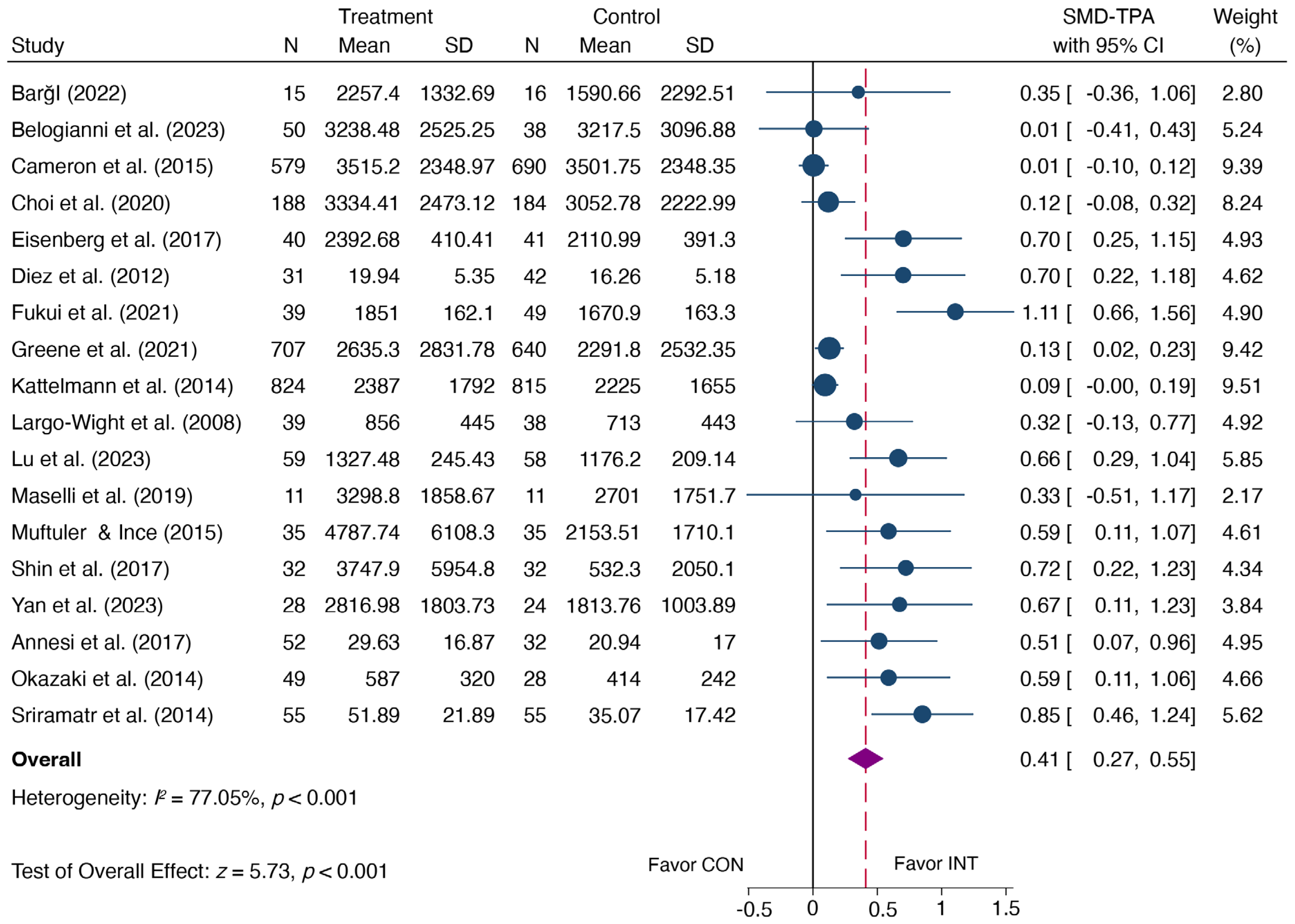
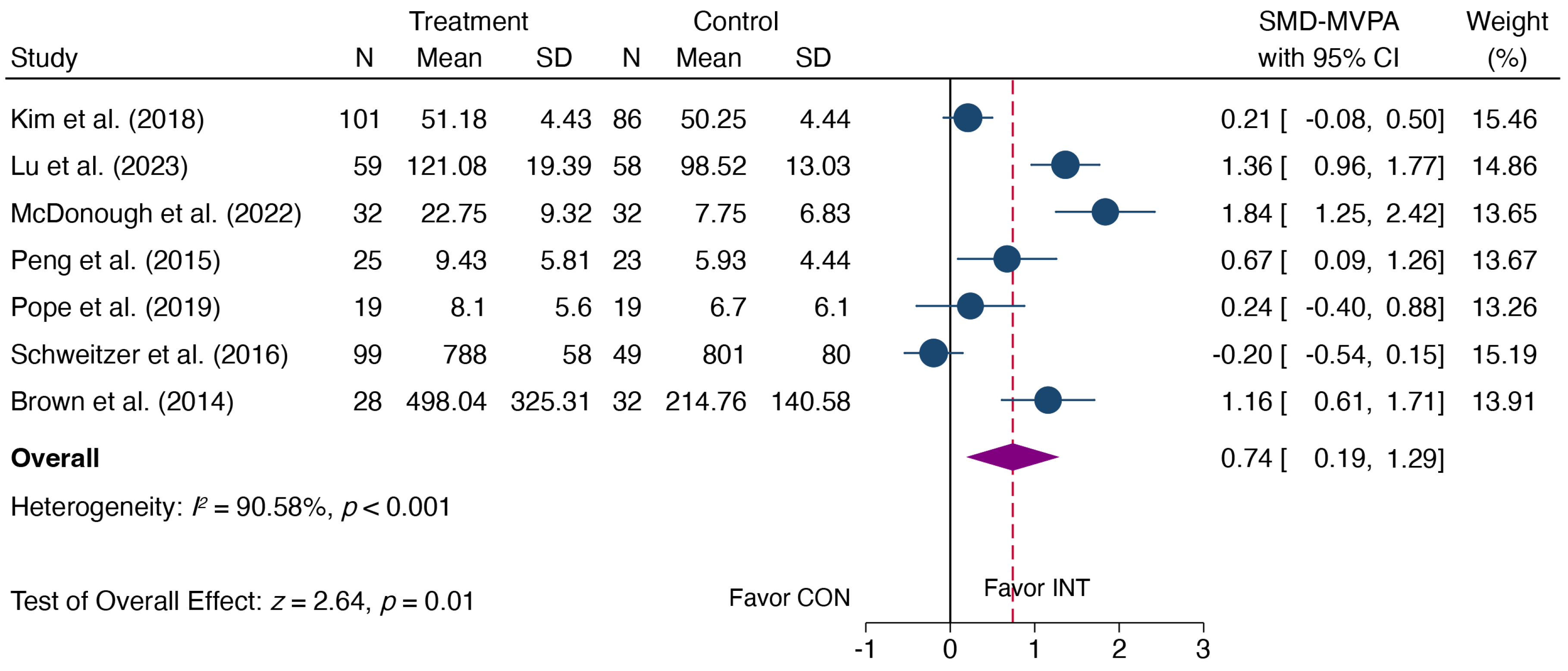
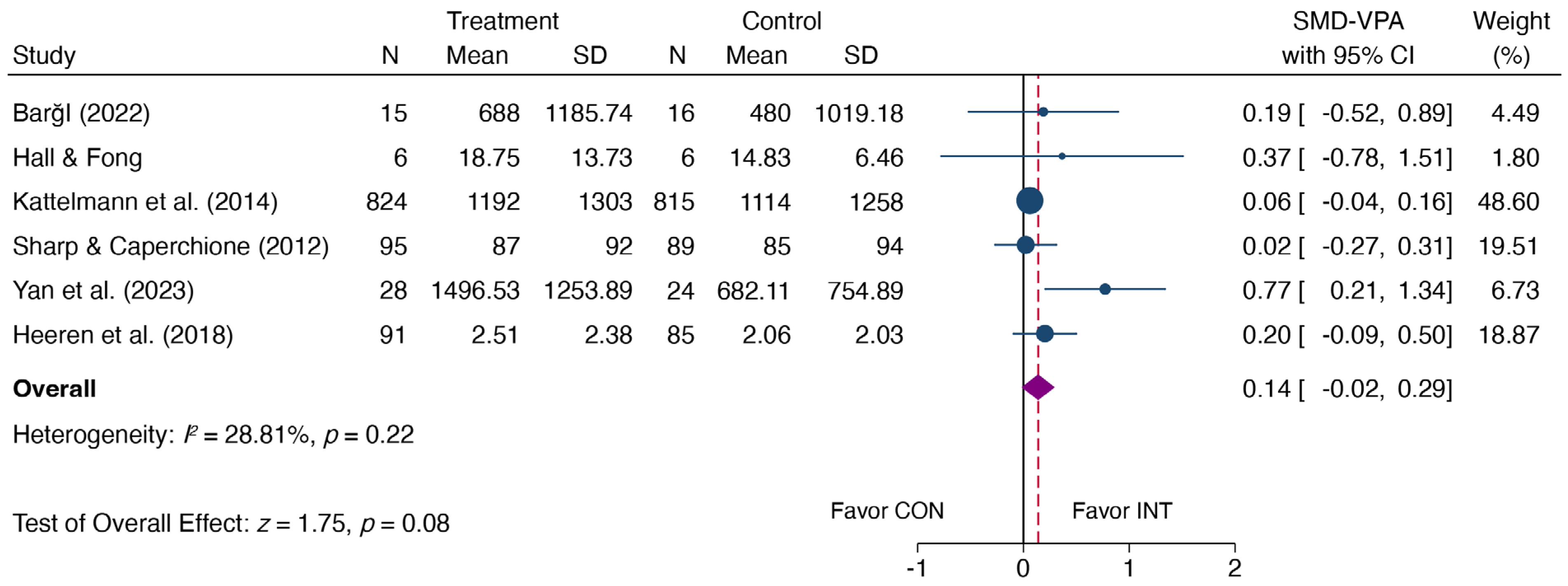
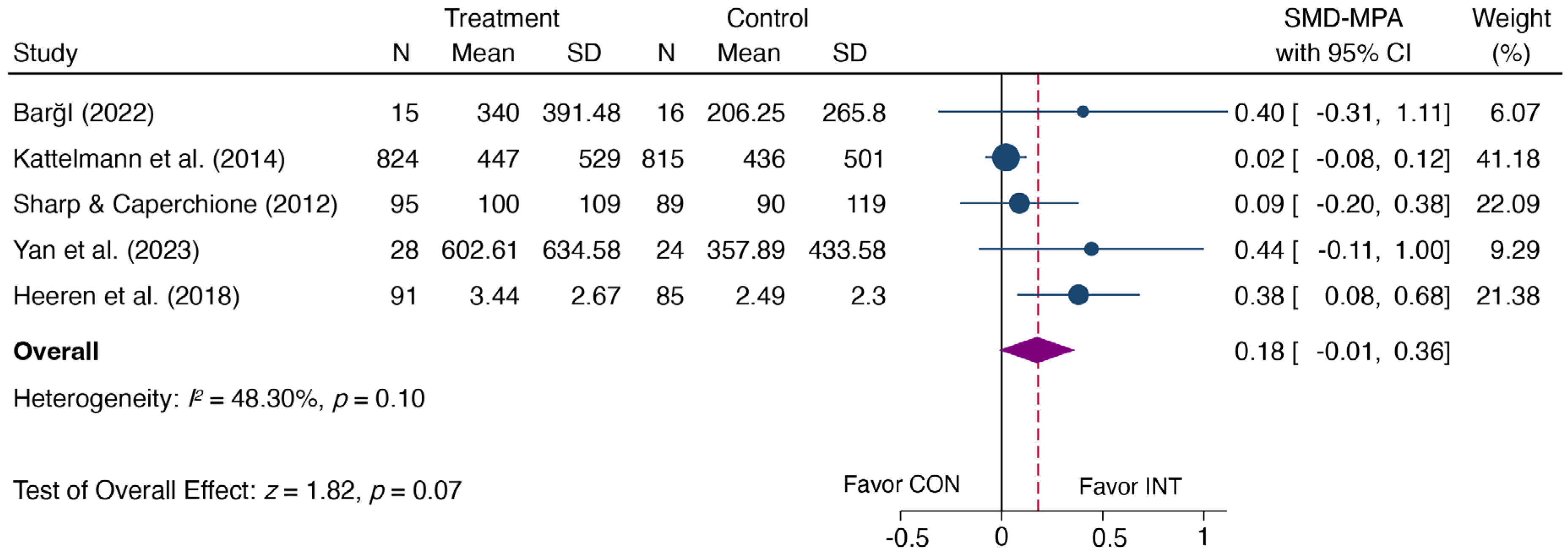
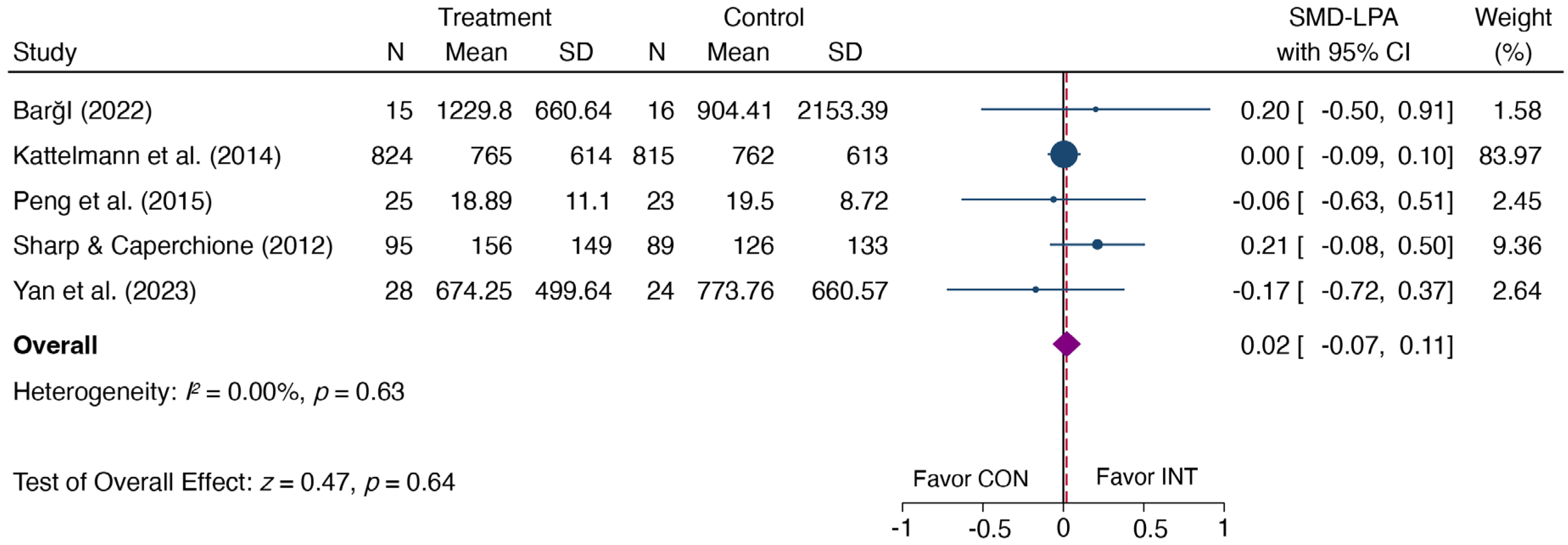
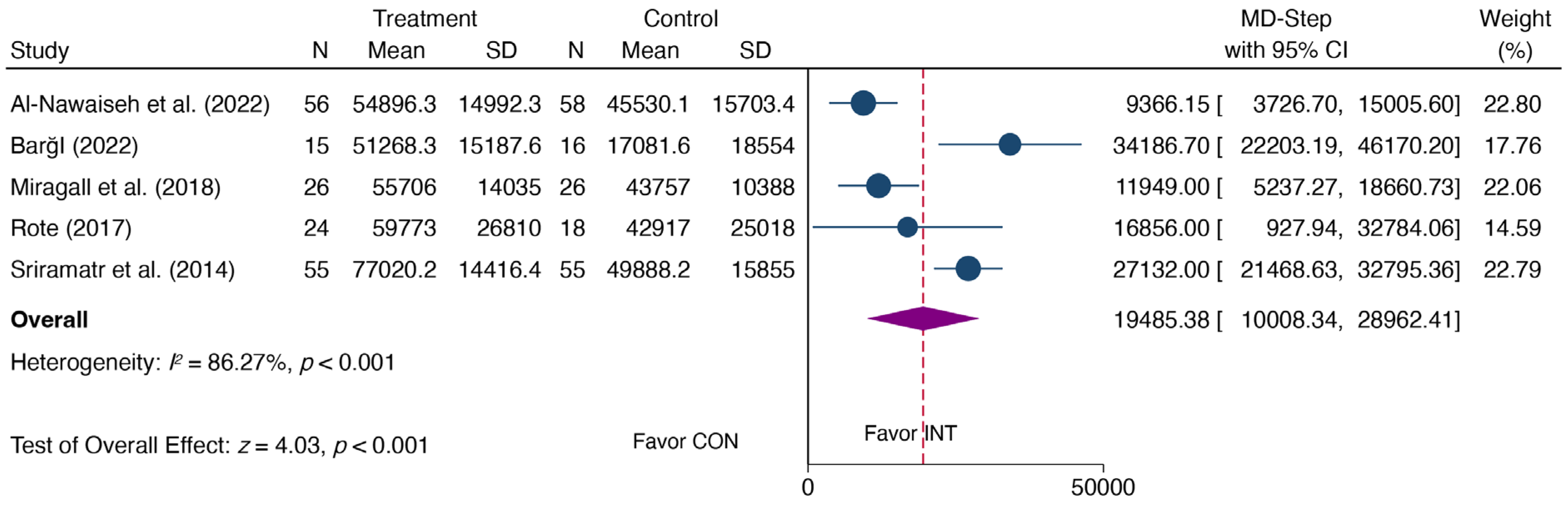
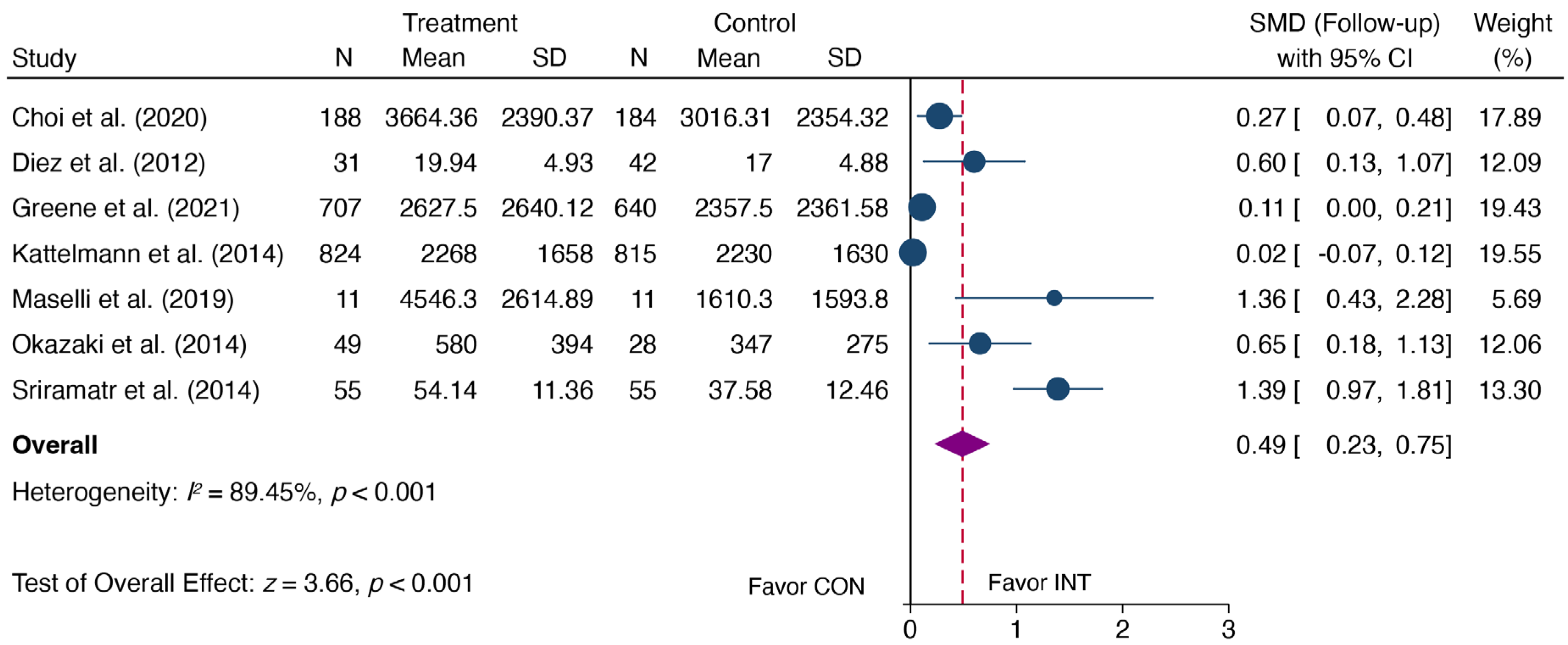
3.4. Meta-Analysis
3.5. Subgroups Analyses
3.6. Publication Bias and Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour, 2020; World Health Organization: Geneva, Switzerland, 2020; p. 3. [Google Scholar]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [PubMed]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U.; Lancet Physical Activity Series Working, G. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef] [PubMed]
- American College Health Association. National College Health Assessment II: Undergraduate Student Executive Summary; American College Health Association: Silver Spring, MD, USA, 2018. [Google Scholar]
- Pengpid, S.; Peltzer, K.; Kassean, H.K.; Tsala Tsala, J.P.; Sychareun, V.; Muller-Riemenschneider, F. Physical inactivity and associated factors among university students in 23 low-, middle- and high-income countries. Int. J. Public Health 2015, 60, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Telleria-Aramburu, N.; Arroyo-Izaga, M. Risk factors of overweight/obesity-related lifestyles in university students: Results from the EHU12/24 study. Br. J. Nutr. 2022, 127, 914–926. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Hwang, Y.; Campbell, S.; McCullick, B.A.; Yli-Piipari, S. Institutional factors associated with college students’ healthy physical activity and body composition: A first semester follow-up. J. Am. Coll. Health 2023, 71, 1134–1142. [Google Scholar] [CrossRef] [PubMed]
- Wang, J. The association between physical fitness and physical activity among Chinese college students. J. Am. Coll. Health 2019, 67, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Lederer, A.M.; Oswalt, S.B. The value of college health promotion: A critical population and setting for improving the public’s health. Am. J. Health Educ. 2017, 48, 215–218. [Google Scholar] [CrossRef]
- Whatnall, M.C.; Sharkey, T.; Hutchesson, M.J.; Haslam, R.L.; Bezzina, A.; Collins, C.E.; Ashton, L.M. Effectiveness of interventions and behaviour change techniques for improving physical activity in young adults: A systematic review and meta-analysis. J. Sports Sci. 2021, 39, 1754–1771. [Google Scholar] [CrossRef]
- Maselli, M.; Ward, P.B.; Gobbi, E.; Carraro, A. Promoting Physical Activity Among University Students: A Systematic Review of Controlled Trials. Am. J. Health Promot. 2018, 32, 1602–1612. [Google Scholar] [CrossRef]
- Peng, S.; Yuan, F.; Othman, A.T.; Zhou, X.; Shen, G.; Liang, J. The Effectiveness of E-Health Interventions Promoting Physical Activity and Reducing Sedentary Behavior in College Students: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 20, 318. [Google Scholar] [CrossRef]
- Goncalves, A.; Deshayes, M.; Gisclard, B.; Philippe, A.G.; Bernal, C.; Krawczyk, S.; Korchi, K.; Nogrette, M.; Charbonnier, E. Exploring the Health Effectiveness of a Physical Activity Program Co-Constructed with Students after the COVID-19 Pandemic. Nutrients 2023, 15, 2913. [Google Scholar] [CrossRef]
- Yan, Z.; Peacock, J.; Cohen, J.F.W.; Kurdziel, L.; Benes, S.; Oh, S.; Bowling, A. An 8-Week Peer Health Coaching Intervention among College Students: A Pilot Randomized Study. Nutrients 2023, 15, 1284. [Google Scholar] [CrossRef]
- Abu-Moghli, F.A.; Khalaf, I.A.; Barghoti, F.F. The influence of a health education programme on healthy lifestyles and practices among university students. Int. J. Nurs. Pract. 2010, 16, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Claxton, D.; Wells, G.M. The effect of physical activity homework on physical activity among college students. J. Phys. Act. Health 2009, 6, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Ulla Diez, S.M.; Fortis, A.P.; Franco, S.F. Efficacy of a health-promotion intervention for college students: A randomized controlled trial. Nurs. Res. 2012, 61, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Pope, Z.C.; Gao, Z. Feasibility of smartphone application- and social media-based intervention on college students’ health outcomes: A pilot randomized trial. J. Am. Coll. Health 2022, 70, 89–98. [Google Scholar] [CrossRef] [PubMed]
- McDonough, D.J.; Helgeson, M.A.; Liu, W.; Gao, Z. Effects of a remote, YouTube-delivered exercise intervention on young adults’ physical activity, sedentary behavior, and sleep during the COVID-19 pandemic: Randomized controlled trial. J. Sport Health Sci. 2022, 11, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Miragall, M.; Dominguez-Rodriguez, A.; Navarro, J.; Cebolla, A.; Banos, R.M. Increasing physical activity through an Internet-based motivational intervention supported by pedometers in a sample of sedentary students: A randomised controlled trial. Psychol. Health 2018, 33, 465–482. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, K.; Okano, S.; Haga, S.; Seki, A.; Suzuki, H.; Takahashi, K. One-year outcome of an interactive internet-based physical activity intervention among university students. Int. J. Med. Inform. 2014, 83, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Lumpkin, A.; Lochbaum, M.; Stegemeier, S.; Kitten, K. Promoting physical activity using a wearable activity tracker in college students: A cluster randomized controlled trial. J. Sports Sci. 2018, 36, 1889–1896. [Google Scholar] [CrossRef]
- Pope, Z.C.; Barr-Anderson, D.J.; Lewis, B.A.; Pereira, M.A.; Gao, Z. Use of Wearable Technology and Social Media to Improve Physical Activity and Dietary Behaviors among College Students: A 12-Week Randomized Pilot Study. Int. J. Environ. Res. Public Health 2019, 16, 3579. [Google Scholar] [CrossRef]
- Schweitzer, A.L.; Ross, J.T.; Klein, C.J.; Lei, K.Y.; Mackey, E.R. An Electronic Wellness Program to Improve Diet and Exercise in College Students: A Pilot Study. JMIR Res. Protoc. 2016, 5, e29. [Google Scholar] [CrossRef] [PubMed]
- Plotnikoff, R.C.; Costigan, S.A.; Williams, R.L.; Hutchesson, M.J.; Kennedy, S.G.; Robards, S.L.; Allen, J.; Collins, C.E.; Callister, R.; Germov, J. Effectiveness of interventions targeting physical activity, nutrition and healthy weight for university and college students: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 45. [Google Scholar] [CrossRef] [PubMed]
- Favieri, F.; French, M.N.; Casagrande, M.; Chen, E.Y. Physical activity interventions have a moderate effect in increasing physical activity in university students-a meta-analysis. J. Am. Coll. Health 2023, 71, 2823–2834. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. In Methodological Issues and Strategies in Clinical Research; American Psychological Association: Washington, DC, USA, 2016. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Al-Nawaiseh, H.K.; McIntosh, W.A.; McKyer, L.J. An-m-Health Intervention Using Smartphone App to Improve Physical Activity in College Students: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 7228. [Google Scholar] [CrossRef]
- Annesi, J.J.; Porter, K.J.; Hill, G.M.; Goldfine, B.D. Effects of Instructional Physical Activity Courses on Overall Physical Activity and Mood in University Students. Res. Q. Exerc. Sport. 2017, 88, 358–364. [Google Scholar] [CrossRef]
- Barği, G. Effectiveness of Physical Activity Counseling in University Students Educated by Distance Learning During COVID-19 Pandemic: A Randomized-Controlled Trial. J. Basic. Clin. Health 2022, 6, 374–384. [Google Scholar] [CrossRef]
- Belogianni, K.; Ooms, A.; Lykou, A.; Nikoletou, D.; Jayne Moir, H. An online game-based intervention using quizzes to improve nutrition and physical activity outcomes among university students. Health Educ. J. 2023, 82, 636–650. [Google Scholar] [CrossRef]
- Cameron, D.; Epton, T.; Norman, P.; Sheeran, P.; Harris, P.R.; Webb, T.L.; Julious, S.A.; Brennan, A.; Thomas, C.; Petroczi, A.; et al. A theory-based online health behaviour intervention for new university students (U@Uni:LifeGuide): Results from a repeat randomized controlled trial. Trials 2015, 16, 555. [Google Scholar] [CrossRef]
- Choi, S.M.; Sum, K.W.R.; Leung, F.L.E.; Wallhead, T.; Morgan, K.; Milton, D.; Ha, S.C.A.; Sit, H.P.C. Effect of sport education on students’ perceived physical literacy, motivation, and physical activity levels in university required physical education: A cluster-randomized trial. High. Educ. 2020, 81, 1137–1155. [Google Scholar] [CrossRef]
- Eisenberg, M.H.; Phillips, L.A.; Fowler, L.; Moore, P.J. The Impact of E-diaries and Accelerometers on Young Adults’ Perceived and Objectively Assessed Physical Activity. Psychol. Sport Exerc. 2017, 30, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Fukui, K.; Suzuki, Y.; Kaneda, K.; Kuroda, S.; Komiya, M.; Maeda, N.; Urabe, Y. Do “Stay-at-Home Exercise” Videos Induce Behavioral Changes in College Students? A Randomized Controlled Trial. Sustainability 2021, 13, 11600. [Google Scholar] [CrossRef]
- Greene, G.W.; White, A.A.; Hoerr, S.L.; Lohse, B.; Schembre, S.M.; Riebe, D.; Patterson, J.; Kattelmann, K.K.; Shoff, S.; Horacek, T.; et al. Impact of an online healthful eating and physical activity program for college students. Am. J. Health Promot. 2012, 27, e47–e58. [Google Scholar] [CrossRef]
- Hall, P.A.; Fong, G.T. The effects of a brief time perspective intervention for increasing physical activity among young adults. Psychol. Health 2003, 18, 685–706. [Google Scholar] [CrossRef]
- Heeren, G.A.; Jemmott, J.B., 3rd; Marange, C.S.; Rumosa Gwaze, A.; Batidzirai, J.M.; Ngwane, Z.; Mandeya, A.; Tyler, J.C. Health-Promotion Intervention Increases Self-Reported Physical Activity in Sub-Saharan African University Students: A Randomized Controlled Pilot Study. Behav. Med. 2018, 44, 297–305. [Google Scholar] [CrossRef]
- Kattelmann, K.K.; Bredbenner, C.B.; White, A.A.; Greene, G.W.; Hoerr, S.L.; Kidd, T.; Colby, S.; Horacek, T.M.; Phillips, B.W.; Koenings, M.M.; et al. The effects of Young Adults Eating and Active for Health (YEAH): A theory-based Web-delivered intervention. J. Nutr. Educ. Behav. 2014, 46, S27–S41. [Google Scholar] [CrossRef]
- Largo-Wight, E.; Todorovich, J.R.; O’Hara, B.K. Effectiveness of Point-Based Physical Activity Intervention. Phys. Educ. 2008, 65, 30–45. [Google Scholar]
- Lee, L.L.; Kuo, Y.C.; Fanaw, D.; Perng, S.J.; Juang, I.F. The effect of an intervention combining self-efficacy theory and pedometers on promoting physical activity among adolescents. J. Clin. Nurs. 2012, 21, 914–922. [Google Scholar] [CrossRef]
- Lu, Y.; Wiltshire, H.D.; Baker, J.S.; Wang, Q.; Ying, S. The effect of Tabata-style functional high-intensity interval training on cardiometabolic health and physical activity in female university students. Front. Physiol. 2023, 14, 1095315. [Google Scholar] [CrossRef]
- Maselli, M.; Gobbi, E.; Carraro, A. Effectiveness of individual counseling and activity monitors to promote physical activity among university students. J. Sports Med. Phys. Fit. 2019, 59, 132–140. [Google Scholar] [CrossRef]
- Muftuler, M.; Ince, M.L. Use of Trans-Contextual Model-Based Physical Activity Course in Developing Leisure-Time Physical Activity Behavior of University Students. Percept. Mot. Skills 2015, 121, 31–55. [Google Scholar] [CrossRef]
- Peng, W.; Pfeiffer, K.A.; Winn, B.; Lin, J.H.; Suton, D. A pilot randomized, controlled trial of an active video game physical activity intervention. Health Psychol. 2015, 34S, 1229–1239. [Google Scholar] [CrossRef]
- Rote, A.E. Physical activity intervention using Fitbits in an introductory college health course. Health Educ. J. 2016, 76, 337–348. [Google Scholar] [CrossRef]
- Sharp, P.; Caperchione, C. The effects of a pedometer-based intervention on first-year university students: A randomized control trial. J. Am. Coll. Health 2016, 64, 630–638. [Google Scholar] [CrossRef]
- Shin, D.W.; Yun, J.M.; Shin, J.H.; Kwon, H.; Min, H.Y.; Joh, H.K.; Chung, W.J.; Park, J.H.; Jung, K.T.; Cho, B. Enhancing physical activity and reducing obesity through smartcare and financial incentives: A pilot randomized trial. Obesity 2017, 25, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.M.; Bray, S.R.; Beatty, K.R.; Kwan, M.Y. Healthy active living: A residence community–based intervention to increase physical activity and healthy eating during the transition to first-year university. J. Am. Coll. Health 2014, 62, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Sriramatr, S.; Berry, T.R.; Spence, J.C. An Internet-based intervention for promoting and maintaining physical activity: A randomized controlled trial. Am. J. Health Behav. 2014, 38, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Duan, Y.; Liang, W.; Peiris, D.L.I.H.K.; Baker, J.S. Effects of Face-to-Face and eHealth Blended Interventions on Physical Activity, Diet, and Weight-Related Outcomes among Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 1560. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-N.; Seo, K. Smartphone-Based Health Program for Improving Physical Activity and Tackling Obesity for Young Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 15. [Google Scholar] [CrossRef] [PubMed]
- Lonsdale, C.; Rosenkranz, R.R.; Peralta, L.R.; Bennie, A.; Fahey, P.; Lubans, D.R. A systematic review and meta-analysis of interventions designed to increase moderate-to-vigorous physical activity in school physical education lessons. Prev. Med. 2013, 56, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Biddle, S.J.H.; Braithwaite, R.; Pearson, N. The effectiveness of interventions to increase physical activity among young girls: A meta-analysis. Prev. Med. 2014, 62, 119–131. [Google Scholar] [CrossRef]
- Cotie, L.; Prince, S.; Elliott, C.; Ziss, M.; McDonnell, L.; Mullen, K.; Hiremath, S.; Pipe, A.; Reid, R.; Reed, J. The effectiveness of eHealth interventions on physical activity and measures of obesity among working-age women: A systematic review and meta-analysis. Obes. Rev. 2018, 19, 1340–1358. [Google Scholar] [CrossRef] [PubMed]
- Grande, G.D.; Oliveira, C.B.; Morelhão, P.K.; Sherrington, C.; Tiedemann, A.; Pinto, R.Z.; Franco, M.R. Interventions promoting physical activity among older adults: A systematic review and meta-analysis. Gerontologist 2020, 60, e583–e599. [Google Scholar] [CrossRef] [PubMed]
- Kettle, V.E.; Madigan, C.D.; Coombe, A.; Graham, H.; Thomas, J.J.C.; Chalkley, A.E.; Daley, A.J. Effectiveness of physical activity interventions delivered or prompted by health professionals in primary care settings: Systematic review and meta-analysis of randomised controlled trials. BMJ 2022, 376, e068465. [Google Scholar] [CrossRef]
- Chaudhry, U.A.R.; Wahlich, C.; Fortescue, R.; Cook, D.G.; Knightly, R.; Harris, T. The effects of step-count monitoring interventions on physical activity: Systematic review and meta-analysis of community-based randomised controlled trials in adults. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 129. [Google Scholar] [CrossRef]
- Conn, V.S.; Hafdahl, A.R.; Mehr, D.R. Interventions to Increase Physical Activity Among Healthy Adults: Meta-Analysis of Outcomes. Am. J. Public Health 2011, 101, 751–758. [Google Scholar] [CrossRef]
- Kang, M.; Marshall, S.J.; Barreira, T.V.; Lee, J.-O. Effect of pedometer-based physical activity interventions: A meta-analysis. In Database of Abstracts of Reviews of Effects (DARE): Quality-Assessed Reviews [Internet]; Centre for Reviews and Dissemination (UK): York, UK, 2009. [Google Scholar]
- Hall, K.S.; Hyde, E.T.; Bassett, D.R.; Carlson, S.A.; Carnethon, M.R.; Ekelund, U.; Evenson, K.R.; Galuska, D.A.; Kraus, W.E.; Lee, I.M.; et al. Systematic review of the prospective association of daily step counts with risk of mortality, cardiovascular disease, and dysglycemia. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 78. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishnan, R.; He, J.-R.; Ponsonby, A.-L.; Woodward, M.; Rahimi, K.; Blair, S.N.; Dwyer, T. Objectively measured physical activity and all cause mortality: A systematic review and meta-analysis. Prev. Med. 2021, 143, 106356. [Google Scholar] [CrossRef] [PubMed]
- Gasana, J.; O’Keeffe, T.; Withers, T.M.; Greaves, C.J. A systematic review and meta-analysis of the long-term effects of physical activity interventions on objectively measured outcomes. BMC Public Health 2023, 23, 1697. [Google Scholar] [CrossRef] [PubMed]
- Madigan, C.D.; Fong, M.; Howick, J.; Kettle, V.; Rouse, P.; Hamilton, L.; Roberts, N.; Gomersall, S.R.; Daley, A.J. Effectiveness of interventions to maintain physical activity behavior (device-measured): Systematic review and meta-analysis of randomized controlled trials. Obes. Rev. 2021, 22, e13304. [Google Scholar] [CrossRef] [PubMed]
- Moenninghoff, A.; Kramer, J.N.; Hess, A.J.; Ismailova, K.; Teepe, G.W.; Car, L.T.; Mueller-Riemenschneider, F.; Kowatsch, T. Long-term Effectiveness of mHealth Physical Activity Interventions: Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Med. Internet Res. 2021, 23, e26699. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.M.; Brennan, S.F.; French, D.P.; Patterson, C.C.; Kee, F.; Hunter, R.F. Effectiveness of physical activity interventions in achieving behaviour change maintenance in young and middle aged adults: A systematic review and meta-analysis. Soc. Sci. Med. 2017, 192, 125–133. [Google Scholar] [CrossRef]
- Robertson, M.C.; Lee, C.Y.; Wu, I.H.; Liao, Y.; Raber, M.; Parker, N.; Le, T.; Gatus, L.; Basen-Engquist, K.M. Changes in physical activity associated with the COVID-19 pandemic in individuals with overweight and obesity: An interrupted time series analysis with historical controls. J. Behav. Med. 2022, 45, 186–196. [Google Scholar] [CrossRef]
- Olfert, M.D.; Wattick, R.A.; Saurborn, E.G.; Hagedorn, R.L. Impact of COVID-19 on college student diet quality and physical activity. Nutr. Health 2022, 28, 721–731. [Google Scholar] [CrossRef]
- Santos, A.C.; Willumsen, J.; Meheus, F.; Ilbawi, A.; Bull, F.C. The cost of inaction on physical inactivity to public health-care systems: A population-attributable fraction analysis. Lancet Glob. Health 2023, 11, e32–e39. [Google Scholar] [CrossRef]
- Baumann, H.; Fiedler, J.; Wunsch, K.; Woll, A.; Wollesen, B. mHealth Interventions to Reduce Physical Inactivity and Sedentary Behavior in Children and Adolescents: Systematic Review and Meta-analysis of Randomized Controlled Trials. JMIR mHealth uHealth 2022, 10, e35920. [Google Scholar] [CrossRef]
- Gourlan, M.; Bernard, P.; Bortolon, C.; Romain, A.J.; Lareyre, O.; Carayol, M.; Ninot, G.; Boiche, J. Efficacy of theory-based interventions to promote physical activity. A meta-analysis of randomised controlled trials. Health Psychol. Rev. 2016, 10, 50–66. [Google Scholar] [CrossRef]
- Belanger-Gravel, A.; Godin, G.; Amireault, S. A meta-analytic review of the effect of implementation intentions on physical activity. Health Psychol. Rev. 2013, 7, 23–54. [Google Scholar] [CrossRef]
- Peng, S.; Othman, A.T.; Yuan, F.; Liang, J. The Effectiveness of Planning Interventions for Improving Physical Activity in the General Population: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 7337. [Google Scholar] [CrossRef]
- Casado-Robles, C.; Viciana, J.; Guijarro-Romero, S.; Mayorga-Vega, D. Effects of Consumer-Wearable Activity Tracker-Based Programs on Objectively Measured Daily Physical Activity and Sedentary Behavior Among School-Aged Children: A Systematic Review and Meta-analysis. Sports Med. Open 2022, 8, 18. [Google Scholar] [CrossRef]
- Peyer, K.L.; Hathaway, E.D.; Doyle, K. Gender differences in stress, resilience, and physical activity during the COVID-19 pandemic. J. Am. Coll. Health, 2022; online ahead of print. [Google Scholar] [CrossRef]
- Tafireyi, C.G.S.; Grace, J.M. The physical activity and health promotion activities of global university students: A review of reviews. Glob. Health Promot. 2022, 29, 17579759221099308. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.M.; Wang, X.Z.; Koh, K.T. Association between physical activity, sedentary time, and physical fitness of female college students in China. BMC Women’s Health 2022, 22, 502. [Google Scholar] [CrossRef] [PubMed]
- Ferreira Silva, R.M.; Mendonca, C.R.; Azevedo, V.D.; Raoof Memon, A.; Noll, P.; Noll, M. Barriers to high school and university students’ physical activity: A systematic review. PLoS ONE 2022, 17, e0265913. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Sample Size | Country | Female (%) | Intervention Characteristics | Outcomes | ||||
|---|---|---|---|---|---|---|---|---|---|
| IG | CG | Intervention Content | Theory | Duration/ Follow-Up | Instruments | Indicators | |||
| Al-Nawaiseh et al., 2022 [31] | 56 | 58 | USA | 80.70% | Theory-based smartphone app | Goal Setting | 12 W | Pedometer | Steps |
| Annesi et al., 2017 [32] | 52 | 32 | USA | 69.00% | IPACs | No | 5 W | GLTEQ | TPA |
| Barği, 2022 [33] | 15 | 16 | Turkey | 61.29% | PA counselling through distance learning | No | 4 W | Pedometer; IPAQ | Steps; TPA; VPA; MPA; LPA |
| Belogianni et al., 2023 [34] | 50 | 38 | UK | 67.05% | Online digital interventions using game elements | Gamification theory | 10 W | IPAQ | TPA |
| Brown et al., 2014 [52] | 28 | 32 | Canada | 68.33% | A residence community–based intervention | No | 20 W | GPAQ | MVPA |
| Cameron et al., 2015 [35] | 579 | 690 | UK | 55.36% | Online theory-based intervention | TPB; II | 1 M | IPAQ-SV | TPA |
| Choi et al., 2020 [36] | 188 | 184 | Hong Kong | 70.16% | Sport education within a compulsory physical education program | No | 10 W/15 W | IPAQ-SV | TPA |
| Diez et al., 2012 [17] | 31 | 42 | Mexico | 73.97% | Health-promoting intervention using cognitive-behavioral techniques | Health Promotion Model | 1 W/3 M | HPLP-II | TPA |
| Eisenberg et al., 2017 [37] | 40 | 41 | USA | 75.00% | Electronic behavioral monitoring (E-diaries and accelerometers) | No | 1 W | IPAQ-SV | TPA |
| Fukui et al., 2021 [38] | 39 | 49 | Japan | 54.40% | “Stay-at-Home Exercise” videos | No | 8 W | IPAQ-LV | TEE |
| Greene et al., 2012 [39] | 707 | 640 | USA | 35.00% | Online healthy eating and PA Program | No | 10 W/15 M | IPAQ-SV | TPA |
| Hall & Fong, 2003 [40] | 6 | 6 | Canada | 94.40% | A brief time perspective intervention | No | 3 W | A 30-day recall measure derived from the Stanford seven-day recall | VPA |
| Heeren et al., 2018 [41] | 91 | 85 | USA | 53.40% | Health-promotion intervention | No | 6 M | Three open-ended items | VPA |
| Kattelmann et al., 2014 [42] | 824 | 815 | USA | 67.20% | Twenty-one mini-educational lessons and e-mail messages (called nudges) | Yes/NR | 3 M/15 M | IPAQ-SV | TPA; VPA; MPA; LPA |
| Kim et al., 2018 [22] | 101 | 86 | USA | 62.03% | Wearable activity tracker in a credit-based PA instructional program | No | 15 W | ActiGraph Actitrainer | MVPA |
| Largo-Wight et al., 2008 [43] | 39 | 38 | USA | 62.00% | PA logs | No | 10 W | Health Canada and national quality institute questions | TPA |
| Lee et al., 2012 [44] | 46 | 48 | Taiwan | 100% | An intervention combining self-efficacy theory and pedometers | SET | 12 W | Pedometer | Steps |
| Lu et al., 2023 [45] | 59 | 58 | China | 100% | Tabata-style functional high-intensity interval training | No | 12 W | Accelerometer | TPA; MVPA |
| Maselli et al., 2019 [46] | 11 | 11 | Italy | 60.61% | Individual counselling and activity monitors | SCT + TTM | 12 W/3 M | IPAQ | TPA |
| McDonough et al., 2022 [19] | 32 | 32 | USA | 75% | A home-based, YouTube-delivered PA intervention grounded in self-determination theory | SDT | 12 W | Accelerometer | MVPA |
| Miragall et al., 2018 [20] | 26 | 26 | Spain | 85.50% | An internet-based motivational intervention | TTM | 3 W/3 M | Pedometer | Steps |
| Muftuler & Ince, 2015 [47] | 35 | 35 | Turkey | 42.86% | A PA course based on the trans-contextual Model | TCM | 12 W | IPAQ | TPA |
| Okazaki et al., 2014 [21] | 49 | 28 | Japan | 35.06% | An interactive internet-based PA intervention | No | 4 M | IPAQ | TPA |
| Peng et al., 2015 [48] | 25 | 23 | USA | 39.20% | An active video game | SDT | 4 W | Accelerometer | MVPA; LPA |
| Pope et al., 2019 [23] | 19 | 19 | USA | 73.68% | Wearable technology and social media | SCT + SDT | 12 W | Accelerometer | MVPA |
| Rote, 2017 [49] | 24 | 18 | USA | 47.62% | A Fitbit activity monitor | No | One semester | Pedometer | Steps |
| Schweitzer et al., 2016 [24] | 99 | 49 | USA | 68.24% | An electronic wellness program via email | No | 24 W | CCAPQ | MVPA |
| Sharp & Caperchione, 2016 [50] | 95 | 89 | Canada | 53.26% | A pedometer-based intervention | SCT | 12 W | The modified GLTEQ | VPA; VPA; LPA |
| Shin et al., 2017 [51] | 32 | 32 | Korea | 0 | SmartCare and financial incentives | No | 12 W | IPAQ, validated in Korean; | TPA |
| Sriramatr et al., 2014 [53] | 55 | 55 | Canada | 100% | A social cognitive theory-based internet intervention | SCT | 12 W/3 M | The Thai version of GLTEQ; Pedometer | Steps; TPA |
| Yan et al., 2023 [54] | 28 | 24 | USA | 80.77% | An eight-week peer health coaching intervention | No | 8 W | IPAQ | TPA; VPA; MPA; LPA |
| Categories | Category | Studies | Heterogeneity Test | SMD and 95% CI | p | |
|---|---|---|---|---|---|---|
| p | I2 (%) | |||||
| Trial Period | Post-COVID-19 | 14 | <0.001 | 72.00% | 0.31 (0.18, 0.45) | <0.001 |
| After-COVID-19 | 4 | 0.276 | 22.50% | 0.75 (0.47, 1.03) | <0.001 | |
| Overall | 18 | <0.001 | 77.00% | 0.41 (0.27, 0.55) | <0.001 | |
| Between | 0.006 | |||||
| Region | Developed | 14 | <0.001 | 77.90% | 0.36 (0.21, 0.51) | <0.001 |
| Developing | 4 | 0.868 | 0.00% | 0.61 (0.38, 0.86) | <0.001 | |
| Overall | 18 | <0.001 | 77.00% | 0.41 (0.27, 0.55) | <0.001 | |
| Between | 0.066 | |||||
| Intervention Mode | E-health | 11 | <0.001 | 80.90% | 0.37 (0.19, 0.54) | <0.001 |
| In-person | 7 | 0.054 | 51.50% | 0.47 (0.25, 0.55) | <0.001 | |
| Overall | 18 | <0.001 | 77.00% | 0.41 (0.27, 0.55) | <0.001 | |
| Between | 0.488 | |||||
| Theory | Yes | 7 | <0.001 | 78.20% | 0.30 (0.09, 0.50) | 0.006 |
| No | 11 | <0.001 | 73.60% | 0.50 (0.29, 0.71) | <0.001 | |
| Overall | 18 | <0.001 | 77.00% | 0.41 (0.27, 0.55) | <0.001 | |
| Between | 0.172 | |||||
| Duration | >5 W | 13 | <0.001 | 77.00% | 0.42 (0.25, 0.59) | <0.001 |
| ≤5 W | 5 | 0.001 | 79.50% | 0.43 (0.05, 0.81) | <0.001 | |
| Overall | 18 | 0.0001 | 77.00% | 0.41 (0.27, 0.55) | <0.001 | |
| Between | 0.974 | |||||
| Female Ratio | >50% | 13 | <0.001 | 80.70% | 0.45 (0.27, 0.63) | <0.001 |
| ≤50% | 5 | 0.021 | 65.50% | 0.35 (0.08, 0.63) | 0.013 | |
| Overall | 18 | <0.001 | 77.00% | 0.41 (0.27, 0.55) | <0.001 | |
| Between | 0.572 | |||||
| Sample Size | >100 | 6 | <0.001 | 80.70% | 0.26 (0.06, 0.36) | 0.006 |
| ≤100 | 12 | 0.172 | 27.80% | 0.56 (0.39, 0.73) | <0.001 | |
| Overall | 18 | <0.001 | 77.00% | 0.41 (0.27, 0.55) | <0.001 | |
| Between | 0.002 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuan, F.; Peng, S.; Khairani, A.Z.; Liang, J. A Systematic Review and Meta-Analysis of the Efficacy of Physical Activity Interventions among University Students. Sustainability 2024, 16, 1369. https://doi.org/10.3390/su16041369
Yuan F, Peng S, Khairani AZ, Liang J. A Systematic Review and Meta-Analysis of the Efficacy of Physical Activity Interventions among University Students. Sustainability. 2024; 16(4):1369. https://doi.org/10.3390/su16041369
Chicago/Turabian StyleYuan, Fang, Sanying Peng, Ahmad Zamri Khairani, and Jinghong Liang. 2024. "A Systematic Review and Meta-Analysis of the Efficacy of Physical Activity Interventions among University Students" Sustainability 16, no. 4: 1369. https://doi.org/10.3390/su16041369