

Effects of 12 Weeks of Physical-Cognitive Dual-Task Training on Executive Functions, Depression, Sleep Quality, and Quality of Life in Older Adult Women: A Randomized Pilot Study
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
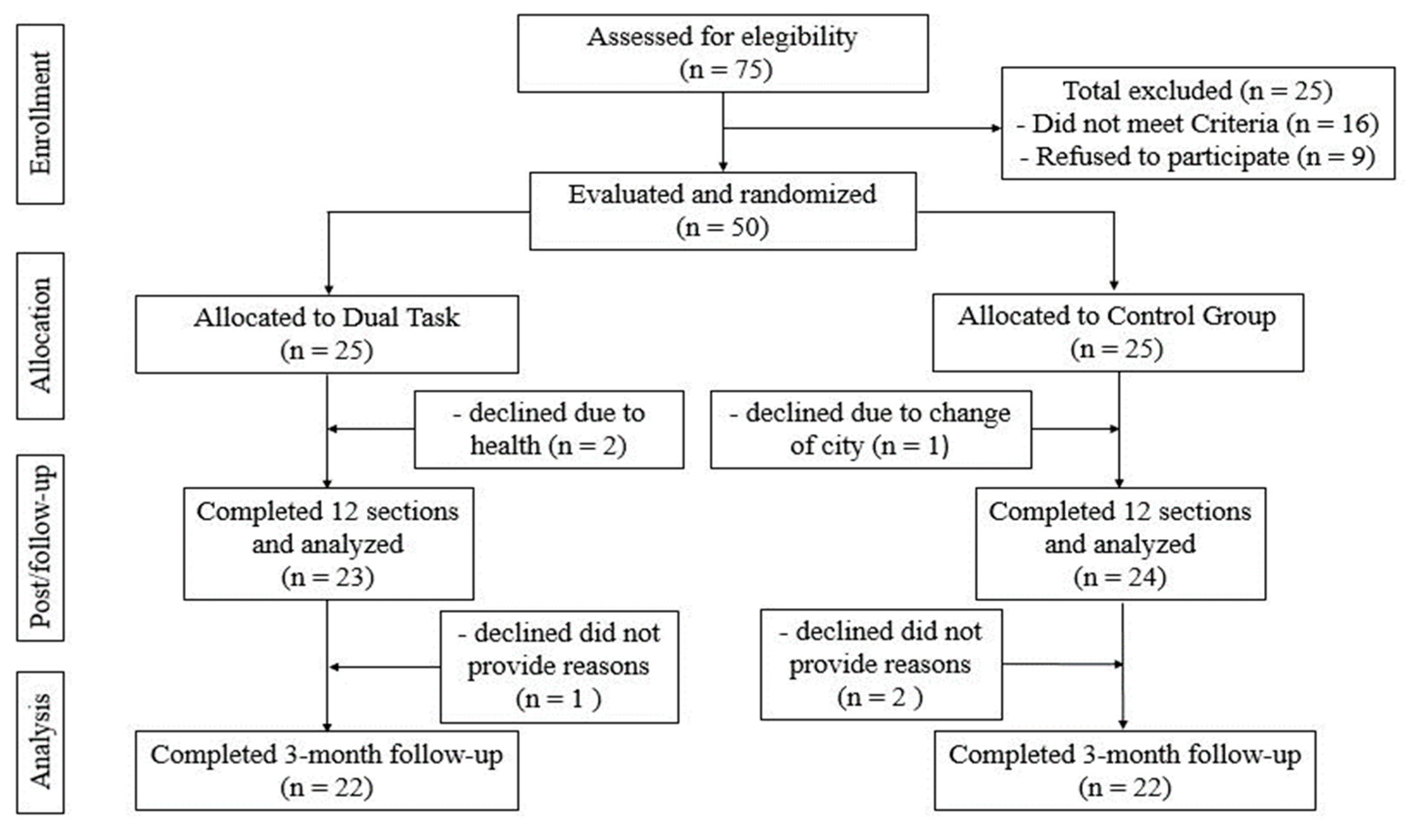
2.1.1. Sample
2.1.2. Eligibility
2.2. Intervention
2.2.1. Dual-Task Training
- -
- Phase I: A warm-up at the beginning of each session (10 min) with supervised walking exercises on a flat surface, general joint mobilization, and stretching exercises;
- -
- Phase II: Dual-task training (40 min), consisting of balance and gait exercises arranged in four stations, with a 10-min permanence in each station, 4 sets/8–12 repetitions per exercise. Over 12 weeks, the following training strategies were used:(1) two concurrent motor tasks (e.g., walking with hand engagement manipulating objects), (2) walking and simultaneously performing a cognitive task with internal interference factors (Stroop, calculations, fluency verbal, memorization), (3) walking on an unstable and/or reduced surface with the simultaneous requirement of visual tasks, word spelling and/or countdown, (4) in posture activities: semi-tandem standing with eyes open or closed (with changes in arm movement or cognitive tasks), (5) walking across obstacles or overcoming them (with a simultaneous resolution of cognitive tasks);
- -
- Phase III: Return to calm (10 min) with relaxation and breathing exercises, lying on the floor. The training protocol was performed in a fitness room (20 × 20 m). Progression of cognitive-motor difficulty/load level occurred every two weeks (after four training sessions). To enhance the social component, DT training was performed in groups of 5-6 people at each station of the circuit, switching to a new station every eight minutes. Table 1 summarizes the four approaches that integrated the DT training, as well as the strategies used for the progression of tasks.
2.2.2. Education Control Group
2.3. Adherence
2.4. Outcome and Measurements
2.4.1. Primary Outcome
2.4.2. Secondary Outcomes
2.5. Covariates
2.6. Statistics
3. Results
3.1. Sample Characteristic
3.2. Intervention Effects
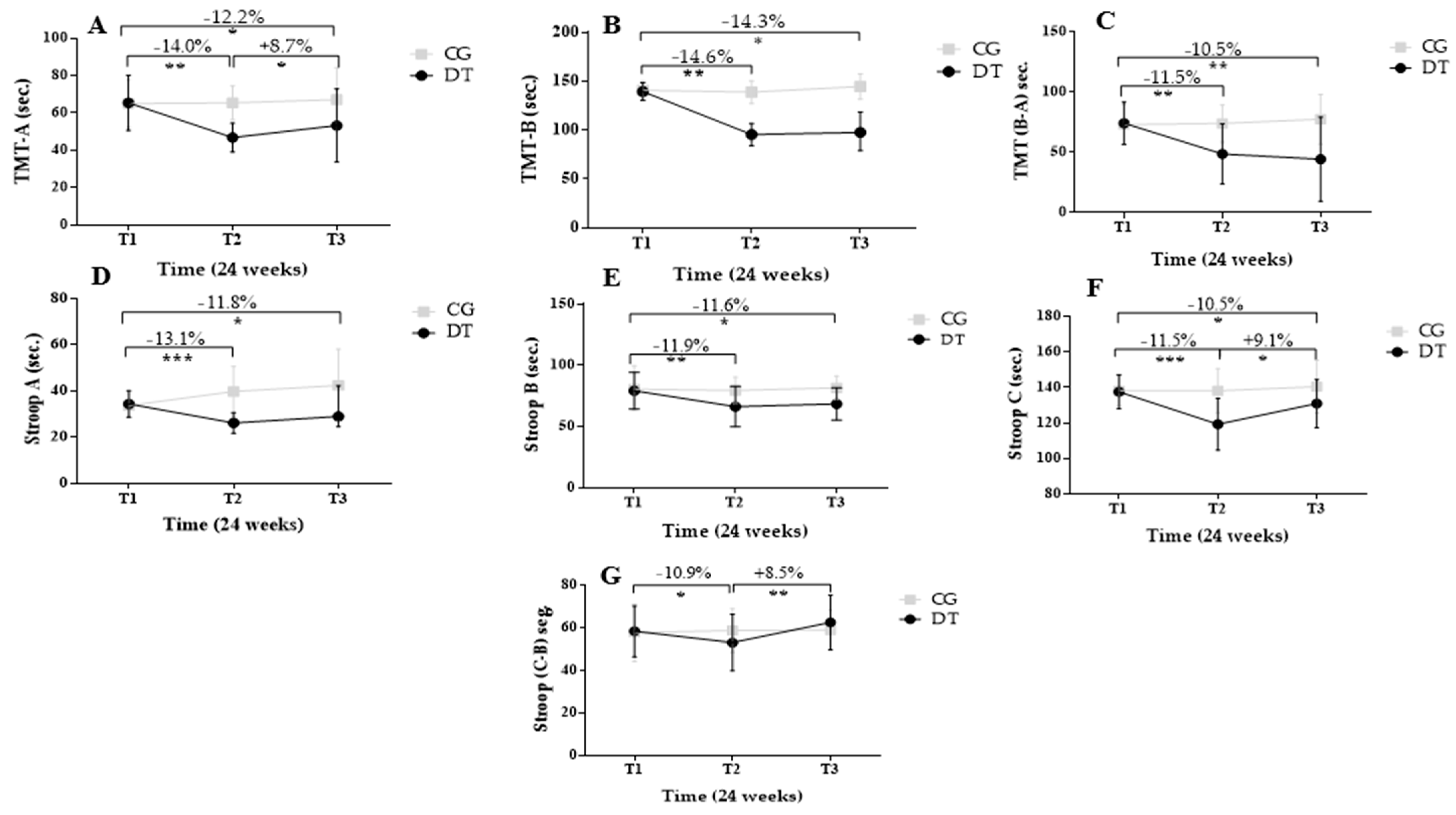
3.2.1. Cognitive Assessments
3.2.2. Depression and Sleep Quality
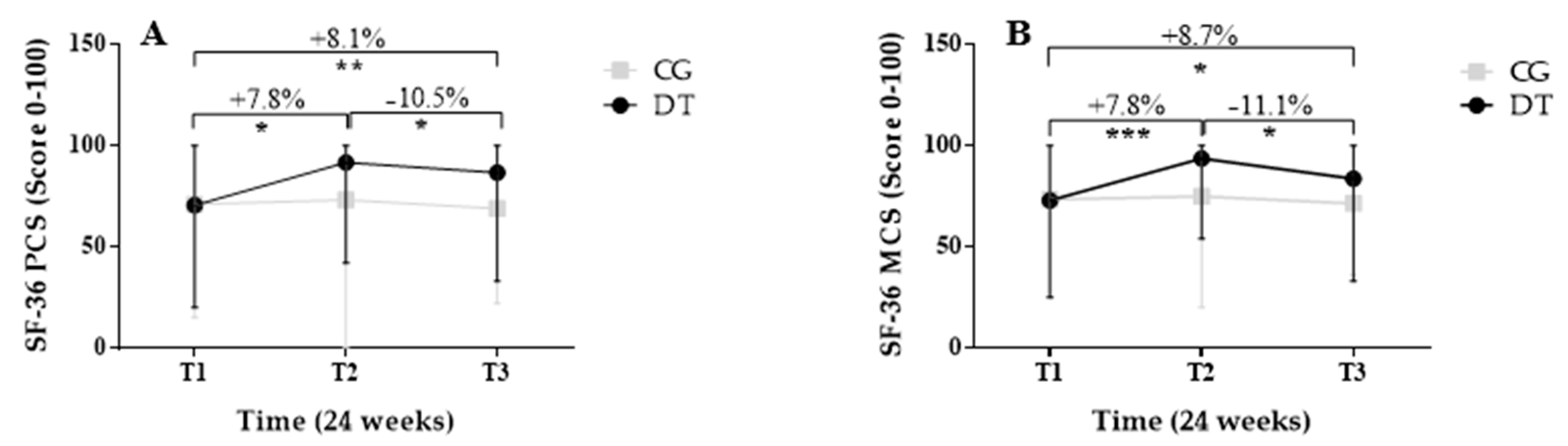
3.2.3. Quality of Life (QoL)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dziechciaż, M.; Filip, R. Biological psychological and social determinants of old age: Bio-psycho-social aspects of human aging. Ann. Agric. Environ. Med. 2014, 21, 835–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabinovici, G.D.; Stephens, M.L.; Possin, K.L. Executive Dysfunction. Contin. Lifelong Learn. Neurol. 2015, 21, 646–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murman, D. The Impact of Age on Cognition. Semin. Heart 2015, 36, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Harada, C.N.; Natelson Love, M.C.; Triebel, K.L. Normal Cognitive Aging. Clin. Geriatr. Med. 2013, 29, 737–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oschwald, J.; Guye, S.; Liem, F.; Rast, P.; Willis, S.; Röcke, C.; Jäncke, L.; Martin, M.; Mérillat, S. Brain structure and cognitive ability in healthy aging: A review on longitudinal correlated change. Rev. Neurosci. 2019, 31, 1–57. [Google Scholar] [CrossRef] [Green Version]
- MacPherson, S.E. Definition: Dual-tasking and multitasking. Cortex 2018, 106, 313–314. [Google Scholar] [CrossRef]
- Peters, R. Ageing and the brain. Postgrad. Med. J. 2006, 82, 84–88. [Google Scholar] [CrossRef]
- Wollesen, B.; Voelcker-Rehage, C. Training effects on motor–cognitive dual-task performance in older adults. Eur. Rev. Aging Phys. Act. 2014, 11, 5–24. [Google Scholar] [CrossRef] [Green Version]
- Lauenroth, A.; Ioannidis, A.E.; Teichmann, B. Influence of combined physical and cognitive training on cognition: A systematic review. BMC Geriatr. 2016, 16, 141. [Google Scholar] [CrossRef] [Green Version]
- Wollesen, B.; Wanstrath, M.; van Schooten, K.S.; Delbaere, K. A taxonomy of cognitive tasks to evaluate cognitive-motor interference on spatiotemoporal gait parameters in older people: A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 2019, 16, 12. [Google Scholar] [CrossRef]
- Murillo-Garcia, A.; Villafaina, S.; Collado-Mateo, D.; Leon-Llamas, J.L.; Gusi, N. Effect of dance therapies on motor-cognitive dual-task performance in middle-aged and older adults: A systematic review and meta-analysis. Disabil. Rehabil. 2021, 43, 3147–3158. [Google Scholar] [CrossRef] [PubMed]
- Bayot, M.; Dujardin, K.; Tard, C.; Defebvre, L.; Bonnet, C.T.; Allart, E.; Delval, A. The interaction between cognition and motor control: A theoretical framework for dual-task interference effects on posture, gait initiation, gait and turning. Neurophysiol. Clin. 2018, 48, 361–375. [Google Scholar] [CrossRef]
- Leone, C.; Feys, P.; Moumdjian, L.; D’Amico, E.; Zappia, M.; Patti, F. Cognitive-motor dual-task interference: A systematic review of neural correlates. Neurosci. Biobehav. Rev. 2017, 75, 348–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hötting, K.; Röder, B. Beneficial effects of physical exercise on neuroplasticity and cognition. Neurosci. Biobehav. Rev. 2013, 37, 2243–2257. [Google Scholar] [CrossRef] [PubMed]
- Bayot, M.; Dujardin, K.; Dissaux, L.; Tard, C.; Defebvre, L.; Bonnet, C.T.; Allart, E.; Allali, G.; Delval, A. Can dual-task paradigms predict Falls better than single task?—A systematic literature review. Neurophysiol. Clin. 2020, 50, 401–440. [Google Scholar] [CrossRef] [PubMed]
- Teraz, K.; Šlosar, L.; Paravlić, A.H.; de Bruin, E.D.; Marusic, U. Impact of Motor-Cognitive Interventions on Selected Gait and Balance Outcomes in Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Psychol. 2022, 13, 837710. [Google Scholar] [CrossRef]
- Mccrum, C.; Karamanidis, K.; Willems, P.; Zijlstra, W.; Meijer, K. Retention, savings and interlimb transfer of reactive gait adaptations in humans following unexpected perturbations. Commun. Biol. 2018, 1, 230. [Google Scholar] [CrossRef] [Green Version]
- Muir-Hunter, S.W.; Wittwer, J.E. Dual-task testing to predict falls in community-dwelling older adults: A systematic review. Physiotherapy 2016, 102, 29–40. [Google Scholar] [CrossRef]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. The role of executive function and attention in gait. Mov. Disord. 2008, 23, 329–342. [Google Scholar] [CrossRef] [Green Version]
- Kearney, F.C.; Harwood, R.H.; Gladman, J.R.F.; Lincoln, N.; Masud, T. The relationship between executive function and falls and gait abnormalities in older adults: A systematic review. Dement. Geriatr. Cogn. Disord. 2013, 36, 20–35. [Google Scholar] [CrossRef]
- Montero-Odasso, M.; Speechley, M. Falls in Cognitively Impaired Older Adults: Implications for Risk Assessment And Prevention. J. Am. Geriatr. Soc. 2018, 66, 367–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gobbo, S.; Bergamin, M.; Sieverdes, J.C.; Ermolao, A.; Zaccaria, M. Effects of exercise on dual-task ability and balance in older adults: A systematic review. Arch. Gerontol. Geriatr. 2014, 58, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Li, K.Z.H.; Roudaia, E.; Lussier, M.; Bherer, L.; Leroux, A.; McKinley, P.A. Benefits of Cognitive Dual-Task Training on Balance Performance in Healthy Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2010, 65, 1344–1352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arcos-Burgos, M.; Lopera, F.; Sepulveda-Falla, D.; Mastronardi, C. Neural Plasticity during Aging. Neural Plast. 2019, 2019, 6042132. [Google Scholar] [CrossRef]
- Bherer, L. Cognitive plasticity in older adults: Effects of cognitive training and physical exercise. Ann. N. Y. Acad. Sci. 2015, 1337, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Plummer, P.; Zukowski, L.A.; Giuliani, C.; Hall, A.M.; Zurakowski, D. Effects of Physical Exercise Interventions on Gait-Related Dual-Task Interference in Older Adults: A Systematic Review and Meta-Analysis. Gerontology 2015, 62, 94–117. [Google Scholar] [CrossRef] [PubMed]
- Springer, S.; Giladi, N.; Peretz, C.; Yogev, G.; Simon, E.S.; Hausdorff, J.M. Dual-tasking effects on gait variability: The role of aging, falls, and executive function. Mov. Disord. 2006, 21, 950–957. [Google Scholar] [CrossRef]
- Agmon, M.; Shochat, T.; Kizony, R. Sleep quality is associated with walking under dual-task, but not single-task performance. Gait Posture 2016, 49, 127–131. [Google Scholar] [CrossRef]
- Cox, S.R.; Ritchie, S.J.; Allerhand, M.; Hagenaars, S.P.; Radakovic, R.; Breen, D.P.; Davies, G.; Riha, R.L.; Harris, S.E.; Starr, J.M.; et al. Sleep and cognitive aging in the eighth decade of life. Sleep 2019, 42, zsz019. [Google Scholar] [CrossRef]
- Steptoe, A.; Deaton, A.; Stone, A.A. Subjective wellbeing, health, and ageing. Lancet 2015, 385, 640–648. [Google Scholar] [CrossRef]
- Curi, V.S.; Vilaça, J.; Haas, A.N.; Fernandes, H.M. Effects of 16-weeks of Pilates on health perception and sleep quality among elderly women. Arch. Gerontol. Geriatr. 2018, 74, 118–122. [Google Scholar] [CrossRef]
- Archer, T.; Josefsson, T.; Lindwall, M. Effects of Physical Exercise on Depressive Symptoms and Biomarkers in Depression. CNS Neurol. Disord.-Drug Targets 2015, 13, 1640–1653. [Google Scholar] [CrossRef] [PubMed]
- Bjerk, M.; Brovold, T.; Skelton, D.A.; Liu-Ambrose, T.; Bergland, A. Effects of a falls prevention exercise programme on health-related quality of life in older home care recipients: A randomised controlled trial. Age Ageing 2019, 48, 213–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trombini-Souza, F.; de Souza Azevedo Nogueira, R.T.; Serafim, A.C.B.; de Lima, T.M.M.; Xavier, M.K.A.; Perracini, M.R.; de Araújo, R.C.; Sacco, I.C.N.; de Maio Nascimento, M. Concern About Falling, Confidence in Balance, Quality of Life, and Depression Symptoms in Community-Dwelling Older Adults After a 24-week Dual-Task Training With Variable and Fixed Priority: A Randomized Controlled Trial. Res. Aging 2022, 44, 658–668. [Google Scholar] [CrossRef] [PubMed]
- Cepellos, V.M. Feminization of aging: A multifaceted phenomenon beyond the numbers. Rev. Adm. Empres. 2021, 61, 1–7. [Google Scholar] [CrossRef]
- IBGE-Instituto Brasileiro de Geografia e Estatística IBGE Lança Estudo Metodológico Sobre Mudança Demográfica e Projeções de População. Available online: https://agenciadenoticias.ibge.gov.br/agencia-sala-de-imprensa/2013-agencia-de-noticias/releases/9831-ibge-lanca-estudo-metodologico-sobre-mudanca-demografica-e-projecoes-de-populacao (accessed on 20 October 2022).
- Noce Kirkwood, R.; de Souza Moreira, B.; Mingoti, S.A.; Faria, B.F.; Sampaio, R.F.; Alves Resende, R. The slowing down phenomenon: What is the age of major gait velocity decline? Maturitas 2018, 115, 31–36. [Google Scholar] [CrossRef]
- Senicato, C.; de Azevedo, R.C.S.; de Azevedo Barros, M.B. Common mental disorders in adult women: Identifying the most vulnerable segments. Cien. Saude Colet. 2018, 23, 2543–2554. [Google Scholar] [CrossRef]
- Campbell, M.; Fitzpatrick, R.; Haines, A.; Kinmonth, A.L.; Sandercock, P.; Spiegelhalter, D.; Tyrer, P. Framework for design and evaluation of complex interventions to improve health. BMJ 2000, 321, 694–696. [Google Scholar] [CrossRef] [Green Version]
- Wollesen, B.; Schulz, S.; Seydell, L.; Delbaere, K. Does dual task training improve walking performance of older adults with concern of falling? BMC Geriatr. 2017, 17, 213. [Google Scholar] [CrossRef] [Green Version]
- Silsupadol, P.; Lugade, V.; Shumway-Cook, A.; van Donkelaar, P.; Chou, L.-S.; Mayr, U.; Woollacott, M.H. Training-related changes in dual-task walking performance of elderly persons with balance impairment: A double-blind, randomized controlled trial. Gait Posture 2009, 29, 634–639. [Google Scholar] [CrossRef]
- Bertolucci, P.H.F.; Brucki, S.M.D.; Campacci, S.R.; Yara, J. O Mini-Exame do Estado Mental em uma população geral. Impacto da escolaridade. Arq. Neuropsiquiatr. 1994, 52, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Liebherr, M.; Schubert, P.; Schiebener, J.; Kersten, S.; Haas, C.T. Dual-tasking and aging-About multiple perspectives and possible implementations in interventions for the elderly. Cogent Psychol. 2016, 3, 1261440. [Google Scholar] [CrossRef]
- Silsupadol, P.; Shumway-Cook, A.; Lugade, V.; van Donkelaar, P.; Chou, L.S.; Mayr, U.; Woollacott, M.H. Effects of Single-Task Versus Dual-Task Training on Balance Performance in Older Adults: A Double-Blind, Randomized Controlled. Arch. Phys. Med. Rehabil. 2009, 90, 381–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nascimento, M.D.; Ramos, L.S.; Gomes, A.V.T.M.; Maia, N.J.S. Educação em saúde em uma universidade aberta à terceira idade: A experiência de estudantes de medicina. Rev. Educ. Univ. Fed. Val. São Fr. 2020, 10, 55–83. [Google Scholar]
- Sherrington, C.; Tiedemann, A.; Fairhall, N.; Close, J.C.T.; Lord, S.R. Exercise to prevent falls in older adults: An updated meta-analysis and best practice recommendations. NSW Public Health Bull. 2011, 22, 78–83. [Google Scholar] [CrossRef] [Green Version]
- Brucki, S.; Nitrini, R.; Caramelli, P.; Bertolucci, P.H.; Okamoto, I.H. Suggestions for utilization of the mini-mental state examination in Brazil. Arq. Neuropsiquiatr. 2003, 61, 777–781. [Google Scholar] [CrossRef] [Green Version]
- Reitan, R.M. Validity of the Trail Making Test as an Indicator of Organic Brain Damage. Percept. Mot. Ski. 1958, 8, 271–276. [Google Scholar] [CrossRef]
- Stroop, J.R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 1935, 18, 643–662. [Google Scholar] [CrossRef]
- Misdraji, E.L.; Gass, C.S. The Trail Making Test and its neurobehavioral components. J. Clin. Exp. Neuropsychol. 2010, 32, 159–163. [Google Scholar] [CrossRef]
- MacLeod, C.M. Half a century of research on the Stroop effect: An integrative review. Psychol. Bull. 1991, 109, 163–203. [Google Scholar] [CrossRef]
- Castelo, M.S.; Coelho-Filho, J.M.; Carvalho, A.F.; Lima, J.W.O.; Noleto, J.C.S.; Ribeiro, K.G.; Siqueira-Neto, J.I. Validity of the Brazilian version of the Geriatric Depression Scale (GDS) among primary care patients. Int. Psychogeriatr. 2010, 22, 109–113. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J.; III, C.F.R.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Ciconelli, R.M.; Ferraz, M.B.; Santos, W.; Meinão, I.; Quaresma, M.R. Tradução para o português e validação do questionário genérico de avaliação da qualidade de vida “Medical Outcomes Study 36-item Short-Form. Rev. Bras. Reumatol. 1999, 39, 145–150. [Google Scholar]
- Cohen, J. Eta-squared and partial eta-squared in fixed factor ANOVA designs. Educ. Psychol. Meas. 1973, 33, 107–112. [Google Scholar] [CrossRef]
- Wollesen, B.; Mattes, K.; Schulz, S.; Bischoff, L.L.; Seydell, L.; Bell, J.W.; von Duvillard, S.P. Effects of Dual-Task Management and Resistance Training on Gait Performance in Older Individuals: A Randomized Controlled Trial. Front. Aging Neurosci. 2017, 9, 415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eggenberger, P.; Theill, N.; Holenstein, S.; Schumacher, V.; de Bruin, E. Multicomponent physical exercise with simultaneous cognitive training to enhance dual-task walking of older adults: A secondary analysis of a 6-month randomized controlled trial with 1-year follow-up. Clin. Interv. Aging 2015, 10, 1711–1732. [Google Scholar] [CrossRef] [Green Version]
- Falbo, S.; Condello, G.; Capranica, L.; Forte, R.; Pesce, C. Effects of Physical-Cognitive Dual Task Training on Executive Function and Gait Performance in Older Adults: A Randomized Controlled Trial. Biomed. Res. Int. 2016, 2016, 5812092. [Google Scholar] [CrossRef] [Green Version]
- Kitazawa, K.; Showa, S.; Hiraoka, A.; Fushiki, Y.; Sakauchi, H.; Mori, M. Effect of a dual-task net-step exercise on cognitive and gait function in older adults. J. Geriatr. Phys. Ther. 2015, 38, 133–140. [Google Scholar] [CrossRef]
- Azadian, E.; Torbati, H.R.T.; Kakhki, A.R.S.; Farahpour, N. The effect of dual task and executive training on pattern of gait in older adults with balance impairment: A Randomized controlled trial. Arch. Gerontol. Geriatr. 2016, 62, 83–89. [Google Scholar] [CrossRef]
- Nishiguchi, S.; Yamada, M.; Tanigawa, T.; Sekiyama, K.; Kawagoe, T.; Suzuki, M.; Yoshikawa, S.; Abe, N.; Otsuka, Y.; Nakai, R.; et al. A 12-Week Physical and Cognitive Exercise Program Can Improve Cognitive Function and Neural Efficiency in Community-Dwelling Older Adults: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2015, 63, 1355–1363. [Google Scholar] [CrossRef] [Green Version]
- de Bruin, E.; Eggenberger, P.; Schumacher, V.; Angst, M.; Theill, N. Does multicomponent physical exercise with simultaneous cognitive training boost cognitive performance in older adults? A 6-month randomized controlled trial with a 1-year follow-up. Clin. Interv. Aging 2015, 10, 1335–1349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heiden, E.; Lajoie, Y. Games-based biofeedback training and the attentional demands of balance in older adults. Aging Clin. Exp. Res. 2010, 22, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Schoene, D.; Lord, S.R.; Delbaere, K.; Severino, C.; Davies, T.A.; Smith, S.T. A Randomized Controlled Pilot Study of Home-Based Step Training in Older People Using Videogame Technology. PLoS ONE 2013, 8, e57734. [Google Scholar] [CrossRef] [Green Version]
- Buragadda, S.; Alyaemni, A. Effect of Dual-Task Training (Fixed Priority-Versus-Variable Priority) for Improving Balance in Older Adults. World Appl. Sci. J. 2012, 20, 884–888. [Google Scholar]
- Callisaya, M.L.; Blizzard, L.; Schmidt, M.D.; McGinley, J.L.; Srikanth, V.K. Ageing and gait variability-a population-based study of older people. Age Ageing 2010, 39, 191–197. [Google Scholar] [CrossRef] [Green Version]
- Rosano, C.; Aizenstein, H.; Brach, J.; Longenberger, A.; Studenski, S.; Newman, A.B. Gait Measures Indicate Underlying Focal Gray Matter Atrophy in the Brain of Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2008, 63, 1380–1388. [Google Scholar] [CrossRef] [Green Version]
- Allali, G.; Montembeault, M.; Brambati, S.M.; Bherer, L.; Blumen, H.M.; Launay, C.P.; Liu-Ambrose, T.; Helbostad, J.L.; Verghese, J.; Beauchet, O. Brain structure covariance associated with gait control in aging. J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 2019, 74, 705–713. [Google Scholar] [CrossRef]
- Cham, R.; Perera, S.; Studenski, S.A.; Bohnen, N.I. Striatal dopamine denervation and sensory integration for balance in middle-aged and older adults. Gait Posture 2007, 26, 516–525. [Google Scholar] [CrossRef]
- Tombaugh, T. Trail Making Test A and B: Normative data stratified by age and education. Arch. Clin. Neuropsychol. 2004, 19, 203–214. [Google Scholar] [CrossRef]
- Dorfman, M.; Herman, T.; Brozgol, M.; Shema, S.; Weiss, A.; Hausdorff, J.M.; Mirelman, A. Dual-Task Training on a Treadmill to Improve Gait and Cognitive Function in Elderly Idiopathic Fallers. J. Neurol. Phys. Ther. 2014, 38, 246–253. [Google Scholar] [CrossRef]
- Tasvuran Horata, E.; Cetin, S.Y.; Erel, S. Effects of individual progressive single- and dual-task training on gait and cognition among older healthy adults: A randomized-controlled comparison study. Eur. Geriatr. Med. 2021, 12, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Perrochon, A.; Kemoun, G.; Watelain, E.; Dugué, B.; Berthoz, A. The “Stroop Walking Task”: An innovative dual-task for the early detection of executive function impairment. Neurophysiol. Clin. Neurophysiol. 2015, 45, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, J.M.; Rios, D.A.; Edelberg, H.K. Gait variability and fall risk in community-living older adults: A 1-year prospective study. Arch. Phys. Med. Rehabil. 2001, 82, 1050–1056. [Google Scholar] [CrossRef]
- Herssens, N.; Verbecque, E.; Hallemans, A.; Vereeck, L.; Van Rompaey, V.; Saeys, W. Do spatiotemporal parameters and gait variability differ across the lifespan of healthy adults? A systematic review. Gait Posture 2018, 64, 181–190. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Focus | Training Tasks | Method and Progression |
|---|---|---|
| Gait | (a) Tasks: walking with short or long steps, over obstacles, on the heel or tiptoe; (b) Sensory input: impaired vision, enhancement of somatosensory integration; (c) Directions: forward, backward, left/right, diagonal. | (a) Circuit with 5 stations; (b) Intensification of the task through fast or slow walking, inclusion of turns (180° and 360°); (c) Equipment: ropes, bows, balls, foam mattress, ramp, steps. |
| Static balance | (a) Tasks: biped, semi-tandem, tandem, single-leg, weight on the feet (heels, lateral, medial, or toes). | (a) Circuit with 5 stations; (b) Simulation of daily life tasks in a static position (increased demand for hip or ankle strategies); (c) Surface: soft, hard, stable, unstable, or reduced. |
| Dynamic balance | (a) Tasks: during normal gait, narrow gait, lap gait, tandem gait. | (a) Circuit with 5 stations; (b) Challenges: addition of arm movements outside the center of pressure (COP), gait backward; (c) Surface: soft, hard, stable, unstable, or reduced. |
| Cognitive task | Tasks: (a) add and subtract: for example, solve math problems with a countdown (100, 97, 94, 91, 89, …), (b) verbal fluency: name fruits, people, or cities starting with different letters of the alphabet; (c) working memory: memorizing a sequence of 3–5 different words and after reproducing; (d) reaction time: react as quickly as possible to questions or images (Stroop effect). | (a) Increase the difficulty of the category, expand the count or elements of memorization; (b) Inverting the order of the sequence of words or numbers (back to front); (c) Variation of response time; (d) Alternating combination of series or length of tasks; (e) Alternating combination of incongruent and congruent task. |
| Variable | Dual-Task (n = 22) | Control Group (n = 22) | p-Value |
|---|---|---|---|
| Age (years) | 66.14 ± 4.15 | 66.27 ± 4.04 | 0.913 † |
| BMI (kg/m2) | 27.68 ± 3.93 | 28.18 ± 4.67 | 0.703 † |
| Falls (12 months) | 0.27 ± 0.19 | 0.185 ± 0.21 | 0.132 † |
| Medication | 0.161 † | ||
| 1–4 types (f) | 20 (90.9%) | 19 (86.3%) | |
| >4 types (f) | 2 (9.0%) | 3 (13.6%) | |
| Education level | 0.574 † | ||
| 1–4 years | 3 (13.6) | 4 (18.1) | |
| ≥5 years | 19 (86.3) | 18 (81.8) | |
| MMSE | 25.27 ± 1.38 | 25.32 ± 3.57 | 0.688 † |
| Comorbidities | |||
| Diabetes mellitus | 0.545 * | ||
| Yes (f) | 4 (18.1%) | 18 (81.8%) | |
| Hypertension | 0.680 * | ||
| Yes (f) | 9 (40.9%) | 13 (59.0%) | |
| Visual acuity | 0.761 * | ||
| Yes (f) | 20 (90.9%) | 2 (9.0%) | |
| Hearing | 0.550 * | ||
| Yes (f) | 11 (50.0%) | 12 (54.5%) | |
| Labyrinthitis | 0.079 * | ||
| Yes (f) | 4 (18.1%) | 2 (9.0%) | |
| Osteoporosis | 0.294 * | ||
| Yes (f) | 14 (63.6%) | 8 (36.3%) | |
| Rheumatism | 0.488 * | ||
| Yes (f) | 6 (27.2%) | 16 (72.7%) |
| Dual-Task | Group Control | Time | Time * Group † | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (Baseline) n = 22 | (12 Weeks) n = 22 | (24 Weeks) n = 22 | (Baseline) n = 22 | (12 Weeks) n = 22 | (24 Weeks) n = 22 | F | p | ηp2 | F | p | ηp2 | |
| Cognition (s) | ||||||||||||
| TMT-A | 65.45 ± 14.71 a,b | 46.86 ± 7.71 c,† | 53.32 ± 19.64 † | 65.00 ± 12.55 | 65.45 ± 9.10 | 67.18 ± 17.08 | 8.738 | <0.001 | 0.096 | 5.066 | 0.008 | 0.080 |
| TMT-B | 139.59 ± 8.95 a,b | 95.55 ± 11.42 | 97.68 ± 20.70 | 140.86 ± 9.80 | 139.05 ± 11.78 | 144.68 ± 13.00 | 36.794 | <0.001 | 0.099 | 39.558 | <0.001 | 0.099 |
| ΔTMT (B-A) | 74.13 ± 17.58 a,b | 48.68 ± 25.12 | 44.36 ± 34.95 | 73.09 ± 16.76 | 74.04 ± 15.42 | 77.50 ± 20.69 | 6.301 | 0.006 | 0.081 | 9.754 | <0.001 | 0.095 |
| Stroop A | 34.36 ± 5.72 a,b | 26.14 ± 4.48 | 28.95 ± 4.36 | 33.73 ± 5.27 b | 39.77 ± 10.81 | 42.36 ± 15.68 | 2.622 | 0.028 | 0.050 | 2.109 | 0.014 | 0.040 |
| Stroop B | 79.18 ± 14.95 a,b | 66.23 ± 16.60 | 68.45 ± 13.13 | 80.41 ± 18.22 | 79.45 ± 10.74 | 81.59 ± 9.58 | 3.482 | 0.036 | 0.060 | 3.278 | 0.028 | 0.057 |
| Stroop C | 137.59 ± 9.54 a,b | 119.36 ± 14.63 c,† | 122.00 ± 13.53 | 138.18 ± 8.47 | 138.23 ± 12.44 | 140.55 ± 14.83 | 6.781 | 0.040 | 0.091 | 6.253 | 0.039 | 0.088 |
| Stroop (C-B) | 58.41 ± 11.82 a | 53.13 ± 13.21 c,† | 53.55 ± 12.73 | 57.77 ± 13.45 | 58.78 ± 10.21 | 58.96 ± 9.36 | 2.654 | 0.008 | 0.074 | 2.832 | 0.004 | 0.078 |
| Depression | ||||||||||||
| GDS | 3.00 (1–10) | 1.50 (0–9) | 1.50 (0–5) | 3.50 (1–11) | 2.50 (0–15) | 3.00 (0–9) | 3.043 | 0.068 | 0.049 | 0.820 | 0.415 | 0.016 |
| Sleep Quality | ||||||||||||
| PSQI | 5.00 (2–10) | 5.00 (1–11) | 5.50 (1–9) | 4.00 (2–10) | 4.00 (1–9) | 5.00 (1–13) | 1.695 | 0.190 | 0.034 | 1.173 | 0.176 | 0.036 |
| SF-36 | ||||||||||||
| PCS | 70.67 (20–100) a,b | 91.87 (42–100) c,† | 86.87 (42–100) † | 71.75 (15–100) | 73.25 (0–100) | 69.00 (22–100) | 7.643 | 0.006 | 0.066 | 3.043 | 0.012 | 0.062 |
| MCS | 73.00 (25–100) a,b | 93.75 (0–100) c,† | 83.87 (33–100) † | 73.50 (25–100) | 75.00 (20–100) | 71.62 (36–100) | 6.373 | 0.004 | 0.044 | 1.953 | 0.009 | 0.054 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nascimento, M.d.M.; Maduro, P.A.; Rios, P.M.B.; Nascimento, L.d.S.; Silva, C.N.; Kliegel, M.; Ihle, A. Effects of 12 Weeks of Physical-Cognitive Dual-Task Training on Executive Functions, Depression, Sleep Quality, and Quality of Life in Older Adult Women: A Randomized Pilot Study. Sustainability 2023, 15, 97. https://doi.org/10.3390/su15010097
Nascimento MdM, Maduro PA, Rios PMB, Nascimento LdS, Silva CN, Kliegel M, Ihle A. Effects of 12 Weeks of Physical-Cognitive Dual-Task Training on Executive Functions, Depression, Sleep Quality, and Quality of Life in Older Adult Women: A Randomized Pilot Study. Sustainability. 2023; 15(1):97. https://doi.org/10.3390/su15010097
Chicago/Turabian StyleNascimento, Marcelo de Maio, Paula Andreatta Maduro, Pâmala Morais Bagano Rios, Lara dos Santos Nascimento, Carolina Nascimento Silva, Matthias Kliegel, and Andreas Ihle. 2023. "Effects of 12 Weeks of Physical-Cognitive Dual-Task Training on Executive Functions, Depression, Sleep Quality, and Quality of Life in Older Adult Women: A Randomized Pilot Study" Sustainability 15, no. 1: 97. https://doi.org/10.3390/su15010097