1. Introduction
With the internet’s reach and data processing power on the rise, the global health business, and telemedicine in particular, has new growth opportunities. Data sharing and analysis, wearables, cloud computing, robotics, and the Internet of Things (IoT) are just a few of the potential areas for innovation in the coming decade. These considerations highlight the importance of artificial intelligence (AI) in healthcare technology administration and deployment. In healthcare, it is utilized to deal with the influx of data, the need for precision in complicated operations, and the growing demand for medical treatment. Automating hospital logistics is necessary to improve the efficacy of resource allocation and the delivery of healthcare demands and operations [
1].
Telemedicine is the practice of conducting remote medical consultations, exams, and operations and facilitating interprofessional teamwork in the healthcare industry. It is frequently emphasized that telemedicine is an “open and continually growing science” that reacts and adapts to the changing health demands and settings of communities by incorporating new technological developments. The major goals of telemedicine include: [
2]
- 1.
Increasing access to healthcare.
- 2.
Improving communication between healthcare providers.
- 3.
Improved time efficiency and reduced cost of logistics.
Research on effective and reliable procedures for medical fields and studies on wireless technology’s application to sensors have been growing over the last decade, particularly in the context of electronic patient records and home monitoring. In the healthcare industry, data have always played a vital role in the provision of quality patient care and decision-making. With the advent of digital technology in healthcare, a vast amount of data is being generated from various sources, such as medical equipment, insurance, life sciences, and medical research [
3,
4]. The abundance of data presents a tremendous opportunity to transform healthcare by providing valuable insights to support decision-making, improve patient care, respond to real-time situations, and save more lives. This transformation is made possible by leveraging advanced analytics, machine learning, and artificial intelligence techniques that allow stakeholders to extract meaningful and actionable insights from the data [
5]. In addition to analyzing historical data, these techniques enable predictive analytics to forecast future outcomes and prescriptive analytics to determine the best course of action for the current situation. By harnessing the power of data, healthcare stakeholders can optimize resource utilization, improve processes and services, and reduce costs on the operational and financial front [
6,
7].
However, our understanding of AI and data analytics is expanding, allowing for even greater potential applications. Telemedicine aims to improve productivity by allocating resources according to the most pressing needs while also making available a wider range of specialized knowledge and trained personnel [
8]. In this study, we will examine the significance of AI and its potential future application to the goals of telemedicine. Uses of AI in telehealth, patient monitoring, IT healthcare, and information analysis will be discussed in the article. Furthermore, the novelty of this review and its importance is as follows:
This study provides a comprehensive overview of the potential benefits and challenges of using AI in telehealth, which is lacking in many existing studies that focus on a specific aspect of AI or telehealth.
It emphasizes the importance of understanding the ethical, legal, and social implications of using AI in telehealth, which is a critical issue in the current healthcare landscape.
It discusses the potential of AI to improve patient outcomes and reduce healthcare costs, which aligns with the goals of many existing studies.
It highlights the potential of AI to address the issue of healthcare access, which is a major concern in many existing studies.
It discusses the potential of AI to enable personalized medicine and patient-centered care, which is an important topic in many existing studies.
It provides examples of AI applications in telehealth, such as decision support, diagnosis, monitoring, and personalized treatment, which is valuable information for researchers and practitioners.
It acknowledges the limitations of AI in telehealth, such as the need for high-quality data and the risk of bias and error, which is an important consideration in many existing studies.
It provides recommendations for future research, such as the need for rigorous evaluation of AI applications in telehealth and the importance of involving stakeholders in the design and implementation of AI systems, which is useful guidance for researchers and practitioners.
It emphasizes the need for interdisciplinary collaboration between healthcare providers, data scientists, and other stakeholders in the development of AI applications in telehealth, which aligns with the recommendations of many existing studies.
It contributes to the ongoing dialogue on the role of AI in telehealth and highlights the need for continued research and development in this area, which is an important contribution to the field of telehealth.
AI in telehealth can have a positive impact on sustainability in several ways.
Reduced carbon footprint: Telehealth eliminates the need for patients to travel to clinics or hospitals for routine appointments, which reduces the carbon footprint associated with transportation. By reducing the number of vehicles on the road, telehealth can help to reduce air pollution and greenhouse gas emissions.
Efficient use of resources: Telehealth can help healthcare providers to use resources more efficiently. For example, AI algorithms can help to predict which patients are at risk of developing certain conditions and enable providers to intervene early, potentially reducing the need for more costly interventions later on.
Better patient outcomes: By using AI to analyze patient data and provide personalized care plans, telehealth can help patients to manage chronic conditions more effectively and reduce the need for hospitalizations and emergency department visits.
Improved access to care: Telehealth can help to improve access to care for patients in rural or remote areas, who may not have easy access to healthcare facilities. This can help to reduce health disparities and ensure that everyone has access to quality care.
Overall, AI in telehealth has the potential to improve sustainability by reducing waste, improving efficiency, and improving patient outcomes. By leveraging technology to provide better care, we can create a more sustainable healthcare system that benefits both patients and the environment.
2. Research Methodology
To address the research questions driving this review, the systematic literature review (SLR) methodology was chosen because it makes it easier to develop trustworthy knowledge from a dispersed knowledge base and allows the researcher to map and assess the body of knowledge that is currently available. In fact, the SLR is a research approach that can synthesize the body of current information, identify gaps in the literature, and create new research objectives, all of which are aims of this study. The SLR identifies, selects, and critically assesses research to provide a solution to a well-stated issue. It adheres to a set of precise rules to conduct a thorough, repeatable, and transparent search for the most pertinent literature [
9]. In that regard, an SLR was carried out by adhering to the three-step method recommended by Tranfield et al. [
9] to respond to the research questions in this paper: planning, carrying out, reporting and disseminating the review are the first three steps.
2.1. Planning the Review and Database Search
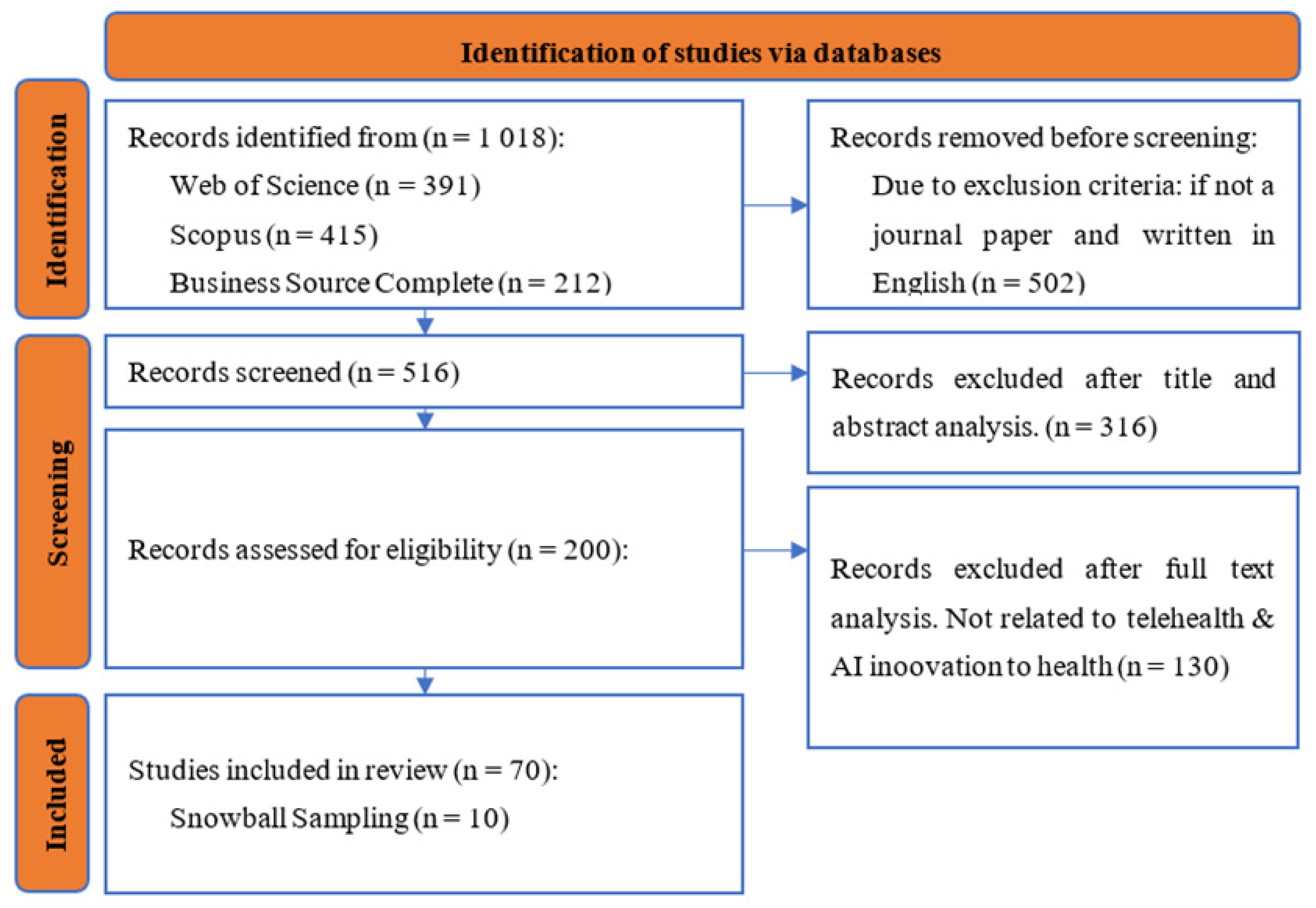
The first step of the SLR includes planning and searching for relevant articles using electronic databases. Therefore, the process began by identifying the relevant, peer-reviewed literature relating to the issue being investigated. The article selection process, shown in
Figure 1, followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A set of keywords to search the academic research databases was defined by the authors. Several keywords related to telehealth, artificial intelligence, and telemedicine were used to create different strings to search the databases and the final string the authors agreed upon was the following:
((“Health innovation” AND “Telehealth”) OR (“innovation in telehealth” AND “Artificial intelligence”) OR “health issues” OR “smart health” OR (“health management” AND “telehealth management”) OR (“innovation for health” AND “e-health”)).
The search was conducted in December of 2022 using three academic databases, viz., Scopus, Web of Science (WoS), and the Business Source Complete and Academic Search Complete collections in the EBSCO database. The search string was searched for in titles, keywords, and abstracts and the initial search encountered 1018 papers (391 in WoS, 415 in Scopus, 212 in Business Source Complete and Academic Search Complete).
Only peer-reviewed papers were considered in this research. Articles published in outlets such as conference proceedings, reviews, book chapters, etc., and articles not written in the English language were excluded. Duplicates were also eliminated, reducing the number for further analysis to 516. Next, a preliminary screening was performed by analyzing the papers’ titles and, if needed, their abstracts. Only 200 papers—all of which the authors unanimously agreed discussed the links between health innovation and telehealth—were chosen for full-text analysis. This includes 10 papers that were identified through the snowball sampling technique. The authors determined from the full-text analysis that 70 articles contributed to the topic and were pertinent to respond to the research questions guiding this paper. All papers were examined by the three authors to guarantee the validity of the selection procedure, and any disagreements were discussed until an agreement was achieved; only then were the articles chosen for full-text analysis.
2.2. Conducting the Review
In total, 116 articles chosen in the preliminary screening were examined to gauge the caliber of the sources and the applicability of the subject under investigation as well as their annual distribution. The journals were chosen from Scopus, Business Source Complete, and Web of Science for further article clarity based on the references. After screening the papers, a full-text analysis was performed on the 70 papers selected to enable the content analysis. The technique proposes a structured approach which enables the identification of the papers’ focus and the emerging patterns in the body of knowledge.
2.3. Reporting and Disseminating the Review
To enable the content analysis, the articles’ basic information was translated into an Excel file, according to an initial codebook developed by the authors, which was adjusted and updated during the full-text analysis to incorporate new categories, until no new categories emerged. The authors first coded all the selected articles and subsequently compared and discussed the results for each article to resolve any discrepancies in coding
Table 1. Themes found inductively during the literature review process could be examined through full-text analysis of the literature.
3. Telehealth in Healthcare
Through electronic means of communication, telehealth facilitates the transmission of health-related data that may then be used to provide direct patient care, as well as patient education and training. It aims to make healthcare more accessible and affordable in developed and developing countries by removing barriers such as time, distance, and geography. It plays an important part in times of crisis, such as natural disasters. Lengthier life expectancy and the accompanying rise in the prevalence of chronic illnesses have increased both the need for and complexity of treatment, resulting in longer contacts between patients and clinicians (and across providers) and, therefore, a greater need for telehealth care assistance.
In the past, telehealth was divided into two distinct types: synchronous, where the patient and doctor are in constant contact, and asynchronous, where messages are stored and sent at a later time. Telemonitoring, the third kind, has recently been recognized; it entails gathering information from dispersed devices, such as those connected to the Internet of Things (IoT). Four examples of well-embedded telehealth services were identified in the most recent WHO global eHealth observatory survey: teleradiology, telepathology, teledermatology, and telepsychiatry. The first three use asynchronous models of care, while the fourth uses a synchronous model. This exemplifies the inherent challenge of substituting or supplementing services supplied in real time by clinicians. More than 60% of respondents to the same poll also cited a lack of knowledge of clinical practice connected to telehealth as a major barrier to widespread adoption [
10].
Telemedicine is the remote delivery of medical treatment via electronic medical records, videoconferencing, and other information and communication technologies. A physician’s provision of remote medical care is known as telemedicine, but telehealth incorporates a broader range of non-physician services.
It is common practice to employ telemedicine to manage long-term conditions such as cardiovascular disease, diabetes mellitus, cancer, and mental illness. In certain cases, such as with elderly patients, telemedicine may be a viable, cost-effective option. Patients, particularly those in remote places, may easily keep tabs on their care with mHealth applications.
One of the most promising uses of telehealth is in the field of digital psychotherapy. It facilitates constant two-way communication between patients and their psychiatrists. Telepsychiatry may save money compared to traditional therapy sessions. To make up for the absence of psychiatrists and other mental health specialists in the country’s outlying regions, digital psychotherapy has emerged as a means for individuals to connect with their metropolitan providers. Patients may find that mobile applications are a more convenient and cost-effective option than telepsychiatry. Smartphones may provide home care for those with mental diseases such as depression, anxiety, schizophrenia, and more. Across the globe, cancer is the biggest killer. Most people with cancer need to be monitored consistently to keep their condition under control.
For cancer patients, telehealth has made it easier to receive palliative care at home. With the help of mobile applications, patients can communicate with their doctors and loved ones and access the necessary resources for providing quality care. This seamless communication allows for timely support, enhancing patient care and improving the quality of life during long-term treatment processes. Telehealth plays an essential role in enhancing patient care by providing timely resources and support, even when patients are receiving treatment from the comfort of their homes. It is a cost-effective and convenient alternative for managing long-term conditions and providing access to mental health specialists in remote regions. With the rapid advancement in communication technologies, telehealth will undoubtedly continue to revolutionize the delivery of medical treatment in the future [
11].
4. Why Artificial Intelligence Is Necessary
Artificial intelligence has been studied for decades. Artificial intelligence technology could be used in several ways:
To improve medical care;
To enhance procedures through incorporating digital intelligence into medical equipment and instruments or;
To provide a means of assessing patient records to identify error-causing factors;
To propose new treatments in light of existing ones.
The ability to spot patterns quickly and with planned accuracy helps find the best medical practices and judgments. The ability to enhance surgical procedures and foresee problems depends on identifying patterns in the outcomes of these procedures. More and more hospitals are using such tools to maximize the impact of their available resources [
12].
5. Concept of Artificial Intelligence
AI popularized the term “artificial intelligence” (AI) in the 1950s [
13]. Artificial intelligence, or AI, is the capacity of computers to simulate human intelligence by acting and reacting to events in a predictable manner. Developers and scientists have been working to enhance AI-based algorithms ever since the late 1990s when network and technological infrastructures began to mature. Functionality and technical considerations led to the categorization of AI into seven distinct varieties. Machine learning and deep learning are two branches of artificial intelligence [
14]. Artificial intelligence (AI) describes computer programs that can learn and improve their performance over time. Artificial neural networks are used in deep learning to think like human brains. Machine learning uses methods to learn based on the previous experiments and to make judgments [
15] (
Table 2).
Artificial intelligence (AI) has become a valuable resource in many industries today. The following are the uses of AI in different industries [
23]:
Online and personalized shopping (E-commerce);
Navigation (traffic prediction and GPS technology);
Robotics (artificial intelligence-based robots);
Healthcare (disease diagnose and cure);
Agriculture (identification of soil defects and nutrients);
Gaming (prediction of human behavior, human–computer interaction);
Facial recognition.
Disease hotspots were located, and their geographical patterns were evaluated using artificial geospatial intelligence (GeoAI). It was utilized for modelling and tracking disease outbreaks in infectious disease research. An artificial neural network-specific algorithm was used to geotag tweets from Twitter and statistics on CDC cases of influenza-like sickness to provide real-time disease predictions. These geotagged tweets centered on the location from when the tweet was sent and enabled the Twitter App to track the tweet’s movement. Another research employed a machine learning strategy to forecast seasonal influenza epidemiology in the United States [
21,
22,
23].
Different initiatives are starting to use location-based information and GeoAI for treatment and other healthcare applications. Expanding existing GeoAI technology will allow for new avenues of study in spatial epidemiology and public health, such as modelling places that still need to be recorded in high resolution or analytics to produce new geographically vast data sources [
24].
Artificial Intelligence in Telehealth
Artificial intelligence (AI) has been rapidly expanding into the healthcare industry, and telehealth is no exception. Telehealth refers to the use of technology to deliver remote healthcare services, including diagnosis, treatment, and monitoring. AI technology can assist telehealth in several ways, such as improving diagnostic accuracy, enhancing patient outcomes, and increasing the efficiency of healthcare delivery [
25].
One significant benefit of AI in telehealth is the ability to process large amounts of data quickly and accurately. AI algorithms can sift through medical records, lab results, and patient-generated data to identify patterns and make predictions about a patient’s health status. This information can help healthcare providers make more informed decisions about patient care and treatment plans, leading to better outcomes [
26].
Another important application of AI in telehealth is in the development of chatbots and virtual assistants. Chatbots and virtual assistants can help patients access healthcare resources and provide basic medical advice. These tools can also help healthcare providers manage their workflows, such as scheduling appointments and reminding patients to take their medication [
27].
AI can also be used in telehealth for remote monitoring and early detection of health problems. Wearable devices and sensors can collect patient data and send them to AI algorithms for analysis. These algorithms can detect changes in a patient’s health status and alert healthcare providers if action is necessary, allowing for early intervention and improved patient outcomes. AI can also assist in reducing healthcare costs by automating routine tasks and improving the efficiency of healthcare delivery. For example, AI algorithms can help optimize staffing levels and improve patient flow, leading to reduced wait times and shorter hospital stays [
28].
In recent years, the use of artificial intelligence (AI) in healthcare and telehealth has been steadily increasing. One area of development is the use of computer-generated conversation to facilitate communication between patients and healthcare providers. This technology can provide a range of benefits, from enabling remote therapy sessions to automating simple healthcare tasks. The potential uses of automated conversational interactions are vast and can range from simple message delivery to more complex interactions. For basic tasks, such as providing reminders or confirming appointments, simple audio or visual cues may be sufficient. These types of interactions can be managed by rule-based systems, which rely on pre-defined decision trees or expert systems to construct responses to user inputs [
29].
However, more complex interactions require a higher level of AI sophistication. These may include virtual assistants capable of responding to questions, providing health advice, or even performing basic diagnosis. For example, virtual assistants could provide assistance to individuals with cognitive impairments or offer avatar-based support to elderly patients. To facilitate these types of interactions, AI models must be capable of understanding the context of the conversation and adapting to the user’s needs [
30].
In healthcare, the potential for AI-assisted virtual assistants is significant. They can provide healthcare professionals with a cost-effective and scalable solution for patient care, helping to reduce the burden on overworked healthcare systems [
31]. Furthermore, the use of AI can help to improve patient outcomes by providing personalized, real-time advice and support. As the technology continues to evolve, we can expect to see an increasing number of healthcare applications that leverage AI to improve patient care and outcomes [
32].
Dealing with cognitively impaired individuals, making online clinical information more accessible, and providing avatar-based patient agents are just a few examples of health applications where virtual assistants can provide a viable supplement or alternative to conventional healthcare delivery models [
33]. In these situations, the conversational goal and knowledge base need to be increasingly complicated, and the complexity of the AI agent increases as it learns more from the data it collects. To have a genuine discussion, it may be important to include emotive behavior via multimodal contextual awareness processes [
34]. For instance, a personalized model of the individual’s context will be required in addition to the context model for the present discussion if difficulties emerging from the patient’s prior interactions or past medical history need to be addressed in making conversational judgments [
35].
According to [
36], that looked at the most recent developments in the field of telehealth, two major forces are driving change: high volume demand, which is occurring because it is becoming increasingly difficult to co-locate the patient physically, the clinicians, and the associated data; and high criticality applications, which are situations in which specialized expertise is required at the precise moment that clinical demand arises. The provision of medical treatment will always include at least one face-to-face clinical encounter, the needed frequency of which will vary depending on the case’s specifics [
37]. This is true regardless of the mode of delivery that is chosen. In the telehealth field, information and communication technology (ICT) applications may be used to find solutions to problems caused by an imbalance between the demand for and supply of medical services. AI could help with this problem by building algorithms that match the number of care providers who have the relevant clinical abilities to the number of people who need those skill sets in the nearby area [
38]. Telehealth does, however, provide several operational challenges, such as when the connection to the remote communications system breaks or when the physician providing remote treatment is not accessible remotely. AI can eliminate various issues in healthcare departments. Interaction between humans and computers can be increased by using artificial intelligence to provide better situations and solve problems [
39,
40,
41].
Medical care is becoming more complex due to the steady stream of discoveries and advancements, so a single clinician can no longer handle it. By tailoring care to the unique needs of each patient or patient cohort, AI can facilitate the development of expertise in clinical procedures. Artificial intelligence (AI) may be used, for instance, to learn how to use recent medical care advances best. To extend life expectancy and effectively treat chronic illnesses that include numerous ailments, a team approach comprising specialists from many fields is essential. Care must be provided at the patient’s own home or another location within the community [
42]. Inadequate adherence to integrated care pathways and care continuums has a detrimental effect on healthcare access and quality for all patients. Support or remote care is required due to the inability of all team members to be physically present at all times. There should be consistent communication and connections between the various parts of the healthcare delivery system. Artificial intelligence (AI) might assist in meeting this demand by creating a smart information and communication environment in which practitioners could collaborate and by keeping a comprehensive virtual knowledge base throughout a patient’s illness and therapy [
43].
As [
44] elaborated, artificial intelligence encompasses “problem-solving and search, logic and inference, planning, probabilistic reasoning and decision making, learning, communication, vision, and robotics.” They also theorized that computers may act as “intelligent agents” in the field of AI and that these machines would be able to replicate human cognitive behavior and cognitive performance to the point that they would be able to outperform humans in these areas. The reasoning behind this was the assumption that computers might execute mental tasks in a human-like manner and have human-like cognitive abilities. In a recent article, ref. [
45] summarized the possible influence of AI in telemedicine based on four developing themes serving different healthcare goals. A few examples of these tendencies include:
- 1.
The expansion of healthcare IT to remote patient monitoring.
- 2.
The use of AI in medical diagnosis and support.
- 3.
The growing emphasis on teamwork in data analysis.
This is a reasonable approach to summarize the possible effects of AI on telehealth, given the breadth of those effects. They may be merged into two main foci, both of which will become topics of discussion in the next sections of this study. First, bolstering high standards for established clinical practice and service delivery, and second, developing and bolstering experimental approaches to patient care.
6. Artificial Intelligence, Telehealth, and Quality Improvement
There has been an explosion in the volume of health-related data generated digitally by patients and medical professionals in the last few years. As a result, there has been a push for the general use of EHRs (electronic health record systems) and the automated collection of patients’ data. The availability of huge datasets and the rapid development of computational data science allow for the extraction of innovative findings and actionable insights with the potential to significantly improve health outcomes (including AI-based machine learning approaches). As a result of the increased sophistication of the data available, clinical decision-making may be supported by automated methods, which in turn encourages progress toward intelligent aid and diagnosis [
45].
6.1. Clinical Assessment and Evaluation
Clinical assessment used to rely heavily on a patient’s history, and a physical exam before sophisticated diagnostic tools and imaging technologies such as MRI and CT were widely available. The authors of [
46] found that a patient’s medical history accounted for 76% of the diagnostic process, whereas a physical exam only accounted for 11%. The researchers discovered that the significance of the history was about the same, while the importance of the examination was considerably lower (7.6%). Healthcare is deteriorating due to the declining skill in taking and analyzing patient histories in the present day [
47].
Investigations simplify telecare because of the convenience of collecting and transmitting data in this way. Computed tomography, magnetic resonance imaging (MRI), and ultrasound (gallstone, liver abscess) have helped in the diagnosis and enhanced the importance of computed diagnosis. The expenses associated with this level of complexity have yet to be justified by the quality gains seen in healthcare delivery. Because it is time-consuming and tedious for doctors to take a patient’s history, telemedicine is only sometimes utilized to its full potential. It is a pity since it is a step that can be accomplished remotely and does not call for any specialized tools. However, the cost–benefit advantage of telecare is diminished when conducting high-end examinations due to the need for more expensive distant infrastructure.
A patient’s medical history might provide important insights for a seasoned doctor trying to diagnose their condition. It helps with the diagnosis, of course, but it also helps narrow down the scope of the study. Artificial intelligence (AI) has the potential to streamline the history-taking process by giving suggestions, diagnostic clues, and the right follow-up questions depending on the clinician’s response. Someone with gastritis, for instance, may have long-term, dull aching discomfort in the upper abdomen without disrupting sleep. Effective use of mobile ICT may allow for the delivery of a summary of such queries asked in succession as part of a telehealth application.
For instance, if a patient is experiencing chest discomfort and the risk of myocardial infarction, streptokinase or at least Sorbitrate or aspirin should be urgently considered for remote administration even if a doctor cannot be reached. With the help of a local nurse practitioner, the patient may immediately benefit from these inquiries and their findings. The user interface may be made more accessible for such questions by using universally understood icons.
6.2. Telediagnosis of Clinical Conditions
Because of advancements in telemedicine, off-site medical diagnosis is now a real possibility. Medical professionals may now diagnose and treat patients remotely. Patients with diabetic retinopathy, for instance, have seen fewer doctor’s appointments. Artificial intelligence (AI) in screening procedures is expected to reduce visits even more. If an AI system is included in the screening method, the algorithm will require only retinal images. The AI system can analyze the photos and precisely assess the disease’s severity by comparing them to historical data. Doctors and patients would benefit greatly from using AI in the screening process since it will reduce the amount of time and effort required. Because of the ease of identification enabled by AI in telemedicine, doctors and patients may expect the diagnosis to become more efficient, saving both time and money [
48].
In the past, doctors relied on clinical examinations to make diagnoses. Still, nowadays, patients and doctors rely on a combination of objective evidence and the doctor’s expert interpretation of that data. In this context, AI has emerged to greatly assist medical professionals in evaluating evidence in recent years. Considering the progression of illnesses related to the creation of malignancies, various disease diagnostic patterns may represent varied cancer risk profiles. This is especially important in oncology. The prediction may be improved by simulating illness development and possible course changes. AI is on track to significantly affect illness diagnosis worldwide by using machine learning algorithms to enormous databases of disease populations [
49].
Teledermatology is an established branch of telediagnostics that may benefit greatly from AI-powered automation. The current state of melanoma diagnosis relies on the expertise and training of the examining physician. It was recently discovered that a computer program that used convolutional neural networks was more accurate in detecting melanoma than most of the 58 dermatologists who were also assessed (median area under the receiver operating characteristic curve 0.86 vs. 0.79, P 0.01). Another study classified skin lesions using deep convolutional neural networks (CNNs). These CNNs relied only on pixel-level image data and disease labels during training. By using CNNs, we can show that AI is capable of skin cancer classification at a level of expertise on par with that of dermatologists. For example, screening for breast and cervical cancer might benefit greatly from automated diagnosis [
7,
50].
7. Artificial Intelligence, Telehealth, and Models of Care
There has been a notable rise in the prevalence of chronic illnesses throughout the world. The traditional methods of healthcare delivery are overstressed to the point that they are no longer viable. This is compounded by the fact that the base of aging people with numerous morbidities is expanding. Telehealth is a viable option that may maximize the use of information and communication technology for diagnosing, monitoring, and delivering healthcare at a distance. However, the full promise of delivering healthcare across long distances has yet to be realized because of several system-level restrictions that have precluded the scaling up of revolutionary telehealth models at the national or regional levels. Recent studies on telehealth interventions have found that to successfully implement a complex innovation, such as remote care, it needs to be allowed to develop naturally, respond to and adapt to the local health and social care system, and be pushed forward with the backing of front-line staff and management. Consequently, the improved healthcare opportunities afforded by patient monitoring must be implemented in an environment that places a premium on information analysis and communication between care teams and organizations accountable for health systems.
7.1. Conversational Agents and Virtual Assistants
Computer-to-human engagement in telehealth is a logical extension of human-to-human communication. This expansion is made possible by advances in computer-based dialogue production and interpretation. The benefits of choosing between a human counsellor or a computer have been well recognized for some time. Recent years have shown the benefits of synchronous and task-oriented computer-generated discourse for various applications, including those dealing with mental health. There are several applications throughout the care continuum where automated conversational interactions may supplement or even replace human carer duties [
51].
Virtual assistant (or conversational agent) solutions may range widely in scope and sophistication. Audio speech or visual text communication is typically sufficient for basic activities, which need nothing more than a message or signal to alert the receiver. It may also transmit a low complexity response, such as a confirmation acknowledgement. Chatbots that can take voice or textual inputs and respond in kind are one such technology. They may be programmed with restricted dialogue systems that can understand and generate just a small subset of sentences for a certain task. Solutions such as this work best when both the circumstance and the user’s context are well established and straightforward. Expert systems and decision trees are common rule-based AI methods used by these agents [
48,
52].
Ref. [
53] state that a chatbot is “a system that aims to imitate dialogue rather than comprehend it.” Chatbots may answer customer service questions, provide instructions, or perform searches. In the corporate world, they are used as virtual assistants or as the initial point of contact. The first successful chatbot, ELIZA, successfully engaged in natural-sounding conversations with humans. It worked by paraphrasing phrases as input when they conformed to a set of rules. Vocal recognition is another developing tool. These advancements in technology allow for the provision of a service available around the clock to assist patients and their caretakers. There is also the possibility of a hybrid technology in which chatbots and people work together to provide patient care.
Health applications where virtual assistants may be a useful addition to or replacement for conventional healthcare providers include helping people with cognitive impairments and increasing access to online clinical information. In these cases, it is crucial to have a deeper conversational purpose and knowledge base, and the complexity of AI grows as the AI agent learns more about its surroundings. Using multimodal contextual awareness techniques, including elements of emotional behavior, may be necessary to promote a genuine conversational dialogue.
7.2. Remote Patient Monitoring and Management
The complete patient monitoring system works in a managed way. Data are collected from patients by using a sensor. Data are then transmitted to the clinics and combined with other data. The combination of previous and current data is used to make proper actions such as the escalated care of the patient. Telemonitoring AI systems are dependent on and contribute to the growth of other ICT parts of the healthcare system. In certain situations, they may even be superior to humans. They reliably and mathematically carry out their commands, mostly based on internal logic but also factoring in statistical evidence acquired through machine learning techniques from massive datasets. Data from other devices, such as global positioning systems (GPS), accelerometers, motion sensors, gyroscopes, etc., may be instantly integrated and coordinated. Humans would require education and training to incorporate these new data into care delivery, which is time-consuming.
Studies on patients with chronic diseases, including diabetes, COPD, and heart failure, have tested the viability of telemonitoring as a means of remote surveillance. There have been improvements in both the therapy and monitoring of COPD thanks to AI methods. Classification and Regression Tree algorithm has been used in the research to diagnose a patient. Data are taken from telehealth measurements at home and them used to early diagnose a disease. Algorithms and procedures are very useful to diagnose disease at early stages. In addition to the measures described above that are focused on deterioration, the management of recovery conditions provides another option for patient monitoring through telehealth. For instance, software that measures the extent of wounds may be used as a complement to visual evaluation, which can improve performance and help with remote treatment. In this particular illustration, a specialized scale that computers can read is made available, and automated image-processing techniques are used to modify the contrast of the picture to facilitate the accurate sizing and automatic determination of the border and area dimensions. Human supervision and correction are currently required, and this may continue to be the case for a significant portion of AI-based telemonitoring, at least in the short-term [
54].
Artificial intelligence has made it possible to simulate face-to-face interactions between medical professionals and their patients while also allowing for remote patient health monitoring. There has been a recent uptick in interest in using artificial intelligence in telehealth settings. The automated decision-making solution based on AI is available for use by general practitioners and experts. The most general applications of artificial intelligence in telehealth include the following:
Data analysis and cooperation.
Remote patient monitoring.
Intelligent diagnosis and assistance.
Competent support.
AI could be utilized to aid physicians in diagnosing and treating patients, as well as to prevent professional burnout and enhance the overall patient experience. These applications could also be used to improve the overall patient experience.
Because public health problems are not going away, executives in the healthcare industry are increasingly focusing on artificial intelligence (AI) and telehealth. Artificial intelligence has been of great use in monitoring customers’ welfare in the comfort of their homes.
8. Trends of Artificial Intelligence in Telehealth
8.1. Patient Monitoring
Telemedicine has been used for various purposes, one of the oldest and most common being the distant observation of patients. This paves the way for a less expensive and more efficient way to have regular doctor-to-patient consultations via the phone or internet to assess the current health of the patient and the clinical results. This has been designed to work similarly to an in-person consultation via video conferencing and the attachment of digital medical equipment to gather and record the patient’s clinical data. This development aims to enhance the practicability, efficiency, cost-effectiveness, and ease of use of patient monitoring compared to the standard approach.
Recent telepresence robot designs prioritize autonomy, allowing them to find their way through doors and rooms without human input. This is achieved using a software interface that permits remote control of the robot through a Wi-Fi connection between the user and the robot. This concept has recently expanded thanks to the integration of AI and vision systems for mapping environments and spotting hazards. Dr Rho, Medical Telepresence Robot, is an example; it features a screen and a mobile body to improve patient–doctor communication. Its microprojector and intuitive visual system facilitate collaborative examinations and surgeries. When AI is put into practice, the concept of machine learning will work well with it. The sensors on board will allow for simultaneous mapping and interior navigation, allowing the software to plot a course for the robot based on the user’s input of simply its final destination. A similar system might be used to customize the robot’s physical configuration for the patient’s benefit. Modifying the monitor’s or camera’s viewing angle and height may be necessary.
The research on an ankle rehabilitation system using feedback from a smartphone wireless gyroscope platform and machine learning classification exemplifies the use of AI and telemedicine to track a patient’s recovery without the need for live video or in-person consulting. Therefore, the sick person has greater privacy. This research proposes employing a gadget consisting of a wireless gyroscope platform on a 3D-printed frame linked by way of a smartphone to keep track of the numerous beneficial consequences of the ankle treatment and to “evaluate the success of the rehabilitation plan” using a machine learning algorithm. Therefore, it is shown that vital wireless sensors play an important role in telemedicine. Given the rapidity with which information may be sent to devices, robust wireless sensors are crucial for 24/7 monitoring. If you are looking for a more effective and real-time method of gathering information from patients with sickle cell disease, a web-based management system that makes use of machine learning methodologies is one option. The system’s artificial intelligence component allows for accurate dosing predictions based on historical data [
55]. The system’s primary function is management, including but not limited to patient housing and monitoring. The recent improvements in patient monitoring have led to a rise in the use of self-diagnosis techniques and telemedicine in hospitals and people’s homes. The increasing storage capacity necessitates the development of uniform data architectures across all devices. Most non-hospital applications of patient monitoring equipment and technologies focus on the care of the elderly and those with long-term diseases.
8.2. Healthcare Information Technology
In hospitals, data are captured not via manual registration but through self-diagnosing technology; it will be difficult to maintain such a huge record. This is because of the large size of the data. In addition, given that the purpose of telemedicine is to link medical experts and patients from different parts of the globe, it is necessary to develop a universal record system that can be used by all institutions participating in the practice.
The up-and-coming technology uses big data analytics in conjunction with neural networks to efficiently maintain and retrieve electronic medical information. The current trend of using AI in the process of systematizing the retrieval and analysis of data offers a solution to the challenges presented by medical operations. As a result of research indicating that physicians spend fifty per cent of their time on electronic health records and desk work, Remedy was developed. This technology streamlines the patient intake procedure by substituting the traditional method of taking a patient’s vitals with a chat-based questionnaire, storing the data, and alerting the attending physician. The patient and medical personnel can communicate more effectively thanks to this method. Because of this, it is now possible to immediately deliver prescriptions and other information to the patient, who may even provide images or videos for assessment. This makes the process much quicker [
56].
The use of cloud computing as a solution to problems with electronic infrastructure, such as the limited bandwidth available in certain regions and the complexity of the installation process, is another trend in the development of patient monitoring. By using the services in data centers and utilizing distant servers to store and handle the information, this innovation intends to make gathering and disseminating patient information more efficient. This concept has been used in a research project titled “A Cloud Computing Based Telemedicine Service” to increase the rate at which medical assessments are performed through the transmission of ECG wave signals to a diverse number of locations, including a mobile phone, by way of the cloud. The “traditional healthcare information system architecture and developing eHealth consumer electronics technology” may be linked via cloud computing, which is another use of this technology. The use of cloud computing in this situation will result in an improved capacity for transactional processing and enhanced speed when retrieving data. Not only will this be important for data processing and collaboration, but it will also be important for the widespread application of an automated system in facilities throughout the region. This can be a step toward standardizing medical information and records throughout areas, and it can be a step in the right direction. Because of this, the processes involved in telemedicine will be completed more quickly, and the new programs will be implemented more consistently [
57].
Since telemedicine relies on wireless connections and the constant transfer of patient information, there was a potential risk to patient privacy and confidentiality. This was one of several factors making some medical facilities wary about telemedicine. There remains more to be achieved in the field of data security utilizing wavelet-based watermarking, despite the fact that various studies using image processing and AI have offered techniques for doing so. The results of this study, which was conducted in India, suggest using an algorithm for the digital watermarking of medical pictures to safeguard patient confidentiality. Incorporating authentication and evaluating the demonstration of the device’s capabilities into device-to-device interactions make for a secure mode of transmission.
Even though telemedicine has the potential to reduce the number of in-person hospital visits, these trips are nevertheless often required. When faced with such circumstances, AI can aid in lowering the time patients are required to wait before being seen and in ensuring that patients are treated as quickly as feasible. The artificial intelligence system provides members of staff with up-to-date information on the influx of patients visiting the hospital, high-priority cases, the need for more beds, and other aspects of patient care. As a direct result of the initiative, the medical facility’s ability to treat patients with complex medical conditions has increased by around sixty per cent. In addition, the effectiveness of ambulance services has increased, which has resulted in ambulances being sent one hour sooner. Patients in the emergency department may also be given a bed up to thirty per cent quicker in certain places thanks to artificial intelligence and predictive analytics. As telemedicine and telehealth gain in popularity, the role of artificial intelligence (AI) in the industry will grow significantly. Healthcare workers will benefit greatly from incorporating AI into telehealth applications. Decreasing patient wait times, advising on the best treatment options, and, most importantly, making healthcare available 24 h a day, 7 days a week will help cut costs, deliver better healthcare to people, and enhance the work environment. Better healthcare for the public is another benefit.
8.3. Intelligent Assistance
Healthcare delivery through telemedicine is another area where AI is being used. Healthcare, including medical treatment, may now be provided to patients over great distances because of advancements in telemedicine. Patients in rural locations or those with mobility issues may benefit from this care delivery. Artificial intelligence (AI) is being utilized in telemedicine, for instance, to provide doctors with instantaneous feedback. Machine learning algorithms are used to examine patient data and draw conclusions that may be used to enhance medical treatment. Teladoc is a service that connects patients with physicians via video conferencing and utilizes machine learning to provide clinicians with immediate feedback during in-person appointments. Automatic reminders are another way that AI is being utilized in telemedicine. Machine learning techniques are used to examine patient records to achieve this goal.
The incorporation of mechanical aids and the intelligent use of medical data and findings are two major current trends in robotic technology. Both aspects are designed to benefit the present healthcare system by helping patients in some way, either physically or through studying the initial medical assessment. Neural networks and machine learning may be used algorithmically to make these instruments functional. Because of this, the technology may learn from its inputs and improve over time. Self-diagnosis technologies in telehealth are already under development, with a variety of software and smartphone apps on the horizon [
58].
As is typical for the industry, self-diagnosing software and gadgets have emerged for rapid assessments of vital signs, including pulse, heart rate, and respiration. For example, a new firm, named Lemonaid Health, has created an AI model for screening and evaluating patients based on their responses to a questionnaire and their satisfaction with a few conditions. After the initial evaluation, the patient will be assigned to a certain group. After determining the best course of action, doctors may provide telephone consultations or arrange for direct prescription delivery, depending on the circumstances. Carbon Health has also designed a chatbot-based triage evaluation method. A consultation will be scheduled if necessary. The program will keep an eye on medication compliance and the emergence of new symptoms [
59].
Wireless telemedicine applications may also be used in emergency circumstances, such as when an ambulance has to share its patient’s medical records with a hospital or clinic nearby to work together to provide the patient with prompt, high-quality treatment [
59] (
Figure 2).
9. Role of Healthcare 4.0 in Telemedicine
Healthcare 4.0, often known as the fourth healthcare revolution, is the actualization of the idea of speeding up medical innovation while simultaneously enhancing the effectiveness of patient care. Healthcare 4.0 describes the recent advancements in medicine made possible by automation, management, and data processing [
60]. The term “healthcare 4.0” refers to the increased integration of cyber and physical components and the connectivity solutions made possible by cutting-edge information and communication technologies such as big data, the Internet of Things (IoT), and cloud computing. The healthcare 4.0 systems combine these technologies and promise to provide truly individualized healthcare to patients, doctors, and carers in real time. There has been a rise in interest in using engineering methods to deliver healthcare services throughout the globe in the aftermath of significant developments in medical equipment, clinical advancements, and data analytics. These technological advances have presented enormous opportunities and severe challenges to the healthcare industry [
61].
Specifically, healthcare 4.0 facilitates the shift from a hospital-centered to a patient-centered system, whereby many departments, roles, and duties are combined to provide the best possible healthcare results for individual patients. Healthcare 4.0 improves upon the capabilities of the conventional medical system, which in turn aids in strategizing support for the distant provision of high-quality treatment. Healthcare 4.0 aspires to improve the quality of care provided to patients and health promotion, cost management, and clinician happiness. Accessing data from anywhere is a crucial feature of this approach, which also involves deploying computing power for data management. Those parts of our society that have begun to embrace these technological breakthroughs stand to benefit significantly from these dramatic shifts [
62].
Some healthcare 4.0-promoting innovations are given in the
Table 3.
Open Innovation in Telehealth
One industry that may gain from open innovation is healthcare. Around 12.8 percent of the world’s economy is devoted to healthcare, making it one of the largest users of human information systems in the service of problem-solving. When applied to the healthcare industry, open innovation can boost the quality and quantity of ideas, help solve problems more quickly, save money, reduce risk, motivate workers, encourage new perspectives, and boost a company’s reputation. The delivery of both online and in-person medical care is one area that could use some help from the open innovation movement. Ninety percent of healthcare executives have developed or implemented a telehealth program within their organization as a result of the COVID-19 pandemic. As the COVID-19 pandemic subsides, however, a hybrid in-person/remote model of telehealth visits may emerge [
65].
10. Discussion: Issues and Considerations
AI has a lot of promise for expanding access to healthcare via telehealth solutions, but we must think about the social and ethical repercussions before we accept it. AI and other technology breakthroughs in the healthcare industry will change many facets of healthcare delivery, including processes, communication, access to medicines, and relationships between physicians and patients. Instead of focusing on developing cutting-edge AI tools and algorithms, we should be developing means of incorporating AI into daily life, since this is where the “last mile” issue most often originates. This implementation is the “last mile” of any project. Medical informaticians have been looking at HIT-related UICs for a while now. These UICs occur not necessarily as a result of negligence on the side of system designers, but rather as a result of our failure to anticipate the emergence of novel forms of connection and communication as a result of the widespread use of HIT. Optimism and hope for the future of AI-enabled telehealth will inevitably peak, followed by disappointment and fear as the field matures. Rapid progress toward peace should be our top priority. This essay will highlight four important social and ethical considerations that should be made before deploying telemedicine assisted by artificial intelligence.
While telemedicine has the potential to improve healthcare in many ways, it also comes with certain risks. Dismantling the wall between doctors and their patients, examining how doctors talk to one another, addressing worries about the quality of health data, and overcoming organizational and legal barriers are all essential to the successful implementation of telemedicine.
There has been a rise in interest in mobile devices, cloud computing, internet networking, and wearable technology among academics, businesspeople, and consumers. Academics and professionals in the healthcare industry are now functioning in a digital ecosystem. This ecosystem consists of technologies that are simple to install, have a loose coupling between them, and provide effective care delivery and monitoring capabilities. Nevertheless, there are many obstacles to overcome to protect the privacy of persons and the confidentiality of their information.
Concerns have been expressed about the ethical and contextual implications of data sharing, particularly the absence of uniform privacy standards. Methods for enhancing health data sharing and linking, as well as a consensus on data governance, are urgently required. The European Union’s General Data Protection Regulation is one example of a comprehensive piece of law that has started to address this issue, but additional tailored solutions, such as the voluntary privacy regulation for mobile health apps, are needed. Recent ethical studies have also shown that users need to consider the full scope of their results before acting.
Lack of control, suboptimal benefits for information producers or administrators, unfair advantages resulting from a more advanced technological background, and technical questions related to data consistency, interoperability, and misinterpretation risks are just a few of the difficulties that plague Africa’s data exchange. It is generally accepted that most of the technical issues have been handled. In regions such as Africa, where there is a possibility that data exchange needs to be maximized, there needs to be more documentation of problems relating to worry, danger, and insecurity. Ethical issues are also acknowledged or dealt with less often in these nations.
Sometimes there are gaps in the official data-sharing norms, and others could be more precise and consistent. There is only sometimes a good control or definition of the balance that should exist between making data available, protecting individuals’ right to privacy, and safeguarding the intellectual, time, and monetary contributions made by public health staff.
Advocates for public health research will not stop pushing for change and developing mechanisms for data sharing. However, the obstacles responsible for the lack of data sharing have yet to be sufficiently examined. Lack of financing, employment routes that underestimate the importance of crucial data-processing skills, and systems that promote research are considered. In addition, certain logistical issues need to be answered, such as:
How and where may long-term data be stored?
Where may data be stored?
Who will regulate access?
Who will pay for these services?
The rules now in place for metadata need to be relaxed to make health information more readily available.
The expense involved in putting telemedicine programs and equipment into action is one of the most significant obstacles in the way. It is inevitable that healthcare institutions, such as hospitals, would have to invest in installing and training new technology, despite efforts to develop more cost-effective cost models. Moreover, there is an issue with the availability or speed of the connection, which hinders efforts to build a system for the rapid and dependable transmission of high-quality telemedicine data. Changes to the infrastructure may be required, which may be challenging in any setting, but especially in remote or poorly equipped areas. There is a lot of potential for future directions of artificial intelligence in healthcare information because there are concerns about protecting the secrecy and security of telemedicine consultations and operations. Under the subject of healthcare IT, it was mentioned that there is still a security and privacy risk. Studies that intend to solve this issue have yet to be thoroughly polished, and it may still take some time before their use in real telemedicine technology. The risk of malpractice, which occurs with other medical procedures and equipment, is another concern. This risk has led to the mandated need for training and licensing to use telemedicine devices correctly. Because of the increased cost and length of time required, this may discourage facilities from putting the plan into action. Patients’ consistency and preferences might be negatively impacted by unprofessional medical care and a lack of understanding, which can result in disdain for the use of or advancement in technology.
While AI and other forms of technology may improve access to and delivery of services, it also has the potential to widen the gap between those who have and those who do not. People who live in rural and distant locations and underdeveloped nations are some of the populations who benefit the most from implementing healthcare delivery systems enabled by technological advances. There are many different kinds of people in the world. While some cultures have mastered the art of using technology, others have yet to do so. Those who are expected to reap the most benefits from telehealth innovations, such as the elderly and the gravely ill, may not be as tech savvy as others. In order to ensure that all of our citizens have access to high-quality, patient-centered care, it is our responsibility to ensure that the use of artificial intelligence does not further the digital divide. There is an old adage that “health information technology adoption is a journey, not a destination,” but as healthcare continues to be digitized at unprecedented speeds, this is truer than ever before. We have no choice but to accept the idea of AI if we want to create a healthcare system capable of continuous improvement. However, we must take a practical approach to develop and distribute AI-enhanced instruments. People are the first and foremost consideration when providing medical treatment. AI technologies will revolutionize the way interactions take place between various actors in the healthcare system. We need to ensure that these tools’ primary emphasis is on outcomes such as the emancipation of patients and the prevention of burnout among providers.
Telehealth has become an essential part of healthcare delivery, particularly in recent years as a result of the COVID-19 pandemic. Telehealth organizations are experiencing an increased demand for remote healthcare services, and they are turning to artificial intelligence (AI) to provide innovative solutions that improve patient outcomes and increase efficiency.
One of the main issues in telehealth organizations is ensuring the privacy and security of patient data. Telehealth services are delivered through remote communication channels, such as video conferencing and messaging, which can be vulnerable to cyber-attacks. AI can play a crucial role in securing these communication channels by providing end-to-end encryption, multi-factor authentication, and other cybersecurity measures.
Another consideration in telehealth organizations is ensuring equitable access to healthcare services. AI-powered telehealth solutions can help to reduce barriers to healthcare access, particularly for underserved populations. For example, AI algorithms can analyze patient data to predict health outcomes and identify potential health issues before they become more severe, which can help to improve patient outcomes and reduce the need for expensive medical procedures. However, the use of AI in telehealth also raises ethical concerns, particularly around issues such as bias, transparency, and accountability. AI algorithms are only as unbiased as the data that they are trained on, and there is a risk that biased datasets can result in biased healthcare outcomes. Furthermore, the use of AI in healthcare can lead to concerns around accountability, particularly if the AI system makes a mistake or fails to detect a potential health issue. Despite these challenges, AI-powered telehealth solutions offer enormous potential for improving healthcare outcomes and increasing efficiency. Recent studies have shown that AI-powered telehealth solutions can improve the accuracy of diagnostic assessments, increase the speed of treatment, and reduce the cost of healthcare delivery [
49,
66,
67].
In conclusion, telehealth organizations are facing a range of issues and considerations when implementing AI-powered solutions. Privacy and security, equitable access to healthcare services, and ethical concerns around bias, transparency, and accountability are all key areas that need to be addressed. However, with careful planning and consideration, AI-powered telehealth solutions can improve patient outcomes and increase efficiency, making them an important tool for the future of healthcare delivery.
11. Future Considerations for AI in Telehealth: Research Perspectives
Artificial intelligence (AI) is expected to revolutionize the field of telehealth by providing innovative solutions that can enhance the quality of care and improve patient outcomes. As we continue to develop new AI-powered telehealth solutions, there are several important future considerations that need to be taken into account.
One key area for future research is the development of AI-powered diagnostic tools. Currently, many telehealth services rely on video conferencing to provide remote consultations with healthcare providers. However, AI-powered diagnostic tools have the potential to take telehealth to the next level by providing accurate and reliable diagnoses without the need for in-person consultations. For example, AI algorithms could be trained to analyze patient data such as medical images, lab test results, and vital signs to provide a diagnosis. This would greatly enhance the accessibility and efficiency of telehealth services, particularly in areas where there is a shortage of healthcare providers.
Another future consideration for AI in telehealth is the need for standardized data collection and analysis. In order for AI algorithms to be effective, they require large volumes of high-quality data to be trained on. However, the quality of data in healthcare can vary greatly, and there is a risk that AI algorithms could be trained on biased or incomplete datasets. Standardized data collection and analysis protocols can help to address these issues by ensuring that data are collected in a consistent and reliable manner, and that datasets are representative of diverse patient populations.
Additionally, ethical considerations around the use of AI in telehealth will continue to be a focus of future research. One of the key ethical concerns with AI is the potential for bias. AI algorithms are only as unbiased as the data they are trained on, and there is a risk that biased datasets can result in biased healthcare outcomes. Future research should focus on developing AI algorithms that are more transparent and explainable, so that patients and healthcare providers can better understand how AI-powered telehealth solutions are making healthcare decisions.
Another ethical consideration is the potential for AI-powered telehealth solutions to exacerbate existing healthcare disparities. For example, AI algorithms may be less accurate when diagnosing certain health conditions in underrepresented populations. Future research should aim to address these disparities by ensuring that AI algorithms are trained on diverse datasets that are representative of all patient populations [
68,
69,
70]. Finally, there is a need for ongoing evaluation of the effectiveness of AI-powered telehealth solutions. While there is great potential for AI to improve healthcare outcomes and increase efficiency, it is important to ensure that these solutions are actually delivering on these promises. Future research should aim to evaluate the impact of AI-powered telehealth solutions on patient outcomes, healthcare costs, and healthcare provider satisfaction.
Another important area for future research is the development of AI-powered predictive models. These models can be used to identify patients who are at risk of developing certain health conditions, allowing healthcare providers to intervene early and prevent the onset of disease. For example, AI algorithms can be used to analyze patient data such as lifestyle factors, medical history, and genetics to identify patients who are at risk of developing conditions such as diabetes, heart disease, or cancer. By identifying these patients early, healthcare providers can take proactive measures to prevent the onset of disease and improve patient outcomes. In addition to predictive models, there is also potential for AI-powered virtual assistants to improve the patient experience in telehealth. Virtual assistants can be used to answer patient questions, provide basic medical advice, and even assist with scheduling appointments. By leveraging AI technology, virtual assistants can provide personalized and efficient support to patients, freeing up healthcare providers to focus on more complex tasks. However, it is important to ensure that virtual assistants are designed with patient privacy and security in mind, and that patients are fully informed about the role of AI in their care [
50,
71].
In conclusion, the development of AI-powered telehealth solutions has the potential to transform the way healthcare is delivered. However, as we continue to develop these solutions, it is important to take into account key future considerations such as the development of AI-powered diagnostic tools, standardized data collection and analysis, ethical considerations around bias and healthcare disparities, and ongoing evaluation of effectiveness. By doing so, we can ensure that AI-powered telehealth solutions are able to deliver on their promise of improving healthcare outcomes and increasing efficiency.
12. Conclusions
In light of what has been said thus far, AI-enabled telehealth may make useful contributions in the form of quality enhancements to established practice and the introduction of novel approaches to medical treatment. We explored many facets of telehealth, including teleassessment, telediagnosis, tele-interactions, and telemonitoring. Expanded use will need further research into foundational algorithms and technique validation.
Computer intelligence is now at an advanced stage of development, and it has the potential to vastly improve upon both human processes and already existing technologies. This article highlights the significance of this technology’s use in the medical profession and discusses the many areas in which it has proven useful. Because of its adaptability and vast growth potential, telemedicine already has a profound influence. However, certain problems must yet be fixed. Telemedicine has caught up with the times in terms of the use of AI.
As AI-enabled telemedicine grows more widespread, it is important to consider a number of social and ethical implications. In contrast to humans, artificial intelligence systems never lack desire or drive; yet, in the absence of emotions, such systems lack the capacity to evaluate the morality of actions and the repercussions thereof. Continuous testing and improvement are necessary to advance human–AI interaction since most AI technologies need a lengthy learning period that can only attain dependability after a very long time. Controlling telehealth services is especially challenging since certain parts of the service delivery infrastructure may only include a person sometimes. If anything goes wrong in such a situation, society will have to figure out who to punish (
Table 4).





{kind=link}
{kind=link}