
Syndromic Surveillance among Evacuees at a Houston “Megashelter” following Hurricane Harvey

Abstract
:1. Introduction
2. Materials and Methods
2.1. Cot Survey Tool
2.2. Cot Survey Administration
2.3. Survey Metrics and Data Analysis
2.4. Geospatial Analysis
3. Results
3.1. Cot Survey Performance
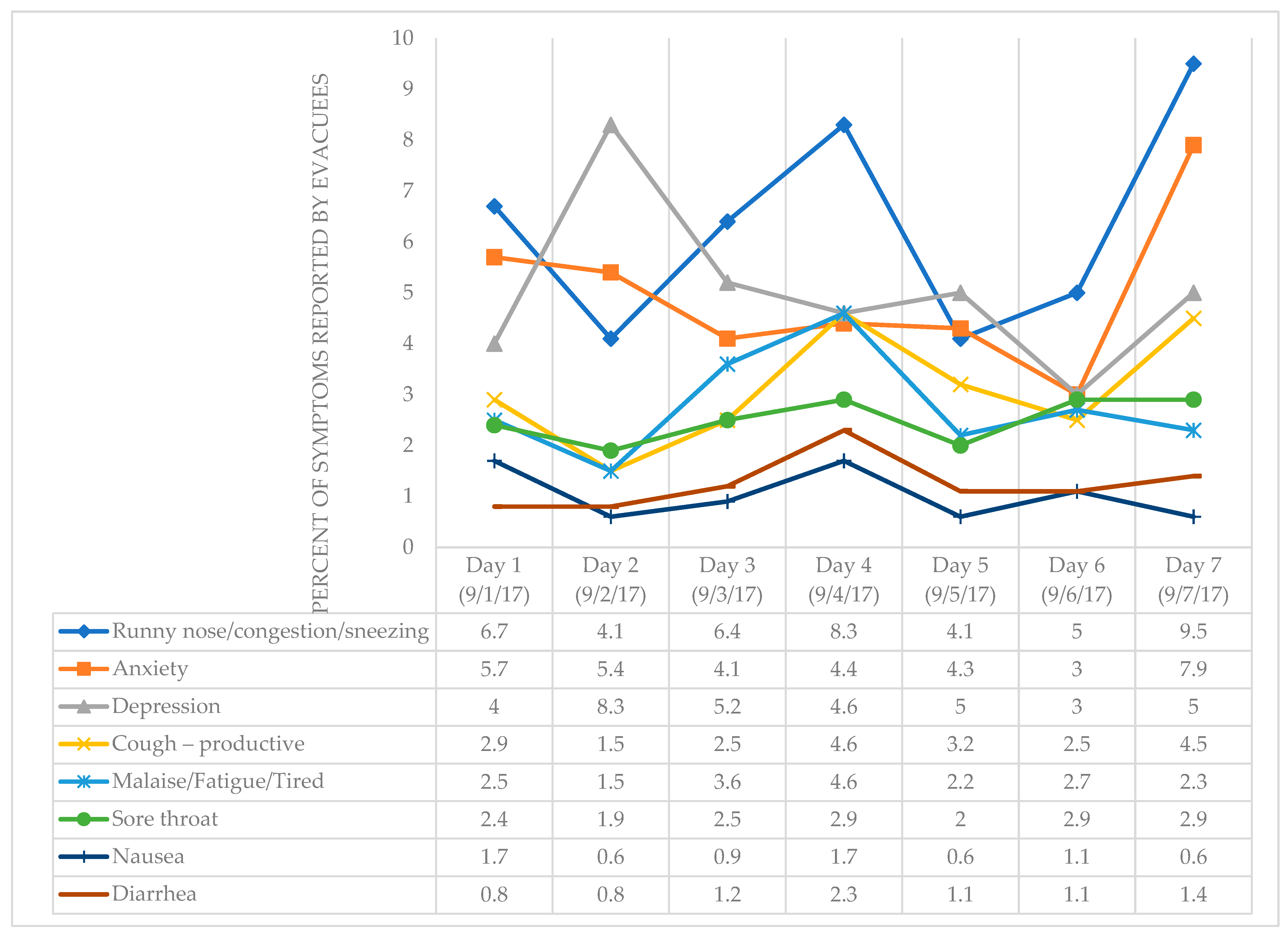
3.2. Syndromic Surveillance
3.3. Geospatial Analysis
4. Discussion
4.1. Syndromic Surveillance
4.2. Strengths of the Digital Drop-In Cot Survey
4.3. Limitations of the Digital Drop-In Cot Survey
4.4. Implications in Disaster Epidemiology
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Night Question Was Asked | Question | Response Options English/Spanish |
|---|---|---|
| All nights | Hello, my name is [enter name], and we are working with the City of Houston to monitor the health of everyone in the shelter. May we ask you a couple of questions to see how you are feeling? Hola, mi nombre es [tu nombre] y estamos trabajando con la Ciudad de Houston para monitorear la salud de todos que usan este refugio. ¿Podemos preguntarle un poco para ver cómo se siente? |
|
| All nights | Agree to participate? |
|
| All nights 1 | How old are you? ¿Cuantos años tiene usted? |
|
| All nights | How are you feeling? Any symptoms of illness? If yes, what are your symptoms? ¿Siente algún síntoma de enfermedad? ¿Cuáles son sus síntomas? |
|
| Night 1 | What zip code are you from? ¿Cuál es su código postal? |
|
| Night 1 | Do you have any pets with you? ¿Tiene mascotas con usted? |
|
| Night 1 | If yes, what type of pet and how many? Si sí, ¿qué tipos de mascotas y cuántos? |
|
| Night 2 | How many nights have you stayed at the shelter? ¿Cuantas noches ha pasado en el refugio? |
|
| Night 2 | What type of living arrangement did you have before Hurricane Harvey? ¿Dónde vivió antes de venir al refugio por el huracán Harvey? |
|
| All nights | Any questions or concerns raised by the evacuee? ¿Tiene algunas preguntas o dudas? |
|
| All nights | Thank you for your time. We appreciate your help. Gracias por su tiempo. Apreciamos su ayuda. {End of participant survey. Move to next evacuee.} |
|
References
- Watson, K.M.; Harwell, G.R.; Wallace, D.S.; Welborn, T.L.; Stengel, V.G.; McDowell, J.S. Characterization of Peak Streamflows and Flood Inundation of Selected Areas in Southeastern Texas and Southwestern Louisiana from the August and September 2017 Flood Resulting from Hurricane Harvey; U.S. Geological Survey Scientific Investigations Report 2018–5070; U.S. Department of the Interior, U.S. Geological Survey, Texas Water Science Center: Reston, VA, USA, 2018.
- OAA National Weather Service. Major Hurricane Harvey—August 25–29, 2017. U.S. Department of Commerce. National Oceanic and Atmospheric Administration, National Weather Service: Silver Spring, MD, USA. Available online: https://www.weather.gov/crp/hurricane_harvey (accessed on 23 June 2021).
- Blinder, A.; Healy, J. Coffee and Cots as Houston Houses Thousands in a Convention Center. The New York Times. 28 August 2017. Available online: https://www.nytimes.com/2017/08/28/us/harvey-evacuations-texas.html (accessed on 9 October 2021).
- Gale, C. 22 Days at George R. Brown. PCMA Convene. 1 December 2017. Available online: https://www.pcmaconvene.org/convene-magazine/22-days-george-r-brown/ (accessed on 9 October 2021).
- Blake, E.S.; Zelinsky, D.A. Tropical Cyclone Report: Hurricane Harvey (17 August–1 September 2017); AL092017; 77p, National Hurricane Center; U.S. Department of Commerce, National Oceanic and Atmospheric Administration, National Weather Service: Silver Spring, MD, USA, 2018. Available online: https://www.nhc.noaa.gov/data/tcr/AL092017_Harvey.pdf (accessed on 23 June 2021).
- Waddell, S.; Jayaweera, D.; Mirsaeidi, M.; Beier, J.; Kumar, N. Perspectives on the Health Effects of Hurricanes: A Review and Challenges. Int. J. Environ. Res. Public Health 2021, 18, 2756. [Google Scholar] [CrossRef] [PubMed]
- City of Houston. Houston’s Hazards—Office of Emergency Management. Available online: https://www.houstonoem.org/houstons-hazards/ (accessed on 18 February 2022).
- Henning, K.J. Overview of Syndromic Surveillance What is Syndromic Surveillance? MMWR Morb. Mortal. Wkly. Rep. 2004, 53, 5–11. [Google Scholar]
- Murray, K.O.; Kilborn, C.; Desvignes-Kendrick, M.; Koers, E.; Page, V.; Selwyn, B.J.; Shah, U.; Palacio, H. Emerging Disease Syndromic Surveillance for Hurricane Katrina Evacuees Seeking Shelter in Houston’s Astrodome and Reliant Park Complex. Public Health Rep. 2009, 124, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, S.A.; Goodman, R.A. The CDC Field Epidemiology Manual, 4th ed.; Oxford University Press: New York, NY, USA, 2019. [Google Scholar]
- Caillouet, L.P.; Paul, P.J.; Sabatier, S.M.; Caillouet, K.A. Eye of the storm: Analysis of shelter treatment records of evacuees to Acadiana from Hurricanes Katrina and Rita. Am. J. Disaster Med. 2012, 7, 253–271. [Google Scholar] [CrossRef]
- Hurricane Ike Rapid Needs Assessment—Houston, Texas, September 2008. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5838a3.htm (accessed on 18 February 2022).
- Stone, G.; Lekht, A.; Burris, N.; Williams, C. Data Collection and Communications in the Public Health Response to a Disaster: Rapid Population Estimate Surveys and the Daily Dashboard in Post-Katrina New Orleans. J. Public Health Manag. Pract. 2007, 13, 453–460. [Google Scholar] [CrossRef]
- Bathaei, S.A.; Abolghasem-Gorji, H.; Delgoshaei, B.; Khankeh, H.R. Emergency health evaluation of affected population during disasters: Are there new approaches? J. Educ. Health Promot. 2019, 8, 2. [Google Scholar]
- Llamas, T.; Shapiro, E.; Jacobo, J. Inside the Houston convention center where Harvey evacuees are double the capacity. ABC News. 30 August 2017. Available online: https://abcnews.go.com/US/inside-houston-convention-center-harvey-evacuees-double-capacity/story?id=49487937 (accessed on 9 October 2021).
- Esri. United States ZIP Code Boundaries 2020—Overview. Available online: https://esri.maps.arcgis.com/home/item.html?id=46b350fa939149debfd9cc71566b43b4 (accessed on 2 November 2021).
- Tunstall, S.; Tapsell, S.; Green, C.; Floyd, P.; George, C. The health effects of flooding: Social research results from England and Wales. J. Water Health 2006, 4, 365–380. [Google Scholar] [CrossRef]
- Taioli, E.; Tuminello, S.; Lieberman-Cribbin, W.; Bevilacqua, K.; Schneider, S.; Guzman, M.; Kerath, S.; Schwartz, R.M. Mental health challenges and experiences in displaced populations following Hurricane Sandy and Hurricane Harvey: The need for more comprehensive interventions in temporary shelters. J. Epidemiol. Community Health 2018, 72, 867–870. [Google Scholar] [CrossRef]
- Makwana, N. Disaster and its impact on mental health: A narrative review. J. Fam. Med. Prim. Care 2019, 8, 3090–3095. [Google Scholar] [CrossRef]
- Peek, L. Children and Disasters: Understanding Vulnerability, Developing Capacities, and Promoting Resilience—An Introduction. Child. Youth Environ. 2008, 18, 1–29. [Google Scholar]
- Schnall, A.H.; Hanchey, A.; Nakata, N.; Wang, A.; Jeddy, Z.; Alva, H.; Tan, C.; Boehmer, T.; Bayleyegn, T.; Casey-Lockyer, M. Disaster-Related Shelter Surveillance during the Hurricane Harvey Response—Texas 2017. Disaster Med. Public Health Prep. 2020, 14, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Travia, K.R.; Kahkoska, A.R.; Igudesman, D.; Souris, K.J.; Beasley, C.; Mayer-Davis, E.J. Impact of Hurricane Matthew on Diabetes Self-Management and Outcomes. North Carol. Med. J. 2021, 82, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.; Lee, D.C.; Doran, K.M.; Grudzen, C.R.; Worthing, J.; Portelli, I.; Goldfrank, L.R.; Smith, S.W. Vulnerability of Older Adults in Disasters: Emergency Department Utilization by Geriatric Patients After Hurricane Sandy. Disaster Med. Public Health Prep. 2018, 12, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Norovirus outbreak among evacuees from hurricane Katrina—Houston, Texas, September 2005. MMWR Morb. Mortal. Wkly. Rep. 2005, 54, 1016–1018. [Google Scholar]
- Neilson-Gammon, J.; Escobedo, J.; Ott, C.; Dedrick, J.; Van Fleet, A. Assessment of Historic and Future Trends of Extreme Weather in Texas, 1900–2036. Office of the Texas State Climatologist, Texas A&M University. Available online: https://texas2036.org/weather/ (accessed on 15 October 2021).
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef] [Green Version]
- Hicks, K. Deputy Secretary of Defense Dr. Kathleen H. Hicks’ Remarks at Worldwide Logistics Symposium 2022: “Global Security Implications of Climate Change”. Available online: https://www.defense.gov/News/Transcripts/Transcript/Article/2959502/deputy-secretary-of-defense-dr-kathleen-h-hicks-remarks-at-worldwide-logistics/ (accessed on 18 March 2022).
- International Federation of Red Cross and Red Crescent Societies. World Disasters Report 2020. Available online: https://oldmedia.ifrc.org/ifrc/world-disaster-report-2020/ (accessed on 18 March 2022).
- Frank, T. 2020 Is a Record Year for Disaster Shelters, Red Cross Says. Scientific American. 2 December 2020. Available online: https://www.scientificamerican.com/article/2020-is-a-record-year-for-disaster-shelters-red-cross-says/ (accessed on 18 March 2022).
- Smith, A.B. U.S. Billion-Dollar Weather and Climate Disasters, 1980–present (NCEI Accession 0209268); NOAA National Centers for Environmental Information: Asheville, NC, USA, epub ahead of printing; 2022. [CrossRef]
- Understanding Houston. Natural Disaster Risks in Houston. Available online: https://www.understandinghouston.org/topic/disasters/disaster-risks#flooding_risks (accessed on 18 March 2022).
- Liu, L.; Haynie, A.; Jin, S.; Zangeneh, A.; Bakota, E.; Hornstein, B.D.; Beckham, D.; Reed, B.C.; Kiger, J.; McClendon, M.; et al. Influenza A (H3) Outbreak at a Hurricane Harvey Megashelter in Harris County, Texas: Successes and Challenges in Disease Identification and Control Measure Implementation. Disaster Med. Public Health Prep. 2019, 13, 97–101. [Google Scholar] [CrossRef]
- Fazel, S.; Geddes, J.R.; Kushel, M. The health of homeless people in high-income countries: Descriptive epidemiology, health consequences, and clinical and policy recommendations. Lancet 2014, 384, 1529–1540. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Surveillance Strategy Repot—Syndromic Reporting. Public Health Surveillance and Data. Available online: https://www.cdc.gov/surveillance/initiatives/symptoms-signal.html (accessed on 14 March 2022).
- Centers for Disease Control and Prevention (CDC). A Primer for Understanding the Principles and Practices of Disaster Surveillance in the United States, 1st ed.; CDC: Atlanta, GA, USA, 2016.
- Comfort, L.K.; Haase, T.W. Communication, Coherence, and Collective Action: The Impact of Hurricane Katrina on Communications Infrastructure. Public Work. Manag. Policy 2006, 10, 328–343. [Google Scholar] [CrossRef]
- Santos-Burgoa, C.; Goldman, A.; Andrade, E.; Barrett, N.; Colon-Ramos, U.; Edberg, M.; Garcia-Meza, A.; Goldman, L.; Roess, A.; Sandberg, J.; et al. Ascertainment of the Estimated Excess Mortality from Hurricane María in Puerto Rico; The George Washington University: Washington, DC, USA, 2018. [Google Scholar]
- Schnall, A.H.; Roth, J.; Ekpo, L.L.; Guendel, I.; Davis, M.; Ellis, E.M. Disaster-Related Surveillance Among US Virgin Islands (USVI) Shelters During the Hurricanes Irma and Maria Response. Disaster Med. Public Health Prep. 2019, 13, 38–43. [Google Scholar] [CrossRef]
- Surveillance in Hurricane Evacuation Centers—Louisiana, September–October 2005. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5502a3.htm (accessed on 14 March 2022).
- CDC Shelter Assessment Tool | Emergency Preparedness and Response. Available online: https://emergency.cdc.gov/shelterassessment/ (accessed on 14 March 2022).
- New Hampshire Department of Health and Human Services. Shelter Surveillance in Emergency Shelters. Available online: https://www.dhhs.nh.gov/esu/shelter-surveillance.htm (accessed on 14 March 2022).
- Public Health Assessment and Surveillance|Natural Disasters and Severe Weather|CDC. Available online: https://www.cdc.gov/disasters/surveillance/index.html (accessed on 14 March 2022).
- Fleischauer, A.; Young, S.; Mott, J.; Ratard, R. Disaster Surveillance Revisited: Passive, Active and Electronic Syndromic Surveillance during Hurricane Katrina, New Orleans, LA–2005. Corpus ID: 57880136. Available online: https://www.semanticscholar.org/paper/Disaster-Surveillance-Revisited%3A-Passive%2C-Active-LA-Fleischauer-Young/8723a2ed07af8dce43f7cc0c3a4312012b7317be (accessed on 18 March 2022).
- Stoto, M.A. Syndromic Surveillance. Available online: https://issues.org/stoto/ (accessed on 14 March 2022).
- Customer Story, Google Workspace. Eagle County, Colorado: Powering Real-Time Emergency Response through Cloud Collaboration. Available online: https://workspace.google.com/customers/eagle-county.html (accessed on 18 March 2022).
- Shumate, A.M.; Yard, E.E.; Casey-Lockyer, M.; Apostolou, A.; Chan, M.; Tan, C.; Noe, R.S.; Wolkin, A.F. Effectiveness of Using Cellular Phones to Transmit Real-Time Shelter Morbidity Surveillance Data After Hurricane Sandy, New Jersey, October to November, 2012. Disaster Med. Public Health Prep. 2016, 10, 525–528. [Google Scholar] [CrossRef]
- Zhang, M.W.; Ho, C.S.; Fang, P.; Lu, Y.; Ho, R.C. Usage of social media and smartphone application in assessment of physical and psychological well-being of individuals in times of a major air pollution crisis. JMIR Mhealth Uhealth 2014, 2, e16. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| Survey Draft | Date Used | Number of Survey Questions | Number of Volunteers | Number of Spanish-Speaking Volunteers | Total Participants Approached | Cumulative Daily Survey Duration (Minutes) | Average Time per Interview (in Minutes) | Participation Rate (%) |
|---|---|---|---|---|---|---|---|---|
| 1 | 9/1/17 | 5 | 24 | 6 | 682 | 131 | 5.18 | 89.0% |
| 2 | 9/2/17 | 4 | 20 | 6 | 537 | 193 | 7.94 | 90.5% |
| 3 | 9/3/17 | 2 | 31 | 6 | 624 | 95 | 5.17 | 91.3% |
| 9/4/17 | 2 | 21 | 5 | 621 | 170 | 6.21 | 92.6% | |
| 4 * | 9/5/17 | 2 | 13 | 5 | 575 | 143 | 3.39 | 95.3% |
| 9/6/17 | 2 | 30 | 8 | 602 | 99 | 5.25 | 93.9% | |
| 9/7/17 | 2 | 26 | 8 | 515 | 87 | 4.59 | 95.5% | |
| Mean | 3 | 24 | 6 | 594 | 131 | 5.2 | 92.6% |
| 1-September | 2-September | 3-September | 4-September | 5-September | 6-September | 7-September | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Count | Percent | Count | Percent | Count | Percent | Count | Percent | Count | Percent | Count | Percent | Count | Percent | |
| Cot Survey Participation | ||||||||||||||
| Total active cots | 2016 | - | 1067 | - | - | - | 1460 | - | - | - | - | - | - | - |
| Agreed to participate | 607 | - | 486 | - | 570 | - | 575 | - | 548 | - | 565 | - | 492 | - |
| Reported Age Range | ||||||||||||||
| Total * | 594 | 482 | 563 | 521 | 538 | 559 | 484 | |||||||
| <1 year | 9 | 1.5 | 3 | 0.6 | 7 | 1.2 | 7 | 1.3 | 7 | 1.3 | 6 | 1.1 | 9 | 1.9 |
| 1–5 years | 36 | 6.1 | 24 | 5.0 | 22 | 3.9 | 28 | 5.4 | 28 | 5.2 | 25 | 4.5 | 22 | 4.5 |
| 6–10 years | 19 | 3.2 | 19 | 3.9 | 24 | 4.3 | 23 | 4.4 | 26 | 4.8 | 19 | 3.4 | 19 | 3.9 |
| 11–18 years | 43 | 7.2 | 28 | 5.8 | 43 | 7.6 | 29 | 5.6 | 46 | 8.6 | 39 | 7.0 | 31 | 6.4 |
| 19–25 years | 43 | 7.2 | 38 | 7.9 | 32 | 5.7 | 36 | 6.9 | 45 | 8.4 | 39 | 7.0 | 30 | 6.2 |
| 26–40 years | 139 | 23.4 | 105 | 21.8 | 134 | 23.8 | 128 | 24.6 | 127 | 23.6 | 131 | 23.4 | 112 | 23.1 |
| 41–64 years | 265 | 44.6 | 222 | 46.1 | 262 | 46.5 | 240 | 46.1 | 226 | 42.0 | 271 | 48.5 | 231 | 47.7 |
| ≥65 years | 40 | 6.7 | 43 | 8.9 | 39 | 6.9 | 30 | 5.8 | 33 | 6.1 | 29 | 5.2 | 30 | 6.2 |
| Reported Symptoms 1 | ||||||||||||||
| Runny nose/congestion/sneezing | 40 | 6.7 | 20 | 4.1 | 36 | 6.4 | 43 | 8.3 | 22 | 4.1 | 28 | 5.0 | 46 | 9.5 |
| Achy muscles/joints | 37 | 6.2 | 23 | 4.8 | 27 | 4.8 | 17 | 3.3 | 14 | 2.6 | 14 | 2.5 | 16 | 3.3 |
| Anxiety | 34 | 5.7 | 26 | 5.4 | 23 | 4.1 | 23 | 4.4 | 23 | 4.3 | 17 | 3.0 | 38 | 7.9 |
| Headache | 27 | 4.5 | 15 | 3.1 | 23 | 4.1 | 16 | 3.1 | 18 | 3.3 | 12 | 2.1 | 17 | 3.5 |
| Depression | 24 | 4.0 | 40 | 8.3 | 29 | 5.2 | 24 | 4.6 | 27 | 5.0 | 17 | 3.0 | 24 | 5.0 |
| Cough—productive | 17 | 2.9 | 7 | 1.5 | 14 | 2.5 | 24 | 4.6 | 17 | 3.2 | 14 | 2.5 | 22 | 4.5 |
| Stomach pain/cramping | 14 | 2.4 | 10 | 2.1 | 6 | 1.1 | 10 | 1.9 | 9 | 1.7 | 6 | 1.1 | 7 | 1.4 |
| Sore throat | 14 | 2.4 | 9 | 1.9 | 14 | 2.5 | 15 | 2.9 | 11 | 2.0 | 16 | 2.9 | 14 | 2.9 |
| Cough—non-productive | 12 | 2.0 | 15 | 3.1 | 13 | 2.3 | 23 | 4.4 | 14 | 2.6 | 16 | 2.9 | 9 | 1.9 |
| Injury/Skin wounds | 12 | 2.0 | 4 | 0.8 | 9 | 1.6 | 5 | 1.0 | 3 | 0.6 | 3 | 0.5 | 3 | 0.6 |
| Malaise/Fatigue/Tired | 15 | 2.5 | 7 | 1.5 | 20 | 3.6 | 24 | 4.6 | 12 | 2.2 | 15 | 2.7 | 11 | 2.3 |
| Fever | 10 | 1.7 | 8 | 1.7 | 5 | 0.9 | 5 | 1.0 | 0 | 0.0 | 2 | 0.4 | 3 | 0.6 |
| Nausea | 10 | 1.7 | 3 | 0.6 | 5 | 0.9 | 9 | 1.7 | 3 | 0.6 | 6 | 1.1 | 3 | 0.6 |
| Rash | 8 | 1.3 | 9 | 1.9 | 6 | 1.1 | 2 | 0.4 | 2 | 0.4 | 5 | 0.9 | 2 | 0.4 |
| Diarrhea | 5 | 0.8 | 4 | 0.8 | 7 | 1.2 | 12 | 2.3 | 6 | 1.1 | 6 | 1.1 | 7 | 1.4 |
| Animal or insect bites | 2 | 0.3 | 2 | 0.4 | 5 | 0.9 | 6 | 1.2 | 2 | 0.4 | 1 | 0.2 | 1 | 0.2 |
| Vomiting | 2 | 0.3 | 3 | 0.6 | 2 | 0.4 | 3 | 0.6 | 1 | 0.2 | 3 | 0.5 | 2 | 0.4 |
| All Participants with Age Reported (n = 3741) | Adults 18 and Older (n = 3100) | Children under 18 Years (n = 641) | Statistical Differences between Children and Adults | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | OR 1 | 95% CI 2 | p-Value | |
| Reported Symptoms | 1347 | 36 | 1187 | 38 | 160 | 25 | 1.87 | [1.53, 2.28] | <0.0001 |
| Mental Health | |||||||||
| Anxiety | 180 | 5 | 171 | 6 | 9 | 1 | 4.09 | [2.09, 9.17] | <0.0001 |
| Depression | 183 | 5 | 183 | 6 | 0 | 0 | undefined | undefined | N/A |
| Physical Health | |||||||||
| Runny nose/congestion/sneezing | 230 | 6 | 163 | 5 | 67 | 10 | 0.48 | [0.35, 0.65] | <0.0001 |
| Achy muscles/joints | 146 | 4 | 143 | 5 | 3 | 0 | 10.3 | [3.43, 50.60] | <0.0001 |
| Headache | 126 | 3 | 109 | 4 | 17 | 3 | 1.34 | [0.79, 2.40] | 0.2697 |
| Cough—productive | 114 | 3 | 90 | 3 | 24 | 4 | 0.77 | [0.48, 1.27] | 0.2595 |
| Cough—non-productive | 96 | 3 | 71 | 2 | 25 | 4 | 0.58 | [0.36, 0.96] | 0.019 |
| Stomach pain/cramping | 62 | 2 | 54 | 2 | 8 | 1 | 1.4 | [0.66, 3.43] | 0.3726 |
| Sore throat | 91 | 2 | 77 | 2 | 14 | 2 | 1.14 | [0.64, 2.20] | 0.6538 |
| Injury/Skin wounds | 35 | 1 | 35 | 1 | 0 | 0 | undefined | undefined | N/A |
| Rash | 31 | 1 | 25 | 1 | 6 | 1 | 0.86 | [0.34, 2.58] | 0.7418 |
| Malaise/Fatigue/Tired | 82 | 2 | 80 | 3 | 2 | 0 | 8.46 | [2.26, 71.24] | 0.0004 |
| Fever | 30 | 1 | 23 | 1 | 7 | 1 | 0.68 | [0.28, 1.88] | 0.3656 |
| Nausea | 39 | 1 | 39 | 1 | 0 | 0 | undefined | undefined | N/A |
| Diarrhea | 46 | 1 | 34 | 1 | 12 | 2 | 0.58 | [0.29, 1.24] | 0.1049 |
| Vomiting | 16 | 0 | 13 | 0 | 3 | 0 | 0.9 | [0.25, 4.91] | 0.8635 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leining, L.M.; Short, K.; Erickson, T.A.; Gunter, S.M.; Ronca, S.E.; Schulte, J.; Murray, K.O. Syndromic Surveillance among Evacuees at a Houston “Megashelter” following Hurricane Harvey. Sustainability 2022, 14, 6018. https://doi.org/10.3390/su14106018
Leining LM, Short K, Erickson TA, Gunter SM, Ronca SE, Schulte J, Murray KO. Syndromic Surveillance among Evacuees at a Houston “Megashelter” following Hurricane Harvey. Sustainability. 2022; 14(10):6018. https://doi.org/10.3390/su14106018
Chicago/Turabian StyleLeining, Lauren M., Kirstin Short, Timothy A. Erickson, Sarah M. Gunter, Shannon E. Ronca, Joann Schulte, and Kristy O. Murray. 2022. "Syndromic Surveillance among Evacuees at a Houston “Megashelter” following Hurricane Harvey" Sustainability 14, no. 10: 6018. https://doi.org/10.3390/su14106018