
Digitalization as an Engine for Change? Building a Vision Pathway towards a Sustainable Health Care System by Using the MLP and Health Economic Decision Modelling


Abstract
:1. Introduction
2. Multi-Level Perspective and Health Economic Decision Modelling as a Theoretical Framing of Digital Socio-Technical Change
2.1. Digital Technologies Create Promises in Changing the Health Care System towards Prevention
2.2. Finnish Health Care System and Multi-Level Perspective (MLP) Explaining the Socio-Technical Change
2.3. Transition Pathways
2.4. Quantitative Modelling Tools in Transition Studies
2.5. Health Economic Decision Modelling
3. Materials and Methods
3.1. Data Collection for Vision Pathway Formulation
3.2. Data Collection and Analysis of the Health Economic Decision Model and an Online Tool
- Developing the conceptual model. Modelling process was started by defining the parts of reality in a case of T2D prevention in the Finnish adult population aged 45–75 years, where the incidence of T2D is the most typical. The focus was on the modelling of the incidence of T2D based on its known risk factors; and how the modification of this underlying risk could affect the annual incidence of T2D at the target population level.
- Constructing the model. A simple, commonly applied cohort-based, Markov-type, discrete state transition model with three health states (i.e., no T2D, T2D, and death) were developed to model population transitions between the defined health states in the model.
- Informing the model parameters. Models require evidence to inform their parameters. In this case, the age- and sex-specific proportions of Finnish adult population at moderately or high risk of T2D was derived from the national FINRISK follow-up data [62] by applying the FINDRISC score [35], which predicts 10-year risk to develop T2D based on socio-demographic, behavioral and anthropometric factors. Additional direct (i.e., due to health care use) and productivity (i.e., due to work absenteeism and permanent work disability) costs associated with T2D were obtained from a previous study applying the national social and health care registries [3]. Changes in risk of all-cause mortality due to T2D was obtained from a previously published study [63].
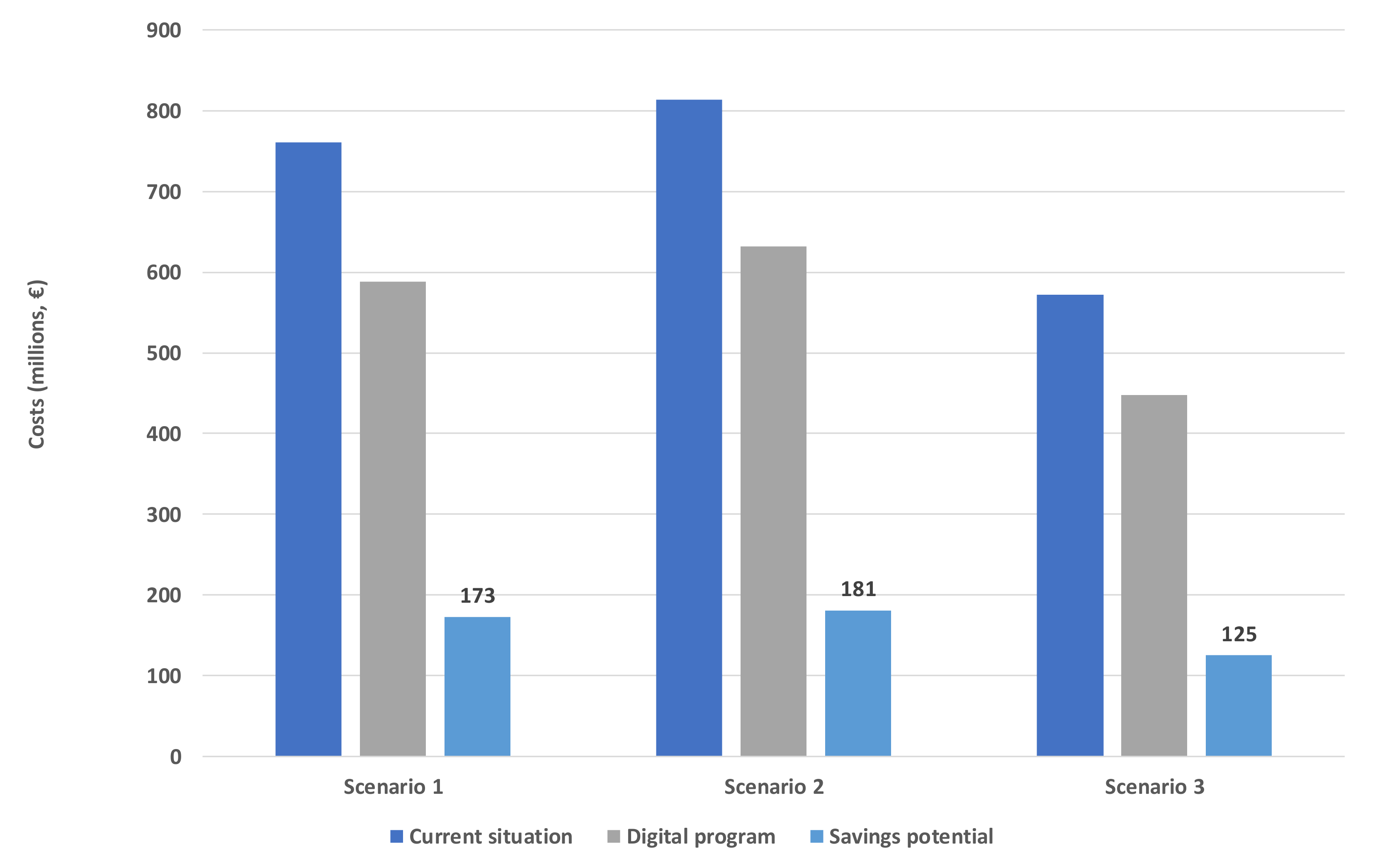
- Exercising the developed model. Formulating scenarios, which were developed for the purposes of the present study focusing on digital tools.
- Online tool. The developed model was published as a web-based online tool with automatic reporting to allow different stakeholders from various organizations to build their own projections and manipulate model assumptions related to, e.g., a level of baseline risk in a target population or an applied perspective of analysis (i.e., a health care payer vs. societal perspective), as well as change parameter values (e.g., a size of target population, a cost of prevention program, etc.) as needed. The pdf report that the users receive from using the tool included the calculations of potential savings and the vision pathway with identified themes from the interviews. The transition-focused storylines of each of the themes gives users information of the barriers and facilitators of the needed changes in the health care system.
4. Results
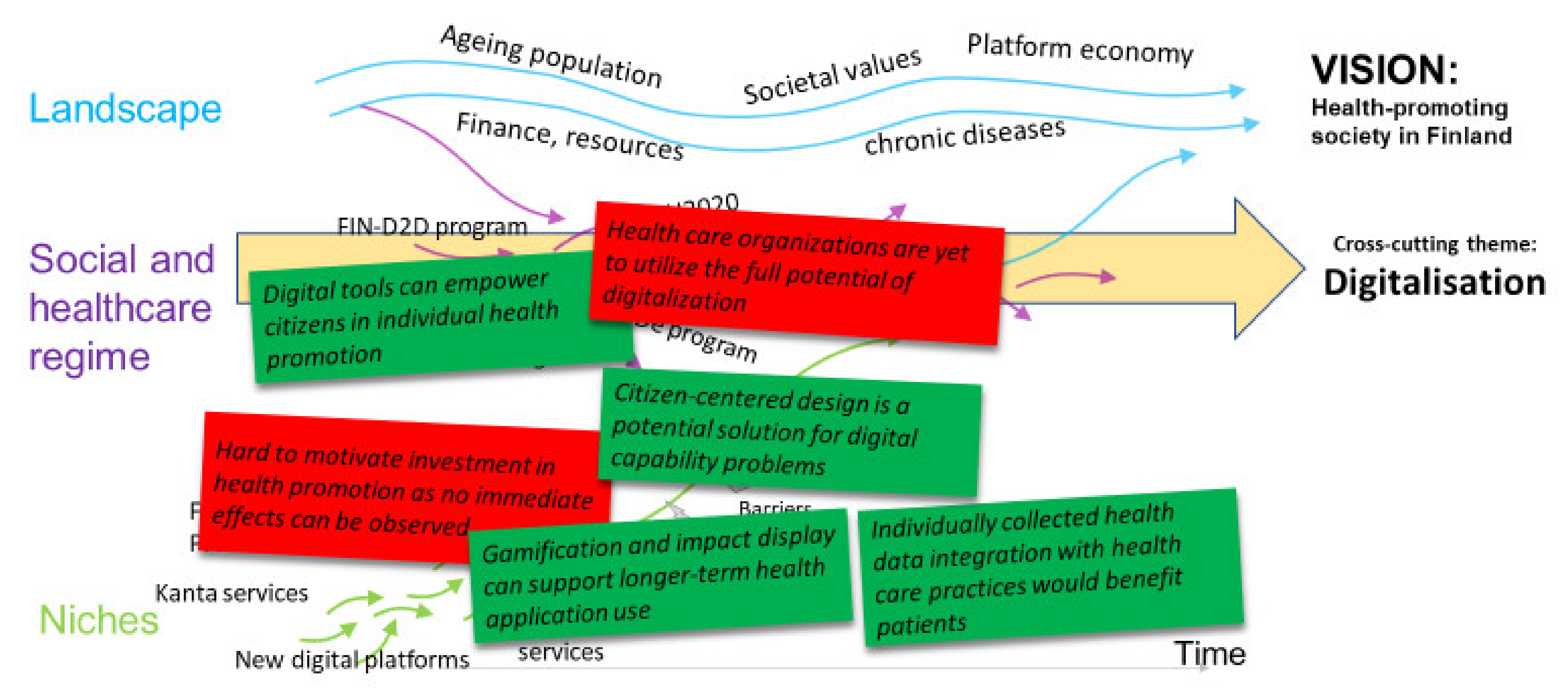
4.1. Contextualizing the Digital Transition for T2D Prevention
4.2. The Opportunities and Barriers of Digital Tools for a Transition towards T2D Prevention—Analysis of the Interviews
4.2.1. Health Care Organizations Are Yet to Utilize the Full Potential of Digitalization
4.2.2. Digital Tools Can Empower Citizens in Individual Health Promotion
4.2.3. Individually Collected Health Data Integration with Health Care Practices Would Benefit Patients
4.2.4. Hard to Motivate Investment in Health Promotion as No Immediate Effects Can Be Observed
4.2.5. Citizen-Centered Design Is a Potential Solution for Digital Capability Problems
4.2.6. Gamification and Displaying Impacts Can Support Longer-Term Health Application Use
4.2.7. Identified Facilitators and Barriers towards the Change in MLP Model
4.3. The Use of a Digitally Supported Prevention Program in Different Target Populations—Health Economic Outcomes
4.4. Online Tool Combining Transition-Focused Storylines and Forward-Looking Scenario Analyses
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Noncommunicable Diseases. Available online: http://www.euro.who.int/en/health-topics/noncommunicable-diseases (accessed on 17 December 2020).
- IDF Europe 2017 Publication-Integrating Diabetes Evidence into Practice: Challenges and Opportunities to Bridge the Gaps. Available online: https://www.idf.org/our-network/regions-members/europe/publications-and-resources/54-idf-europe-2017-publication-integrating-diabetes-evidence-into-practice-challenges-and-opportunities-to-bridge-the-gaps.html (accessed on 1 August 2018).
- Koski, S.; Ilanne-Parikka, P.; Kurkela, O.; Jarvala, T.; Rissanen, P. Diabeteksen kustannukset: Lisäsairauksien ilmaantumisen puolittaminen toisi satojen miljoonien säästöt vuodessa. Diabetes Ja Lääkäri 2018, 47, 13–17. [Google Scholar]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- Lindström, J.; Peltonen, M.; Eriksson, J.G.; Aunola, S.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Uusitupa, M.; Tuomilehto, J. For the finnish diabetes prevention study (DPS) group determinants for the effectiveness of lifestyle intervention in the finnish diabetes prevention study. Diabetes Care 2008, 31, 857–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herman, W.H. The cost-effectiveness of diabetes prevention: Results from the Diabetes Prevention Program and the Diabetes Prevention Program Outcomes Study. Clin. Diabetes Endocrinol. 2015, 1, 9. [Google Scholar] [CrossRef] [Green Version]
- Thomas, C.; Sadler, S.; Breeze, P.; Squires, H.; Gillett, M.; Brennan, A. Assessing the potential return on investment of the proposed UK NHS diabetes prevention programme in different population subgroups: An economic evaluation. BMJ Open 2017, 7, e014953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olchanski, N.; van Klaveren, D.; Cohen, J.T.; Wong, J.B.; Ruthazer, R.; Kent, D.M. Targeting of the diabetes prevention program leads to substantial benefits when capacity is constrained. Acta Diabetol. 2021, 58, 707–722. [Google Scholar] [CrossRef] [PubMed]
- Brundtland, G. Report of the World Commission on Environment and Development: Our Common Future. In United Nations General Assembly Document; Oxford University Press: Oxford, UK, 1987. [Google Scholar]
- Jameton, A.; McGuire, C. Toward sustainable health-care services: Principles, challenges, and a process. Int. J. Sustain. High. Educ. 2002, 3, 113–127. [Google Scholar] [CrossRef]
- Fineberg, H.V. A successful and sustainable health system—How to get there from here. N. Engl. J. Med. 2012, 366, 1020–1027. [Google Scholar] [CrossRef] [Green Version]
- United Nations. The 2030 Agenda for Sustainable Development. 2021. Available online: https://sdgs.un.org/goals (accessed on 26 March 2021).
- Report of the EXpert Panel on Effective Ways of Investing in Health (EXPH). Assessing the Impact of Digital Transformation of Health Services. 2019. Available online: https://ec.europa.eu/health/sites/default/files/expert_panel/docs/022_digitaltransformation_en.pdf (accessed on 21 October 2021).
- Virtanen, P.; Stenvall, J. Intelligence Health Policy. Theory, Concept and Practice; Springer International Publishing: Cham, Switzerland, 2018. [Google Scholar]
- Tatara, N.; Arsand, E.; Skrøvseth, S.O.; Hartvigsen, G.; Mattila, E.; De Alarcon-Sanchez, P. Long-term engagement with a mobile self-management system for people with type 2 diabetes. JMIR mHealth uHealth 2013, 1, e1. [Google Scholar] [CrossRef] [Green Version]
- Geels, F.; Kemp, R. Dynamics in socio-technical systems: Typology of change processes and contrasting case studies. Technol. Soc. 2007, 29, 441–455. [Google Scholar] [CrossRef]
- Köhler, J.; Geels, F.W.; Kern, F.; Markard, J.; Onsongo, E.; Wieczorek, A.; Alkemade, F.; Avelino, F.; Bergek, A.; Boons, F.; et al. An agenda for sustainability transitions research: State of the art and future directions. Environ. Innov. Soc. Transit. 2019, 31, 1–32. [Google Scholar] [CrossRef] [Green Version]
- Geels, F.W.; Schwanen, T.; Sorrell, S.; Jenkins, K.; Sovacool, B.K. Reducing energy demand through low carbon innovation: A sociotechnical transitions perspective and thirteen research debates. Energy Res. Soc. Sci. 2018, 40, 23–35. [Google Scholar] [CrossRef]
- Fortes, P.; Alvarenga, A.; Seixas, J.; Rodrigues, A.M.A. Long-term energy scenarios: Bridging the gap between socio-economic storylines and energy modeling. Technol. Forecast. Soc. Chang. 2015, 91, 161–178. [Google Scholar] [CrossRef]
- Geels, F.W. Technological transitions as evolutionary reconfiguration processes: A multi-level perspective and a case-study. Res. Policy 2002, 31, 1257–1274. [Google Scholar] [CrossRef] [Green Version]
- Kraus, S.; Schiavone, F.; Pluzhnikova, A.; Invernizzi, A.C. Digital transformation in healthcare: Analyzing the current state-of-research. J. Bus. Res. 2021, 123, 557–567. [Google Scholar] [CrossRef]
- Lupton, D. Health promotion in the digital era: A critical commentary. Health Promot. Int. 2015, 30, 174–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koivumäki, T.; Pekkarinen, S.; Lappi, M.; Väisänen, J.; Juntunen, J.; Pikkarainen, M. Consumer adoption of future MyData-based preventive ehealth services: An acceptance model and survey study. J. Med. Internet Res. 2017, 19, e429. [Google Scholar] [CrossRef] [PubMed]
- Mäkinen, M. Digital empowerment as a process for enhancing citizens’ participation. E-Learn. Digit. Media 2006, 3, 381–395. [Google Scholar] [CrossRef]
- Honka, A.; Kaipainen, K.; Hietala, H.; Saranummi, N. Rethinking health: ICT-enabled services to empower people to manage their health. IEEE Rev. Biomed. Eng. 2011, 4, 119–139. [Google Scholar] [CrossRef]
- Xie, B. Effects of an eHealth literacy intervention for older adults. J. Med. Internet Res. 2011, 13, e90. [Google Scholar] [CrossRef] [Green Version]
- Leväsluoto, J.; Hyytinen, K.; Toivonen, M. Child and family services in the digital era. New opportunities for multiprofessional collaboration and the empowerment of users. Eur. Rev. Serv. Econ. Manag. 2017, 4, 17–47. [Google Scholar] [CrossRef]
- Whitson, J.R. Gaming the quantified self. Surveill. Soc. 2013, 11, 163–176. [Google Scholar] [CrossRef]
- Lupton, D. Quantified sex: A critical analysis of sexual and reproductive self-tracking using apps. Cult. Health Sex. 2015, 17, 440–453. [Google Scholar] [CrossRef]
- Kaipainen, K. Design and Evaluation of Online and Mobile Applications for Stress Management and Healthy Eating. Ph.D. Dissertation, Tampere University of Technology, Tampere, Finland, VTT Publications 55, Espoo, Finland, 2014. [Google Scholar]
- Harjumaa, M.; Absetz, P.; Ermes, M.; Mattila, E.; Männikkö, R.; Tilles-Tirkkonen, T.; Lintu, N.; Schwab, U.; Umer, A.; Leppänen, J.; et al. Internet-based lifestyle intervention to prevent type 2 diabetes through healthy habits: Design and 6-month usage results of randomized controlled trial. JMIR Diabetes 2020, 5, e15219. [Google Scholar] [CrossRef]
- Kivisaari, S.; Saari, E.; Lehto, J.; Kokkinen, L.; Saranummi, N. System innovations in the making: Hybrid actors and the challenge of up-scaling. Technol. Anal. Strat. Manag. 2013, 25, 187–201. [Google Scholar] [CrossRef]
- Health Care in Finland. Ministry of Social Affairs and Health, Finland. Brochures 2eng. 2013. Available online: http://julkaisut.valtioneuvosto.fi/bitstream/handle/10024/69930/URN_ISBN_978-952-00-3395-8.pdf (accessed on 1 August 2018).
- Lindström, J.; Tuomilehto, J. The diabetes risk score: A practical tool to predict type 2 diabetes risk. Diabetes Care 2003, 26, 725–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindström, J.; Peltonen, M.; Eriksson, J.G.; Ilanne-Parikka, P.; Aunola, S.; Keinänen-Kiukaanniemi, S.; Uusitupa, M.; Tuomilehto, J. For the Finnish diabetes prevention study (DPS). Improved lifestyle and decreased diabetes risk over 13 years: Long-term follow-up of the randomised Finnish diabetes prevention study (DPS). Diabetologia 2013, 56, 284–293. [Google Scholar] [CrossRef] [Green Version]
- Elzen, B.; Geels, F.W.; Green, K. System Innovation and the Transition to Sustainability: Theory, Evidence and Policy; Edward Elgar Publishing: Cheltenham, UK, 2004. [Google Scholar]
- Geels, F. From sectoral systems of innovation to socio-technical systems: Insights about dynamics and change from sociology and institutional theory. Res. Policy 2004, 33, 897–920. [Google Scholar] [CrossRef]
- Geels, F.W. Major system change through stepwise reconfiguration: A multi-level analysis of the transformation of American factory production (1850–1930). Technol. Soc. 2006, 28, 445–476. [Google Scholar] [CrossRef]
- Geels, F.W.; Schot, J. Typology of sociotechnical transition pathways. Res. Policy 2007, 36, 399–417. [Google Scholar] [CrossRef]
- Geels, F.W.; Kern, F.; Fuchs, G.; Hinderer, N.; Kungl, G.; Mylan, J.; Neukirch, M.; Wassermann, S. The enactment of socio-technical transition pathways: A reformulated typology and a comparative multi-level analysis of the German and UK low-carbon electricity transitions (1990–2014). Res. Policy 2016, 45, 896–913. [Google Scholar] [CrossRef]
- Hammond, G.P.; Howard, H.R.; Jones, C.I. The energy and environmental implications of UK more electric transition pathways: A whole systems perspective. Energy Policy 2013, 52, 103–116. [Google Scholar] [CrossRef]
- Foxon, T.J. Transition pathways for a UK low carbon electricity future. Energy Policy 2013, 52, 10–24. [Google Scholar] [CrossRef]
- Papachristos, G.; Sofianos, A.; Adamides, E. System interactions in socio-technical transitions: Extending the multi-level perspective. Environ. Innov. Soc. Transit. 2013, 7, 53–69. [Google Scholar] [CrossRef]
- Rosenbloom, D.; Berton, H.; Meadowcroft, J. Framing the sun: A discursive approach to understanding multi-dimensional interactions within socio-technical transitions through the case of solar electricity in Ontario, Canada. Res. Policy 2016, 45, 1275–1290. [Google Scholar] [CrossRef]
- Rosenbloom, D. Framing low-carbon pathways: A discursive analysis of contending storylines surrounding the phase-out of coal-fired power in Ontario. Environ. Innov. Soc. Transit. 2018, 27, 129–145. [Google Scholar] [CrossRef]
- Rogge, K.S.; Pfluger, B.; Geels, F.W. Transformative policy mixes in socio-technical scenarios: The case of the low-carbon transition of the German electricity system (2010–2050). Technol. Forecast. Soc. Chang. 2020, 151, 119259. [Google Scholar] [CrossRef]
- Pel, B.; Raven, R.; van Est, R. Transitions governance with a sense of direction: Synchronization challenges in the case of the dutch ‘Driverless Car’ transition. Technol. Forecast. Soc. Chang. 2020, 160, 120244. [Google Scholar] [CrossRef]
- Foxon, T.J.; Hammond, G.; Pearson, P.J. Developing transition pathways for a low carbon electricity system in the UK. Technol. Forecast. Soc. Chang. 2010, 77, 1203–1213. [Google Scholar] [CrossRef] [Green Version]
- Trutnevytea, E.; Strachana, N.; Bartonb, J.; O’Gradyc, A.; Ogunkunled, D.; Pudjiantoe, D.; Robertson, E. Linking storylines with multiple models: An interdisciplinary analysis of the UK power system transition. Technol. Forecast. Soc. Chang. 2014, 29, 26–42. [Google Scholar] [CrossRef] [Green Version]
- Köhler, J.; Turnheim, B.; Hodson, M. Low carbon transitions pathways in mobility: Applying the MLP in a combined case study and simulation bridging analysis of passenger transport in the Netherlands. Technol. Forecast. Soc. Chang. 2020, 151, 119314. [Google Scholar] [CrossRef] [Green Version]
- Turnheim, B.; Berkhout, F.; Geels, F.; Hof, A.; McMeekin, A.; Nykvist, B.; van Vuuren, D. Evaluating sustainability transitions pathways: Bridging analytical approaches to address governance challenges. Glob. Environ. Chang. 2015, 35, 239–253. [Google Scholar] [CrossRef] [Green Version]
- Caro, J.; Briggs, A.; Siebert, U.; Kuntz, K.M. Modeling Good Research Practices Task Force. Modeling good research practices—Overview: A report of the ISPOR-SMDM modeling good research practices task force-1. Med. Decis. Mak. 2012, 32, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.; Russell, L.B.; Paltiel, A.D.; Chambers, M.; McEwan, P.; Krahn, M. Modeling good research practices task force. Conceptualizing a model: A report of the ISPOR-SMDM modeling good research practices task force-2. Med. Decis. Mak. 2012, 32, 678–689. [Google Scholar] [CrossRef]
- Siebert, U.; Alagoz, O.; Bayoumi, A.M.; Jahn, B.; Owens, D.K.; Cohen, D.J.; Kuntz, K.M. Modeling good research practices task force. State-transition modeling: A report of the ISPOR-SMDM modeling good research practices task force-3. Med. Decis. Mak. 2012, 32, 690–700. [Google Scholar] [CrossRef] [PubMed]
- Briggs, A.H.; Weinstein, M.C.; Fenwick, E.A.; Karnon, J.; Sculpher, M.J.; Paltiel, A.D. Modeling good research practices task force. Model parameter estimation and uncertainty analysis: A report of the ISPOR-SMDM modeling good research practices task force-6. Value Health 2012, 15, 835–842. [Google Scholar] [CrossRef] [Green Version]
- Eddy, D.M.; Hollingworth, W.; Caro, J.; Tsevat, J.; McDonald, K.M.; Wong, J.B. Modeling good research practices task force. Model transparency and validation: A report of the ISPOR-SMDM modeling good research practices task force-7. Med. Decis. Mak. 2012, 32, 733–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigfrids, A.; Leväsluoto, J.; Kohl, J. Hyvinvoinnin Edistäminen nyt! StopDia-Hankkeen Toimijahaastatteluiden Antia; VTT Technical Research Centre of Finland; VTT Technology: Espoo, Finland, 2018. [Google Scholar]
- Ryu, B.; Kim, N.; Heo, E.; Yoo, S.; Lee, K.; Hwang, H.; Kim, J.-W.; Kim, Y.; Lee, J.; Jung, S.Y.; et al. Impact of an electronic health record-integrated personal health record on patient participation in health care: Development and randomized controlled trial of myHealthKeeper. J. Med. Internet Res. 2017, 19, e401. [Google Scholar] [CrossRef] [Green Version]
- Svensson, M.; Hult, M.; Van Der Mark, M.; Grotta, A.; Jonasson, J.; Von Hausswolff-Juhlin, Y.; Rössner, S.; Lagerros, Y.T. The change in eating behaviors in a web-based weight loss program: A longitudinal analysis of study completers. J. Med. Internet Res. 2014, 16, e234. [Google Scholar] [CrossRef]
- Imanaka, M.; Ando, M.; Kitamura, T.; Kawamura, T.; Funk, K.; Langrial, S.; Gardiner, P. Effectiveness of web-based self-disclosure peer-to-peer support for weight loss: Randomized controlled trial. J. Med. Internet Res. 2013, 15, e136. [Google Scholar] [CrossRef]
- Block, G.; Azar, K.M.; Romanelli, R.J.; Block, T.J.; Hopkins, D.; Carpenter, H.A.; Dolginsky, M.S.; Hudes, M.L.; Palaniappan, L.P.; Block, C.H. Diabetes prevention and weight loss with a fully automated behavioral intervention by email, web, and mobile phone: A randomized controlled trial among persons with prediabetes. J. Med. Internet Res. 2015, 17, e240. [Google Scholar] [CrossRef] [PubMed]
- The National FINRISK Study. National Institute of Health and Welfare. Available online: https://thl.fi/en/web/thlfi-en/research-and-expertwork/population-studies/the-national-finrisk-study (accessed on 12 September 2018).
- Taylor, K.S.; Heneghan, C.J.; Farmer, A.J.; Fuller, A.M.; Adler, A.I.; Aronson, J.K.; Stevens, R.J. All-cause and cardiovascular mortality in middle-aged people with type 2 diabetes compared with people without diabetes in a large U.K. primary care database. Diabetes Care 2013, 36, 2366–2371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Ministry of Finance. Action Programme on eServices and eDemocracy (SADe Programme). Available online: https://vm.fi/sade?p_p_id=56_INSTANCE_fybJlIiDK2er&p_p_lifecycle=0&p_p_state=normal&p_p_mode=view&p_p_col_id=column-2&p_p_col_count=2&_56_INSTANCE_fybJlIiDK2er_languageId=en_US (accessed on 12 September 2018).
- FIN D2D. Finnish Diabetes Association. Available online: https://www.diabetes.fi/en/finnish_diabetes_association/dehko/fin-d2d (accessed on 12 September 2018).
- Lindström, J.; Louheranta, A.; Mannelin, M.; Rastas, M.; Salminen, V.; Eriksson, J.; Uusitupa, M.; Tuomilehto, J. The Finnish diabetes prevention study (DPS): Lifestyle intervention and 3-year results on diet and physical activity. Diabetes Care 2003, 26, 3230–3236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haverinen, J.; Keränen, N.; Falkenbach, P.; Maijala, A.; Kolehmainen, T.; Reponen, J. Digi-HTA: Health technology assessment framework for digital healthcare services. Finn. J. eHealth eWelfare 2019, 11, 326–341. [Google Scholar] [CrossRef] [Green Version]
- Larsen, L.B.; Sondergaard, J.; Thomsen, J.L.; Halling, A.; Sønderlund, A.L.; Christensen, J.R.; Thilsing, T. Step-wise approach to prevention of chronic diseases in the Danish primary care sector with the use of a personal digital health profile and targeted follow-up–an assessment of attendance. BMC Public Health 2019, 19, 1–14. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Occupations Include | N 23 | Expertise Areas Include | N 23 |
|---|---|---|---|
| Medical adviser | 4 | Diabetes | 4 |
| Senior Researcher | 2 | Social-, health- or labor policy | 4 |
| Business manager | 1 | Occupational healthcare | 3 |
| Chairman of the board | 1 | Public health | 2 |
| Chief Director | 1 | Human Resources | 1 |
| Chief occupational health physician | 1 | Cardiology | 1 |
| Chief physician | 1 | Funding Preparations | 1 |
| Chief public health nurse | 1 | Healthy physical activity | 1 |
| Executive manager | 1 | Solution architect | 1 |
| Expert Pharmacist | 1 | Immigrant health | 1 |
| Grants officer | 1 | Nutrition research and obesity prevention | 1 |
| HR manager | 1 | Political science | 1 |
| Medical director | 1 | Public administration | 1 |
| Program Director | 1 | Youth- and physical education policy | 1 |
| Project manager | 1 | ||
| Research Director (tai: CEO) | 1 | ||
| Secretary General | 1 | ||
| Senior physician | 1 | ||
| Social policy specialist | 1 |
| Scenarios | Description of Scenario |
|---|---|
| Scenario 1 | A digitally supported prevention program targeted to all Finnish adults at 45–75 years of age |
| Scenario 2 | A digitally supported prevention program targeted to all 45–75-year-old adults at the moderately elevated risk of T2D (FINDRISC Score > 12) |
| Scenario 3 | A digitally supported prevention program targeted to all 45–75-year-old adults at the high elevated risk of T2D (FINDRISC Score > 15) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leväsluoto, J.; Kohl, J.; Sigfrids, A.; Pihlajamäki, J.; Martikainen, J. Digitalization as an Engine for Change? Building a Vision Pathway towards a Sustainable Health Care System by Using the MLP and Health Economic Decision Modelling. Sustainability 2021, 13, 13007. https://doi.org/10.3390/su132313007
Leväsluoto J, Kohl J, Sigfrids A, Pihlajamäki J, Martikainen J. Digitalization as an Engine for Change? Building a Vision Pathway towards a Sustainable Health Care System by Using the MLP and Health Economic Decision Modelling. Sustainability. 2021; 13(23):13007. https://doi.org/10.3390/su132313007
Chicago/Turabian StyleLeväsluoto, Johanna, Johanna Kohl, Anton Sigfrids, Jussi Pihlajamäki, and Janne Martikainen. 2021. "Digitalization as an Engine for Change? Building a Vision Pathway towards a Sustainable Health Care System by Using the MLP and Health Economic Decision Modelling" Sustainability 13, no. 23: 13007. https://doi.org/10.3390/su132313007