

Factors Contributing to Surgical Site Infections: A Comprehensive Systematic Review of Etiology and Risk Factors
 , , , , ,
, , , , ,
Abstract
:1. Introduction
1.1. Background
1.2. Risk Factors
1.3. Etiology
1.4. Objectives
2. Materials and Methods
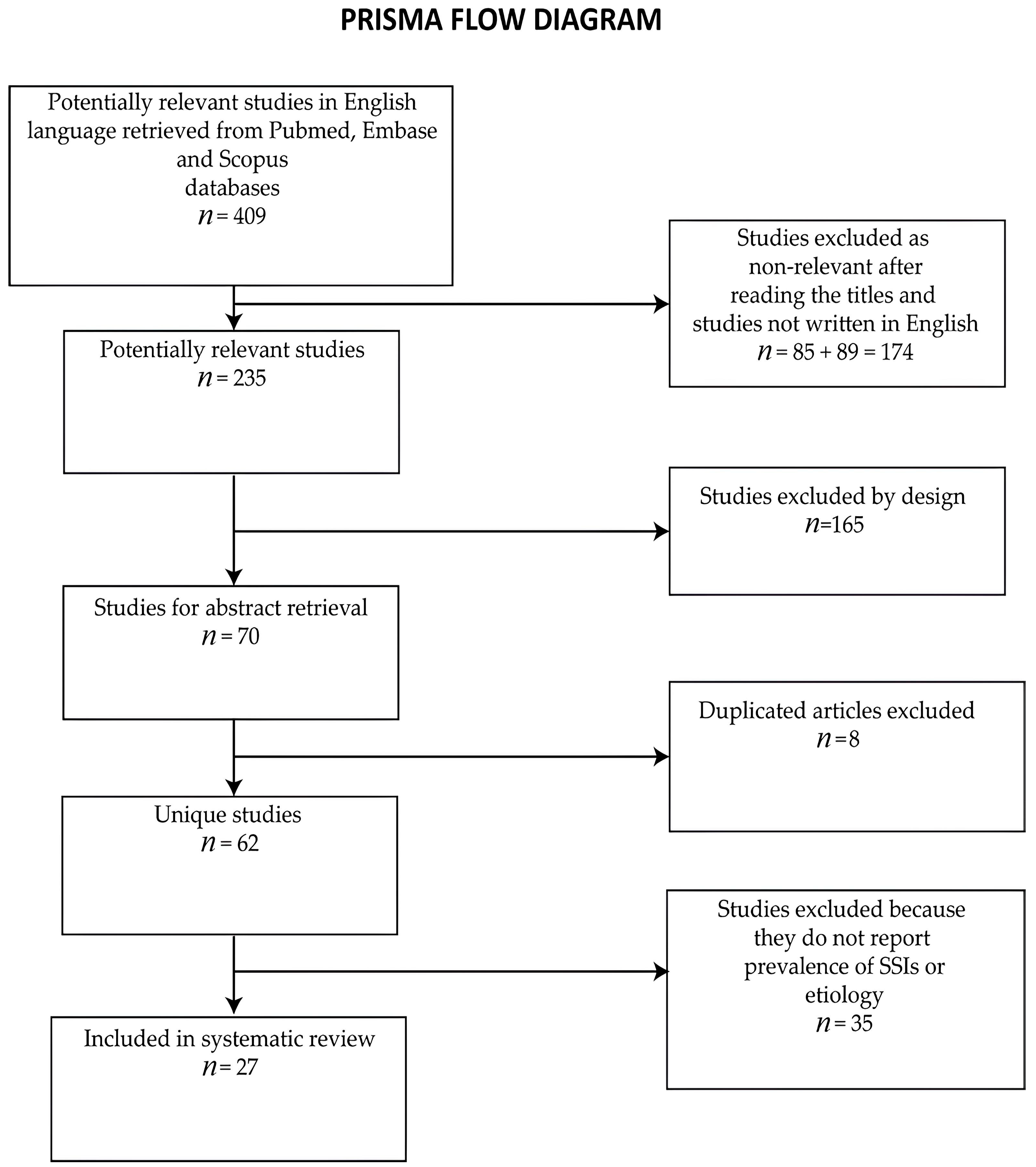
2.1. Study Design and Selection Criteria
2.2. Data Extraction
2.3. Quality Assessment
3. Results

{kind=link}
{kind=link}
| Authors | Type of Surgery | Period of Study, Region, Centers Involved | No. of Participants | SSI Rate | Etiology | Quality Score |
|---|---|---|---|---|---|---|
| Elliman et al., 2017 [11] | Cardiac surgery Orthopedic surgery Colorectal surgery Vascular surgery Hysterectomy | 2008–2013 USA National Veterans Affairs cohort | 70,101 | 3.5% | S. aureus MRSA—7.9% S. aureus MSSA—24.1% CNS—12% Streptococcus spp.—0% Enterobacteriaceae—40% | 13 |
| Shah et al., 2020 [12] | General surgery | 2013–2018 India 1 hospital | 55,553 | 1.% (0.97% in clean surgeries and 0.03% in contaminated surgeries) | S. aureus—12% S. epidermidis—7% Streptococcus spp.—0% P. aeruginosa—13% K. pneumoniae—17% E. coli—19% | 11 |
| Hou et al., 2020 [16] | Colorectal surgery | 2015–2018 China 19 hospitals | 3663 | 3.7% Superficial SSIs 2.1% Deep SSIs 0.7% | S. aureus—3.7% S. epidermidis—0% Streptococcus spp.—0% P. aeruginosa—6.00% K. pneumoniae—7.5% E. coli—40.3% | 12 |
| Panos et al., 2021 [17] | Colorectal surgery | 2019–2021 Greece 1 hospital | 133 | 21.8% Superficial SSIs 15% Deep SSIs 6% Organ space 0.8% | S. aureus 4% CNS- Streptococcus spp.— P. aeruginosa— Klebsiella pneumoniae—12% E. coli—44% | 12 |
| Du et al., 2019 [18] | Colorectal surgery | 2015–2016 China 26 hospitals | 5729 | 3.6% Radical resection of colon SSI 2.6% Superficial SSIs 0.9% Deep SSIs 0.6% Organ 1.1% Radical resection of rectum SSI 5.1% Superficial SSIs 2.3% Deep SSIs 1.1% Organ 1.7% | Radical resection of colon: S. aureus— Streptococcus spp.— P. aeruginosa—13.2% Klebsiella pneumoniae—7.9% E. coli—55.3% Radical resection of rectum: S. aureus— Streptococcus spp.— Pseudomonas aeruginosa—6.2% Klebsiella pneumoniae—6.2% E. coli—36.9% | 12 |
| Alkaaki et al., 2019 [19] | Abdominal surgery | 2016 Saudi Arabia 1 hospital | 337 | 16.3% | Gram-positive cocci—38% P. aeruginosa—14% K. pneumoniae—20% E. coli—52% | 11 |
| Benito et al., 2014 [20] | Knee/hip arthroplasty | 2004–2010 Barcelona 1 hospital | 2333 (knee/hip arthroplasties) | 4.2% | S. aureus MRSA—28.6% S. aureus MSSA—6.8% CNS—24.2% P. aeruginosa—11.1% | 12 |
| Taherpour et al., 2021 [21] | Orthopedic surgery | 2017–2018 Iran 6 hospitals | 503 | - | E. coli—11.1% S. aureus—23% CNS—8% P. aeruginosa—7% Klebsiella spp.—22% E. coli—8% | 11 |
| Slowik et al., 2020 [22] | Knee/Hip Arthroplasties | 2012–2018 Poland 1 hospital | 2340 | 1.6% | S. aureus—18.9% CNS—35.1% Streptococcus spp.— P. aeruginosa— Klebsiella pneumoniae—10.8% E. coli—2.7% | 11 |
| Meng et al., 2020 [23] | Foot and ankle surgery | 2015–2018 China 1 hospital | 1201 | 2.1% (1.3% superficial SSI; 0.8% deep SSI) | S. aureus MRSA—23.1% S. aureus MSSA—19.2% CNS—7.7% Streptococcus spp.— P. aeruginosa— Klebsiella spp.— E. coli—7.7% | 11 |
| Mathur et al., 2022 [24] | Orthopedic surgery | 2018–2019 India 1 hospital | 850 | 5.5% | S. aureus—36% CNS—2% Streptococcus pyogenes—4% P. aeruginosa—8% Klebsiella pneumoniae—10% E. coli—12% | 12 |
| Nagaya et al., 2017 [25] | Orthopedic surgery | 1987–2012 Brazil 1 hospital | 158 | 9.5% | S. aureus—12.5% CNS—6.2% Streptococcus spp.— Pseudomonas aeruginosa 18.7% Klebsiella pneumoniae— E. coli— | 12 |
| Maritati et al., 2022 [26] | Orthopedic surgery | 2019–2020 Italy 1 hospital | 760 | 3.3% | S. aureus—10% CNS—40% Streptococcus spp.— Pseudomonas aeruginosa—10% Klebsiella pneumoniae – E. coli— | 11 |
| Lu et al., 2019 [27] | Orthopedic surgery | 2013–2017 China 3 hospitals | 895 | 4% Deep SSIs 1.5% Superficial SSIs 2.5% | S. aureus—42.1% CNS—15.8% Streptococcus spp.— Pseudomonas aeruginosa—5.3% Klebsiella pneumoniae— E. coli— | 11 |
| Wang et al., 2018 [28] | Orthopedic surgery | 2014–2017 China 1 hospital | 725 | 9.7% Deep SSIs 2.9% Superficial SSIs 6.8% | S. aureus—19.7% S. aureus MRSA—2.1% CNS Streptococcus spp.— Pseudomonas aeruginosa 1.5% Klebsiella pneumoniae— E. coli—6.1% | 11 |
| Sun et al., 2018 [29] | Orthopedic surgery | 2015–2016 China 3 hospitals | 1511 | 4.4% Deep SSIs 1.3% Superficial SSIs 3.1% | MRSA—29.7% CNS Streptococcus spp.— Pseudomonas aeruginosa Klebsiella pneumoniae— E. coli— | 11 |
| Kahl et al., 2019 [30] | Cardiac surgery | 2018 Spain 1 hospital | 150 | 29.3% | S. aureus—8.8% CNS—8% P. aeruginosa—15.6% Klebsiella spp.—20.6% E. coli—4.2% | 12 |
| AlFawaz et al., 2022 [31] | Vascular surgery | 2014–2019 Kuwait 1 hospital | 391 | 14% | S. aureus—25.5% CNS— Streptococcus spp.— P. aeruginosa—34% Klebsiella pneumoniae— E. coli—13% | 11 |
| Banjanovic et al., 2022 [32] | Cardiac surgery | 2015–2020 Bosnia 1 hospital | 15 | 14.9% | MRSA—9% CNS— Streptococcus spp.— P. aeruginosa—4.5% Klebsiella pneumoniae—13% E. coli—4.5% | 10 |
| Zejnullahu et al., 2019 [33] | Obstetrics | 2018 Kosovo 1 hospital | 325 | 9.9% | S. aureus—28.1% CNS—6.3% Streptococcus spp.— P. aeruginosa—3.1% Klebsiella spp.—3.1% E. coli—9.4% | 12 |
| Gupta et al., 2021 [34] | Obstetrics surgery | 2016 India 1 hospital | 611 | 10.3% 66.7% superficial SSI; 27% deep SSI; 6.3% organ space | MSSA—42% MRSA—3% Streptococcus spp.— P. aeruginosa—5% Klebsiella pneumoniae—24% E. coli—13% | 12 |
| Zhang et al., 2022 [35] | Spinal surgery | 2010–2020 China 1 hospital | 521 | 1.8% | S. aureus Streptococcus spp.— Pseudomonas aeruginosa 10% Klebsiella pneumoniae— E. coli 6.7% | 12 |
| Pei et al., 2021 [36] | Spinal surgery | 2016–2019 China 1 hospital | 1269 | 3.4% | S. aureus MRSA—16% MRCNS—48% Streptococcus spp.— Pseudomonas aeruginosa Klebsiella pneumoniae— | 11 |
| Hamdeh et al., 2014 [37] | Neurosurgery | 2010 Sweden | 448 | 4.3% | ESBL—32% E. coli S. aureus—21.7% CNS—34.8% | 12 |
| Pereira et al., 2017 [38] | Neurosurgery | 2011–2014 Spain 1 hospital | 521 | 4.9% | S. aureus—23.1% S. epidermidis—23.1% Streptococcus spp.—11.5% P. aeruginosa—11.5% K. pneumoniae—11.5% E. coli—3.9% | 11 |
| Kolpa et al., 2019 [39] | Neurosurgery | 2003- 2017 Poland 1 hospital | 10,332 | 1.5% | S. aureus—49.7% CNS—3.2% Streptococcus spp.—1.9% P. aeruginosa—4.5% Klebsiella spp.—1.3% E. coli—5.7% | 12 |
| Morikane, 2018 [40] | Thoracic surgery | 2012–2014 Japan Japan Nosocomial Infections Surveillance database | 3538 | 4.1% | MRSA—19.2% CNS—16.4% Streptococcus spp.— P. aeruginosa— Klebsiella pneumoniae— E. coli—3.4% | 12 |
3.1. Colorectal Surgery
3.2. Abdominal Surgery
3.3. Orthopedic Surgery
3.4. Cardiovascular and Cardiac Surgery
3.5. Obstetrics Surgery
3.6. Neurosurgery
3.7. Spinal Surgery
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Center for Disease Control Surgical Site Infection Event (SSI). Available online: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf (accessed on 24 August 2023).
- Kathju, S.; Nistico, L.; Tower, I.; Lasko, L.A.; Stoodley, P. Bacterial biofilms on implanted suture material are a cause of surgical site infection. Surg. Infect. 2014, 15, 592–600. [Google Scholar] [CrossRef] [PubMed]
- Doyle, D.J.; Hendrix, J.M.; Garmon, E.H. American Society of Anesthesiologists Classification; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- European Centre for Disease Prevention and Control Surveillance of Surgical Site Infections and Prevention Indicators in European Hospitals—HAISSI Protocol. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-surgical-site-infections-and-prevention-indicators-european (accessed on 24 August 2023).
- European Center for Disease Prevention and Control Healthcare-Associated Infections: Surgical Site Infections—Annual Epidemiological Report for 2017. Available online: https://www.ecdc.europa.eu/en/publications-data/healthcare-associated-infections-surgical-site-infections-annual-1 (accessed on 12 June 2023).
- Kean, J. The effects of smoking on the wound healing process. J. Wound Care 2010, 19, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Trevejo-Nunez, G.; Kolls, J.K.; de Wit, M. Alcohol Use As a Risk Factor in Infections and Healing: A Clinician’s Perspective. Alcohol Res. Curr. Rev. 2015, 37, 177–184. [Google Scholar]
- Pinchera, B.; Buonomo, A.R.; Schiano Moriello, N.; Scotto, R.; Villari, R.; Gentile, I. Update on the Management of Surgical Site Infections. Antibiotics 2022, 11, 1608. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Guidelines for the Prevention of Surgical Site Infection, 2nd ed.; World Health Organization: Geneva, Switzerland, 2018; ISBN 9789241550475.
- Shakir, A.; Abate, D.; Tebeje, F.; Weledegebreal, F. Magnitude of Surgical Site Infections, Bacterial Etiologies, Associated Factors and Antimicrobial Susceptibility Patterns of Isolates among Post-Operative Patients in Harari Region Public Hospitals, Harar, Eastern Ethiopia. Infect. Drug Resist. 2021, 14, 4629. [Google Scholar] [CrossRef] [PubMed]
- Branch-Elliman, W.; Ripollone, J.E.; O’Brien, W.J.; Itani, K.M.F.; Schweizer, M.L.; Perencevich, E.; Strymish, J.; Gupta, K. Risk of Surgical Site Infection, Acute Kidney Injury, and Clostridium Difficile Infection following Antibiotic Prophylaxis with Vancomycin plus a Beta-Lactam versus Either Drug Alone: A National Propensity-Score-Adjusted Retrospective Cohort Study. PLoS Med. 2017, 14, e1002340. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Singhal, T.; Naik, R.; Thakkar, P. Predominance of Multidrug-Resistant Gram-Negative Organisms as Cause of Surgical Site Infections at a Private Tertiary Care Hospital in Mumbai, India. Indian J. Med. Microbiol. 2020, 38, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Edmiston, C.E.; McBain, A.J.; Roberts, C.; Leaper, D. Clinical and Microbiological Aspects of Biofilm-Associated Surgical Site Infections. Adv. Exp. Med. Biol. 2015, 830, 47–67. [Google Scholar] [CrossRef]
- Allegranzi, B.; Bischoff, P.; de Jonge, S.; Kubilay, N.Z.; Zayed, B.; Gomes, S.M.; Abbas, M.; Atema, J.J.; Gans, S.; van Rijen, M.; et al. New WHO Recommendations on Preoperative Measures for Surgical Site Infection Prevention: An Evidence-Based Global Perspective. Lancet Infect. Dis. 2016, 16, e276–e287. [Google Scholar] [CrossRef]
- Study Quality Assessment Tools, NHLBI, NIH. NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 29 August 2023).
- Hou, T.Y.; Gan, H.Q.; Zhou, J.F.; Gong, Y.J.; Li, L.Y.; Zhang, X.Q.; Meng, Y.; Chen, J.R.; Liu, W.J.; Ye, L.; et al. Incidence of and Risk Factors for Surgical Site Infection after Colorectal Surgery: A Multiple-Center Prospective Study of 3663 Consecutive Patients in China. Int. J. Infect. Dis. 2020, 96, 676–681. [Google Scholar] [CrossRef]
- Panos, G.; Mulita, F.; Akinosoglou, K.; Liolis, E.; Kaplanis, C.; Tchabashvili, L.; Vailas, M.; Maroulis, I. Risk of Surgical Site Infections after Colorectal Surgery and the Most Frequent Pathogens Isolated: A Prospective Single-Centre Observational Study. Med. Glas. 2021, 18. [Google Scholar] [CrossRef]
- Du, M.; Liu, B.; Li, M.; Cao, J.; Liu, D.; Wang, Z.; Wang, Q.; Xiao, P.; Zhang, X.; Gao, Y.; et al. Multicenter Surveillance Study of Surgical Site Infection and Its Risk Factors in Radical Resection of Colon or Rectal Carcinoma. BMC Infect. Dis. 2019, 19, 411. [Google Scholar] [CrossRef] [PubMed]
- Alkaaki, A.; Al-Radi, O.O.; Khoja, A.; Alnawawi, A.; Alnawawi, A.; Maghrabi, A.; Altaf, A.; Aljiffry, M. Surgical Site Infection Following Abdominal Surgery: A Prospective Cohort Study. Can. J. Surg. 2019, 62, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Benito, N.; Franco, M.; Coll, P.; Gálvez, M.L.; Jordán, M.; López-Contreras, J.; Pomar, V.; Monllau, J.C.; Mirelis, B.; Gurguí, M. Etiology of Surgical Site Infections after Primary Total Joint Arthroplasties. J. Orthop. Res. 2014, 32, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Taherpour, N.; Mehrabi, Y.; Seifi, A.; Eshrati, B.; Hashemi Nazari, S.S. Epidemiologic Characteristics of Orthopedic Surgical Site Infections and Under-Reporting Estimation of Registries Using Capture-Recapture Analysis. BMC Infect. Dis. 2021, 21, 3. [Google Scholar] [CrossRef]
- Słowik, R.; Kołpa, M.; Wałaszek, M.; Różańska, A.; Jagiencarz-Starzec, B.; Zieńczuk, W.; Kawik, Ł.; Wolak, Z.; Wójkowska-Mach, J. Epidemiology of Surgical Site Infections Considering the NHSN Standardized Infection Ratio in Hip and Knee Arthroplasties. Int. J. Environ. Res. Public Health 2020, 17, 3167. [Google Scholar] [CrossRef] [PubMed]
- Meng, J.; Zhu, Y.; Li, Y.; Sun, T.; Zhang, F.; Qin, S.; Zhao, H. Incidence and Risk Factors for Surgical Site Infection Following Elective Foot and Ankle Surgery: A Retrospective Study. J. Orthop. Surg. Res. 2020, 15, 449. [Google Scholar] [CrossRef]
- Mathur, P.; Mittal, S.; Trikha, V.; Srivastav, S.; Pandey, R.M.; Katyal, S.; Singh, P.; Khurana, S.; Malhotra, R.; Walia, K. Surveillance for Surgical Site Infections in Orthopedic Trauma Surgeries at an Indian Hospital. Indian J. Med. Microbiol. 2022, 40, 268–273. [Google Scholar] [CrossRef]
- Nagaya, L.H.; Salles, M.J.C.; Takikawa, L.S.C.; Fregoneze, M.; Doneux, P.; Silva, L.A.D.; Sella, G.D.V.; Miyazaki, A.N.; Checchia, S.L. Infections after Shoulder Arthroplasty Are Correlated with Higher Anesthetic Risk Score: A Case-Control Study in Brazil. Braz. J. Infect. Dis. 2017, 21, 613–619. [Google Scholar] [CrossRef]
- Maritati, M.; Trentini, A.; Chemello, D.; Mazzoni, E.; Cervellati, C.; Zanoli, G.A.; Contini, C.; De Rito, G. Predictive Factors of Surgical Site Infection in Prosthetic Joint Surgery: A Prospective Study on 760 Arthroplasties. Mediat. Inflamm. 2022, 2022, 2150804. [Google Scholar] [CrossRef]
- Lu, K.; Zhang, J.; Cheng, J.; Liu, H.; Yang, C.; Yin, L.; Wang, H.; You, X.; Qu, Q. Incidence and Risk Factors for Surgical Site Infection after Open Reduction and Internal Fixation of Intra-Articular Fractures of Distal Femur: A Multicentre Study. Int. Wound J. 2019, 16, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Pei, H.; Chen, M.; Wang, H. Incidence and Predictors of Surgical Site Infection after ORIF in Calcaneus Fractures, a Retrospective Cohort Study. J. Orthop. Surg. Res. 2018, 13, 293. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Wang, H.; Tang, Y.; Zhao, H.; Qin, S.; Xu, L.; Xia, Z.; Zhang, F. Incidence and Risk Factors for Surgical Site Infection after Open Reduction and Internal Fixation of Ankle Fracture. Medicine 2018, 97, e9901. [Google Scholar] [CrossRef] [PubMed]
- Kahl, E.R.P.Y.; Brião, R.D.C.; Costa, L.M.D.; Silveira, L.R.; Moraes, M.A.P.D. Ambulatory Setting of Patients with Surgical Site Infections after a Cardiac Intervention. Rev. Gaúcha Enferm. 2019, 40, e20180200. [Google Scholar] [CrossRef] [PubMed]
- AlFawaz, A.A.; Safar, A.H.; Al-Mukhaizeem, A.; Kamal, E.; Alloush, M.; Hanbal, E. Risk Factors for Wound Infections after Vascular Surgery: Kuwait Experience. Med. Princ. Pract. 2022, 31, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Banjanovic, B.; Karabdic, I.H.; Straus, S.; Berberovic, B.H.; Djedovic, M.; Granov, N. Deep Sternal Wound Infection After Open-Heart Cardiac Surgery and Vacuum-Assisted Closure Therapy: A Single-Center Study. Med. Arch. 2022, 76, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Zejnullahu, V.A.; Zejnullahu, V.A.; Isjanovska, R.; Sejfija, Z. Surgical Site Infections after Cesarean Sections at the University Clinical Center of Kosovo: Rates, Microbiological Profile and Risk Factors. BMC Infect. Dis. 2019, 19, 752. [Google Scholar] [CrossRef]
- Gupta, S.; Manchanda, V.; Sachdev, P.; Kumar Saini, R.; Joy, M. Study of Incidence and Risk Factors of Surgical Site Infections in Lower Segment Caesarean Section Cases of Tertiary Care Hospital of North India. Indian J. Med. Microbiol. 2021, 39, 1–5. [Google Scholar] [CrossRef]
- Zhang, T.; Lian, X.; Chen, Y.; Cai, B.; Xu, J. Clinical Outcome of Postoperative Surgical Site Infections in Patients with Posterior Thoracolumbar and Lumbar Instrumentation. J. Hosp. Infect. 2022, 128, 26–35. [Google Scholar] [CrossRef]
- Pei, H.; Wang, H.; Chen, M.; Ma, L.; Liu, G.; Ding, W. Surgical Site Infection after Posterior Lumbar Interbody Fusion and Instrumentation in Patients with Lumbar Degenerative Disease. Int. Wound J. 2021, 18, 608–615. [Google Scholar] [CrossRef]
- Abu Hamdeh, S.; Lytsy, B.; Ronne-Engström, E. Surgical Site Infections in Standard Neurosurgery Procedures-a Study of Incidence, Impact and Potential Risk Factors. Br. J. Neurosurg. 2014, 28, 270–275. [Google Scholar] [CrossRef] [PubMed]
- López Pereira, P.; Díaz-Agero Pérez, C.; López Fresneña, N.; Las Heras Mosteiro, J.; Palancar Cabrera, A.; Rincón Carlavilla, Á.L.; Aranaz Andrés, J.M. Epidemiology of Surgical Site Infection in a Neurosurgery Department. Br. J. Neurosurg. 2017, 31, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Kołpa, M.; Wałaszek, M.; Różańska, A.; Wolak, Z.; Wójkowska-Mach, J. Epidemiology of Surgical Site Infections and Non-Surgical Infections in Neurosurgical Polish Patients—Substantial Changes in 2003–2017. Int. J. Environ. Res. Public Health 2019, 16, 911. [Google Scholar] [CrossRef] [PubMed]
- Morikane, K. Epidemiology and Risk Factors Associated with Surgical Site Infection Following Surgery on Thoracic Aorta. Epidemiol. Infect. 2018, 146, 1841–1844. [Google Scholar] [CrossRef]
- Kiran, R.P.; El-Gazzaz, G.H.; Vogel, J.D.; Remzi, F.H. Laparoscopic Approach Significantly Reduces Surgical Site Infections after Colorectal Surgery: Data from National Surgical Quality Improvement Program. J. Am. Coll. Surg. 2010, 211, 232–238. [Google Scholar] [CrossRef]
- Gandaglia, G.; Ghani, K.R.; Sood, A.; Meyers, J.R.; Sammon, J.D.; Schmid, M.; Varda, B.; Briganti, A.; Montorsi, F.; Sun, M.; et al. Effect of Minimally Invasive Surgery on the Risk for Surgical Site Infections: Results from the National Surgical Quality Improvement Program (NSQIP) Database. JAMA Surg. 2014, 149, 1039–1044. [Google Scholar] [CrossRef]


| Classification | Definition | Criteria |
|---|---|---|
| Superficial Incisional SSI | Infection occurs within 30 days after the operation and involves only skin and subcutaneous tissue of the incision. | Purulent drainage, with or without laboratory confirmation, from the superficial incision. |
| Deep Incisional SSI | Infection occurs within 30 days after the operation and involves deep soft tissues, such as fascial and muscle layers. | Purulent drainage from the deep incision but not from the organ/space component of the surgical site. |
| Organ/Space SSI | Infection occurs within 30 days after the operation and involves any part of the anatomy (e.g., organs or spaces) other than the incision, which was opened or manipulated during the operation. | Infection involving any part of the anatomy (e.g., organs or spaces) other than the incision, which was opened or manipulated during the operation. |
| Surgical Procedure | Common Risk Factors |
|---|---|
| Orthopedic Surgery | Prolonged surgery duration, foreign material (e.g., implants), inadequate sterilization |
| Cardiac Surgery | Use of heart–lung machine, lengthy operations, blood transfusions |
| Abdominal Surgery | Emergency procedures, contamination of the surgical site, prolonged preoperative stay |
| Transplant Surgery | Immunosuppressive therapy, allograft contamination, technical issues |
| Neurosurgery | Shaving of the surgical site, dural exposure, implant use |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bucataru, A.; Balasoiu, M.; Ghenea, A.E.; Zlatian, O.M.; Vulcanescu, D.D.; Horhat, F.G.; Bagiu, I.C.; Sorop, V.B.; Sorop, M.I.; Oprisoni, A.; et al. Factors Contributing to Surgical Site Infections: A Comprehensive Systematic Review of Etiology and Risk Factors. Clin. Pract. 2024, 14, 52-68. https://doi.org/10.3390/clinpract14010006
Bucataru A, Balasoiu M, Ghenea AE, Zlatian OM, Vulcanescu DD, Horhat FG, Bagiu IC, Sorop VB, Sorop MI, Oprisoni A, et al. Factors Contributing to Surgical Site Infections: A Comprehensive Systematic Review of Etiology and Risk Factors. Clinics and Practice. 2024; 14(1):52-68. https://doi.org/10.3390/clinpract14010006
Chicago/Turabian StyleBucataru, Alexandra, Maria Balasoiu, Alice Elena Ghenea, Ovidiu Mircea Zlatian, Dan Dumitru Vulcanescu, Florin George Horhat, Iulia Cristina Bagiu, Virgiliu Bogdan Sorop, Madalina Ioana Sorop, Andrada Oprisoni, and et al. 2024. "Factors Contributing to Surgical Site Infections: A Comprehensive Systematic Review of Etiology and Risk Factors" Clinics and Practice 14, no. 1: 52-68. https://doi.org/10.3390/clinpract14010006