
Improvement in Left and Right Ventricular Function after Introduction of SGLT2 Inhibitors in Heart Failure Outpatients with Reduced Ejection Fraction
 ,
,
Abstract
:1. Introduction
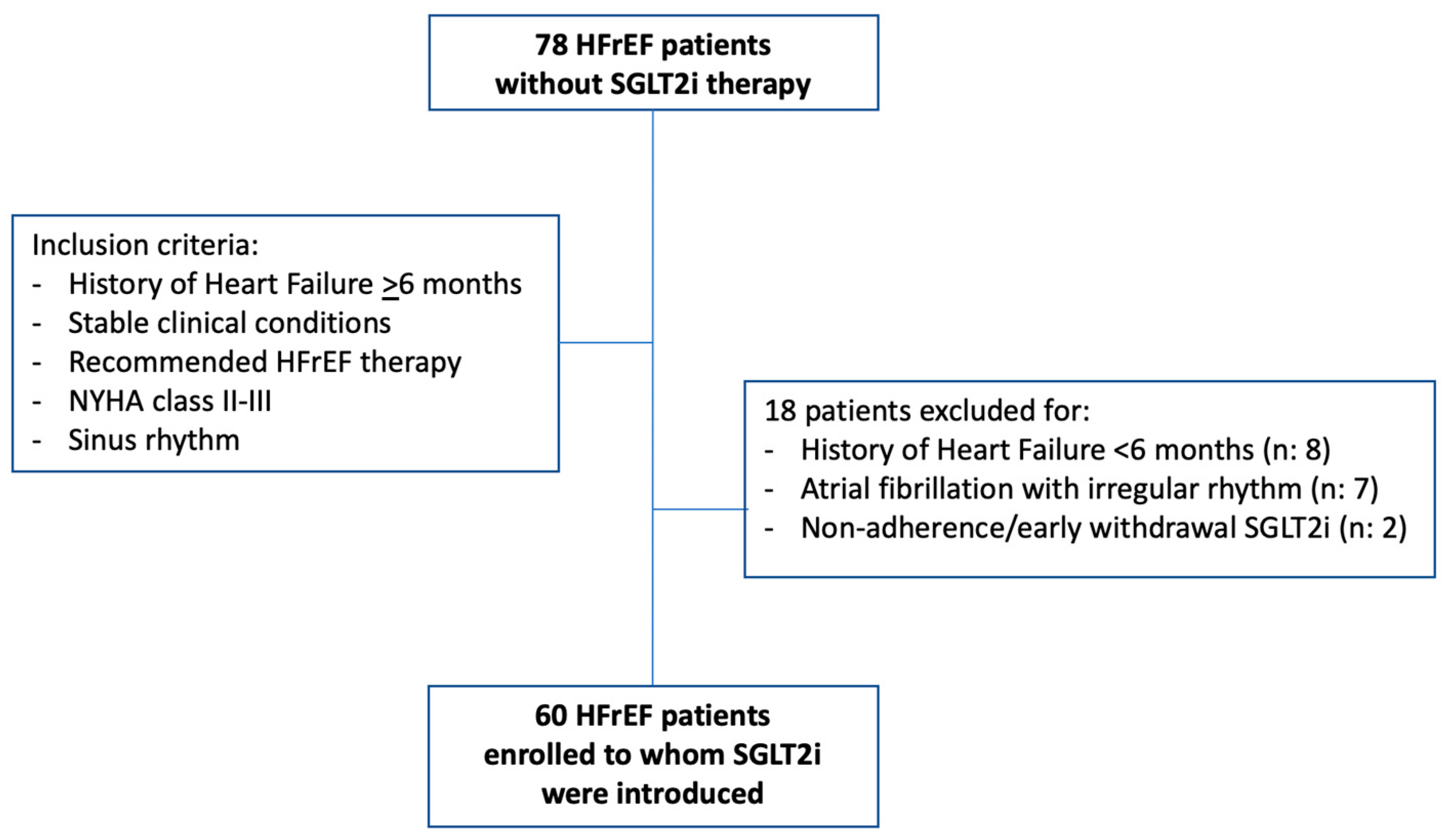
2. Materials and Methods
- -
- Medical visit and ECG: history of ischemic heart disease, arterial hypertension, diabetes mellitus, estimated glomerular filtration rate (GFR), NYHA class, arterial pressure, and rhythm and heart rate at ECG were recorded. The dose of heart failure classes of drugs was evaluated as follows: for ACEi, the equivalent enalapril dose was calculated according to the following proportions: enalapril 20 mg/day equivalent to ramipril 10 mg/day, zofenopril 30 mg/day, and lisinopril 20 mg/day. For ARBs, the equivalent valsartan dose was calculated according to the following proportions: valsartan 320 mg/day equivalent to losartan 100 mg/day, and candesartan 32 mg/day [3]. For beta-blockers, the equivalent bisoprolol dose was calculated according to the following proportions: bisoprolol 10 mg/day equivalent to carvedilol 50 mg/day, nebivolol 10 mg/day, metoprolol tartrate 200 mg/day. Finally, the sacubitril/valsartan dose of 24/26 mg b.i.d. was computed as 100 mg/day, that of 49/51 mg b.i.d. as 200 mg/day, and that of 97/103 mg b.i.d. as 400 mg/day.
- -
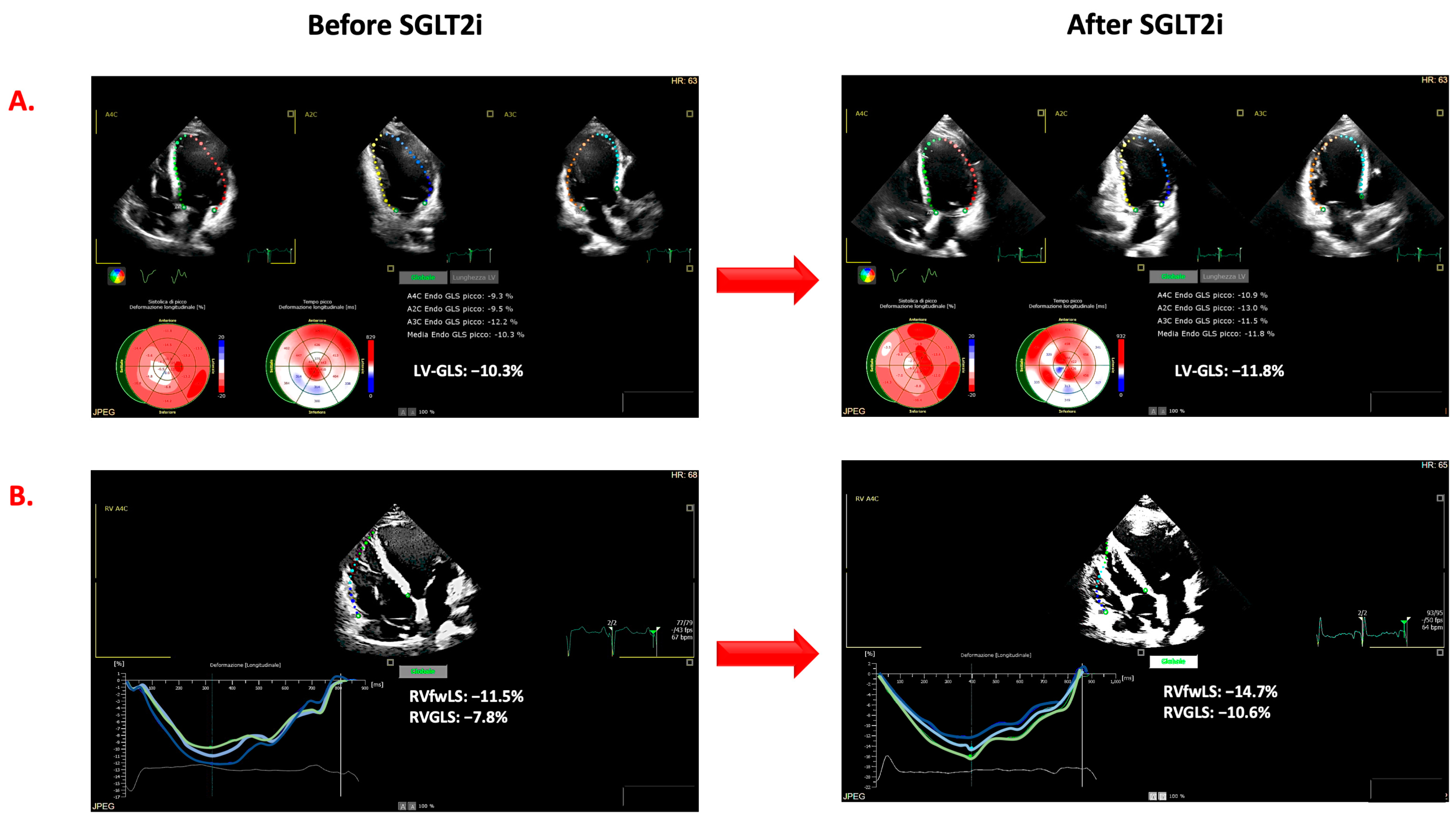
- Echocardiographic examinations. Echocardiographic examinations were analyzed by two operators (G.A., R.P.) who were in the blind from the time of the evaluation as well as from the results of the other examinations of each patient. In accordance with current recommendations, LVEF was calculated on the basis of left ventricular end-diastolic volume (LVEDV) and end-systolic volume (LVESV) (Simpson’s rule). The ratio between E and e′ (E/e′) was based on the peak of the E wave (E) at pulsed Doppler and the TDI peak of early diastolic velocity peak (e′) at the level of the septal and lateral mitral annulus [18]. Mitral (MR) and tricuspid (TR) regurgitation were evaluated and quantified by arbitrary units (a.u. range from 0 to 4). Tricuspid annular plane systolic excursion (TAPSE) was assessed in order to evaluate RV systolic function. As shown in Figure 1, the strain measurements were obtained by the AutoStrain application of the Philips EPIQ CVx ultrasound system. From the “off-cart” analysis of the stored examinations, the LV global longitudinal strain (LV-GLS) was measured by the analysis of standard two-, three-, and four-chamber views and the average values of all segments. Using the RV-focused four-chamber view, the RV function was assessed by automatically calculating the global longitudinal strain of the right ventricle (RV-GLS) and that of the free wall (RV-fwLS). Although the AutoStrain application allows for semiautomatic evaluation, the region of interest, the automatically detected cardiac cycle, and the segmental analyses’ accuracy were verified and corrected when appropriate. Ventricular strain measurements are expressed as negative values, i.e., the lower the value, the better the ventricular function. For this reason, in the manuscript, we indicated more negative values than those determined at baseline as improved ventricular systolic strain. LV reverse remodeling was defined as a reduction of LVESV greater than 15% from baseline [19], whereas a significant improvement in LVEF was defined as an absolute increase of more than 5% from baseline. The improvement in LV-GLS, RV-GLS, and RV-fwLS was defined as a relative change of more than 10% from baseline [20].
3. Results
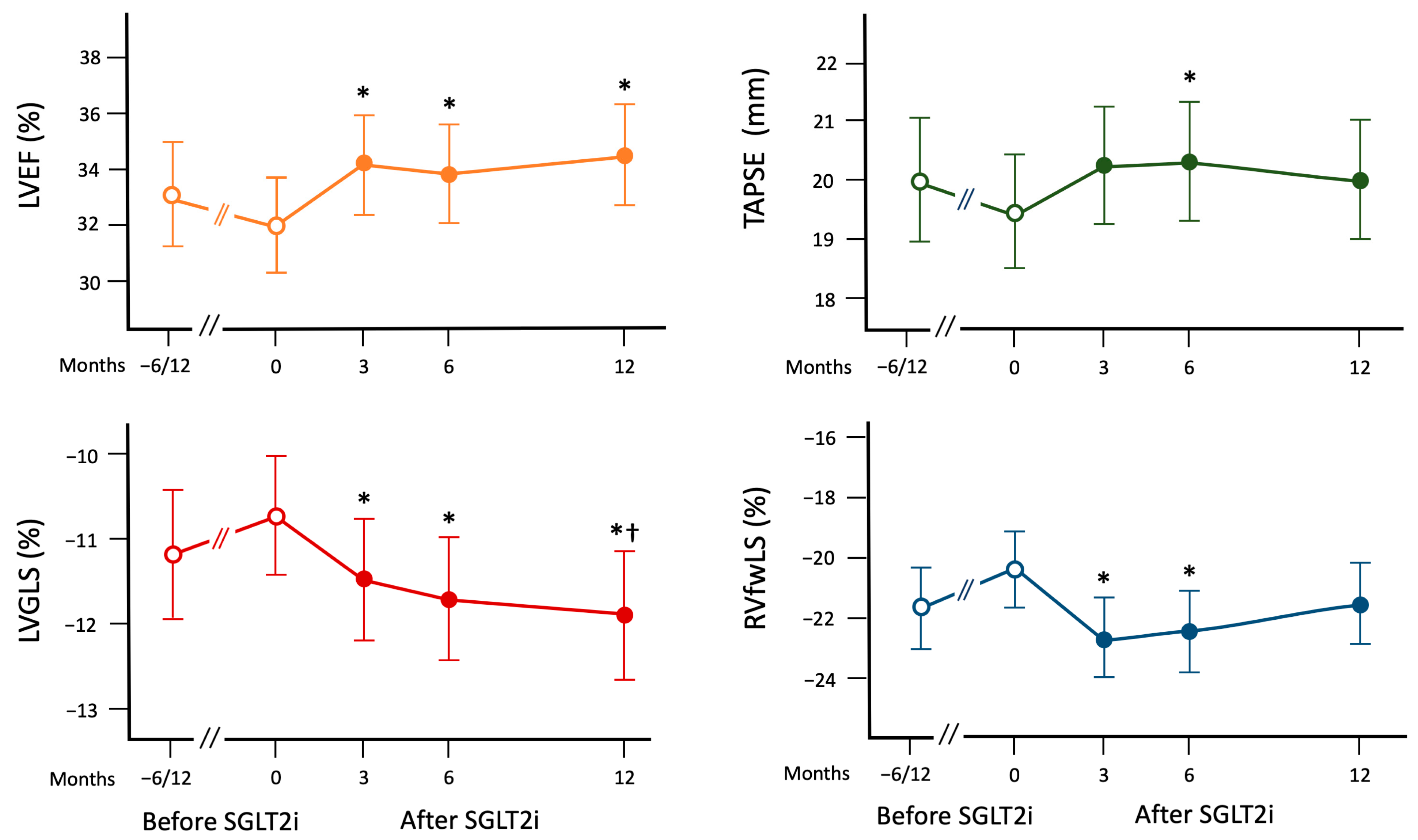
3.1. Changes in Echocardiographic Parameters before SGLT2i Introduction
3.2. Changes in Echocardiographic Parameters after the Introduction of SGLT2i
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Vallon, V.; Verma, S. Effects of SGLT2 Inhibitors on Kidney and Cardiovascular Function. Annu. Rev. Physiol. 2021, 83, 503–528. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; McMurray, J.J.V. SGLT2 inhibitors and mechanisms of cardiovascular benefit: A state-of-the-art review. Diabetologia 2018, 61, 2108–2117. [Google Scholar] [CrossRef]
- Marton, A.; Kaneko, T.; Kovalik, J.P.; Yasui, A.; Nishiyama, A.; Kitada, K.; Titze, J. Organ protection by SGLT2 inhibitors: Role of metabolic energy and water conservation. Nat. Rev. Nephrol. 2021, 17, 65–77. [Google Scholar] [CrossRef]
- Natali, A.; Nesti, L.; Tricò, D.; Ferrannini, E. Effects of GLP-1 receptor agonists and SGLT-2 inhibitors on cardiac structure and function: A narrative review of clinical evidence. Cardiovasc. Diabetol. 2021, 20, 196. [Google Scholar] [CrossRef]
- Gronda, E.; Vanoli, E.; Iacoviello, M.; Caldarola, P.; Gabrielli, D.; Tavazzi, L. The Benefit of Sodium-Glucose Co-Transporter Inhibition in Heart Failure: The Role of the Kidney. Int. J. Mol. Sci. 2022, 23, 11987. [Google Scholar] [CrossRef]
- Packer, M. Critical Reanalysis of the Mechanisms Underlying the Cardiorenal Benefits of SGLT2 Inhibitors and Reaffirmation of the Nutrient Deprivation Signaling/Autophagy Hypothesis. Circulation 2022, 146, 1383–1405. [Google Scholar] [CrossRef] [PubMed]
- Ferrannini, E.; Baldi, S.; Frascerra, S.; Astiarraga, B.; Heise, T.; Bizzotto, R.; Mari, A.; Pieber, T.R.; Muscelli, E. Shift to Fatty Substrate Utilization in Response to Sodium-Glucose Cotransporter 2 Inhibition in Subjects without Diabetes and Patients with Type 2 Diabetes. Diabetes 2016, 65, 1190–1195. [Google Scholar] [CrossRef] [PubMed]
- Baartscheer, A.; Schumacher, C.A.; Wüst, R.C.; Fiolet, J.W.; Stienen, G.J.; Coronel, R.; Zuurbier, C.J. Empagliflozin decreases myocardial cytoplasmic Na+ through inhibition of the cardiac Na+/H+ exchanger in rats and rabbits. Diabetologia 2017, 60, 568–573. [Google Scholar] [CrossRef]
- Packer, M. How can sodium-glucose cotransporter 2 inhibitors stimulate erythrocytosis in patients who are iron-deficient? Implications for understanding iron homeostasis in heart failure. Eur. J. Heart Fail. 2022, 24, 2287–2296. [Google Scholar] [CrossRef]
- Gamaza-Chulián, S.; Díaz-Retamino, E.; González-Testón, F.; Gaitero, J.C.; Castillo, M.J.; Alfaro, R.; Rodríguez, E.; González-Caballero, E.; Martín-Santana, A. Effect of sodium-glucose cotransporter 2 (SGLT2) inhibitors on left ventricular remodelling and longitudinal strain: A prospective observational study. BMC Cardiovasc. Disord. 2021, 21, 456. [Google Scholar] [CrossRef] [PubMed]
- Hwang, I.-C.; Cho, G.-Y.; Yoon, Y.E.; Park, J.J.; Park, J.-B.; Lee, S.-P.; Kim, H.-K.; Kim, Y.-J.; Sohn, D.-W. Different effects of SGLT2 inhibitors according to the presence and types of heart failure in type 2 diabetic patients. Cardiovasc. Diabetol. 2020, 19, 69. [Google Scholar] [CrossRef] [PubMed]
- Mustapic, I.; Bakovic, D.; Susilovic-Grabovac, Z.; Borovac, J.A. Left Ventricular Systolic Function after 3 Months of SGLT2 Inhibitor Therapy in Heart Failure Patients with Reduced Ejection Fraction. J. Cardiovasc. Transl. Res. 2023, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mustapic, I.; Bakovic, D.; Susilovic Grabovac, Z.; Borovac, J.A. Impact of SGLT2 Inhibitor Therapy on Right Ventricular Function in Patients with Heart Failure and Reduced Ejection Fraction. J. Clin. Med. 2023, 12, 42. [Google Scholar] [CrossRef]
- Theofilis, P.; Antonopoulos, A.S.; Katsimichas, T.; Oikonomou, E.; Siasos, G.; Aggeli, C.; Tsioufis, K.; Tousoulis, D. The impact of SGLT2 inhibition on imaging markers of cardiac function: A systematic review and meta-analysis. Pharmacol. Res. 2022, 180, 106243. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Himelman, R.B.; Cassidy, M.M.; Landzberg, J.S.; Schiller, N.B. Reproducibility of quantitative two-dimensional echocardiography. Am. Heart J. 1988, 115, 425–431. [Google Scholar] [CrossRef]
- Di Terlizzi, V.; Barone, R.; Manuppelli, V.; Correale, M.; Casavecchia, G.; Goffredo, G.; Pellegrino, P.; Puteo, A.; Ieva, R.; Di Biase, M.; et al. Influence of Heart Rate on Left and Right Ventricular Longitudinal Strain in Patients with Chronic Heart Failure. Appl. Sci. 2022, 12, 556. [Google Scholar] [CrossRef]
- Januzzi, J.L., Jr.; Prescott, M.F.; Butler, J.; Felker, G.M.; Maisel, A.S.; McCague, K.; Camacho, A.; Piña, I.L.; Rocha, R.A.; Shah, A.M.; et al. Association of Change in N-Terminal Pro-B-Type Natriuretic Peptide Following Initiation of Sacubitril-Valsartan Treatment with Cardiac Structure and Function in Patients with Heart Failure with Reduced Ejection Fraction. JAMA 2019, 322, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Bao, J.; Kan, R.; Chen, J.; Xuan, H.; Wang, C.; Li, D.; Xu, T. Combination pharmacotherapies for cardiac reverse remodeling in heart failure patients with reduced ejection fraction: A systematic review and network meta-analysis of randomized clinical trials. Pharmacol. Res. 2021, 169, 105573. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Claggett, B.L.; Jhund, P.S.; Cunningham, J.W.; Ferreira, J.P.; Zannad, F.; Packer, M.; Fonarow, G.C.; McMurray, J.J.; Solomon, S.D. Estimating lifetime benefits of comprehensive disease-modifying phar-macological therapies in patients with heart failure with reduced ejection fraction: A comparative analysis of three random-ised controlled trials. Lancet 2020, 396, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Monteagudo-Vela, M.; Tindale, A.; Monguió-Santín, E.; Reyes-Copa, G.; Panoulas, V. Right ventricular failure: Current strategies and future development. Front. Cardiovasc. Med. 2023, 10, 998382. [Google Scholar] [CrossRef]
- Zhang, J.; Du, L.; Qin, X.; Guo, X. Effect of Sacubitril/Valsartan on the Right Ventricular Function and Pulmonary Hypertension in Patients with Heart Failure with Reduced Ejection Fraction: A Systematic Review and Meta-Analysis of Observational Studies. J. Am. Heart Assoc. 2022, 11, e024449. [Google Scholar] [CrossRef]
- Dandel, M.; Lehmkuhl, H.; Knosalla, C.; Suramelashvili, N.; Hetzer, R. Strain and strain rate imaging by echocardiog-raphy—Basic concepts and clinical applicability. Curr. Cardiol. Rev. 2009, 5, 133–148. [Google Scholar] [CrossRef]
- Kalam, K.; Otahal, P.; Marwick, T.H. Prognostic implications of global LV dysfunction: A systematic review and meta-analysis of global longitudinal strain and ejection fraction. Heart 2014, 100, 1673–1680. [Google Scholar] [CrossRef]
- Anastasiou, V.; Papazoglou, A.S.; Moysidis, D.V.; Daios, S.; Tsalikakis, D.; Giannakoulas, G.; Karamitsos, T.; Delgado, V.; Ziakas, A.; Kamperidis, V. The prognostic value of right ventricular longitudinal strain in heart failure: A systematic review and meta-analysis. Heart Fail. Rev. 2023; Epub ahead of print. [Google Scholar] [CrossRef]
- Alcidi, G.; Goffredo, G.; Correale, M.; Brunetti, N.D.; Iacoviello, M. Brain Natriuretic Peptide Biomarkers in Current Clinical and Therapeutic Scenarios of Heart Failure. J. Clin. Med. 2022, 11, 3192. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | |
|---|---|
| Number | 60 |
| Age (years) | 62 ± 15 |
| Males, n (%) | 48 (80) |
| Median time from diagnosis of CHF (years) | 7 |
| Ischemic etiology, n (%) | 27 (45) |
| Diabetes mellitus, n (%) | 13 (22) |
| Arterial Hypertension, n (%) | 35 (58) |
| NYHA class II, n (%) | 46 (75) |
| III, n (%) | 14 (25) |
| BMI (kg/m2) | 27 ± 5 |
| SAP (mm Hg) | 118 ± 17 |
| Heart rate (beats/minute) | 68 ± 11 |
| LVEF (%) | 32 ± 6 |
| Creatinine (mg/dL) | 1.18 ± 0.34 |
| GFR-EPI (mL/min/1.73 m2) | 66 ± 22 |
| Concomitant therapy at the enrollment | |
| Sacubitril/Valsartan, n (% among treated) | 41 (68) |
| Sacubitril/Valsartan > 50% target dose | 14 (34) |
| ACE-I/ARB, n (%) | 19 (32) |
| ACE-I/ARB ≥ 50% target dose, n (% among treated) | 4 (21) |
| Beta-blockers (%) | 59 (98) |
| Beta-blocker ≥ 50% target dose, n (% among treated) | 35 (59) |
| MRA, n (%) | 51 (85) |
| MRA dose ≥ 100% target dose, n (% among treated) | 30 (59) |
| Ivabradine, n (%) | 17 (28) |
| Loop diuretics, n (%) | 39 (64) |
| Furosemide-equivalent dose (mg/day) | 54 ± 50 |
| ICD, n (%) | 55 (90) |
| CRT, n (%) | 37 (22) |
| Baseline Values | Relative Changes from T0 | |||
|---|---|---|---|---|
| T0 | T3 | T6 | T12 | |
| LVEDV | 155 ± 58 mL | −4.7 ± 14.6% | −3.6 ± 17.3 | −4.4 ± 17.3 |
| LVEF | 32 ± 6% | +8.2 ± 18.0% * | +8.5 ± 24.9% * | +10.4 ± 26.1% * |
| LV-GLS | −10.7 ± 2.7% | −8.7 ± 21.1% * | −12.2 ± 26.0% * | −14.1 ± 33.2% * |
| MR | 1.4 ± 0.7 a.u. | +1.6 ± 36.9% | +3.8 ± 40.8% | +10.3 ± 45.4% |
| LAVI | 36 ± 18 mL/m2 | +5.4 ± 33.5% | +10.2 ± 39.1% | +0.1 ± 33.8% |
| E/e′ | 9.6 ± 3.2 | +3.3 ± 38% | +3.2 ± 38% | +17.9 ± 53.8% |
| TAPSE | 19.5 ± 3.8 mm | +6.4 ± 19.8% | +4.8 ± 18.9% * | +4.3 ± 18.2% |
| RV-GLS | −14.6 ± 3.3% | −15.6 ± 32.1% * | −9.9 ± 27.8% * | −11.0 ± 29.5% |
| RV-fwLS | −20.4 ± 4.3% | −13.5 ± 22.6% * | −10.9 ± 22.3% * | −8.9 ± 25.7% |
| TR | 1.3 ± 0.6 a.u. | +2.9 ± 37.6% | −2.1 ± 37.1% | +5.6 ± 49.1% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alcidi, G.; Pugliese, R.; Ioannoni, S.; Romano, M.; Palmieri, G.; Tabella, E.; Correale, M.; Di Biase, M.; Brunetti, N.D.; Iacoviello, M. Improvement in Left and Right Ventricular Function after Introduction of SGLT2 Inhibitors in Heart Failure Outpatients with Reduced Ejection Fraction. Clin. Pract. 2023, 13, 1303-1312. https://doi.org/10.3390/clinpract13060116
Alcidi G, Pugliese R, Ioannoni S, Romano M, Palmieri G, Tabella E, Correale M, Di Biase M, Brunetti ND, Iacoviello M. Improvement in Left and Right Ventricular Function after Introduction of SGLT2 Inhibitors in Heart Failure Outpatients with Reduced Ejection Fraction. Clinics and Practice. 2023; 13(6):1303-1312. https://doi.org/10.3390/clinpract13060116
Chicago/Turabian StyleAlcidi, Gianmarco, Rosanna Pugliese, Sara Ioannoni, Matteo Romano, Gianpaolo Palmieri, Erika Tabella, Michele Correale, Matteo Di Biase, Natale Daniele Brunetti, and Massimo Iacoviello. 2023. "Improvement in Left and Right Ventricular Function after Introduction of SGLT2 Inhibitors in Heart Failure Outpatients with Reduced Ejection Fraction" Clinics and Practice 13, no. 6: 1303-1312. https://doi.org/10.3390/clinpract13060116