
Use of Oral Anticoagulants in Patients with Atrial Fibrillation: Preliminary Data from the Italian Atrial Fibrillation (ITALY-AF) Registry

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
- -
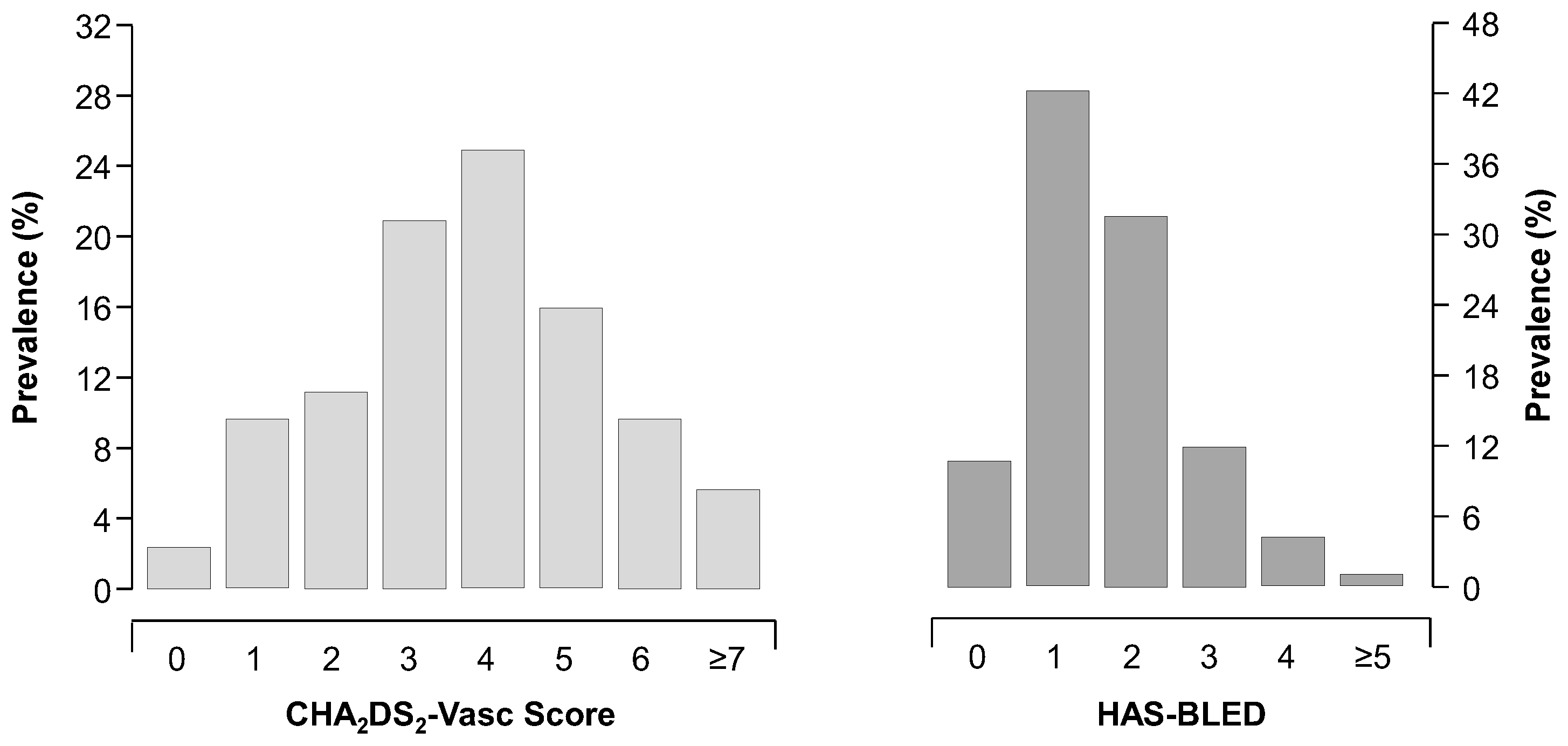
- HAS-BLED (hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile international normalized ratio, elderly (> 65 years), drugs/alcohol concomitantly) score to assess the individual bleeding risk of real-world patients with AFIB [13];
- -
- CHA2DS2-VASc score for stroke risk stratification [12].
Statistical Analysis
3. Results
4. Discussion
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Friberg, L.; Bergfeldt, L. Atrial fibrillation prevalence revisited. J. Intern. Med. 2013, 274, 461–468. [Google Scholar] [CrossRef]
- Heeringa, J.; van der Kuip, D.A.; Hofman, A.; Kors, J.A.; van Herpen, G.; Stricker, B.H.; Stijnen, T.; Lip, G.Y.; Witteman, J.C. Prevalence, incidence and lifetime risk of atrial fibrillation: The Rotterdam study. Eur. Heart J. 2006, 27, 949–953. [Google Scholar] [CrossRef]
- Bjorck, S.; Palaszewski, B.; Friberg, L.; Bergfeldt, L. Atrial fibrillation, stroke risk, and warfarin therapy revisited: A population-based study. Stroke 2013, 44, 3103–3108. [Google Scholar] [CrossRef]
- McBride, R.; Stroke Prevention in Atrial Fibrillation Investigators. Stroke Prevention in Atrial Fibrillation Study. Final results. Circulation 1991, 84, 527–539. [Google Scholar] [CrossRef]
- Stroke Prevention in Atrial Fibrillation Investigators. Warfarin versus aspirin for prevention of thromboembolism in atrial fibrillation: Stroke Prevention in Atrial Fibrillation II Study. Lancet 1994, 343, 687–691. [Google Scholar]
- Hart, R.G.; Pearce, L.A.; Aguilar, M.I. Adjusted-dose warfarin versus aspirin for preventing stroke in patients with atrial fibrillation. Ann. Intern. Med. 2007, 147, 590–592. [Google Scholar] [CrossRef]
- Andersson, N.W.; Svanstrom, H.; Lund, M.; Pasternak, B.; Melbye, M. Comparative effectiveness and safety of apixaban, dabigatran, and rivaroxaban in patients with non-valvular atrial fibrillation. Int. J. Cardiol. 2018, 268, 113–119. [Google Scholar] [CrossRef]
- Graham, D.J.; Baro, E.; Zhang, R.; Liao, J.; Wernecke, M.; Reichman, M.E.; Hu, M.; Illoh, O.; Wei, Y.; Goulding, M.R.; et al. Comparative Stroke, Bleeding, and Mortality Risks in Older Medicare Patients Treated with Oral Anticoagulants for Nonvalvular Atrial Fibrillation. Am. J. Med. 2019, 132, 596–604.e511. [Google Scholar] [CrossRef]
- Verdecchia, P.; Angeli, F.; Bartolini, C.; De Filippo, V.; Aita, A.; Di Giacomo, L.; Poltronieri, C.; Lip, G.Y.; Reboldi, G. Safety and efficacy of non-vitamin K oral anticoagulants in non-valvular atrial fibrillation: A Bayesian meta-analysis approach. Expert Opin. Drug Saf. 2015, 14, 7–20. [Google Scholar] [CrossRef]
- Verdecchia, P.; Angeli, F.; Reboldi, G. Hypertension and Atrial Fibrillation: Doubts and Certainties from Basic and Clinical Studies. Circ. Res. 2018, 122, 352–368. [Google Scholar] [CrossRef]
- Apostolakis, S.; Sullivan, R.M.; Olshansky, B.; Lip, G.Y.H. Factors affecting quality of anticoagulation control among patients with atrial fibrillation on warfarin: The SAMe-TT(2)R(2) score. Chest 2013, 144, 1555–1563. [Google Scholar] [CrossRef]
- Lip, G.Y.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; de Vos, C.B.; Crijns, H.J.; Lip, G.Y. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: The Euro Heart Survey. Chest 2010, 138, 1093–1100. [Google Scholar] [CrossRef]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef]
- Steffel, J.; Verhamme, P.; Potpara, T.S.; Albaladejo, P.; Antz, M.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur. Heart J. 2018, 39, 1330–1393. [Google Scholar] [CrossRef]
- Angeli, F.; Reboldi, G.; Garofoli, M.; Ramundo, E.; Poltronieri, C.; Mazzotta, G.; Ambrosio, G.; Verdecchia, P. Atrial fibrillation and mortality in patients with acute myocardial infarction: A systematic overview and meta-analysis. Curr. Cardiol. Rep. 2012, 14, 601–610. [Google Scholar] [CrossRef]
- Angeli, F.; Reboldi, G.; Verdecchia, P. Hypertension, inflammation and atrial fibrillation. J. Hypertens. 2014, 32, 480–483. [Google Scholar] [CrossRef]
- Verdecchia, P.; Angeli, F.; Cavallini, C.; Aita, A.; Turturiello, D.; De Fano, M.; Reboldi, G. Sudden Cardiac Death in Hypertensive Patients. Hypertension 2019, 73, 1071–1078. [Google Scholar] [CrossRef]
- Friberg, L.; Rosenqvist, M.; Lip, G.Y. Net clinical benefit of warfarin in patients with atrial fibrillation: A report from the Swedish atrial fibrillation cohort study. Circulation 2012, 125, 2298–2307. [Google Scholar] [CrossRef]
- Ogilvie, I.M.; Newton, N.; Welner, S.A.; Cowell, W.; Lip, G.Y. Underuse of oral anticoagulants in atrial fibrillation: A systematic review. Am. J. Med. 2010, 123, 638–645.e634. [Google Scholar] [CrossRef]
- Oldgren, J.; Healey, J.S.; Ezekowitz, M.; Commerford, P.; Avezum, A.; Pais, P.; Zhu, J.; Jansky, P.; Sigamani, A.; Morillo, C.A.; et al. Variations in cause and management of atrial fibrillation in a prospective registry of 15,400 emergency department patients in 46 countries: The RE-LY Atrial Fibrillation Registry. Circulation 2014, 129, 1568–1576. [Google Scholar] [CrossRef] [PubMed]
- Clarkesmith, D.E.; Pattison, H.M.; Khaing, P.H.; Lane, D.A. Educational and behavioural interventions for anticoagulant therapy in patients with atrial fibrillation. Cochrane Database Syst. Rev. 2017, 4, CD008600. [Google Scholar] [CrossRef] [PubMed]
- Clarkesmith, D.E.; Pattison, H.M.; Lip, G.Y.; Lane, D.A. Educational intervention improves anticoagulation control in atrial fibrillation patients: The TREAT randomised trial. PLoS ONE 2013, 8, e74037. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Overall (n = 2470) | Men (n = 1374) | Women (n = 1096) | p |
|---|---|---|---|---|
| Age (years) * | 77 (70–83) | 76 (67–82) | 79 (72–85) | <0.0001 |
| Current smokers (%) | 6.8 | 8.7 | 4.5 | <0.0001 |
| Diabetes (%) | 19.2 | 20.1 | 18.1 | 0.212 |
| Body mass index (kg/m2) | 27.2 (4.9) | 27.4 (4.5) | 26.9 (5.3) | 0.011 |
| Office systolic BP (mmHg) | 130 (120–140) | 130 (120–140) | 130 (120–140) | 0.371 |
| Office diastolic BP (mmHg) | 80 (70–85) | 80 (70–85) | 80 (70–82) | 0.155 |
| Hemoglobin (g/dL) | 13.3 (2.1) | 13.8 (2.1) | 12.6 (1.9) | <0.0001 |
| Creatinine (mg/dL) | 1.08 (0.61) | 1.16 (0.62) | 0.98 (0.57) | <0.0001 |
| eGFR < 60 (%) | 35.5 | 28.2 | 44.7 | <0.0001 |
| Serum glucose (mg/dL) | 101 (89–119) | 100 (90–119) | 101 (88–120) | 0.363 |
| Total cholesterol (mg/dL) | 170 (139–198) | 167 (134–194) | 175 (142–202) | 0.0002 |
| LDL cholesterol (mg/dL) | 98 (75–121) | 98 (74–118) | 100 (77–123) | 0.139 |
| Types of AFIB (%) | ||||
| First diagnosed | 16.4 | 14.7 | 18.6 | 0.060 |
| Paroxysmal | 17.3 | 16.5 | 18.3 | for trend |
| Persistent | 28.4 | 29.5 | 27.0 | |
| Long-standing | 2.1 | 2.1 | 2.0 | |
| Permanent | 35.8 | 37.2 | 34.1 | |
| Previous events | ||||
| Myocardial infarction (%) | 14.0 | 17.1 | 10.1 | <0.0001 |
| Pulmonary embolism (%) | 1.8 | 1.2 | 2.6 | 0.010 |
| Stroke (%) | 12.0 | 11.4 | 12.8 | 0.384 |
| Transient ischemic attack (%) | 6.6 | 7.0 | 6.0 | 0.339 |
| Heart failure (%) | 22.1 | 21.4 | 23.0 | 0.334 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angeli, F.; Reboldi, G.; Agnelli, G.; Ambrosio, G.; Capucci, A.; Carreras, G.; Cavallini, C.; Murrone, A.; Vaudo, G.; Zingarini, G.; et al. Use of Oral Anticoagulants in Patients with Atrial Fibrillation: Preliminary Data from the Italian Atrial Fibrillation (ITALY-AF) Registry. Clin. Pract. 2023, 13, 1173-1181. https://doi.org/10.3390/clinpract13050105
Angeli F, Reboldi G, Agnelli G, Ambrosio G, Capucci A, Carreras G, Cavallini C, Murrone A, Vaudo G, Zingarini G, et al. Use of Oral Anticoagulants in Patients with Atrial Fibrillation: Preliminary Data from the Italian Atrial Fibrillation (ITALY-AF) Registry. Clinics and Practice. 2023; 13(5):1173-1181. https://doi.org/10.3390/clinpract13050105
Chicago/Turabian StyleAngeli, Fabio, Gianpaolo Reboldi, Giancarlo Agnelli, Giuseppe Ambrosio, Alessandro Capucci, Giovanni Carreras, Claudio Cavallini, Adriano Murrone, Gaetano Vaudo, Gianluca Zingarini, and et al. 2023. "Use of Oral Anticoagulants in Patients with Atrial Fibrillation: Preliminary Data from the Italian Atrial Fibrillation (ITALY-AF) Registry" Clinics and Practice 13, no. 5: 1173-1181. https://doi.org/10.3390/clinpract13050105