
The Age of Young Nurses Is a Predictor of Burnout Syndrome during the Care of Patients with COVID-19
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
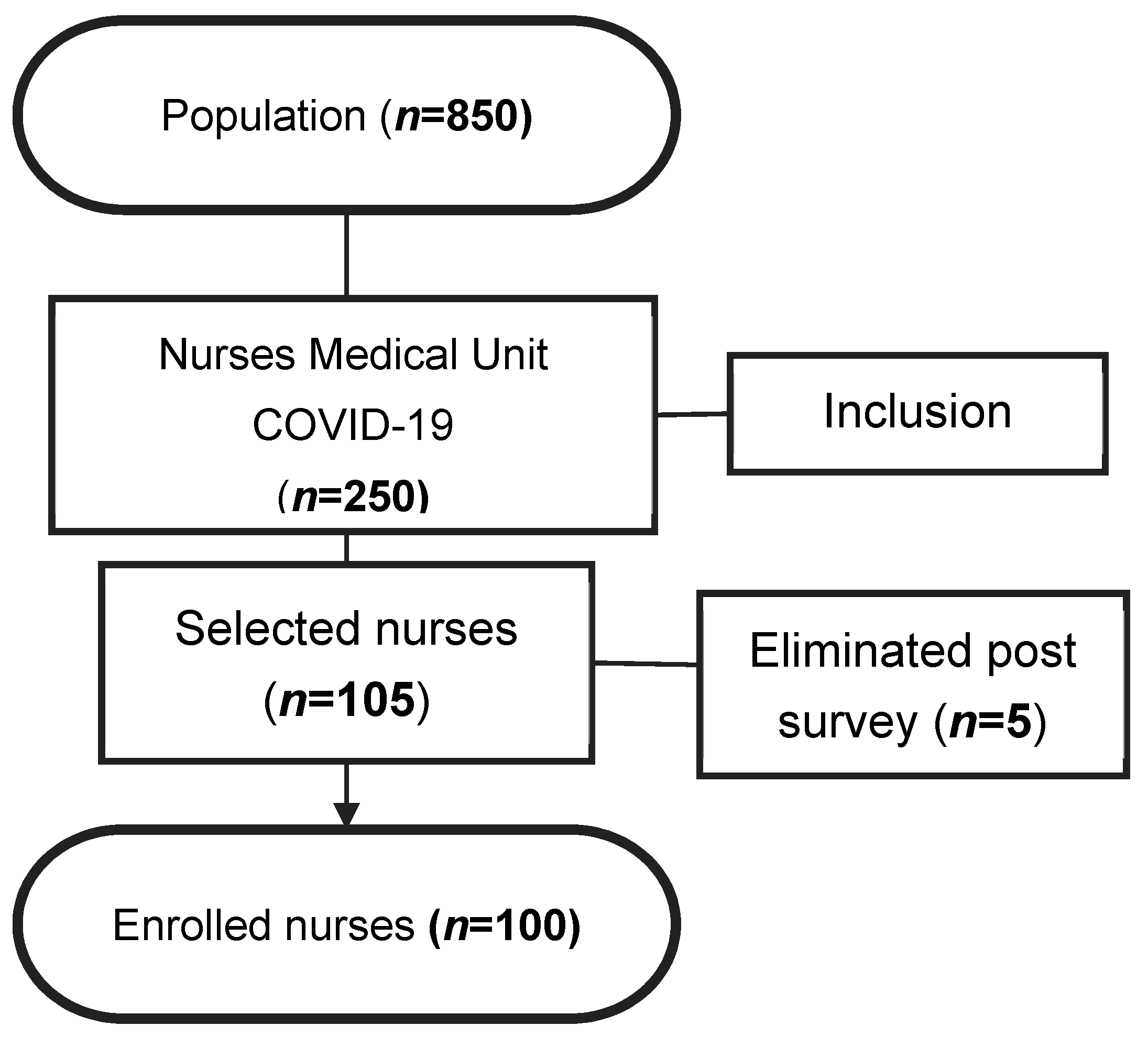
2.2. Population, Inclusion Criteria, and Instruments
2.3. Variables, Data Processing and Analysis
2.4. Ethical Aspect
3. Results
4. Discussion
4.1. Limitations
4.2. Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Caldwell, J.A.; Caldwell, J.L.; Thompson, L.A.; Lieberman, H.R. Fatigue and its management in the workplace. Neurosci. Biobehav. Rev. 2019, 96, 272–289. [Google Scholar] [CrossRef]
- Jaber, M.J.; AlBashaireh, A.M.; AlShatarat, M.H.; Alqudah, O.M.; Preez, S.E.D.; AlGhamdi, K.S.; AlTmaizy, H.M.; Dawass, M.A.A. Stress, Depression, Anxiety, and Burnout among Healthcare Workers during the COVID-19 Pandemic: A Cross-sectional Study in a Tertiary Centre. Open Nurs. J. 2021, 16, e187443462203140. [Google Scholar] [CrossRef]
- Makkai, K. Evaluating the Level of Burnout among Healthcare Professionals. Acta Univ. Sapientiae Soc. Anal. 2018, 8, 23–39. [Google Scholar] [CrossRef]
- Loya-Murguía, K.M.; Valdez-Ramírez, J.; Bacardí-Gascón, M.; Jiménez-Cruz, A. El síndrome de agotamiento en el sector salud de Latinoamérica: Revisión sistemática. J. Negat. No Posit. Results 2018, 3, 40–48. [Google Scholar] [CrossRef]
- Suñer-Soler, R.; Grau-Martín, A.; Flichtentrei, D.; Prats, M.; Braga, F.; Font-Mayolas, S.; Gras, M.E. The consequences of burnout syndrome among healthcare professionals in Spain and Spanish speaking Latin American countries. Burn. Res. 2014, 1, 82–89. [Google Scholar] [CrossRef]
- Ghahramani, S.; Lankarani, K.B.; Yousefi, M.; Heydari, K.; Shahabi, S.; Azmand, S. A Systematic Review and Meta-Analysis of Burnout among Healthcare Workers During COVID-19. Front. Psychiatry 2021, 12, 758849. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Nurses’ burnout and associated risk factors during the COVID-19 pandemic: A systematic review and meta-analysis. J. Adv. Nurs. 2021, 77, 3286–3302. [Google Scholar] [CrossRef]
- Maticorena-Quevedo, J.; Beas, R.; Anduaga-Beramendi, A.; Mayta-Tristán, P. Prevalencia del síndrome de burnout en médicos y enfermeras del Perú, Ensusalud 2014. Rev. Peru. Med. Exp. Salud Pública 2016, 33, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Benites, S.F. Nivel de Síndrome de Burnout en Enfermeras, Técnicas y Auxiliares de Enfermería del Hospital Las Palmas de la Fuerza Aérea del Perú, Lima 2017. Bachelor’s Thesis, Universidad Inca Garcilaso de La Vega, Lima, Peru, 2017. [Google Scholar]
- Min, A.; Min, H.; Hong, H.C. Work schedule characteristics and fatigue among rotating shift nurses in hospital setting: An integrative review. J. Nurs. Manag. 2019, 27, 884–895. [Google Scholar] [CrossRef] [PubMed]
- Moya-Salazar, J.; Cañari, B.; Zuñiga, N.; Jaime-Quispe, A.; Rojas-Zumaran, V.; Contreras-Pulache, H. Deaths, infections, and herd immunity in the COVID-19 pandemic: A comparative study of the strategies for disease containment implemented in Peru and the United Kingdom. Rev. Fac. Med. 2022, 70, e92823. [Google Scholar] [CrossRef]
- Mejía, F.; Medina, C.; Cornejo, E.; Morello, E.; Vasquez, S.; Alave, J.; Schwalb, A.; Malaga, G. Características Clínicas y Factores Asociados a Mortalidad en Pacientes Adultos Hospitalizados por COVID-19 en un Hospital Público de Lima, Perú. SciELO Prepr. 2022. Available online: https://preprints.scielo.org/index.php/scielo/preprint/view/858/1187 (accessed on 21 December 2022).
- Ferry, A.V.; Wereski, R.; Strachan, F.E.; Mills, N.L. Predictors of UK healthcare worker burnout during the COVID-19 pandemic. QJM Int. J. Med. 2021, 114, 374–380. [Google Scholar] [CrossRef]
- Moya-Salazar, J.; Saciga-Saavedra, W.; Cañari, B.; Contreras-Pulache, H. Depression in health-care workers from the COVID-19 care and isolation Center-Villa Panamericana: A single-center prospective study in Peru. Einstein (São Paulo) 2022, 20, eAO6707. [Google Scholar] [CrossRef]
- Betancourt, D.M.T.; Domínguez, Q.W.F.; Peláez, F.B.I.; Herrera, V. M del R. Estrés laboral en el personal de enfermería del área de UCI durante la pandemia de COVID 19. UNESUM-Ciencias. Rev. Científica Multidiscip. 2020, 4, 41–50. Available online: https://revistas.unesum.edu.ec/index.php/unesumciencias/article/view/308/210 (accessed on 21 December 2022).
- Kantorski, L.P.; de Oliveira, M.M.; Alves, P.F.; Treichel, C.A.S.; Wünsch, C.G.; Santos, L.H.; Pinheiro, G.E.W. Intenção em deixar a Enfermagem durante a pandemia de COVID-19. Rev. Lat.-Am. Enferm. 2022, 30, e3612. [Google Scholar] [CrossRef]
- Ministerio de Salud, M. Hospital Nacional “Dos de Mayo”. In Informe de Transferencia de Gestión. Equipo de Gestión Noviembre 2020–Febrero 2021; MINSA: Lima, Peru, 2022; Available online: https://cdn.www.gob.pe/uploads/document/file/1751525/DGOS%20-%20Hospital%20Nacional%20Dos%20de%20Mayo.pdf (accessed on 21 December 2022).
- Filmo, M.; Villanueva, F. Sintomatología y Terapias en Pacientes COVID-19 Positivos Que Acuden al Hospital Nacional dos de Mayo, Abril 2021. Bachelor’s Thesis, Universidad Maria Auxiliadora, Lima, Peru, 2021. Available online: https://hdl.handle.net/20.500.12970/577 (accessed on 21 December 2022).
- Maslach, C.; Jackson, S.E. Maslach Burnout Inventory—ES Form. PsycTESTS Dataset. 1981. Available online: https://psycnet.apa.org/doiLanding?doi=10.1037%2Ft05190-000 (accessed on 20 December 2022).
- Gil-Monte, P.R.; Peiró, J.M. Validez Factorial del Maslach Burnout Inventory en una muestra multiocupacional. Psicothema Reun. 1999, 11, 679–689. Available online: https://reunido.uniovi.es/index.php/PST/article/view/7551 (accessed on 20 December 2022).
- Arpita, R.A.M. Síndrome de Burnout Mediante la Aplicación del Cuestionario Maslach Burnout Inventory en Internos de Obstetricia del Instituto Nacional Materno Perinatal y Hospital Nacional Docente Madre Niño San Bartolomé-Junio 2016. Bachelor’s Tesis, Universidad Nacional Mayor de San Marcos, Lima, Peru, 2016. Available online: https://pesquisa.bvsalud.org/portal/resource/pt/biblio-1114579 (accessed on 20 December 2022).
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach Burnout Inventory Manual, 4th ed.; Mind Garden, Inc.: Menlo Park, CA, USA, 2016. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Elhadi, M.; Msherghi, A.; Elgzairi, M.; Alhashimi, A.; Bouhuwaish, A.; Biala, M.; Abuelmeda, S.; Khel, S.; Khaled, A.; Alsoufi, A.; et al. Burnout Syndrome among Hospital Healthcare Workers during the COVID-19 Pandemic and Civil War: A Cross-Sectional Study. Front. Psychiatry 2020, 11, 579563. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, C.; Pan, W.; Zheng, J.; Gao, J.; Huang, X.; Cai, S.; Zhai, Y.; Latour, J.; Zhu, C. Stress, Burnout, and Coping Strategies of Frontline Nurses During the COVID-19 Epidemic in Wuhan and Shanghai, China. Front. Psychiatry 2020, 11, 565520. [Google Scholar] [CrossRef]
- Robba, H.C.S.; Costa, A.A.; Kozu, K.T.; Silva, C.A.; Farhat, S.C.L.; Ferreira, J.C.d.O.A. Impacto na saúde mental de enfermeiros pediátricos: Um estudo transversal em hospital pediátrico terciário durante a pandemia de COVID-19. Rev. Lat.-Am. Enferm. 2022, 30, e3582. [Google Scholar] [CrossRef]
- Vieira, L.S.; Machado, W.d.L.; Dal Pai, D.; Magnago, T.S.B.D.S.; Azzolin, K.D.O.; Tavares, J.P. Burnout e resiliência em profissionais de enfermagem de terapia intensiva frente à COVID-19: Estudo multicêntrico. Rev. Lat.-Am. Enferm. 2022, 30, e3588. [Google Scholar] [CrossRef]
- Vinueza-Veloz, A.F.; Aldaz-Pachacama, N.R.; Mera-Segovia, C.M.; Pino-Vaca, D.P.; Tapia-Veloz, E.C.; Vinueza-Veloz, M.F. Síndrome de Burnout en médicos/as y enfermeros/as ecuatorianos durante la pandemia de COVID-19. Correo Cientf Med. 2021, 25, 1–7. Available online: https://revcocmed.sld.cu/index.php/cocmed/article/view/3808 (accessed on 15 December 2022).
- World Health Organization. Public Health Surveillance for COVID-19: Interim Guidance, 16 December 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Culquicondor, C.R. Síndrome Burnout en Personal de Enfermería del Área COVID-19 en el Hospital Nacional Arzobispo Loayza, 2020. Bachelor’s Thesis, Universidad Privada Norbert Wiener, Lima, Peru, 2020. Available online: http://repositorio.uwiener.edu.pe/handle/123456789/3934 (accessed on 20 December 2022).
- Burgos, R.; Salazar, M. Nivel de Estrés del Profesional de Enfermería de un Hospital MINSA, Trujillo 2020. Bachelor’s Thesis, Universidad Cesar Vallejo, Lima, Peru, 2020. Available online: https://hdl.handle.net/20.500.12692/91200 (accessed on 20 December 2022).
- Moya-Salazar, J.; Saciga-Saavedra, W.; Cañari, B.; Chicoma-Flores, K.; Contreras-Pulache, H. Can living with COVID-19 patients in a hospital increase anxiety level in healthcare workers? A survey-based single-center study in Peru. Electron. J. Gen. Med. 2022, 19, em389. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization. Pan American Health Organization Response to COVID-19. January to June 2021; PAHO: Washington, DC, USA, 2021. [Google Scholar]
- Moya-Salazar, J.; Cañari, B.; Sánchez-Llanos, A.; Hernández, S.A.; Eche-Navarro, M.; Salazar-Hernández, R.; Contreras-Pulache, H. Factores de riesgo en población rural andina con COVID-19: Un estudio de cohorte retrospectivo. Infectio 2021, 25, 256–261. [Google Scholar] [CrossRef]
- Comisión Económica para América Latina y el Caribe. Mortalidad por COVID-19 y las Desigualdades por Nivel Socioeconómico y Por Territorio; CEPAL Press: Santiago, Chile; Available online: https://www.cepal.org/es/enfoques/mortalidad-covid-19-desigualdades-nivel-socioeconomico-territorio (accessed on 15 December 2022).
- Moya-Salazar, J.; Cañari, B.; Contreras-Pulache, H. How much fear of COVID-19 is there in Latin America? A prospective exploratory study in six countries. Electron. J. Gen. Med. 2022, 19, em339. [Google Scholar] [CrossRef]
- Fajardo-Luna, C.; Espil-Sanchez, S.; Quico-Berrio, R.; Muñoz-Cure, Y.; Salazar, C.R.; Moya-Salazar, J. Comments on patient safety and adverse events regarding the study by Riera-Vázquez et al., (2022). J. Healthc. Qual. Res. 2023, 22, S2603–S6479. [Google Scholar] [CrossRef]
- Caballol-Avendaño, F.; Flores-Hoyos, A.; Guerra-Cruz, J.; Morales-Vizcarra, F.; Reynaldos-Grandón, K.L. Prevención del Síndrome de Burnout en enfermería en pandemia COVID-19: Una revisión sistemática. Rev. Salud Pública 2021, 26, 48–59. Available online: https://revistas.unc.edu.ar/index.php/RSD/article/view/33447 (accessed on 15 December 2022). [CrossRef]
- Moya-Salazar, J.; Rojas-Zumaran, V.; Salazar, C.R.; Contreras-Pulache, H. Transforming institutions in response to health care needs: Comments on a Peruvian experience. J. Healthc. Qual. Res. 2023, in press. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Categories | Burnout | N (%) | |
|---|---|---|---|---|
| Moderate | High | |||
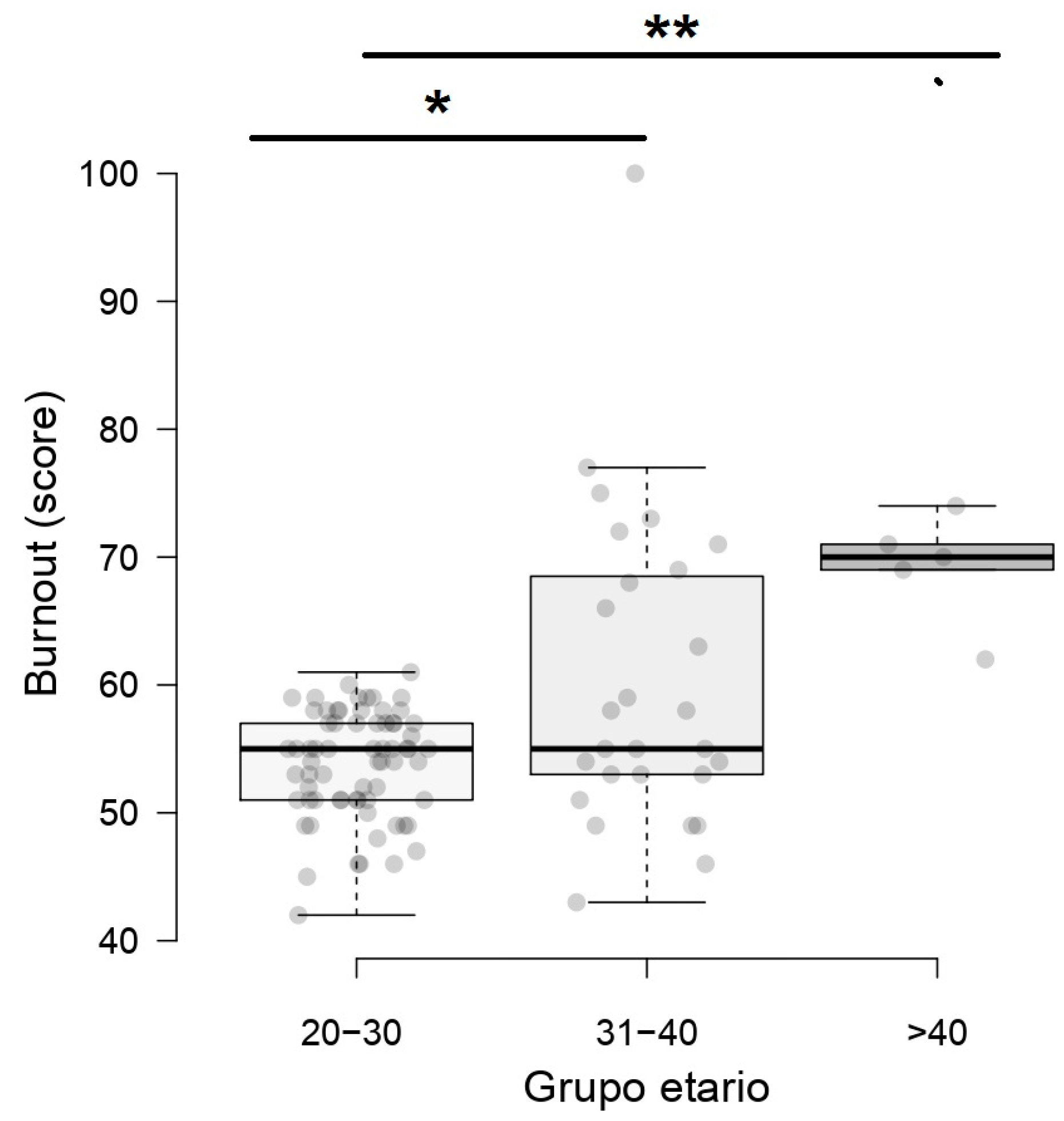
| Age group (years) | 20 to 30 | 68 (100) | 0 (0) | 68 (68) |
| 31 to 40 | 19 (70.4) | 8 (29.6) | 27 (27%) | |
| >41 | 1 (20) | 4 (80) | 5 (5%) | |
| p-value | <0.001 | |||
| Sex | Female | 67 (85.9) | 11 (14.1) | 78 (78%) |
| Male | 21 (95.4) | 1 (4.6) | 22 (22%) | |
| p-value | 0.882 | |||
| Working time (years) | 1 to 10 | 53 (91.4) | 4 (1.6) | 57 (57%) |
| 11 to 20 | 27 (77.1) | 8 (32.9) | 35 (35%) | |
| 21 to 30 | 8 (100) | 0 (0) | 8 (8%) | |
| p-value | 0.239 | |||
| SARS-CoV-2 Infection | Yes | 35 (85.4) | 6 (14.6) | 41 (41%) |
| No | 53 (89.8) | 6 (10.2) | 59 (59%) | |
| p-value | 0.716 | |||
| Dimension | Frequency | Age Group (Years) | ||
|---|---|---|---|---|
| 20 to 30 | 31 to 40 | 41 to 50 | ||
| Emotional exhaustion | Low | 68 (100) | 23 (85.1) | 4 (80) |
| Moderate | 0 (0) | 3 (11.1) | 1 (20) | |
| High | 0 (0) | 1 (3.7) | 0 (0) | |
| Depersonalization | Low | 41 (60.2) | 15 (55.5) | 0 (0) |
| Moderate | 26 (38.2) | 6 (22.2) | 2 (40) | |
| High | 1 (1.4) | 6 (22.2) | 3 (30) | |
| Personal achievements | Low | 0 (0) | 1 (3.7) | 0 (0) |
| Moderate | 17 (25) | 5 (18.5) | 1 (20) | |
| High | 51 (75) | 21 (77.7) | 4 (80) | |
| Variables | Burnout | |||
|---|---|---|---|---|
| B | SE | p-Value | 95% CI | |
| Age (years) | 7.57 | 1.32 | <0.001 * | 4.95 to 10.18 |
| Sex | 3.28 | 1.88 | 0.085 | −0.46 to 7.01 |
| Working time | 0.65 | 1.19 | 0.585 | −1.71 to 3.01 |
| Previous SARS-CoV-2 infection | −0.57 | 1.44 | 0.691 | −3.42 to 2.28 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moya-Salazar, J.; Buitrón, L.A.; Goicochea, E.A.; Salazar, C.R.; Moya-Salazar, B.; Contreras-Pulache, H. The Age of Young Nurses Is a Predictor of Burnout Syndrome during the Care of Patients with COVID-19. Nurs. Rep. 2023, 13, 721-730. https://doi.org/10.3390/nursrep13020063
Moya-Salazar J, Buitrón LA, Goicochea EA, Salazar CR, Moya-Salazar B, Contreras-Pulache H. The Age of Young Nurses Is a Predictor of Burnout Syndrome during the Care of Patients with COVID-19. Nursing Reports. 2023; 13(2):721-730. https://doi.org/10.3390/nursrep13020063
Chicago/Turabian StyleMoya-Salazar, Jeel, Liliana A. Buitrón, Eliane A. Goicochea, Carmen R. Salazar, Belén Moya-Salazar, and Hans Contreras-Pulache. 2023. "The Age of Young Nurses Is a Predictor of Burnout Syndrome during the Care of Patients with COVID-19" Nursing Reports 13, no. 2: 721-730. https://doi.org/10.3390/nursrep13020063