
The Burnout of Nurses in Intensive Care Units and the Impact of the SARS-CoV-2 Pandemic: A Scoping Review

 , ,
, ,  , , , , and
, , , , and
Abstract
:1. Introduction
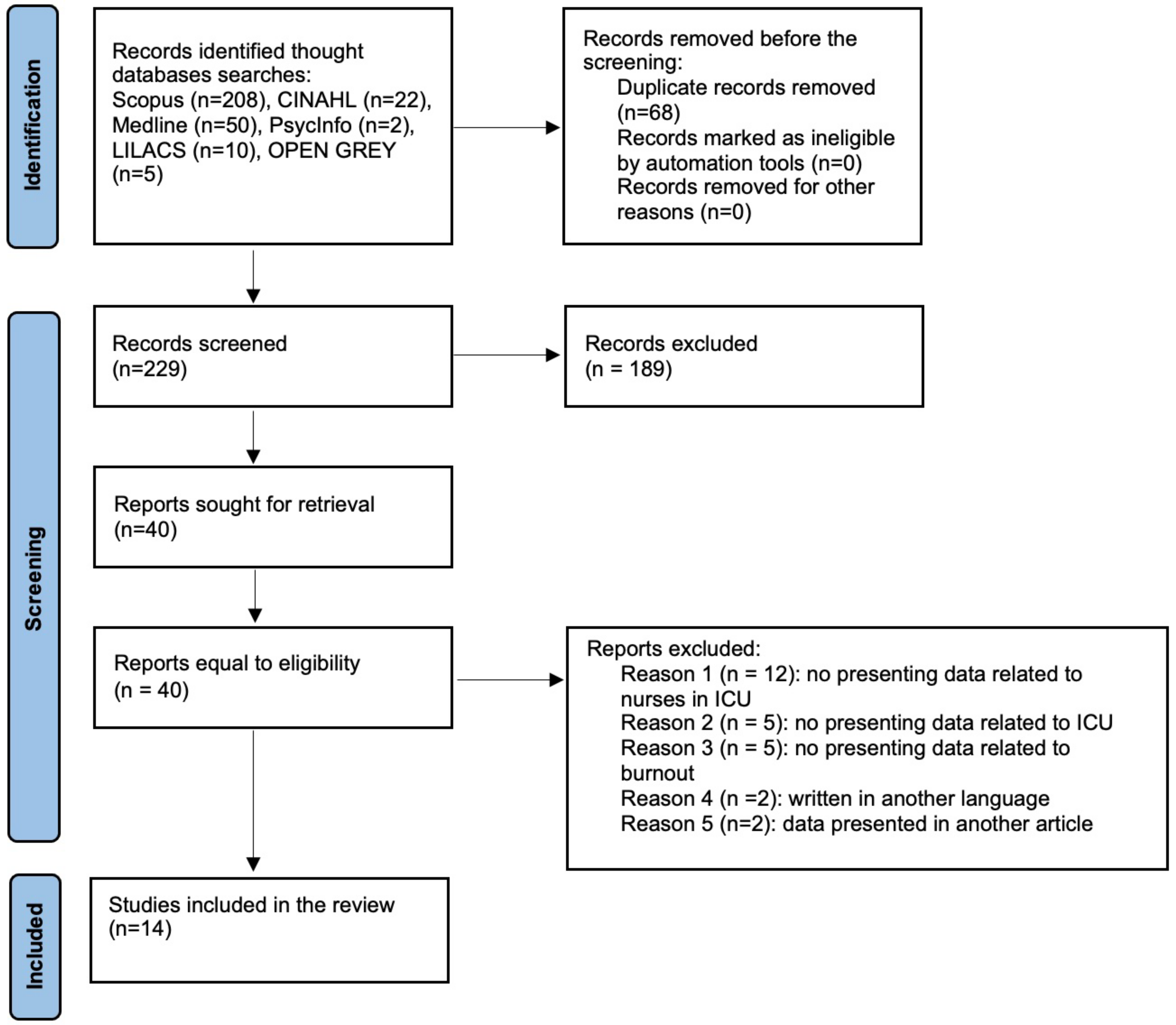
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Search Strategy
3. Results
3.1. Study Characteristics, Settings, and Sample
3.2. Burnout in Intensive Care Units
3.2.1. Emotional Exhaustion
3.2.2. Depersonalisation
3.2.3. Personal Achievement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Peixoto, V.R.; Vieira, A.; Aguiar, P.; Carvalho, C.; Thomas, D.R.; Abrantes, A. Initial Assessment of the Impact of the Emergency State Lockdown Measures on the 1st Wave of the COVID-19 Epidemic in Portugal. Acta Med. Port. 2020, 33, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Limbu, S.; Kongsuwan, W.; Yodchai, K. Lived experiences of intensive care nurses in caring for critically ill patients. Nurs. Crit Care 2019, 24, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Tronstad, O.; Flaws, D.; Lye, I.; Fraser, J.F.; Patterson, S. The intensive care unit environment from the perspective of medical, allied health and nursing clinicians: A qualitative study to inform design of the “ideal” bedspace. Aust. Crit. Care 2021, 34, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Danielis, M.; Palese, A.; Terzoni, S.; Destrebecq, A.L.L. What nursing sensitive outcomes have been studied to-date among patients cared for in intensive care units? Findings from the scoping review. Int. J. Nurs. Stud. 2020, 102, 103491. [Google Scholar] [CrossRef] [PubMed]
- Jakimowicz, S.; Perry, L.; Lewis, J. Insights on compassion and patient-centered nursing in intensive care: A constructivist grounded theory. J. Clin. Nurs. 2018, 27, 1599–1611. [Google Scholar] [CrossRef]
- Barbosa, F.T.; Leão, B.A.; Tavares, G.M.; Santos, J.G. Burnout syndrome and weekly workload of on-call physicians: Cross-sectional study. Sao Paulo Med. J. 2012, 130, 282–288. [Google Scholar] [CrossRef]
- Moraes, C.L.K.; Tavares, D.C.; Freitas, G.B.; Aued, G.K. The perspective of nurses on the companion in the ICU in times of COVID-19. Glob. Acad. Nurs. 2021, 2, e108. [Google Scholar]
- Maslach, C.; Leiter, M.P. The Truth about Burnout: How Organizations Cause Personal Stress and What to Do about It, 1st ed.; Jossey-Bass: San Francisco, CA, USA, 1997; pp. 1–202. [Google Scholar]
- Maslach, C.; Leiter, M.P.; Fink, G. Encyclopedia of Stress, 1st ed.; Academic Press: San Diego, CA, USA, 2000; pp. 358–362. [Google Scholar]
- Tower, M.; Popper, M.S.; Bergesio, A. Burnout prevalence in intensive care nurses in Argentina. Enferm. Intensive 2019, 30, 108–115. [Google Scholar]
- Costa, D.K.; Moss, M. The cost of caring: Emotion, burnout, and psychological distress in critical care clinicians. Ann. Am. Thorac. Soc. 2018, 15, 787–790. [Google Scholar] [CrossRef]
- Rothenberger, D.A. Physician Burnout and Well-Being: A Systematic Review and Framework for Action. Dis. Colon. Rectum. 2017, 60, 567–576. [Google Scholar] [CrossRef]
- Barros, D.S.; Tironi, M.O.S.; Nascimento Sobrinho, C.L.; Neves, F.S.; Bitencourt, A.G.V.; Almeida, A.M.; Marques Filho, E.S.; Reis, E.J.F.B. Physicians on duty at an intensive care unit: Socio-demographic profile, working conditions and factors associated with burnout syndrome. Braz. J. Intensive Ther. 2008, 20, 235–240. [Google Scholar]
- Lima, A.; Moreira, M.T.; Fernandes, C.; Ferreira, M.; Teixeira, J.; Parola, V.; Coelho, A. The Burnout of Nurses in Intensive Care Units and the Impact of the Pandemic of SARS-CoV-2: Protocol of a Scoping Review. Nurs. Rep. 2022, 12, 65. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, F.C.T.; Barbosa, C.P. The impact of the COVID-19 pandemic in an intensive care unit (ICU): Psychiatric symptoms in healthcare professionals. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 110, 110299. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Mulet, C.; Sanso, N.; Carrero-Planells, A.; Lopez-Deflory, C.; Galiana, L.; Garcia-Pazo, P.; Borràs-Mateu, M.M.; Miró-Bonet, M. The Impact of the COVID-19 Pandemic on ICU Healthcare Professionals: A Mixed Methods Study. Int. J. Environ. Res. Public Health 2021, 18, 9243. [Google Scholar] [CrossRef] [PubMed]
- Aromataris, E.; Munn, Z. JBI Manual for Evidence Synthesis. JBI. 2020. Available online: https://doi.org/10.46658/JBIMES-20-01 (accessed on 23 November 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Guttormson, J.L.; Calkins, K.; McAndrew, N.; Fitzgerald, J.; Losurdo, H.; Loonsfoot, D. Critical Care Nurses’ Experiences During the COVID-19 Pandemic: A US National Survey. Am. J. Crit. Care 2022, 31, 96–103. [Google Scholar] [CrossRef]
- Haruna, J.; Unoki, T.; Ishikawa, K.; Okamura, H.; Kamada, Y.; Hashimoto, N. Influence of Mutual Support on Burnout among Intensive Care Unit Healthcare Professionals. SAGE Open Nurs. 2022, 8, 23779608221084977. [Google Scholar] [CrossRef]
- Acar Sevinc, S.; Metin, S.; Balta Basi, N.; Cinar, A.S.; Turkel Ozkan, M.; Oba, S. Anxiety and burnout in anaesthetists and intensive care unit nurses during the COVID-19 pandemic: A cross-sectional study. Braz. J. Anesthesiol. 2022, 72, 169–175. [Google Scholar]
- Seluch, M.; Volchansky, M.; Safronov, R. Dependence of emotional burnout on personality typology in the COVID-19 pandemic. Work 2021, 70, 713–721. [Google Scholar] [CrossRef]
- Gordon, J.M.; Magbee, T.; Yoder, L.H. The experiences of critical care nurses caring for patients with COVID-19 during the 2020 pandemic: A qualitative study. Appl. Nurs. Res. 2021, 59, 151418. [Google Scholar] [CrossRef]
- Vitale, E.; Galatola, V.; Mea, R. Exploring within and between gender differences in burnout levels in Italian nurses engaged in the cOviD-19 health emergency: A cohort observational study. Minerva Psichiatr. 2020, 61, 162–170. [Google Scholar] [CrossRef]
- Srinivas, G.C.; Whitham, A.; Rouse, R.; Hamlyn, V.; Williams, M. Occupational burnout following the first wave of coronavirus disease at a Welsh district general hospital. J. Intensive Care Soc. 2022, 23, 369–371. [Google Scholar] [CrossRef] [PubMed]
- Molina-Mula, J.; González-Trujillo, A.; Perelló-Campaner, C.; Tortosa-Espínola, S.; Tera-Donoso, J.; la Rosa, L.O.D.; Romero-Franco, N. The emotional impact of COVID-19 on Spanish nurses and potential strategies to reduce it. Collegian 2022, 29, 296–310. [Google Scholar] [CrossRef]
- Butera, S.; Brasseur, N.; Filion, N.; Bruyneel, A.; Smith, P. Prevalence and Associated Factors of Burnout Risk Among Intensive Care and Emergency Nurses Before and During the Coronavirus Disease 2019 Pandemic: A Cross-Sectional Study in Belgium. J. Emerg. Nurs. 2021, 47, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, B.; Scorsolini-Comin, F.; de Souza, S.R. Burnout syndrome in intensive care unit nurses during the COVID-19 pandemic. Rev. Bras. Med. Trab. 2021, 19, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Freitas, R.F.; de Barros, I.M.; Miranda, M.A.F.; Freitas, T.F.; Rocha, J.S.B.; Lessa, A.D.C. Predictors of burnout syndrome in nursing technicians in an intensive care unit during the covid-19 pandemic. Braz. J. Psychiatr. 2021, 70, 12–20. [Google Scholar]
- Bruyneel, A.; Bouckaert, N.; Maertens de Noordhout, C. Association of burnout and intention-to-leave the profession with work environment: A nationwide cross-sectional study among Belgian intensive care nurses after two years of pandemic. Int. J. Nurs. Stud. 2021, 65, 104385. [Google Scholar]
- Chen, R.; Sun, C.; Chen, J.J.; Jen, H.J.; Kang, X.L.; Kao, C.C.; Chou, K.-R. A Large-Scale Survey on Trauma, Burnout, and Posttraumatic Growth among Nurses during the COVID-19 Pandemic. Int. J. Ment. Health Nurs. 2021, 30, 102–116. [Google Scholar] [CrossRef]
- Jang, Y.; You, M.; Lee, H.; Lee, M.; Lee, Y.; Han, J.O.; Oh, J.H. Burnout and peritraumatic distress of healthcare workers in the COVID-19 pandemic. BMC Public Health 2021, 21, 2075. [Google Scholar] [CrossRef]
- Lima, M.A.; Rodrigues, S.R.; Sanches, R.S.; Souza, A.R. Stress, burnout and hardiness among active nursing professionals in critical and emergency care. Adm. Hosp. Innovation Health 2020, 17, 82–96. [Google Scholar]


{kind=link}
| Database: CINAHL Complete (via EBSCO) Filters: last 4 years, English, Portuguese, Spanish, excluding MEDLINE Results: 22 Search strategy (14 April 2022) (TI SARS-CoV-2 OR AB SARS-CoV-2 OR MH SARS-CoV-2 OR TI COVID-19 OR AB COVID-19 OR MH COVID-19) AND (TI burnout OR AB burnout OR MH burnout, professional OR TI exhaustion OR AB exhaustion) AND (TI nurse OR AB nurse OR MH nurses) AND (TI intensive care units OR AB intensive care units OR MH intensive care units OR TI intensive care unit OR AB intensive care unit OR TI ICU OR AB ICU) |
| Database: Psychology and Behavioral Sciences Collection Filters: last 4 years, English, Portuguese, Spanish Results: 2 Search strategy (14 April 2022) (((DE “PSYCHOLOGICAL burnout”) OR (burnout) OR (exhaustion)) AND ((DE “NURSES”) OR (nurse) OR (nurses) OR (DE “NURSE practitioners”)) AND ((DE “INTENSIVE care units”) OR (intensive care units) OR (intensive care unit) OR (ICU)) AND ((DE “SARS-CoV-2”) OR (SARS-CoV-2) OR (DE “COVID-19”) OR (COVID-19))) |
| Database: LILACS Filters: last 4 years, English, Portuguese, Spanish Results: 10 Research Strategy (14 April 2022) (COVID AND burnout AND nurse) |
| Database: SCOPUS Filters: last 4 years, English, Portuguese, Spanish Results: 208 Search strategy (14 April 2022) ((TITLE-ABS-KEY ((burnout, professional) OR (burnout) OR (exhaustion)) AND TITLE-ABS-KEY ((nurses) OR (nurse) OR (nurses) OR (nurse practitioners)) AND TITLE-ABS -KEY ((intensive care units) OR (intensive care units)) OR (intensive care unit)) OR (ICU)) AND TITLE-ABS-KEY ((SARS-CoV-2) OR (COVID-19))) |
| Database: MEDLINE (via PubMed) Filters: last 4 years, English, Portuguese, Spanish Results: 50 Search strategy (14 April 2022) (((((burnout, professional[MeSH Terms]) OR (burnout[Title/Abstract])) OR (exhaustion[Title/Abstract])) AND ((((nurses[MeSH Terms]) OR (nurse[Title/Abstract])) OR (nurses[Title/Abstract])) OR (nurse practitioners[MeSH Terms]))) AND ((((intensive care units[MeSH Terms]) OR (intensive care units[Title/Abstract])) OR (intensive care unit[Title/Abstract])) OR (ICU[Title/Abstract]))) AND ((((SARS-CoV-2[MeSH Terms]) OR (SARS-CoV-2[Title/Abstract])) OR (COVID-19[MeSH Terms])) OR (COVID-19[Title/Abstract])) |
| Database: OPEN GRAY Results: 5 Search strategy (14 April 2022) (burnout AND COVID-19) |
| Author, Year and Country | Aims | Population and Sample Size | Results (Level of Burnout) |
|---|---|---|---|
| Guttormson, et al., 2022, USA [19] | To describe the experiences of ICU nurses during the COVID-19 pandemic in the United States. | Nurses sample size (n = 285) | Nurses reported stress related to a lack of evidence-based treatment, poor patient prognosis, and lack of family presence in the ICU. Nurses perceived inadequate leadership support and inequity within the healthcare team. Lack of consistent community support to slow the spread of COVID-19 or recognition that COVID-19 was real increased nurses’ feelings of isolation. Nurses reported physical and emotional symptoms, including exhaustion, anxiety, sleeplessness, and moral distress. Fear of contracting COVID-19 or of infecting family and friends was also prevalent. |
| Haruna et al., 2022, Japan [20] | To verify if lower mutual support among ICU HCP professionals is associated with increased probability of burnout. | HCW (n = 335) Subsample Nurses (n = 196) | The majority of respondents were nurses (58.5%), followed by physicians (18.5%). Nearly half of the respondents (53.7%) were men, with more than 10 years of ICU experience (80.9%). Approximately 85% of respondents were involved in COVID-19 patient management (85.4%). Men had a significantly lower probability of burnout than women (p = 0.021). Respondents with housemates had a significantly lower probability of burnout. (p = 0.049). Nurses had a significantly higher frequency of burnout than other healthcare professionals (p = 0.044). |
| Sevic et al., 2021, Turkey [21] | To measure the levels of anxiety and burnout among healthcare workers during the COVID-19 pandemic. | HCW (n = 104) Subsample nurses (n = 43) | The distributions of emotional exhaustion (EE), personal accomplishment (PA), and depersonalisation (DP) scores were significantly different among HCWs (p = 0.023, 0.000, and 0.000, respectively). Residents and nurses had almost the same EE scores (p = 0.872), both of which turned out to be higher than that for attending physicians (p = 0.007 and 0.003, respectively). The PA score for residents was lower than that for attending physicians (p = 0.039) and nurses (p = 0.000). |
| Seluch et al., 2021, Russia [22] | To establish the features of emotional burnout syndrome and its connection with typological characteristics of the personality in nurses working with COVID-19 patients. | n = 74 Outpatients = 30 ICU = 44 | Emotional burnout level: (24.57 ± 1.46) scores, the average value of DP level was (7.85 ± 0.8) points. Among nurses, 15 (34.1%) had a high level of EE, 23 (52.3%) had an average level, and only 6 (13.6%) had a low level. Regarding DP, among intensive care nurses, a high level of DP was seen in 5 (11.4%) people, medium in 30 (68.2%) people, and low in 9 people (20.4%). A high level of reduction in professional success was found in 3 (6.8%) intensive care nurses, an average level in 17 (38.6%), and a low level in 24 (54.6%). |
| Gordon et al., 2021, USA [23] | To examine ICU nurse’s experiences caring for COVID-19 Patients. | n = 11 | ICU nurses for patients diagnosed with COVID-19 were categorised into five themes and subthemes. Emotions experienced were subcategorised into anxiety/stress, fear, helplessness, worry, and empathy. Physical symptoms were subcategorised into sleep disturbances, headaches, discomfort, exhaustion, and breathlessness. Care environment challenges were subcategorised into nurses as surrogates, inability to provide comforting human connection, dying patients, personal protective equipment (PPE), isolation, care delay, changing practice guidelines, and language barrier. Social effects were subcategorised into stigma, divergent healthcare hero perception, additional responsibilities, strained interactions with others, and isolation/loneliness. Short term coping strategies were subcategorised into co-worker support, family support, distractions, mind/body wellness, and spiritualty/faith. Results showed that ICU nurses experienced intense psychological and physical effects as a result of caring for patients diagnosed with COVID-19 in a challenging care environment. Outside of work, nurses faced pandemic-induced societal changes and divergent public perceptions of them. |
| Vitale el al., 2020, Italy [24] | To evaluate the burnout syndrome among nurses who are engaged in the care of patients with Coronavirus disease (COVID-19) | n = 291 | Regarding EE, female nurses were more exposed to the phenomenon than men (p < 0.001). However, for the other two dimensions, there were no statistically different differences between the two sexes (DP: p = 0.809; personal accomplishment: p = 0.268). It was seen that EE was significantly higher among female nurses with a range of years of work experience ranging from 0 to 10 (p = 0.005) compared to male nurses. Significant levels of EE were also highlighted considering female nurses, both those who were already assigned to an intensive care unit before the COVID-19 pandemic (p = 0.003) and those who were transferred during the health emergency (p = 0.028). |
| Srinivas et al., 2021, UK [25] | To identify the prevalence of burnout and the contributing factors amongst HCPs caring for COVID-19 patients admitted to ICU. | HCW (n = 153) Subsample nurses (n = 47) | The response rate was 79%. Nurses and other staff reassigned to work in the ICU had higher levels of burnout. Working in personal protective equipment was most distressing, followed by direct patient care. There were positive outcomes including learning opportunities, professional development and job satisfaction. The impact of the pandemic on staff burnout may have been mitigated by acknowledging the contribution of staff, improving communication and encouraging their to access support. |
| Molina-Mula, 2021, Spain [26] | To analyse the levels of anxiety, depression, PTS and burnout of nurses during the pandemic to identify possible sociodemographic and related occupational factors. | n = 280 ICU nurses (n = 23) | Nurses working in the COVID-19 ICU had a mean score of 31.67 (p < 0.001). The results showed statistically significant variations in emotional fatigue according to the unit, years of professional experience, health centre and experience in COVID-19 units (p < 0.001; F ANOVA, chi square). The findings indicated that after two months of working in units with COVID-19 patients, nurses began to experience emotional fatigue, which increased over the course of a month. The high fatigue values noted among nurses working in the adult ICU and in ICUs with COVID-19 patients are of concern; they exceeded the mean of 31 points out of 26, which is the detection cut off for fatigue. |
| Butera et al., 2021, Belgium [27] | Assess (1) the prevalence of burnout risk among nurses working in intensive care unitsand emergency department before and during the coronavirus disease 2019 pandemic and (2) the individual and work-related associated factors. | n = 422 (first-wave measurement)n = 1616 (second-wave measurement) | The overall prevalence of burnout risk increased significantly among intensive care unit nurses (from 51.2% to 66.7%, x2 = 23.64, p < 0.003). During the pandemic, changes in workload and the lack of personal protective equipment were significantly associated with a higher likelihood of burnout risk, whereas social support from colleagues and from superiors and management was associated with a lower likelihood of burnout risk. Several determinants of burnout risk were different between intensive care unit and emergency nurses. |
| Ribeiro et al., 2021, Brazil [28] | To review the scientific literature on burnout syndrome among intensive care unit nurses during the COVID-19 pandemic | N/A | This narrative review considered publications on the current pandemic, as well as studies on worker health and burnout, focusing on intensive care unit nurses.The literature was organised into two thematic categories: (1) emotional distress in the daily work of intensive care unit nurses; (2) preventing burnout in these professionals during the COVID-19 pandemic. Although the literature on burnout is expressive, there is a need to transmit data produced during the pandemic and follow these professionals longitudinally, which could lead to the development of specific prevention and health promotion strategies. Changes in the emotional and working conditions of these professionals must become a permanent part of worker health research and practice, rather than a temporary measure during the pandemic. |
| Freitas et al., 2021, Brazil [29] | To evaluate the prevalence and existence of predictive factors for Burnout syndrome in nursing technicians who work in an intensive care unit during the COVID-19 pandemic. | n = 94 | The prevalence of the syndrome was observed in 25.5% of the analysed sample. The variables that, after multiple analyses, were shown to be predictors associated with a higher prevalence of Burnout syndrome were: age > 36 years, overtime considering the rigid workload and being elitist. |
| Bruyneel et al., 2021, Belgium [30] | To assess the prevalence of burnout risk and identify risk factors among ICU nurses during the COVID-19 pandemic. | n = 1135 | The overall prevalence of burnout risk was 68%. A total of 29% of ICU nurses were at risk of DP, 31% of reduced PA, and 38% of EE. A 1:3 nurse-to-patient ratio increased the risk of EE (OR = 1.77, 95% CI: 1.07–2.95) and SD (OR = 1.38, 95% CI: 1.09–2.40). Those who reported having a higher perceived workload during the COVID-19 pandemic were at higher risk for all dimensions of burnout. Shortage of personal protective equipment increased the risk of EE (OR = 1.78, 95% CI: 1.35– 3.34) and nurses who had reported symptoms of COVID-19 without being tested were at higher risk of EE (OR = 1.40, 95% CI: 1.68–1.87). |
| Chen et al., 2021, Taiwan [31] | Report the effects of COVID-19 on healthcare workers’ trauma andburnout and to analyse the factors associated with mental health outcomes | n = 12,596 | The proportion of participants who experienced high levels of DP was significantly higher for men (Women: 17.9%; Men: 22.3%) and those who worked in critical care units (Yes: 21.1%; No: 16.9%) and departments related to COVID-19 (Yes: 22.7%; No: 17.1%). The average score in lack of PA score was 19.0 8.4, indicating that the participants experienced a lack of PA to a small degree. |
| Jang et al., 2021, Korea [32] | To evaluate the current status of emotional exhaustion and peritraumatic distress in healthcareworkers (HCWs) in the COVID-19 pandemic, and identify factors associated with their mental health status | n = 1112 n nurses = 655 | Although no significant difference in peritraumatic distress was observed among the surveyed HCWs, the workers’ experiences of EE varied according to work characteristics. Responders who were female, older, living with a spouse, and/or full-time workers reported higher levels of EE. Public health officers and other medical personnel who did not have direct contact with confirmed patients and full-time workers had a higher level of peritraumatic distress. Forced involvement in work related to COVID-19, worry about stigma, worry about becoming infected, and perceived sufficiency of organisational support negatively predicted EE and peritraumatic distress. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lima, A.; Moreira, M.T.; Fernandes, C.; Ferreira, M.S.; Ferreira, M.; Teixeira, J.; Silva, M.; Parola, V.; Coelho, A. The Burnout of Nurses in Intensive Care Units and the Impact of the SARS-CoV-2 Pandemic: A Scoping Review. Nurs. Rep. 2023, 13, 230-242. https://doi.org/10.3390/nursrep13010022
Lima A, Moreira MT, Fernandes C, Ferreira MS, Ferreira M, Teixeira J, Silva M, Parola V, Coelho A. The Burnout of Nurses in Intensive Care Units and the Impact of the SARS-CoV-2 Pandemic: A Scoping Review. Nursing Reports. 2023; 13(1):230-242. https://doi.org/10.3390/nursrep13010022
Chicago/Turabian StyleLima, Andreia, Maria Teresa Moreira, Carla Fernandes, Maria Salomé Ferreira, Margarida Ferreira, Joana Teixeira, Mafalda Silva, Vítor Parola, and Adriana Coelho. 2023. "The Burnout of Nurses in Intensive Care Units and the Impact of the SARS-CoV-2 Pandemic: A Scoping Review" Nursing Reports 13, no. 1: 230-242. https://doi.org/10.3390/nursrep13010022