
Low-Frequency Air–Bone Gap and Pulsatile Tinnitus Due to a Dural Arteriovenous Fistula: Considerations upon Possible Pathomechanisms and Literature Review

 , ,
, ,  and
and
Abstract
:1. Introduction
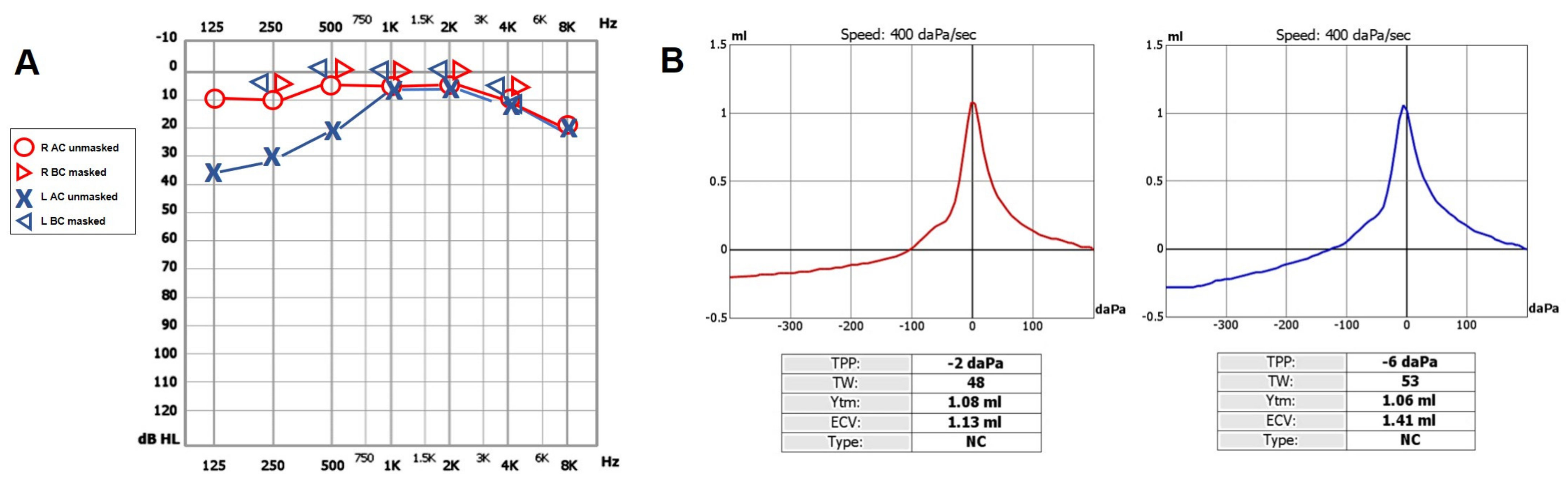
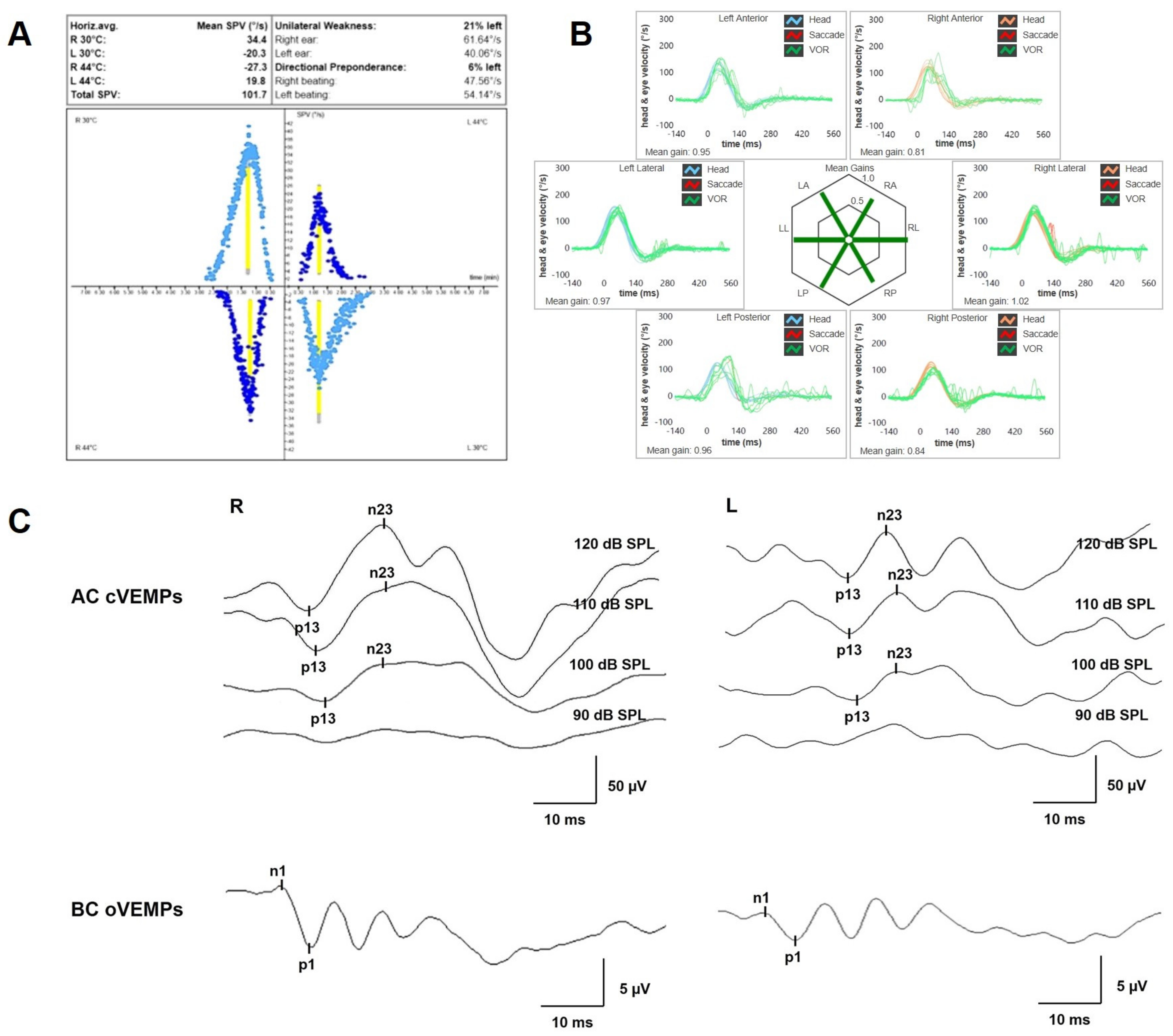
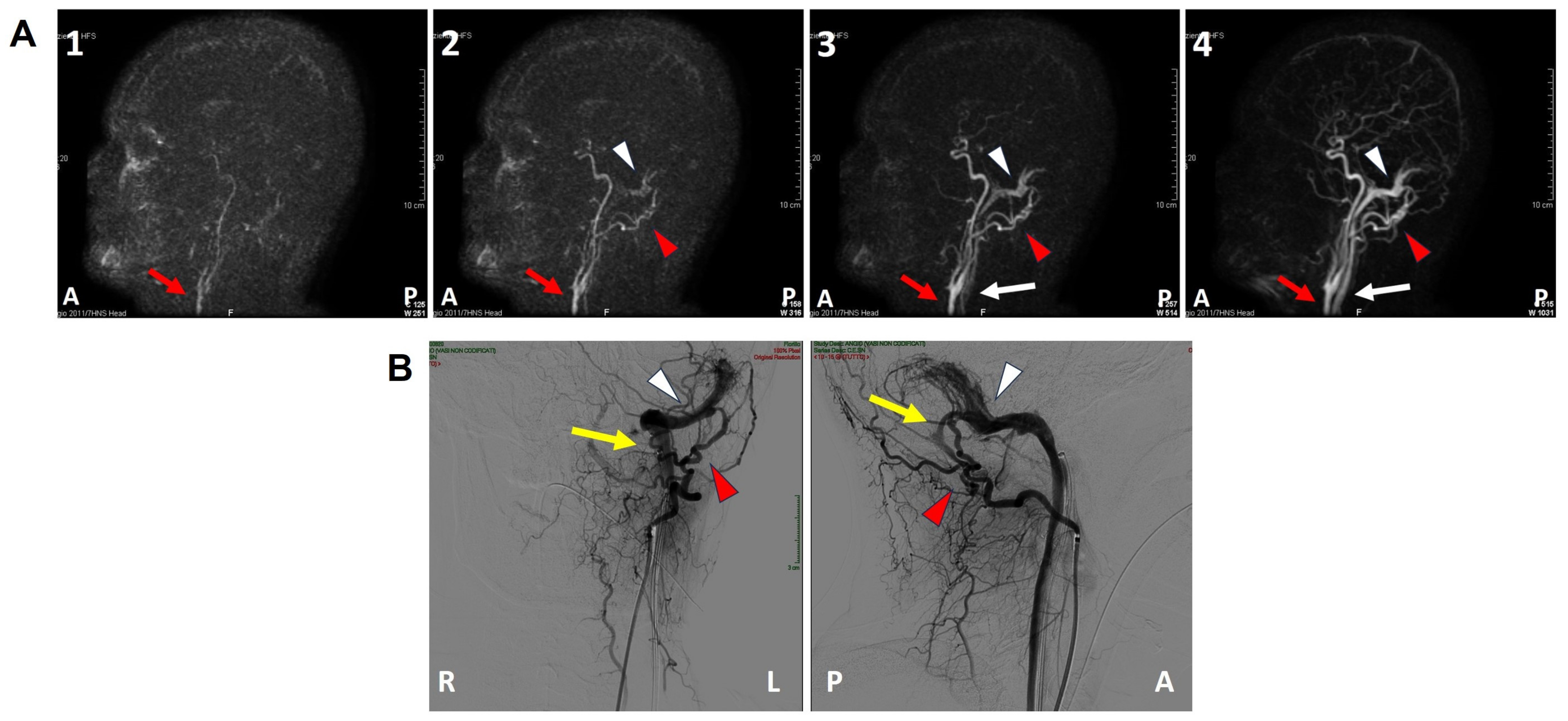
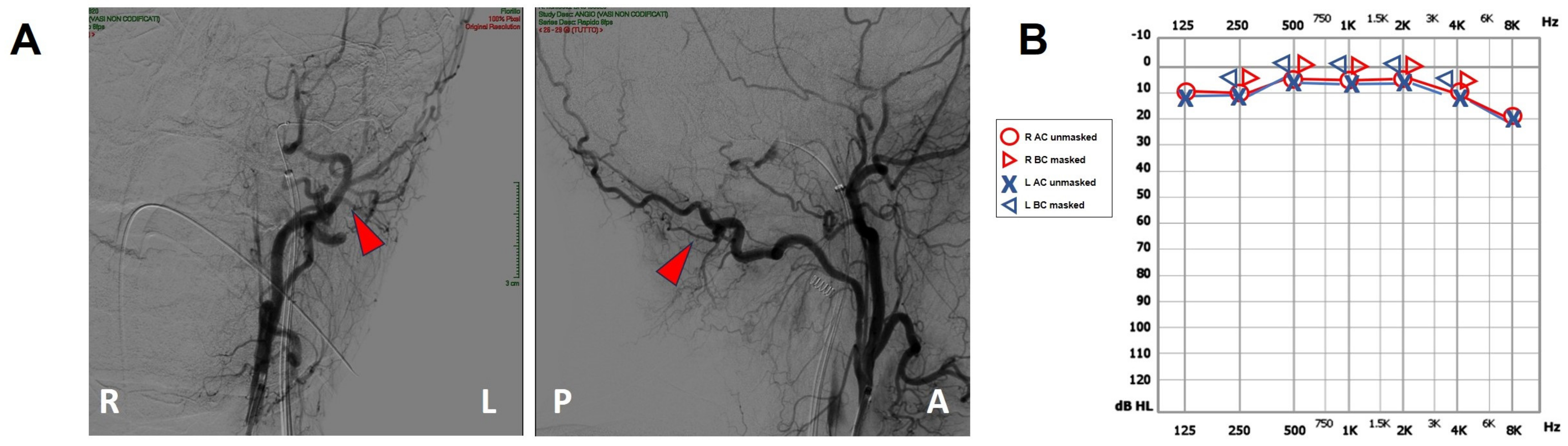
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Esmaili, A.A.; Renton, J. A Review of Tinnitus. Aust. J. Gen. Pract. 2018, 47, 205–208. [Google Scholar] [CrossRef]
- Narsinh, K.H.; Hui, F.; Saloner, D.; Tu-Chan, A.; Sharon, J.; Rauschecker, A.M.; Safoora, F.; Shah, V.; Meisel, K.; Amans, M.R. Diagnostic Approach to Pulsatile Tinnitus: A Narrative Review. JAMA Otolaryngol. Head Neck Surg. 2022, 148, 476. [Google Scholar] [CrossRef]
- Gandhi, D.; Chen, J.; Pearl, M.; Huang, J.; Gemmete, J.J.; Kathuria, S. Intracranial Dural Arteriovenous Fistulas: Classification, Imaging Findings, and Treatment. AJNR Am. J. Neuroradiol. 2012, 33, 1007–1013. [Google Scholar] [CrossRef]
- Kirsch, M.; Liebig, T.; Kühne, D.; Henkes, H. Endovascular Management of Dural Arteriovenous Fistulas of the Transverse and Sigmoid Sinus in 150 Patients. Neuroradiology 2009, 51, 477–483. [Google Scholar] [CrossRef]
- Chung, S.J.; Kim, J.S.; Kim, J.C.; Lee, S.K.; Kwon, S.U.; Lee, M.C.; Suh, D.C. Intracranial Dural Arteriovenous Fistulas: Analysis of 60 Patients. Cerebrovasc. Dis. 2002, 13, 79–88. [Google Scholar] [CrossRef]
- Van Dijk, J.M.C.; terBrugge, K.G.; Willinsky, R.A.; Wallace, M.C. Clinical Course of Cranial Dural Arteriovenous Fistulas With Long-Term Persistent Cortical Venous Reflux. Stroke 2002, 33, 1233–1236. [Google Scholar] [CrossRef]
- Borden, J.A.; Wu, J.K.; Shucart, W.A. A Proposed Classification for Spinal and Cranial Dural Arteriovenous Fistulous Malformations and Implications for Treatment. J. Neurosurg. 1995, 82, 166–179. [Google Scholar] [CrossRef]
- Cognard, C.; Gobin, Y.P.; Pierot, L.; Bailly, A.L.; Houdart, E.; Casasco, A.; Chiras, J.; Merland, J.J. Cerebral Dural Arteriovenous Fistulas: Clinical and Angiographic Correlation with a Revised Classification of Venous Drainage. Radiology 1995, 194, 671–680. [Google Scholar] [CrossRef]
- Padilha, I.G.; Pacheco, F.T.; Araujo, A.I.R.; Nunes, R.H.; Baccin, C.E.; Conti, M.L.M.; Maia Jr, A.C.M.; Rocha, A.J.D. Tips and Tricks in the Diagnosis of Intracranial Dural Arteriovenous Fistulas: A Pictorial Review. J. Neuroradiol. 2020, 47, 369–381. [Google Scholar] [CrossRef]
- Lv, X.; Jiang, C.; Li, Y.; Wu, Z. Results and Complications of Transarterial Embolization of Intracranial Dural Arteriovenous Fistulas Using Onyx-18: Clinical Article. J. Neurosurg. 2008, 109, 1083–1090. [Google Scholar] [CrossRef]
- See, A.P.; Raza, S.; Tamargo, R.J.; Lim, M. Stereotactic Radiosurgery of Cranial Arteriovenous Malformations and Dural Arteriovenous Fistulas. Neurosurg. Clin. N. Am. 2012, 23, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.H.; Choi, J.H.; Kim, B.-S.; Lee, K.S.; Shin, Y.S. Treatment Outcomes According to Various Treatment Modalities for Intracranial Dural Arteriovenous Fistulas in the Onyx Era: A 10-Year Single-Center Experience. World Neurosurg. 2019, 126, e825–e834. [Google Scholar] [CrossRef] [PubMed]
- Merchant, S.N.; Rosowski, J.J. Conductive Hearing Loss Caused by Third-Window Lesions of the Inner Ear. Otol. Neurotol. 2008, 29, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.-L.; Moonis, G.; Halpin, C.F.; Curtin, H.D. Spectrum of Third Window Abnormalities: Semicircular Canal Dehiscence and Beyond. AJNR Am. J. Neuroradiol. 2017, 38, 2–9. [Google Scholar] [CrossRef]
- Scarpa, A.; Ralli, M.; Cassandro, C.; Gioacchini, F.M.; Greco, A.; Stadio, A.D.; Cavaliere, M.; Troisi, D.; De Vincentiis, M.; Cassandro, E. Inner-Ear Disorders Presenting with Air–Bone Gaps: A Review. Int. Adv. Otol. 2020, 16, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Reynard, P.; Idriss, S.; Ltaief-Boudrigua, A.; Bertholon, P.; Pirvan, A.; Truy, E.; Thai-Van, H.; Ionescu, E.C. Proposal for a Unitary Anatomo-Clinical and Radiological Classification of Third Mobile Window Abnormalities. Front. Neurol. 2022, 12, 792545. [Google Scholar] [CrossRef]
- Bance, M. When Is a Conductive Hearing Loss Not a Conductive Hearing Loss? Causes of a Mismatch in Air-Bone Threshold Measurements or a “Pseudoconductive” Hearing Loss. J. Otolaryngol. 2004, 33, 135. [Google Scholar] [CrossRef]
- Zhou, G.; Poe, D.; Gopen, Q. Clinical Use of Vestibular Evoked Myogenic Potentials in the Evaluation of Patients With Air-Bone Gaps. Otol. Neurotol. 2012, 33, 1368–1374. [Google Scholar] [CrossRef]
- Iversen, M.M.; Rabbitt, R.D. Biomechanics of Third Window Syndrome. Front. Neurol. 2020, 11, 891. [Google Scholar] [CrossRef]
- Brantberg, K.; Bagger-Sjöbäck, D.; Mathiesen, T.; Witt, H.; Pansell, T. Posterior Canal Dehiscence Syndrome Caused by an Apex Cholesteatoma. Otol. Neurotol. 2006, 27, 531–534. [Google Scholar] [CrossRef]
- Blake, D.M.; Tomovic, S.; Vazquez, A.; Lee, H.; Jyung, R.W. Cochlear-facial Dehiscence—A Newly Described Entity. Laryngoscope 2014, 124, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Schneiders, S.M.D.; Rainsbury, J.W.; Hensen, E.F.; Irving, R.M. Superior Petrosal Sinus Causing Superior Canal Dehiscence Syndrome. J. Laryngol. Otol. 2017, 131, 593–597. [Google Scholar] [CrossRef] [PubMed]
- Castellucci, A.; Brandolini, C.; Piras, G.; Fernandez, I.J.; Giordano, D.; Pernice, C.; Modugno, G.C.; Pirodda, A.; Ferri, G.G. Superior Canal Dehiscence with Tegmen Defect Revealed by Otoscopy: Video Clip Demonstration of Pulsatile Tympanic Membrane. Auris Nasus Larynx 2018, 45, 165–169. [Google Scholar] [CrossRef]
- Thai, A.; Sayyid, Z.N.; Hosseini, D.K.; Swanson, A.; Ma, Y.; Aaron, K.A.; Vaisbuch, Y. Ambient Pressure Tympanometry Wave Patterns in Patients With Superior Semicircular Canal Dehiscence. Front. Neurol. 2020, 11, 379. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Son, S.-E.; Kim, M.B.; Cho, Y.S.; Chung, W.-H. Significance of Pseudo-Conductive Hearing Loss and Positional Nystagmus for Perilymphatic Fistula: Are They Related to Third-Window Effects? Clin. Exp. Otorhinolaryngol. 2021, 14, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Muchnik, C.; Hildesheimer, M.; Rubinstein, M.; Arenberg, I.K. Low Frequency Air-Bone Gap in Menière’s Disease without Middle Ear Pathology. A Preliminary Report. Am. J. Otol. 1989, 10, 1–4. [Google Scholar]
- Yetişer, S.; Kertmen, M. Cochlear Conductive Hearing Loss in Patients with Meniere’s Disease. Kulak Burun Bogaz Ihtis Derg 2007, 17, 18–21. [Google Scholar]
- Lee, H.J.; Jeon, J.H.; Park, S.; Kim, B.G.; Lee, W.-S.; Kim, S.H. Prevalence and Clinical Significance of Spontaneous Low-Frequency Air-Bone Gaps in Ménière’s Disease. Otol. Neurotol. 2014, 35, 489–494. [Google Scholar] [CrossRef]
- Slattery, E.L.; Babu, S.C.; Chole, R.A.; Zappia, J.J. Intralabyrinthine Schwannomas Mimic Cochleovestibular Disease: Symptoms From Tumor Mass Effect in the Labyrinth. Otol. Neurotol. 2015, 36, 167–171. [Google Scholar] [CrossRef]
- Sugimoto, S.; Yoshida, T.; Teranishi, M.; Okazaki, Y.; Naganawa, S.; Sone, M. The Relationship between Endolymphatic Hydrops in the Vestibule and Low-Frequency Air-Bone Gaps: Endolymphatic Hydrops and Air-Bone Gaps. Laryngoscope 2018, 128, 1658–1662. [Google Scholar] [CrossRef]
- Reda, J.D.; West, N.; Cayé-Thomasen, P. Intracochlear Vestibular Schwannoma Presenting with Mixed Hearing Loss. Int. Adv. Otol. 2021, 17, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Pai, I.; Connor, S. Low Frequency Air-Bone Gap in Meniere’s Disease: Relationship With Magnetic Resonance Imaging Features of Endolymphatic Hydrops. Ear Hear. 2022, 43, 1678–1686. [Google Scholar] [CrossRef] [PubMed]
- Maheu, M.; Alvarado-Umanzor, J.M.; Delcenserie, A.; Champoux, F. The Clinical Utility of Vestibular-Evoked Myogenic Potentials in the Diagnosis of Ménière’s Disease. Front. Neurol. 2017, 8, 415. [Google Scholar] [CrossRef] [PubMed]
- Rosengren, S.M.; Colebatch, J.G.; Young, A.S.; Govender, S.; Welgampola, M.S. Vestibular Evoked Myogenic Potentials in Practice: Methods, Pitfalls and Clinical Applications. Clin. Neurophysiol. Pract. 2019, 4, 47–68. [Google Scholar] [CrossRef]
- Cerchiai, N.; Navari, E.; Dallan, I.; Sellari-Franceschini, S.; Casani, A.P. Assessment of Vestibulo-Oculomotor Reflex in Ménière’s Disease: Defining an Instrumental Profile. Otol. Neurotol. 2016, 37, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Waissbluth, S.; Sepúlveda, V. Dissociation between Caloric and Video Head Impulse Tests in Dizziness Clinics. Audiol. Res. 2022, 12, 423–432. [Google Scholar] [CrossRef]
- Gürkov, R.; Flatz, W.; Louza, J.; Strupp, M.; Ertl-Wagner, B.; Krause, E. Herniation of the Membranous Labyrinth into the Horizontal Semicircular Canal is Correlated with Impaired Caloric Response in Ménière’s Disease. Otol. Neurotol. 2012, 33, 1375–1379. [Google Scholar] [CrossRef]
- McGarvie, L.A.; Curthoys, I.S.; MacDougall, H.G.; Halmagyi, G.M. What Does the Dissociation between the Results of Video Head Impulse versus Caloric Testing Reveal about the Vestibular Dysfunction in Ménière’s Disease? Acta Oto-Laryngol. 2015, 135, 859–865. [Google Scholar] [CrossRef]
- Cassandro, E.; Cassandro, C.; Sequino, G.; Scarpa, A.; Petrolo, C.; Chiarella, G. Inner Ear Conductive Hearing Loss and Unilateral Pulsatile Tinnitus Associated with a Dural Arteriovenous Fistula: Case Based Review and Analysis of Relationship between Intracranial Vascular Abnormalities and Inner Ear Fluids. Case Rep. Otolaryngol. 2015, 2015, 817313. [Google Scholar] [CrossRef]
- Brocks, C.; Bela, C.; Gaebel, C.; Wollenberg, B.; Sommer, K. Arteriovenöse Durafistel als seltene Ursache für einen pulssynchronen Tinnitus. Laryngo-Rhino-Otologie 2008, 87, 573–578. [Google Scholar] [CrossRef]
- Wigansari, G.P.A.; Sani, A.F.; Kurniawan, D.; Qimindra, F.R. Chronic Pulsatile Tinnitus and Continuous Vertigo Due to Very Delayed Diagnosis of Single Slow-Flow Dural Arteriovenous. J. Neurosci. Rural Pract. 2022, 14, 140–142. [Google Scholar] [CrossRef] [PubMed]
- Al-Abdulwahhab, A.H.; Al-Suhibani, S.; Al-Sharydah, A.M.; Al-Jubran, S.A.; Al-Thuneyyan, M.A. Multiple Dural Arteriovenous Fistulas Manifesting as Progressive Otalgia and Tinnitus and Treated Using a Single Session of Endovascular Embolization. Clin. Interv. Aging 2020, 15, 2313–2320. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, W.; Connor, S.; Obholzer, R.; Pai, I. A Dural Arteriovenous Fistula Associated with an Encephalocele Presenting as Otitis Media with Effusion. J. Laryngol. Otol. 2018, 132, 1032–1035. [Google Scholar] [CrossRef] [PubMed]
- Weider, D.J.; Kuo, A.; Spiegel, P.K.; Musiek, F.E. Objective Tinnitus of Vascular Origin with Hearing Improvement after Treatment. Am. J. Otolaryngol. 1990, 11, 437–443. [Google Scholar]
- Baum, G.; Turan, N.; Buonanno, F.; Pradilla, G.; Nogueira, R. Intracranial Dural Arteriovenous Fistula as a Cause for Symptomatic Superficial Siderosis: A Report of Two Cases and Review of the Literature. Surg. Neurol. Int. 2016, 7, 223. [Google Scholar] [CrossRef]
- Kritikos, M.E.; Oselkin, M.; Sharma, N.; Gopal, P.P.; Bigelow, D.C.; Grady, S.; Hurst, R.W.; Pukenas, B.A.; Choudhri, O.; Kung, D. Dural Arteriovenous Fistula Associated With a Vestibular Tumor: An Unusual Case and Review of the Literature. Cureus 2018, 10, e2890. [Google Scholar] [CrossRef]
- Kim, M.S.; Oh, C.W.; Han, D.H.; Kwon, O.-K.; Jung, H.-W.; Han, M.H. Intraosseous Dural Arteriovenous Fistula of the Skull Base Associated with Hearing Loss: Case Report. J. Neurosurg. 2002, 96, 952–955. [Google Scholar] [CrossRef]
- Gioppo, A.; Faragò, G.; Caldiera, V.; Caputi, L.; Cusin, A.; Ciceri, E. Medial Tentorial Dural Arteriovenous Fistula Embolization: Single Experience with Embolic Liquid Polymer SQUID and Review of the Literature. World Neurosurg. 2017, 107, 1050.e1–1050.e7. [Google Scholar] [CrossRef]
- Peto, I.; Abou-Al-Shaar, H.; Dehdashti, A.R. Surgical Disconnection of Posterior Fossa Right Tentorial Incisura Arteriovenous-Fistula Cognard IV. World Neurosurg. 2019, 127, 485. [Google Scholar] [CrossRef]
- Godlowski, Z. Hyperomosis of Endolymph as Primary Pathogenic Mechanism of Menière’s Disease and Its Clinical Management. Acta Otolaryngol. Suppl. 1972, 299, 1–36. [Google Scholar]
- Cognard, C.; Casasco, A.; Toevi, M.; Houdart, E.; Chiras, J.; Merland, J.-J. Dural Arteriovenous Fistulas as a Cause of Intracranial Hypertension Due to Impairment of Cranial Venous Outflow. J. Neurol. Neurosurg. Psychiatry 1998, 65, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Kühner, A.; Krastel, A.; Stoll, W. Arteriovenous Malformations of the Transverse Dural Sinus. J. Neurosurg. 1976, 45, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Rossitti, S. Pathophysiology of Increased Cerebrospinal Fluid Pressure Associated to Brain Arteriovenous Malformations: The Hydraulic Hypothesis. Surg. Neurol. Int. 2013, 4, 42. [Google Scholar] [CrossRef]
- Böhmer, A. Hydrostatic Pressure in the Inner Ear Fluid Compartments and Its Effects on Inner Ear Function. Acta Otolaryngol. Suppl. 1993, 507, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Hurst, R.W.; Hackney, D.B.; Goldberg, H.I.; Davis, R.A. Reversible Arteriovenous Malformation-Induced Venous Hypertension as a Cause of Neurological Deficits. Neurosurgery 1992, 30, 422–425. [Google Scholar] [CrossRef] [PubMed]
- Satzer, D.; Guillaume, D.J. Hearing Loss in Hydrocephalus: A Review, with Focus on Mechanisms. Neurosurg. Rev. 2016, 39, 13–25. [Google Scholar] [CrossRef]
- Barlas, O.; Gökay, H.; Turantan, M.İ.; Başerer, N. Adult Aqueductal Stenosis Presenting with Fluctuating Hearing Loss and Vertigo: Report of Two Cases. J. Neurosurg. 1983, 59, 703–705. [Google Scholar] [CrossRef]
- Dixon, J.F.; Jones, R.O. Hydrocephalus-Associated Hearing Loss and Resolution after Ventriculostomy. Otolaryngol.-Head Neck Surg. 2012, 146, 1037–1039. [Google Scholar] [CrossRef]
- Eggermont, J.J.; Schmidt, P.H. Meniere’s Disease: A Long-Term Follow-up Study of Hearing Loss. Ann. Otol. Rhinol. Laryngol. 1985, 94, 1–9. [Google Scholar] [CrossRef]
- Sun, Q.; Jiang, G.; Xiong, G.; Sun, W.; Wen, W.; Wei, F. Quantification of Endolymphatic Hydrops and Its Correlation with Meniere’s Disease Clinical Features. Clin. Otolaryngol. 2021, 46, 1354–1361. [Google Scholar] [CrossRef]
- Sone, M.; Yoshida, T.; Morimoto, K.; Teranishi, M.; Nakashima, T.; Naganawa, S. Endolymphatic Hydrops in Superior Canal Dehiscence and Large Vestibular Aqueduct Syndromes. Laryngoscope 2016, 126, 1446–1450. [Google Scholar] [CrossRef] [PubMed]
- Rah, Y.C.; Kim, A.R.; Koo, J.-W.; Lee, J.H.; Oh, S.; Choi, B.Y. Audiologic Presentation of Enlargement of the Vestibular Aqueduct According to the SLC 26 A 4 Genotypes: Audiologic Presentation of EVA. Laryngoscope 2015, 125, E216–E222. [Google Scholar] [CrossRef] [PubMed]
- Merchant, S.N.; Nakajima, H.H.; Halpin, C.; Nadol, J.B.; Lee, D.J.; Innis, W.P.; Curtin, H.; Rosowski, J.J. Clinical Investigation and Mechanism of Air-Bone Gaps in Large Vestibular Aqueduct Syndrome. Ann. Otol. Rhinol. Laryngol. 2007, 116, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Valvassori, G.E.; Clemis, J.D. The Large Vestibular Aqueduct Syndrome. Laryngoscope 1978, 88, 723–728. [Google Scholar] [CrossRef]
- Suri, N.M.; Prasad, A.R.; Sayani, R.K.; Anand, A.; Jaychandran, G. Cochlear Implantation in Children with Mondini Dysplasia: Our Experience. J. Laryngol. Otol. 2021, 135, 125–129. [Google Scholar] [CrossRef]
- Dettman, S.; Sadeghi-Barzalighi, A.; Ambett, R.; Dowell, R.; Trotter, M.; Briggs, R. Cochlear Implants in Forty-Eight Children with Cochlear and/or Vestibular Abnormality. Audiol. Neurotol. 2011, 16, 222–232. [Google Scholar] [CrossRef]
- Attanasio, G.; Cagnoni, L.; Masci, E.; Ciciarello, F.; Diaferia, F.; Bruno, A.; Greco, A.; De Vincentiis, M. Chronic Cerebrospinal Venous Insufficiency as a Cause of Inner Ear Diseases. Acta Oto-Laryngol. 2017, 137, 460–463. [Google Scholar] [CrossRef]
- Lopez-Escamez, J.A.; Carey, J.; Chung, W.H.; Goebel, J.A.; Magnusson, M.; Mandalà, M.; Newman-Toker, D.E.; Strupp, M.; Suzuki, M.; Trabalzini, F.; et al. Diagnostic criteria for Menière’s disease. J. Vestib. Res. 2015, 25, 1–7. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Borden Classification | Cognard Classification | ||
|---|---|---|---|
| Type I | Anterograde drainage into the dural sinus/meningeal vein | Type I | Anterograde drainage into venous sinus |
| Type II | Anterograde drainage into dural sinus and retrograde drainage into cortical veins | Type II:
| Drainage into main sinus with reflux into secondary sinus Drainage into main sinus with reflux into cortical vein Drainage into main sinus with reflux into secondary sinus and cortical veins |
| Type III | Isolated retrograde drainage:
| Type III | Direct cortical venous drainage without ectasia |
| Type IV | Direct cortical venous drainage with venous ectasia | ||
| Type V | Drainage into the spinal perimedullary veins | ||
| Author | Year | Study | DAVF Type | Hearing Loss | Treatment | Hearing Recovery |
|---|---|---|---|---|---|---|
| Weider D.J. [44] | 1990 | Case Report | / | SNHL | embolization | Yes |
| / | CHL | surgical resection | Yes | |||
| Kim M.S. et al. [47] | 2002 | Case Report | / | SNHL | embolization | No |
| Cassandro E. et al. [39] | 2015 | Case Report | II Cognard | CHL | Onyx glue embolization | Yes |
| Baum G.R. et al. [45] | 2016 | Case Report | III Borden | SNHL | Onyx glue embolization | No |
| Gioppo A. et al. [48] | 2017 | Case Report | III Cognard | / | squid embolization | / |
| Kritikos M.E. et al. [46] | 2018 | Case Report | IIa + b Cognard | SNHL | surgical resection + Onyx glue embolization | No |
| Peto I. et al. [49] | 2019 | Case Report | IV Cognard | / | surgical resection | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tozzi, A.; Castellucci, A.; Ferrulli, G.; Martellucci, S.; Malara, P.; Brandolini, C.; Armato, E.; Ghidini, A. Low-Frequency Air–Bone Gap and Pulsatile Tinnitus Due to a Dural Arteriovenous Fistula: Considerations upon Possible Pathomechanisms and Literature Review. Audiol. Res. 2023, 13, 833-844. https://doi.org/10.3390/audiolres13060073
Tozzi A, Castellucci A, Ferrulli G, Martellucci S, Malara P, Brandolini C, Armato E, Ghidini A. Low-Frequency Air–Bone Gap and Pulsatile Tinnitus Due to a Dural Arteriovenous Fistula: Considerations upon Possible Pathomechanisms and Literature Review. Audiology Research. 2023; 13(6):833-844. https://doi.org/10.3390/audiolres13060073
Chicago/Turabian StyleTozzi, Andrea, Andrea Castellucci, Giuseppe Ferrulli, Salvatore Martellucci, Pasquale Malara, Cristina Brandolini, Enrico Armato, and Angelo Ghidini. 2023. "Low-Frequency Air–Bone Gap and Pulsatile Tinnitus Due to a Dural Arteriovenous Fistula: Considerations upon Possible Pathomechanisms and Literature Review" Audiology Research 13, no. 6: 833-844. https://doi.org/10.3390/audiolres13060073