
Neuropsychology and Electroencephalography in Rural Children at Neurodevelopmental Risk: A Scoping Review

Abstract
:1. Introduction
2. Methodology
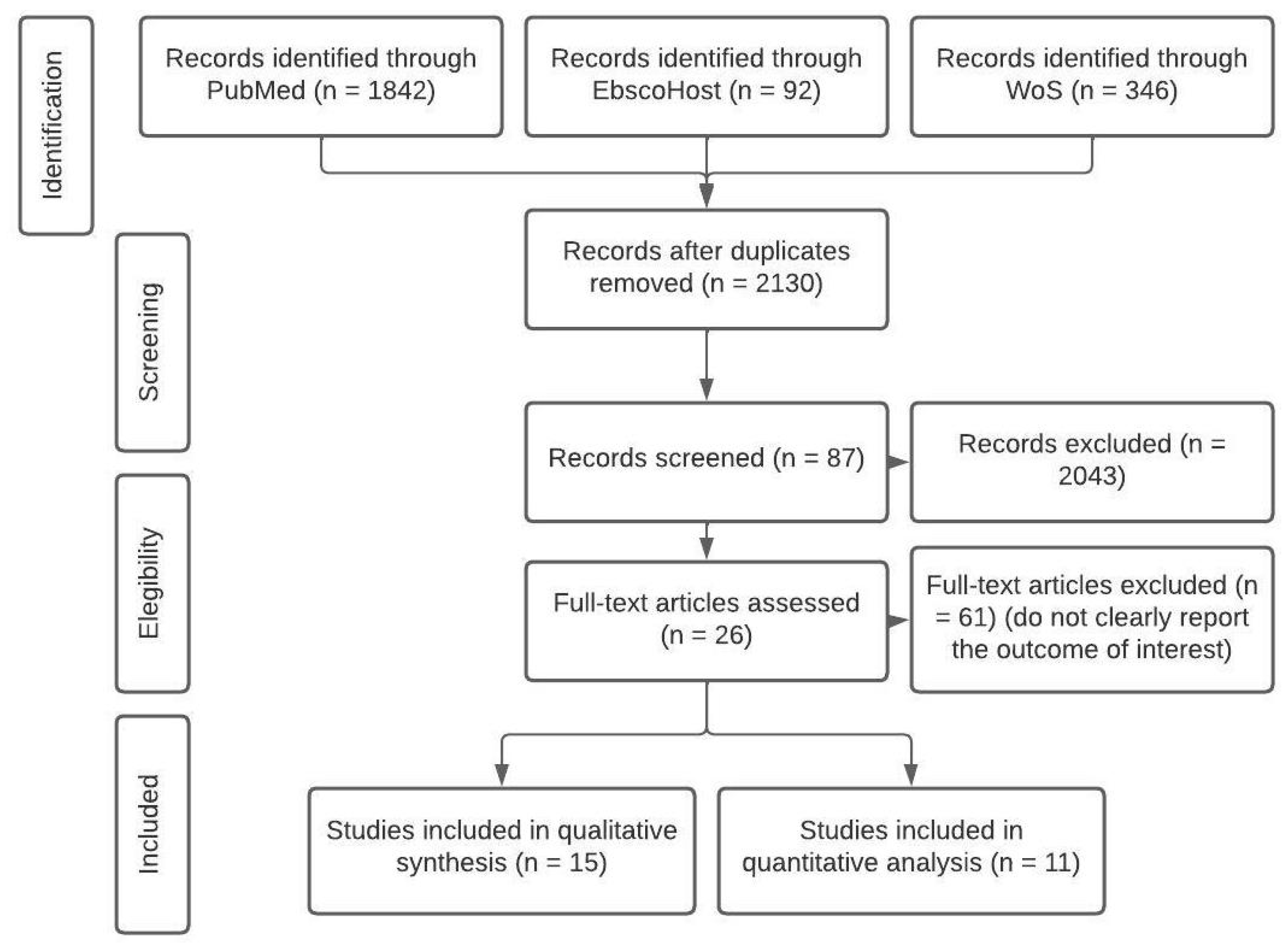
2.1. Search Strategy
2.2. Selection Process and Data Analysis
3. Results
3.1. Qualitative Synthesis
3.1.1. EEG in Children at Neurodevelopmental Risk

{kind=link}
{kind=link}
| EEG Finding | Brain Region | Neuropsychological Finding | n | Covariates | Control Group | Age | Country | Associated with Factor | Ref. |
|---|---|---|---|---|---|---|---|---|---|
| Sharp slow waves, slow waves, generalized sharp and slow waves, sharp and slow waves | Right parietal, bilateral centroparietal, right frontal, bifrontal | Soft neurological signs, poor performance in motor tasks, successive finger tapping, heel–toe tapping, alternating hand pronation supination | 208 | Movement coordination disorders | 35.5% normally nourished | 8–10 years | India | Malnourishment | [46] |
| Lower gamma power | Frontal, and parietal | Better executive function performance, verbal intelligence | 105 | Anemia | Longitudinal study. No control group | From birth, 24, and 48 months | Pakistan | Poverty | [54] |
| Decrease in relative delta and increase in alpha and beta powers | Right frontal, and parietal | Positive correlation with language, and motor development | 55 | Gestational age, body length and head circumference | Longitudinal study. No control group | Prenatal 2-year follow-up | Vietnam (US) | Dioxin in breast milk | [59] |
| Lower relative alpha, and higher relative theta power | Bilateral central, temporal, and parietal | Delayed gratification and non-verbal cognitive ability. Lower scores in risk exposure group for visual reception | 143 | Friendliness | Non-adopted children group | 18 months | US (international adoption) | Adoption, deprivation, parental exposure to drugs, parental malnourishment and premature birth | [60] |
| Decrease in alpha, high theta | Lingual gyrus, and inferior frontal gyrus orbital right middle temporal gyrus | WISC full-scale IQ | 108 | Classification techniques | Healthy classmates matched by age, gender, and handedness | 5–11 years | Caribbean islands | Protein undernutrition | [61] |
| Centro-parietal slow-wave, paroxysmal, and focal abnormalities. Slow increment (<5 Hz). Decrease in alpha power (8.9 Hz) | Fronto-central. Centro-parietal, frontal | NA | 108 | NA | Control recordings | 5–11 years | Barbados | Protein undernutrition | [62] |
| Abnormal slow wave background EEG tracings, paroxysmal activity | Not specified | NA | 194 | Parasitism, and goitre, iodine level | Control group | 9–13 years | Ecuador | Malnutrition | [63] |
| Bilateral slow waves, slow abnormal waves, sharp abnormal waves | Anterior brain areas, subcortical origin, Posterior regions | Reduced verbal abilities, problem solving/concentration, focus, and inhibition control/flexibility in at-risk groups | 194 | Infection protozoan parasite, parent’s education | Control group | 9–13 years | Ecuador | Malnutrition | [64] |
| Alpha 1 band, and alpha-beta power ratio during driving 8 Hz | Temporo–occipital | NA | 20 | Lethargic movement, depressed oxygen consumption, and sodium pump activity | Healthy control group | 5–23 months | Jamaica | Malnutrition, marasmus and kwashiorkor | [65] |
| Synchronous theta waves | Frontal and limbic | Motor and tactile perseverations, emotional-motivational regulation, poor communication skills | 172 | Learning difficulties | No control group | 10–12 years | Russia | NA | [56,57] |
| Less beta and alpha power after stimulus repetition reduced U-shaped pattern | Central | Repetition and change detection responses predicting adaptive functioning at preschool age. | 63 | Intellectual and adaptive functioning | Normocephalic and macrocephalic children | 3–11 months and 2 years follow-up | Canada | Autism spectrum disorder, attention deficit disorder with hyperactivity | [66] |
| Reduced phase locking value in alpha, theta, delta, and beta | Prefrontal regions | Not specified | 128 | Demographic variables | Orphans and controls | 8–18 years | China | HIV/AIDS | [67] |
| Reduced total absolute band power (alpha, beta, delta, theta) | Fp1, Fp2, P3, P4, T3, T4, O1, and O2 | Neurocognitive outcomes and language skills | 48 | Intelligence and adaptive skills | Preterm infants and control <31 weeks of gestation | 12 h after birth and 2 years | Norway | Extremely premature birth | [68] |
| Abnormal EEG grading | Frontal, temporal, central, and occipital | Neurocognitive outcomes | 70 | Cognitive outcomes | Control group by neurocognitive and EEG results | 32–35 weeks 2 years follow-up | Ireland | Preterm birth | [69] |
3.1.2. EEG, Environmental, and Social Risk Factors
3.2. Quantitative Analysis
4. Discussion
5. Current Limitations and Future Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| EEG | Electroencephalography |
| qEEG | Quantitative Electroencephalography |
| CNS | Central Nervous System |
| IQ | Intellectual Quotient |
References
- Buda, A.; Dean, O.; Adams, H.R.; Mwanza-Kabaghe, S.; Potchen, M.J.; Mbewe, E.G.; Kabundula, P.P.; Mweemba, M.; Matoka, B.; Mathews, M.; et al. Neighborhood-Based Socioeconomic Determinants of Cognitive Impairment in Zambian Children with HIV: A Quantitative Geographic Information Systems Approach. J. Pediatr. Infect. Dis. Soc. 2021, 10, 1071–1079. [Google Scholar] [CrossRef] [PubMed]
- D’Angiulli, A.; Lipina, S.J.; Olesinska, A. Explicit and implicit issues in the developmental cognitive neuroscience of social inequality. Front. Hum. Neurosci. 2012, 6, 254. [Google Scholar] [CrossRef] [PubMed]
- Olson, L.; Chen, B.; Fishman, I. Neural correlates of socioeconomic status in early childhood: A systematic review of the literature. Child Neuropsychol. 2021, 27, 390–423. [Google Scholar] [CrossRef]
- Tomasi, D.; Volkow, N.D. Effects of family income on brain functional connectivity in US children: Associations with cognition. Mol. Psychiatry 2023, 1–8. [Google Scholar] [CrossRef]
- Rakesh, D.; Whittle, S. Socioeconomic status and the developing brain—A systematic review of neuroimaging findings in youth. Neurosci. Biobehav. Rev. 2021, 130, 379–407. [Google Scholar] [CrossRef]
- Esqueda-Elizondo, J.J.; Juárez-Ramírez, R.; López-Bonilla, O.R.; García-Guerrero, E.E.; Galindo-Aldana, G.M.; Jiménez-Beristáin, L.; Serrano-Trujillo, A.; Tlelo-Cuautle, E.; Inzunza-González, E. Attention Measurement of an Autism Spectrum Disorder User Using EEG Signals: A Case Study. Math. Comput. Appl. 2022, 27, 21. [Google Scholar] [CrossRef]
- Ramírez-Arias, F.J.; García-Guerrero, E.E.; Tlelo-Cuautle, E.; Colores-Vargas, J.M.; García-Canseco, E.; López-Bonilla, O.R.; Galindo-Aldana, G.M.; Inzunza-González, E. Evaluation of Machine Learning Algorithms for Classification of EEG Signals. Technologies 2022, 10, 79. [Google Scholar] [CrossRef]
- Wu, W.; Ma, L.; Lian, B.; Cai, W.; Zhao, X. Few-Electrode EEG from the Wearable Devices Using Domain Adaptation for Depression Detection. Biosensors 2022, 12, 1087. [Google Scholar] [CrossRef]
- Jan, D.; de Vega, M.; López-Pigüi, J.; Padrón, I. Applying Deep Learning on a Few EEG Electrodes during Resting State Reveals Depressive States. A Data Driven Study. Brain Sci. 2022, 12, 1506. [Google Scholar] [CrossRef]
- Pfurtscheller, G.; Lopes da Silva, F.H. Event-related EEG/MEG synchronization and desynchronization: Basic principles. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 1999, 110, 1842–1857. [Google Scholar] [CrossRef]
- Selim, R.; Benbadis, M.; Aatif, M.; Husain, M.; Peter, W.; Kaplan, M.; William, O.; Tatum, I.V.D. Handbook of EEG Interpretation; Demos Medical: New York, NY, USA, 2008. [Google Scholar]
- Fried, S.; Moshé, S.L. Basic physiology of the EEG. Neurol. Asia 2011, 16, 23–25. [Google Scholar]
- Schomer, D.L.; Lopes da Silva, F.H. Niedermeyer’s Electroencephalography: Basic Principles, Clinical Applications, and Related Fields; Oxford University Press: Oxford, UK, 2017. [Google Scholar] [CrossRef]
- Jellinger, K.A. Niedermeyer’s Electroencephalography: Basic Principles, Clinical Applications, and Related Fields, 6th ed. In Eur. J. Neurol.; 2011; Volume 18, p. e126. [Google Scholar] [CrossRef]
- Miley, C.E.; Forster, F.M. Activation of partial complex seizures by hyperventilation. Arch. Neurol. 1977, 34, 371–373. [Google Scholar] [CrossRef] [PubMed]
- Blackstock, J.S.; Chae, K.B.; Mauk, G.W.; McDonald, A. Achieving Access to Mental Health Care for School-Aged Children in Rural Communities: A Literature Review. Rural Educ. 2018, 39, 12–25. [Google Scholar]
- Smith, S.L.; Franke, M.F.; Rusangwa, C.; Mukasakindi, H.; Nyirandagijimana, B.; Bienvenu, R.; Uwimana, E.; Uwamaliya, C.; Ndikubwimana, J.S.; Dorcas, S.; et al. Outcomes of a primary care mental health implementation program in rural Rwanda: A quasi-experimental implementation-effectiveness study. PLoS ONE 2020, 15, e0228854. [Google Scholar] [CrossRef] [PubMed]
- Crichlow, M.A.; Northover, P.; Giusti-Cordero, J. Race and Rurality in the Global Economy; SUNY Press: Albany, NY, USA, 2018. [Google Scholar]
- Bohem, R.; Visse, S. Book reviews. Prof. Geogr. 1986, 38, 430–457. [Google Scholar] [CrossRef]
- Warren, J.C.; Smalley, K.B. Rural Public Health: Best Practices and Preventive Models; Springer Publishing Company: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Allott, K.; Lloyd, S. The provision of neuropsychological services in rural/regional settings: Professional and ethical issues. Appl. Neuropsychol. 2009, 16, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Costa, L.G.; Cole, T.B.; Dao, K.; Chang, Y.C.; Coburn, J.; Garrick, J.M. Effects of air pollution on the nervous system and its possible role in neurodevelopmental and neurodegenerative disorders. Pharmacol. Ther. 2020, 210, 107523. [Google Scholar] [CrossRef]
- Luo, D.; Du, J.; Wang, P.; Yang, W. Urban-rural comparisons in health risk factor, health status and outcomes in Tianjin, China: A cross-sectional survey (2009–2013). Aust. J. Rural Health 2019, 27, 535–541. [Google Scholar] [CrossRef]
- Jiménez-Ceballos, B.; Martínez-Herrera, E.; Ocharan-Hernández, M.E.; Guerra-Araiza, C.; Farfán García, E.D.; Muñoz-Ramírez, U.E.; Fuentes-Venado, C.E.; Pinto-Almazán, R. Nutritional Status and Poverty Condition Are Associated with Depression in Preschoolers. Children 2023, 10, 835. [Google Scholar] [CrossRef]
- Doyle, C.; Cicchetti, D.; Georgieff, M.K.; Tran, P.V.; Carlson, E.S. Atypical fetal development: Fetal alcohol syndrome, nutritional deprivation, teratogens, and risk for neurodevelopmental disorders and psychopathology. Dev. Psychopathol. 2018, 30, 1063–1086. [Google Scholar]
- Smalley, K.B.; Warren, J.C.; Rainer, J. Rural Mental Health: Issues, Policies, and Best Practices; Springer Publishing Company: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Bell, E.; Merrick, J. Rural Child Health: International Aspects; Health and Human Development, Nova Science Publishers, Inc.: New York, NY, USA, 2010. [Google Scholar]
- Beck, S.; Wojdyla, D.; Say, L.; Betran, A.P.; Merialdi, M.; Requejo, J.H.; Rubens, C.; Menon, R.; Van Look, P.F.A. The worldwide incidence of preterm birth: A systematic review of maternal mortality and morbidity. Bull. World Health Organ. 2010, 88, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Chattopadhyay, N.; Mitra, K. Neurodevelopmental outcome of high risk newborns discharged from special care baby units in a rural district in India. J. Public Health Res. 2015, 4, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Doandes, F.M.; Manea, A.M.; Lungu, N.; Brandibur, T.; Cioboata, D.; Costescu, O.C.; Zaharie, M.; Boia, M. The Role of Amplitude-Integrated Electroencephalography (aEEG) in Monitoring Infants with Neonatal Seizures and Predicting Their Neurodevelopmental Outcome. Children 2023, 10, 833. [Google Scholar] [CrossRef] [PubMed]
- Galindo, G.; Solovieva, Y.; Machinskaya, R.; Quintanar, L. Atención selectiva visual en el procesamiento de letras: Un estudio comparative. OCNOS Rev. De Estud. Sobre Lect. 2016, 15, 69–80. [Google Scholar] [CrossRef]
- Barbiero, C.; Montico, M.; Lonciari, I.; Monasta, L.; Penge, R.; Vio, C.; Tressoldi, P.E.; Carrozzi, M.; De Petris, A.; De Cagno, A.G.; et al. The lost children: The underdiagnosis of dyslexia in Italy. A cross-sectional national study. PLoS ONE 2019, 14, e0210448. [Google Scholar] [CrossRef]
- Cainelli, E.; Vedovelli, L.; Carretti, B.; Bisiacchi, P. EEG correlates of developmental dyslexia: A systematic review. Ann. Dyslexia 2023, 73, 184–213. [Google Scholar] [CrossRef]
- Kong, A.H.; Lai, M.M.; Finnigan, S.; Ware, R.S.; Boyd, R.N.; Colditz, P.B. Background EEG features and prediction of cognitive outcomes in very preterm infants: A systematic review. Early Hum. Dev. 2018, 127, 74–84. [Google Scholar] [CrossRef]
- Lopez-Duran, N.L.; Nusslock, R.; George, C.; Kovacs, M. Frontal EEG asymmetry moderates the effects of stressful life events on internalizing symptoms in children at familial risk for depression. Psychophysiology 2012, 49, 510–521. [Google Scholar] [CrossRef]
- Gieron-Korthals, M.; Barness, L.A. Childhood Epilepsies and Brain Development (Book Review). Arch. Pediatr. Adolesc. Med. 2000, 154, 854. [Google Scholar]
- Gage, S.H.; Munaf, M.R.; Davey Smith, G. Causal Inference in Developmental Origins of Health and Disease (DOHaD) Research. Annu. Rev. Psychol. 2016, 67, 567–585. [Google Scholar] [CrossRef] [PubMed]
- Uauy, R.; Kain, J.; Corvalan, C. How can the Developmental Origins of Health and Disease (DOHaD) hypothesis contribute to improving health in developing countries? Am. J. Clin. Nutr. 2011, 94, 1759S–1764S. [Google Scholar] [CrossRef] [PubMed]
- Aihua, F.; Lijie, W.; Xiang, C.; Xiaoyan, L.; Ling, L.; Baozhen, W.; Huiwen, L.; Xiuting, M.; Ruoyan Gai, T. Developmental Origins of Health and Disease (DOHaD): Implications for health and nutritional issues among rural children in China. BioScience Trends 2015, 9, 82–87. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Corcino, C.O.; Teles, R.B.d.A.; Almeida, J.R.G.d.S.; Lirani, L.d.S.; Araújo, C.R.M.; Gonsalves, A.d.A.; Maia, G.L.d.A. Evaluation of the effect of pesticide use on the health of rural workers in irrigated fruit farming. Cienc. Saude Coletiva 2019, 24, 3117–3128. [Google Scholar] [CrossRef] [PubMed]
- Monjura, K.; Raynes-Greenow, C.; Aminur, R.; Ashraful, A. Correction: Perceptions and practices related to birthweight in rural Bangladesh: Implications for neonatal health programs in low- and middle-income settings. PLoS ONE 2020, 15, e0229165. [Google Scholar]
- Chanchani, D. Maternal and child nutrition in rural Chhattisgarh: The role of health beliefs and practices. Anthropol. Med. 2019, 26, 142–158. [Google Scholar] [CrossRef]
- Rohrer, J.E.; Borders, T.F.; Blanton, J. Rural residence is not a risk factor for frequent mental distress: A behavioral risk factor surveillance survey. BMC Public Health 2005, 5, 46. [Google Scholar] [CrossRef]
- Ueda, T.; Musha, T.; Asada, T.; Yagi, T. Classification Method for Mild Cognitive Impairment Based on Power Variability of EEG Using Only a Few Electrodes. Electron. Commun. Jpn. 2016, 99, 107–114. [Google Scholar] [CrossRef]
- Agarwal, K.N.; Das, D.; Agarwal, D.K.; Upadhyay, S.K.; Mishra, S. Soft neurological signs and EEG pattern in rural malnourished children. Acta Paediatr. Scand. 1989, 78, 873–878. [Google Scholar] [CrossRef]
- Beckwith, L.; Parmelee, A.H.J. EEG patterns of preterm infants, home environment, and later IQ. Child Dev. 1986, 57, 777–789. [Google Scholar] [CrossRef] [PubMed]
- Placencia, M.; Sander, J.W.; Roman, M.; Madera, A.; Crespo, F.; Cascante, S.; Shorvon, S.D. The characteristics of epilepsy in a largely untreated population in rural Ecuador. J. Neurol. Neurosurg. Psychiatry 1994, 57, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Cozac, V.V.; Chaturvedi, M.; Hatz, F.; Meyer, A.; Fuhr, P.; Gschwandtner, U. Increase of EEG Spectral Theta Power Indicates Higher Risk of the Development of Severe Cognitive Decline in Parkinson’s Disease after 3 Years. Front. Aging Neurosci. 2016, 8, 284. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.R.; Varcin, K.J.; O’Leary, H.M.; Tager-Flusberg, H.; Nelson, C.A. EEG power at 3 months in infants at high familial risk for autism. J. Neurodev. Disord. 2017, 9, 34. [Google Scholar] [CrossRef] [PubMed]
- Kanemura, H.; Sano, F.; Ohyama, T.; Mizorogi, S.; Sugita, K.; Aihara, M. EEG characteristics predict subsequent epilepsy in children with their first unprovoked seizure. Epilepsy Res. 2015, 115, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Ehlers, C.L.; Wall, T.L.; Garcia-Andrade, C.; Phillips, E. Effects of age and parental history of alcoholism on EEG findings in mission Indian children and adolescents. Alcohol. Clin. Exp. Res. 2001, 25, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Amores-Villalba, A.; Mateos-Mateos, R. Revisión de la neuropsicología del maltrato infantil: La neurobiología y el perfil neuropsicológico de las víctimas de abusos en la infancia. Psicol. Educ. 2017, 23, 81–88. [Google Scholar] [CrossRef]
- Tarullo, A.R.; Obradović, J.; Keehn, B.; Rasheed, M.A.; Siyal, S.; Nelson, C.A.; Yousafzai, A.K. Gamma power in rural Pakistani children: Links to executive function and verbal ability. Dev. Cogn. Neurosci. 2017, 26, 1–8. [Google Scholar] [CrossRef]
- Machinskaya, R.I.; Semenova, O.A.; Absatova, K.A.; Sugrobova, G.A. Neurophysiological factors associated with cognitive deficits in children with ADHD symptoms: EEG and neuropsychological analysis. Psychol. Neurosci. 2014, 7, 461–473. [Google Scholar] [CrossRef]
- Semenova, O.; Machinskaya, R. The influence of the functional state of brain regulatory systems on the efficiency of voluntary regulation of cognitive activity in children: II. neuropsychological and EEG analysis of brain regulatory functions in 10–12-year-old children with learning difficulties. Hum. Physiol. 2015, 41, 478–486. [Google Scholar]
- Kurgansky, A.; Machinskaya, R. Bilateral frontal theta-waves in EEG of 7–8-year-old children with learning difficulties: Qualitative and quantitative analysis. Hum. Physiol. 2012, 38, 255–263. [Google Scholar] [CrossRef]
- Machinskaya, R.; Kurgansky, A. Frontal bilateral synchronous theta waves and the resting EEG coherence in children aged 7–8 and 9–10 with learning difficulties. Hum. Physiol. 2013, 39, 58–67. [Google Scholar] [CrossRef]
- Nghiem, G.T.; Nishijo, M.; Pham, T.N.; Ito, M.; Pham, T.T.; Tran, A.H.; Nishimaru, H.; Nishino, Y.; Nishijo, H. Adverse effects of maternal dioxin exposure on fetal brain development before birth assessed by neonatal electroencephalography (EEG) leading to poor neurodevelopment; a 2-year follow-up study. Sci. Total Environ. 2019, 667, 718–729. [Google Scholar] [CrossRef] [PubMed]
- Tarullo, A.R.; Gunnar, M.R.; Garvin, M.C. Atypical EEG Power Correlates With Indiscriminately Friendly Behavior in Internationally Adopted Children. Dev. Psychol. 2011, 47, 417–431. [Google Scholar] [CrossRef] [PubMed]
- Bringas Vega, M.L.; Guo, Y.; Tang, Q.; Razzaq, F.A.; Calzada Reyes, A.; Ren, P.; Paz Linares, D.; Galan Garcia, L.; Rabinowitz, A.G.; Galler, J.R.; et al. An Age-Adjusted EEG Source Classifier Accurately Detects School-Aged Barbadian Children That Had Protein Energy Malnutrition in the First Year of Life. Front. Neurosci. 2019, 13, 1222. [Google Scholar] [CrossRef] [PubMed]
- Bringas-Vega, M.L.; Taboada-Crispi, A.; Bosch-Bayard, J.; Galán-García, L.; Bryce, C.; Rabinowitz, A.G.; Prichep, L.S.; Isenhart, R.; Calzada-Reyes, A.A.; Virues, T.; et al. F168. An EEG fingerprint of early protein-energy malnutrition. Clin. Neurophysiol. 2018, 129, e131. [Google Scholar] [CrossRef]
- Levav, M.; Cruz, M.E.; Mirsky, A.F. EEG abnormalities, malnutrition, parasitism and goitre: A study of schoolchildren in Ecuador. Acta Paediatr. 1995, 84, 197–202. [Google Scholar] [CrossRef]
- Levav, M.; Mirsky, A.F.; Schantz, P.M.; Castro, S.; Cruz, M.E. Parasitic infection in malnourished school children: Effects on behaviour and EEG. Parasitology 1995, 110 Pt 1, 103–111. [Google Scholar] [CrossRef]
- Robinson, S.; Young, R.E.; Golden, M.H. Electrophysiological assessment of brain function in severe malnutrition. Acta Paediatr. 1995, 84, 1245–1251. [Google Scholar] [CrossRef]
- Deguire, F.; López-Arango, G.; Knoth, I.S.; Côté, V.; Agbogba, K.; Lippé, S. EEG repetition and change detection responses in infancy predict adaptive functioning in preschool age: A longitudinal study. Sci. Rep. 2023, 13, 9980. [Google Scholar] [CrossRef]
- Gu, H.; Shan, X.; He, H.; Zhao, J.; Li, X. EEG Evidence of Altered Functional Connectivity and Microstate in Children Orphaned by HIV/AIDS. Front. Psychiatry 2022, 13, 898716. [Google Scholar] [CrossRef] [PubMed]
- Nordvik, T.; Schumacher, E.M.; Larsson, P.G.; Pripp, A.H.; Løhaugen, G.C.; Stiris, T. Early spectral EEG in preterm infants correlates with neurocognitive outcomes in late childhood. Pediatr. Res. 2022, 92, 1132–1139. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, R.O.; O’Toole, J.M.; Livingstone, V.; Filan, P.M.; Boylan, G.B. Can EEG accurately predict 2-year neurodevelopmental outcome for preterm infants? Arch. Dis. Childhood. Fetal Neonatal Ed. 2021, 106, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Cottrell, J.N.; Thomas, D.S.; Mitchell, B.L.; Childress, J.E.; Dawley, D.M.; Harbrecht, L.E.; Jude, D.A.; Valentovic, M.A. Rural and urban differences in prenatal exposure to essential and toxic elements. J. Toxicol. Environ. Health. Part A 2018, 81, 1214–1223. [Google Scholar] [CrossRef] [PubMed]
- Thatcher, R.W.; Lester, M.L. Nutrition, environmental toxins and computerized EEG: A mini-max approach to learning disabilities. J. Learn. Disabil. 1985, 18, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Urizar, G.G.J.; Caliboso, M.; Gearhart, C.; Yim, I.S.; Dunkel Schetter, C. Process Evaluation of a Stress Management Program for Low-Income Pregnant Women: The SMART Moms/Mamás LÍSTAS Project. Health Educ. Behav. Off. Publ. Soc. Public Health Educ. 2019, 46, 930–941. [Google Scholar] [CrossRef]
- Atif, N.; Nazir, H.; Zafar, S.; Chaudhri, R.; Atiq, M.; Mullany, L.C.; Rowther, A.A.; Malik, A.; Surkan, P.J.; Rahman, A. Development of a Psychological Intervention to Address Anxiety During Pregnancy in a Low-Income Country. Front. Psychiatry 2020, 10, 927. [Google Scholar] [CrossRef]
- St John, A.M.; Kao, K.; Liederman, J.; Grieve, P.G.; Tarullo, A.R. Maternal cortisol slope at 6 months predicts infant cortisol slope and EEG power at 12 months. Dev. Psychobiol. 2017, 59, 787–801. [Google Scholar] [CrossRef]
- Blair, C.; Berry, D.J. Moderate within-person variability in cortisol is related to executive function in early childhood. Psychoneuroendocrinology 2017, 81, 88–95. [Google Scholar] [CrossRef]
- John, E.R.; Ahn, H.; Prichep, L.; Trepetin, M.; Brown, D.; Kaye, H. Developmental equations for the electroencephalogram. Science 1980, 210, 1255–1258. [Google Scholar] [CrossRef]
- LeBourgeois, M.K.; Dean, D.C.; Deoni, S.C.L.; Kohler, M.; Kurth, S. A simple sleep EEG marker in childhood predicts brain myelin 3.5 years later. NeuroImage 2019, 199, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari-Rafi, A.; Mehdizadeh, R.; Ghaffari-Rafi, S.; Leon-Rojas, J. Demographic and socioeconomic disparities of benign and malignant spinal meningiomas in the United States. Neuro-Chirurgie 2021, 67, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Katus, L.; Mason, L.; Milosavljevic, B.; McCann, S.; Rozhko, M.; Moore, S.E.; Elwell, C.E.; Lloyd-Fox, S.; de Haan, M. ERP markers are associated with neurodevelopmental outcomes in 1-5 month old infants in rural Africa and the UK. NeuroImage 2020, 210, 116591. [Google Scholar] [CrossRef] [PubMed]
- Mattsson, P.; Tomson, T.; Edebol Eeg-Olofsson, K.; Brännström, L.; Ringbäck Weitoft, G. Association between sociodemographic status and antiepileptic drug prescriptions in children with epilepsy. Epilepsia 2012, 53, 2149–2155. [Google Scholar] [CrossRef]
- Kariuki, S.M.; Matuja, W.; Akpalu, A.; Kakooza-Mwesige, A.; Chabi, M.; Wagner, R.G.; Connor, M.; Chengo, E.; Ngugi, A.K.; Odhiambo, R.; et al. Clinical features, proximate causes, and consequences of active convulsive epilepsy in Africa. Epilepsia 2014, 55, 76–85. [Google Scholar] [CrossRef]
- Chidi, I.R.; Chidi, N.A.; Ebele, A.A.; Chinyelu, O.N. Co-Morbidity of attention deficit Hyperactivity Disorder (ADHD) and epilepsy In children seen In University of Nigeria Teaching Hospital Enugu: Prevalence, Clinical and social correlates. Niger. Postgrad. Med. J. 2014, 21, 273–278. [Google Scholar] [CrossRef]
- Burton, K.J.; Rogathe, J.; Whittaker, R.; Mankad, K.; Hunter, E.; Burton, M.J.; Todd, J.; Neville, B.G.R.; Walker, R.; Newton, C.R.J.C. Epilepsy in Tanzanian children: Association with perinatal events and other risk factors. Epilepsia 2012, 53, 752–760. [Google Scholar] [CrossRef]
- Kihara, M.; de Haan, M.; Garrashi, H.H.; Neville, B.G.R.; Newton, C.R.J.C. Atypical brain response to novelty in rural African children with a history of severe falciparum malaria. J. Neurol. Sci. 2010, 296, 88–95. [Google Scholar] [CrossRef]
- Kihara, M.; Hogan, A.M.; Newton, C.R.; Garrashi, H.H.; Neville, B.R.; de Haan, M. Auditory and visual novelty processing in normally-developing Kenyan children. Clin. Neurophysiol. 2010, 121, 564–576. [Google Scholar] [CrossRef]
- Burton, K.; Rogathe, J.; Whittaker, R.G.; Mankad, K.; Hunter, E.; Burton, M.J.; Todd, J.; Neville, B.G.R.; Walker, R.; Newton, C.R.J.C. Co-morbidity of epilepsy in Tanzanian children: A community-based case-control study. Seizure 2012, 21, 169–174. [Google Scholar] [CrossRef]
- Kariuki, S.M.; White, S.; Chengo, E.; Wagner, R.G.; Ae-Ngibise, K.A.; Kakooza-Mwesige, A.; Masanja, H.; Ngugi, A.K.; Sander, J.W.; Neville, B.G.; et al. Electroencephalographic features of convulsive epilepsy in Africa: A multicentre study of prevalence, pattern and associated factors. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2016, 127, 1099–1107. [Google Scholar] [CrossRef] [PubMed]
- Wenger, M.J.; Murray Kolb, L.E.; Scott, S.P.; Boy, E.; Haas, J.D. Modeling relationships between iron status, behavior, and brain electrophysiology: Evidence from a randomized study involving a biofortified grain in Indian adolescents. BMC Public Health 2022, 22, 1619. [Google Scholar]
- Marcos-Vidal, L.; Martínez-García, M.; Pretus, C.; Garcia-Garcia, D.; Martínez, K.; Janssen, J.; Vilarroya, O.; Castellanos, F.X.; Desco, M.; Sepulcre, J.; et al. Local functional connectivity suggests functional immaturity in children with attention-deficit/hyperactivity disorder. Hum. Brain Mapp. 2018, 39, 2442–2454. [Google Scholar] [CrossRef]
- Cao, Q.; Zang, Y.; Sun, L.; Sui, M.; Long, X.; Zou, Q.; Wang, Y. Abnormal neural activity in children with attention deficit hyperactivity disorder: A resting-state functional magnetic resonance imaging study. Neuroreport 2006, 17, 1033–1036. [Google Scholar] [CrossRef] [PubMed]
- Casey, B.J.; Castellanos, F.X.; Giedd, J.N.; Marsh, W.L.; Hamburger, S.D.; Schubert, A.B.; Vauss, Y.C.; Vaituzis, A.C.; Dickstein, D.P.; Sarfatti, S.E.; et al. Implication of right frontostriatal circuitry in response inhibition and attention-deficit/hyperactivity disorder. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 374–383. [Google Scholar] [CrossRef]
- O’Shea, A.; Ahmed, R.; Lightbody, G.; Pavlidis, E.; Lloyd, R.; Pisani, F.; Marnane, W.; Mathieson, S.; Boylan, G.; Temko, A. Deep Learning for EEG Seizure Detection in Preterm Infants. Int. J. Neural Syst. 2021, 31, 2150008. [Google Scholar] [CrossRef] [PubMed]
- Nguyen Huy, H.; Van Nguyen, L. Short report: Mental health problems among left-behind children in Vietnam: Prevalence and an examination of social support and parent-child communication as protective factors. Psychol. Health Med. 2023, 28, 876–883. [Google Scholar] [CrossRef]
- Wild, C.P. Complementing the genome with an “exposome”: The outstanding challenge of environmental exposure measurement in molecular epidemiology. Cancer Epidemiol. Biomarkers Prev. 2005, 14, 1847–1850. [Google Scholar] [CrossRef]
- Tamiz, A.P.; Koroshetz, W.J.; Dhruv, N.T.; Jett, D.A. A focus on the neural exposome. Neuron 2022, 110, 1286–1289. [Google Scholar] [CrossRef]
- Gabard-Durnam, L.J.; Wilkinson, C.; Kapur, K.; Tager-Flusberg, H.; Levin, A.R.; Nelson, C.A. Longitudinal EEG power in the first postnatal year differentiates autism outcomes. Nat. Commun. 2019, 10, 4188. [Google Scholar] [CrossRef]
- Scher, M.S. Automated EEG-sleep analyses and neonatal neurointensive care. Sleep Med. 2004, 5, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Scher, M.S.; Ludington-Hoe, S.; Kaffashi, F.; Johnson, M.W.; Holditch-Davis, D.; Loparo, K.A. Neurophysiologic assessment of brain maturation after an 8-week trial of skin-to-skin contact on preterm infants. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2009, 120, 1812–1818. [Google Scholar] [CrossRef] [PubMed]
- Garmendia, M.L.; Corvalan, C.; Uauy, R. Assessing the Public Health Impact of Developmental Origins of Health and Disease (DOHaD) Nutrition Interventions. Ann. Nutr. Metab. 2014, 64, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Kusin, S.M. Teachers’ Teaching Capability in Urban and Rural Areas: A Comparative Study. Int. J. Multidiscip. Appl. Bus. Educ. Res. 2022, 3, 2432–2439. [Google Scholar] [CrossRef]
- Zhang, J.; Jin, S.; Torero, M.; Li, T. Teachers and Urban-Rural Gaps in Educational Outcomes. Am. J. Agric. Econ. 2018, 100, 1207–1223. [Google Scholar] [CrossRef]
- Han, J.; Hao, Y.; Cui, N.; Wang, Z.; Lyu, P.; Yue, L. Parenting and parenting resources among Chinese parents with children under three years of age: Rural and urban differences. BMC Prim. Care 2023, 24, 38. [Google Scholar] [CrossRef]
- Jakovljević, T.; Janković, M.M.; Savić, A.M.; Soldatović, I.; Čolić, G.; Jakulin, T.J.; Papa, G.; Ković, V. The Relation between Physiological Parameters and Colour Modifications in Text Background and Overlay during Reading in Children with and without Dyslexia. Brain Sci. 2021, 11, 539. [Google Scholar] [CrossRef]
- Lin, J.J.; Dabbs, K.; Riley, J.D.; Jones, J.E.; Jackson, D.C.; Hsu, D.A.; Stafstrom, C.E.; Seidenberg, M.; Hermann, B.P. Neurodevelopment in new-onset juvenile myoclonic epilepsy over the first 2 years. Ann. Neurol. 2014, 76, 660–668. [Google Scholar] [CrossRef]
- Operto, F.F.; Pastorino, G.M.G.; Mazza, R.; Carotenuto, M.; Roccella, M.; Marotta, R.; di Bonaventura, C.; Verrotti, A. Effects on executive functions of antiepileptic monotherapy in pediatric age. Epilepsy Behav. 2020, 102, 106648. [Google Scholar] [CrossRef]
- Liu, X. Construction of Rural Left-Behind Children’s Mental Health Mobile Information System Based on the Internet of Things. Mob. Inf. Syst. 2021, 2021, 5490243. [Google Scholar] [CrossRef]
- Forman, M.R. Mapping a prevention strategy to reduce medically indicated preterm births: A trio of low-risk modifiable factors for the triad of the mother, fetus, and placenta. Am. J. Clin. Nutr. 2021, 114, 410–411. [Google Scholar] [CrossRef] [PubMed]
- Scher, M.S. A Bio-Social Model during the First 1000 Days Optimizes Healthcare for Children with Developmental Disabilities. Biomedicines 2022, 10, 3290. [Google Scholar] [CrossRef]
- Sripada, K.; Bjuland, K.J.; Sølsnes, A.E.; Håberg, A.K.; Grunewaldt, K.H.; Løhaugen, G.C.; Rimol, L.M.; Skranes, J. Trajectories of brain development in school-age children born preterm with very low birth weight. Sci. Rep. 2018, 8, 15553. [Google Scholar] [CrossRef] [PubMed]
- Nalivaeva, N.N.; Turner, A.J.; Zhuravin, I.A. Role of Prenatal Hypoxia in Brain Development, Cognitive Functions, and Neurodegeneration. Front. Neurosci. 2018, 12, 825. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, A.L.B.; Wilkening, G.; Aalborg, J.; Ringham, B.M.; Glueck, D.H.; Tregellas, J.R.; Dabelea, D. Childhood Metabolic Biomarkers Are Associated with Performance on Cognitive Tasks in Young Children. J. Pediatr. 2019, 211, 92–97. [Google Scholar] [CrossRef]
- Shapiro, K.A.; Kim, H.; Mandelli, M.L.; Rogers, E.E.; Gano, D.; Ferriero, D.M.; Barkovich, A.J.; Gorno-Tempini, M.L.; Glass, H.C.; Xu, D. Early changes in brain structure correlate with language outcomes in children with neonatal encephalopathy. NeuroImage Clin. 2017, 15, 572–580. [Google Scholar] [CrossRef]
- Barch, D.M. Introduction to the Special Issue on the Exposome-Understanding Environmental Impacts on Brain Development and Risk for Psychopathology. Biol. Psychiatry Glob. Open Sci. 2022, 2, 193–196. [Google Scholar] [CrossRef]
- Calamandrei, G.; Ricceri, L.; Meccia, E.; Tartaglione, A.M.; Horvat, M.; Tratnik, J.S.; Mazej, D.; Špirić, Z.; Prpić, I.; Vlašić-Cicvarić, I.; et al. Pregnancy exposome and child psychomotor development in three European birth cohorts. Environ. Res. 2020, 181, 108856. [Google Scholar] [CrossRef]
- Jamnik, T.; Flasch, M.; Braun, D.; Fareed, Y.; Wasinger, D.; Seki, D.; Berry, D.; Berger, A.; Wisgrill, L.; Warth, B. Next-generation biomonitoring of the early-life chemical exposome in neonatal and infant development. Nat. Commun. 2022, 13, 2653. [Google Scholar] [CrossRef]
- Rose, N.; Birk, R.; Manning, N. Towards Neuroecosociality: Mental Health in Adversity. Theory Cult. Soc. 2022, 39, 121–144. [Google Scholar] [CrossRef]
- Gladstone, M.; Abubakar, A.; Idro, R.; Langfitt, J.; Newton, C.R. Measuring neurodevelopment in low-resource settings. Lancet Child Adolesc. Health 2017, 1, 258–259. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Bertrand, K.; Naviaux, J.C.; Monk, J.M.; Wells, A.; Wang, L.; Lingampelly, S.S.; Naviaux, R.K.; Chambers, C. Metabolomic and exposomic biomarkers of risk of future neurodevelopmental delay in human milk. Pediatr. Res. 2023, 93, 1710–1720. [Google Scholar] [CrossRef] [PubMed]


| Study Types (%) | Study Control (%) | Health-Related Condition (%) |
|---|---|---|
| Prevalence (28) | Comparative (20) | Epilepsy-related events * (16) |
| Cross-sectional (16) | Randomly assigned (4) | Falciparum malaria (4) |
| Cohort (12) | Control groups (4) | Illiterate family (4) |
| Transversal Survey (12) | Assigned (4) | Preterm (4) |
| Case–control (8) | Randomized (4) | Studies reporting specific |
| EEG health-related conditions (72) | ||
| Longitudinal (8) | Randomly (4) | |
| Age-matched (8) | Trial (4) | |
| Healthy controls (4) | Not clearly identified (56) | |
| Observational (4) | - |
| Reference | EEG Technique | n | Age | p-Value | r | 95% CI Upper Limit | 95% CI Lower Limit | Fisher’s Zr |
|---|---|---|---|---|---|---|---|---|
| [80] | EEG seizures report | 1014 | 0–17 years | <0.01 | 0.0809 | 0.0194 | 0.1417 | 0.081 |
| [84] | ERPs | 50 | 6–7 years | 0.450 | - | - | - | - |
| [85] | ERPs | 178 | 4–12 years | 0.651 | - | - | - | - |
| [81] | EEG seizures report | 494 | † | <0.001 | 0.1476 | 0.0602 | 0.2328 | 0.1487 |
| [82] | EEG seizures report | 16 | † | <0.001 | 0.7419 | 0.3895 | 0.3895 | 0.9548 ** |
| [86] | EEG seizures report | 72 | 6–14 years | † | 0.3798 | 0.1624 | 0.562 | 0.3998 ** |
| [87] | EEG seizures report | 679 | † | † | 0.0833 | 0.0081 | 0.1575 | 0.0835 |
| [83] | EEG seizures report | 112 | 6–14 years | <0.001 | 0.126 | 0.0513 | 0.1994 | 0.1267 |
| [79] | ERPs | 148 | 1–5 months | 0.356 | 0.356 | 0.2065 | 0.4892 | 0.3723 ** |
| [54] | EEG gamma power | 105 | 0–24 months | 0.036 | 0.2049 | 0.0138 | 0.3816 | 0.2079 |
| [88] | EEG alpha and gamma power | 41 | 12–16 years | <0.01 | 0.0016 | −0.3062 | 0.3091 | 0.0016 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galindo-Aldana, G.; Torres-González, C. Neuropsychology and Electroencephalography in Rural Children at Neurodevelopmental Risk: A Scoping Review. Pediatr. Rep. 2023, 15, 722-740. https://doi.org/10.3390/pediatric15040065
Galindo-Aldana G, Torres-González C. Neuropsychology and Electroencephalography in Rural Children at Neurodevelopmental Risk: A Scoping Review. Pediatric Reports. 2023; 15(4):722-740. https://doi.org/10.3390/pediatric15040065
Chicago/Turabian StyleGalindo-Aldana, Gilberto, and Cynthia Torres-González. 2023. "Neuropsychology and Electroencephalography in Rural Children at Neurodevelopmental Risk: A Scoping Review" Pediatric Reports 15, no. 4: 722-740. https://doi.org/10.3390/pediatric15040065