

Association between Children’s Difficulties, Parent-Child Sleep, Parental Control, and Children’s Screen Time: A Cross-Sectional Study in Japan
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Study Design and Participants
2.3. Procedures and Measures
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
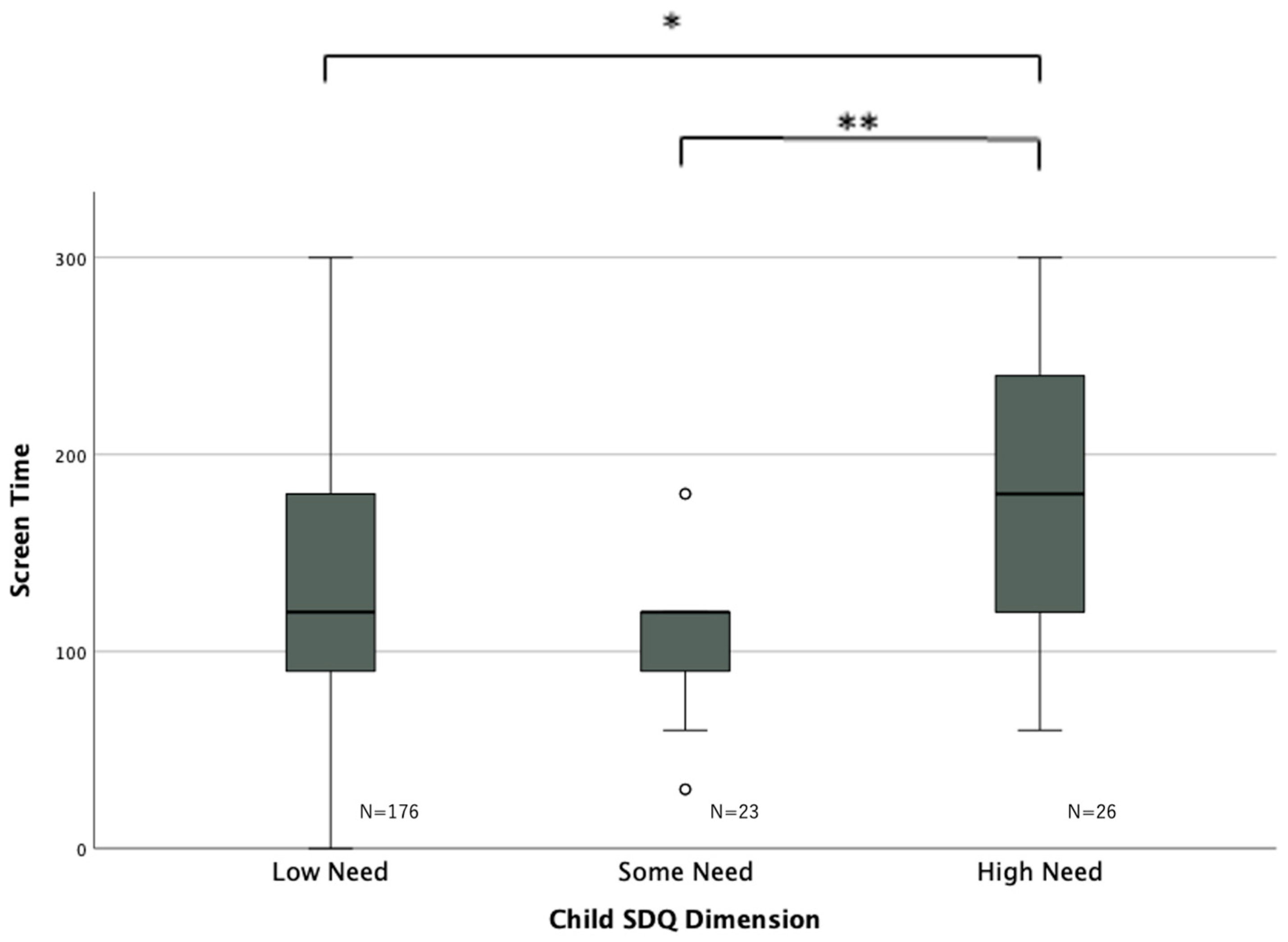
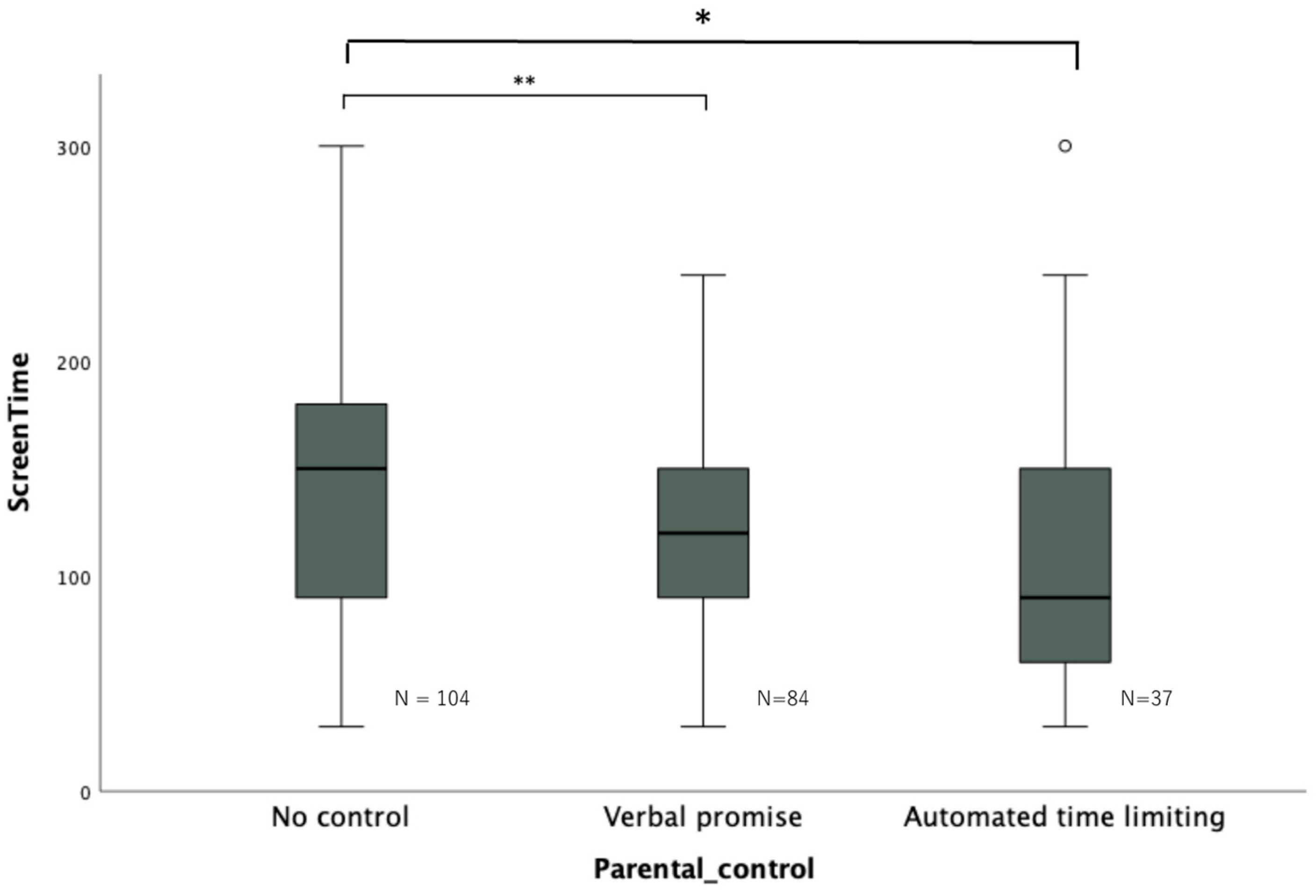
3.2. Association between Screen Time and SDQ, Sleep Variables, and Parental Control
3.3. Stepwise Multiple Linear Regression Analysis for Children’s Screen Time
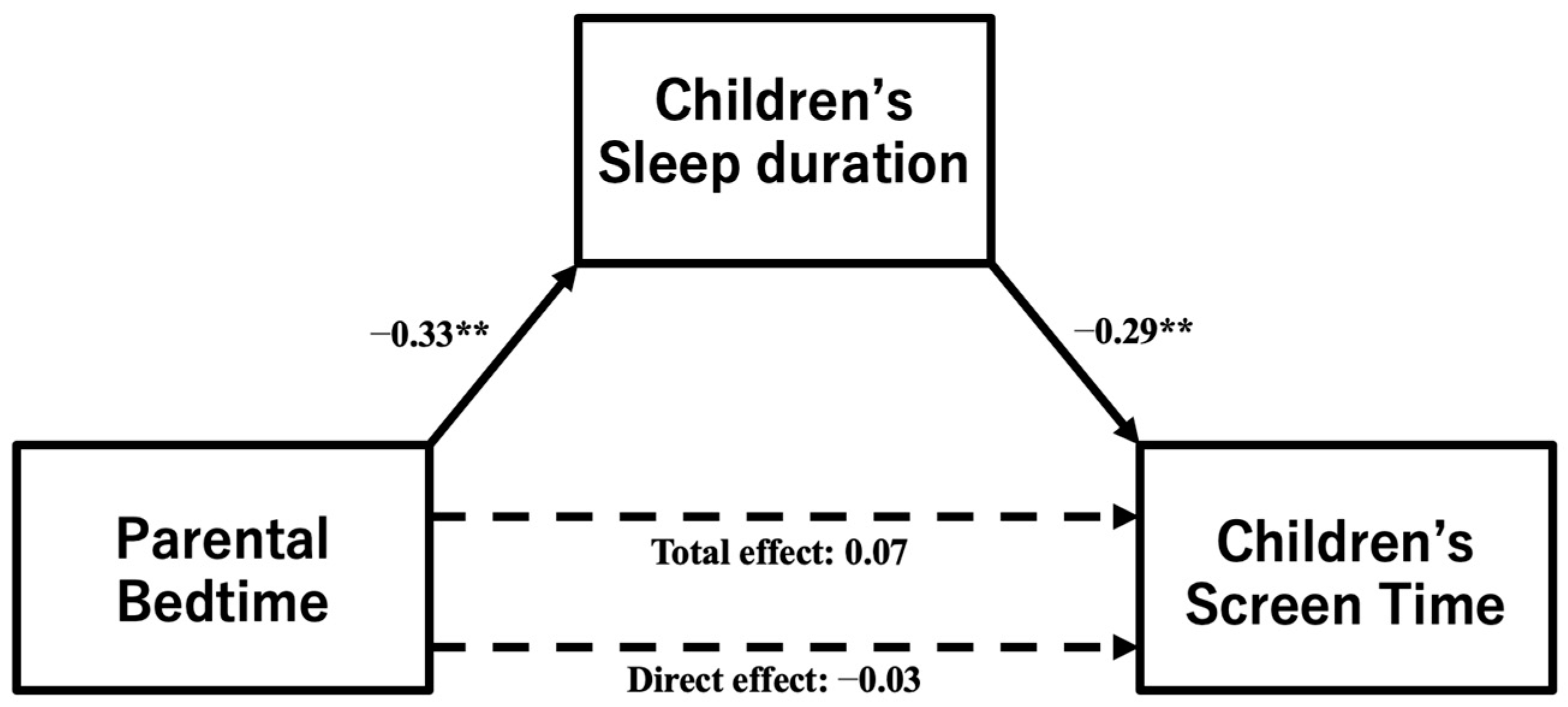
3.4. Indirect Effect of Parental Bedtime on Children’s Screen Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brzęk, A.; Strauss, M.; Sanchis-Gomar, F.; Leischik, R. Physical Activity, Screen Time, Sedentary and Sleeping Habits of Polish Preschoolers during the COVID-19 Pandemic and WHO’s Recommendations: An Observational Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 11173. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Education, Culture, Sports, Science, and Technology-Japan. The Realization of the GIGA School Concept. 2019. Available online: https://www.mext.go.jp/a_menu/other/index_00001.htm (accessed on 10 October 2023).
- Schmidt, M.E.; Haines, J.; O’Brien, A.; McDonald, J.; Price, S.; Sherry, B.; Taveras, E.M. Systematic review of effective strategies for reducing screen time among young children. Obesity 2012, 20, 1338–1354. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Sun, S.; He, Y.; Jiang, B. The effect of interventions targeting screen time reduction: A systematic review and meta-analysis. Medicine 2016, 95, e4029. [Google Scholar] [CrossRef] [PubMed]
- Japan Pediatric Society. Recommendations for “Children and Media” Issues. 2004. Available online: https://www.jpa-web.org/about/organization_chart/cm_committee.html (accessed on 10 July 2023).
- Robinson, T.N.; Banda, J.A.; Hale, L.; Lu, A.S.; Fleming-Milici, F.; Calvert, S.L.; Wartella, E. Screen Media Exposure and Obesity in Children and Adolescents. Pediatrics 2017, 140, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Hisler, G.C.; Hasler, B.P.; Franzen, P.L.; Clark, D.B.; Twenge, J.M. Screen media use and sleep disturbance symptom severity in children. Sleep. Health 2020, 6, 731–742. [Google Scholar] [CrossRef]
- Song, Y.; Li, L.; Xu, Y.; Pan, G.; Tao, F.; Ren, L. Associations between screen time, negative life events, and emotional and behavioral problems among Chinese children and adolescents. J. Affect. Disord. 2020, 264, 506–512. [Google Scholar] [CrossRef] [PubMed]
- French, A.N.; Ashby, R.S.; Morgan, I.G.; Rose, K.A. Time outdoors and the prevention of myopia. Exp. Eye Res. 2013, 114, 58–68. [Google Scholar] [CrossRef]
- Sharif, I.; Sargent, J.D. Association between television, movie, and video game exposure and school performance. Pediatrics 2006, 118, e1061–e1070. [Google Scholar] [CrossRef]
- Novaković, S.; Milenković, S.; Srećković, M.; Backović, D.; Ignjatović, V.; Capo, N.; Stojanović, T.; Vukomanović, V.; Sekulić, M.; Gavrilović, J.; et al. Children’s Internet use and physical and psychosocial development. Front. Public Health 2023, 11, 1163458. [Google Scholar] [CrossRef]
- Cartanyà-Hueso, À.; Lidón-Moyano, C.; Martín-Sánchez, J.C.; González-Marrón, A.; Matilla-Santander, N.; Miró, Q.; Martínez-Sánchez, J.M. Association of screen time and sleep duration among Spanish 1–14 years old children. Paediatr. Perinat. Epidemiol. 2021, 35, 120–129. [Google Scholar] [CrossRef]
- Lissak, G. Adverse physiological and psychological effects of screen time on children and adolescents: Literature review and case study. Environ. Res. 2018, 164, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Parent, J.; Sanders, W.; Forehand, R. Youth Screen Time and Behavioral Health Problems: The Role of Sleep Duration and Disturbances. J. Dev. Behav. Pediatr. 2016, 37, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Magee, C.A.; Lee, J.K.; Vella, S.A. Bidirectional relationships between sleep duration and screen time in early childhood. JAMA Pediatr. 2014, 168, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.B.; Waring, M.E.; Pagoto, S.L.; Lemon, S.C. A television in the bedroom is associated with higher weekday screen time among youth with attention deficit hyperactivity disorder (ADD/ADHD). Prev. Med. Rep. 2015, 2, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Swing, E.L.; Gentile, D.A.; Anderson, C.A.; Walsh, D.A. Television and video game exposure and the development of attention problems. Pediatrics 2010, 126, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Tsuchiya, K.J.; Okumura, A.; Harada, T.; Iwabuchi, T.; Rahman, M.S.; Kuwabara, H.; Nomura, Y.; Nishimura, T. The association between screen time and genetic risks for neurodevelopmental disorders in children. Psychiatry Res. 2023, 327, 115395. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Wang, F.; Angriman, M.; Masi, G.; Bruni, O. Sleep Disorders in Children and Adolescents with Autism Spectrum Disorder: Diagnosis, Epidemiology, and Management. CNS Drugs 2020, 34, 415–423. [Google Scholar] [CrossRef]
- Ahlberg, R.; Garcia-Argibay, M.; Taylor, M.; Lichtenstein, P.; D’Onofrio, B.M.; Butwicka, A.; Hill, C.; Cortese, S.; Larsson, H.; Du Rietz, E. Prevalence of sleep disorder diagnoses and sleep medication prescriptions in individuals with ADHD across the lifespan: A Swedish nationwide register-based study. BMJ Ment. Health 2023, 26, e300809. [Google Scholar] [CrossRef]
- Wu, X.; Tao, S.; Rutayisire, E.; Chen, Y.; Huang, K.; Tao, F. The relationship between screen time, nighttime sleep duration, and behavioural problems in preschool children in China. Eur. Child. Adolesc. Psychiatry 2017, 26, 541–548. [Google Scholar] [CrossRef]
- Kim, K.W.; Koh, Y.K.; Kim, J.H. Associations between Parental Factors and Children’s Screen Time During the COVID-19 Pandemic in South Korea. Child. Psychiatry Hum. Dev. 2022, 54, 1749–1758. [Google Scholar] [CrossRef]
- Leonard, H.; Khurana, A. Parenting Behaviors and Family Conflict as Predictors of Adolescent Sleep and Bedtime Media Use. J. Youth Adolesc. 2022, 51, 1611–1621. [Google Scholar] [CrossRef] [PubMed]
- Jago, R.; Wood, L.; Zahra, J.; Thompson, J.L.; Sebire, S.J. Parental control, nurturance, self-efficacy, and screen viewing among 5- to 6-year-old children: A cross-sectional mediation analysis to inform potential behavior change strategies. Child. Obes. 2015, 11, 139–147. [Google Scholar] [CrossRef]
- Komada, Y.; Adachi, N.; Matsuura, N.; Mizuno, K.; Hirose, K.; Aritomi, R.; Shirakawa, S. Irregular sleep habits of parents are associated with increased sleep problems and daytime sleepiness of children. Tohoku J. Exp. Med. 2009, 219, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Matsuishi, T.; Nagano, M.; Araki, Y.; Tanaka, Y.; Iwasaki, M.; Yamashita, Y.; Nagamitsu, S.; Iizuka, C.; Ohya, T.; Shibuya, K.; et al. Scale properties of the Japanese version of the Strengths and Difficulties Questionnaire (SDQ): A study of infant and school children in community samples. Brain Dev. 2008, 30, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Cabinet Office, Government of Japan. White Paper on Children and Youth. 2015. Available online: https://www8.cao.go.jp/youth/whitepaper/h27honpen/b1_06_01.html (accessed on 10 July 2023).
- NHK Broadcasting Culture Research Institute. National Living Time Survey. 2020. Available online: https://www.nhk.or.jp/bunken/yoron-jikan/column/sleep-2020.html (accessed on 10 July 2023).
- Pan, W.; Jiang, L.; Geng, M.L.; Ding, P.; Wu, X.Y.; Tao, F.B. Correlation between screen-watching time and emotional problems as well as combination effect of outdoor time among preschool children. Zhonghua Liu Xing Bing. Xue Za Zhi 2019, 40, 1569–1572. [Google Scholar] [PubMed]
- Thomas, M.M.; Gugusheff, J.; Baldwin, H.J.; Gale, J.; Boylan, S.; Mihrshahi, S. Healthy Lifestyle Behaviours Are Associated with Children’s Psychological Health: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 1, 7509. [Google Scholar] [CrossRef] [PubMed]
- Niiranen, J.; Kiviruusu, O.; Vornanen, R.; Saarenpää-Heikkilä, O.; Paavonen, E.J. High-dose electronic media use in five-year-olds and its association with their psychosocial symptoms: A cohort study. BMJ Open 2021, 11, e040848. [Google Scholar] [CrossRef]
- Khan, A.; Uddin, R.; Burton, N.W. Insufficient physical activity in combination with high screen time is associated with adolescents’ psychosocial difficulties. Int. Health 2018, 10, 246–251. [Google Scholar] [CrossRef]
- Hale, L.; Guan, S. Screen time and sleep among school-aged children and adolescents: A systematic literature review. Sleep. Med. Rev. 2015, 21, 50–58. [Google Scholar] [CrossRef]
- Christensen, M.A.; Bettencourt, L.; Kaye, L.; Moturu, S.T.; Nguyen, K.T.; Olgin, J.E.; Pletcher, M.J.; Marcus, G.M. Direct Measurements of Smartphone Screen-Time: Relationships with Demographics and Sleep. PLoS ONE 2016, 11, e0165331. [Google Scholar] [CrossRef]
- Guerrero, M.D.; Barnes, J.D.; Chaput, J.P.; Tremblay, M.S. Screen time and problem behaviors in children: Exploring the mediating role of sleep duration. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 105. [Google Scholar] [CrossRef] [PubMed]
- Tambalis, K.D.; Panagiotakos, D.B.; Psarra, G.; Sidossis, L.S. Insufficient Sleep Duration Is Associated with Dietary Habits, Screen Time, and Obesity in Children. J. Clin. Sleep. Med. 2018, 14, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Kahn, M.; Schnabel, O.; Gradisar, M.; Rozen, G.S.; Slone, M.; Atzaba-Poria, N.; Tikotzky, L.; Sadeh, A. Sleep, screen time and behaviour problems in preschool children: An actigraphy study. Eur. Child. Adolesc. Psychiatry 2021, 30, 1793–1802. [Google Scholar] [CrossRef] [PubMed]
- Falbe, J.; Davison, K.K.; Franckle, R.L.; Ganter, C.; Gortmaker, S.L.; Smith, L.; Land, T.; Taveras, E.M. Sleep duration, restfulness, and screens in the sleep environment. Pediatrics 2015, 135, e367–e375. [Google Scholar] [CrossRef] [PubMed]
- Musa, S.; Elyamani, R.; Dergaa, I. COVID-19 and screen-based sedentary behaviour: Systematic review of digital screen time and metabolic syndrome in adolescents. PLoS ONE 2022, 17, e0265560. [Google Scholar] [CrossRef] [PubMed]
- Ishtiaq, A.; Ashraf, H.; Iftikhar, S.; Baig-Ansari, N. Parental perception on screen time and psychological distress among young children. J. Family Med. Prim. Care 2021, 10, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, Y.; Kaneita, Y.; Jike, M.; Osaki, Y. Clarifying the factors affecting the implementation of the “early to bed, early to rise, and don’t forget your breakfast” campaign aimed at adolescents in Japan. Sleep. Biol. Rhythms 2021, 19, 325–336. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Spearman’s Rho | p | 95% CI | |
|---|---|---|---|---|
| Lower | Upper | |||
| Children’s difficulty–Children’s sleep duration | 0.114 | 0.088 | −0.021 | 0.245 |
| Children’s difficulty–Parental control | −0.061 | 0.365 | −0.194 | 0.075 |
| Children’s sleep duration–Parental control | 0.086 | 0.2 | −0.049 | 0.218 |
| N = 225 | |
| Background | Mean (SD or %) |
| School year | 6.16 (2.52) |
| Sex male | 110 (48.9%) |
| Siblings | 2.08 (0.76) |
| Age (primary caregiver) | 44.0 (6.13) |
| Sex male (primary caregiver) | 26 (11.6%) |
| Screen time | Mean (SD) |
| All students (N = 225) | 133.60 (67.7) |
| School year 1–3 (N = 39) | 120.00 (57.6) |
| School year 4–6 (N = 56) | 131.25 (63.9) |
| School year 7–9 (N = 130) | 138.69 (71.9) |
| Bedtime/wake-up time | Mean (SD) |
| All students (N = 225) | 22:03 (56 min)/6:29 (31 min) |
| School year 1–3 (N = 39) | 21:08 (40 min)/6:20 (25 min) |
| School year 4–6 (N = 56) | 21:42 (31 min)/6:32 (22 min) |
| School year 7–9 (N = 130) | 22:30 (53 min)/6:32 (36 min) |
| Primary caregiver (N = 225) | 22:49 (65 min)/5:43 (55 min) |
| SDQ | Mean (SD) |
| Total difficulties score | 9.71 (5.21) |
| Conduct problem | 1.58 (2.03) |
| Hyperactivity/inattention | 2.97 (2.09) |
| Emotional symptoms | 2.48 (2.35) |
| Peer problems | 1.98 (1.74) |
| Prosocial behavior | 6.56 (2.04) |
| Variables | B | β | t | p | 95% CI for B |
|---|---|---|---|---|---|
| Constant | 144.588 | 10.671 | <0.001 | 117.886 to 171.291 | |
| Children’s Sleep Duration | −19.908 | −0.281 | −4.528 | <0.001 | −28.573 to −11.243 |
| Children’s Difficulty | 2.159 | 0.166 | 2.680 | 0.008 | 0.572 to 3.747 |
| Parental Control | −18.775 | −0.204 | −3.281 | 0.001 | −30.053 to 3.747 |
| Product of Coefficients | Bootstrapping Bias-Correlated 95% CI | |||||
|---|---|---|---|---|---|---|
| Relationship | B | β | SE | z | p | Lower to Upper |
| Parental Bedtime →Children’s sleep duration →Children’s screen time | 5.926 | 0.095 | 1.982 | 2.988 | 0.001 | 2.744 to 10.833 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arai, Y.; Sasayama, D.; Suzuki, K.; Nakamura, T.; Kuraishi, Y.; Washizuka, S. Association between Children’s Difficulties, Parent-Child Sleep, Parental Control, and Children’s Screen Time: A Cross-Sectional Study in Japan. Pediatr. Rep. 2023, 15, 668-678. https://doi.org/10.3390/pediatric15040060
Arai Y, Sasayama D, Suzuki K, Nakamura T, Kuraishi Y, Washizuka S. Association between Children’s Difficulties, Parent-Child Sleep, Parental Control, and Children’s Screen Time: A Cross-Sectional Study in Japan. Pediatric Reports. 2023; 15(4):668-678. https://doi.org/10.3390/pediatric15040060
Chicago/Turabian StyleArai, Yusuke, Daimei Sasayama, Kazuhiro Suzuki, Toshinori Nakamura, Yuta Kuraishi, and Shinsuke Washizuka. 2023. "Association between Children’s Difficulties, Parent-Child Sleep, Parental Control, and Children’s Screen Time: A Cross-Sectional Study in Japan" Pediatric Reports 15, no. 4: 668-678. https://doi.org/10.3390/pediatric15040060