
Early Outcome of Multisystem Inflammatory Syndrome in Neonates Diagnosed following Prenatal Maternal COVID-19 Infection: A Three-Case Series
 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
- -
- Negative RT-PCR-SARS-CoV-2 test in infants;
- -
- Negative IgM-SARS-CoV-2 antibodies in infants;
- -
- Positive IgG-SARS-CoV-2 antibodies in infants;
- -
- Maternal COVID-19 infection diagnosed in the third trimester of pregnancy.
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CK-MB | creatine phosphokinase myocardial band |
| COVID-19 | coronavirus disease 2019 |
| CRP | C reactive protein |
| ER | emergency room |
| ESR | erythrocyte sedimentation rate |
| Ig G | immunoglobulin G |
| Ig M | immunoglobulin M |
| MIS | multisystem inflammatory syndrome |
| MIS-C | multisystem inflammatory syndrome in children |
| MIS-N | multisystem Inflammatory syndrome in neonates |
| NT-pro-BNP | N-terminal pro b-type natriuretic peptide |
| RT-PCR | reverse transcription polymerase chain reaction |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
References
- Molloy, E.J.; Nakra, N.; Gale, C.; Dimitriades, V.R.; Lakshminrusimha, S. Multisystem inflammatory syndrome in children (MIS-C) and neonates (MIS-N) associated with COVID-19: Optimizing definition and management. Pediatr. Res. 2022, 93, 1499–1508. [Google Scholar] [CrossRef]
- Słomka, A.; Kowalewski, M.; Żekanowska, E. Coronavirus Disease 2019 (COVID–19): A Short Review on Hematological Manifestations. Pathogens 2020, 9, 493. [Google Scholar] [CrossRef]
- Zhu, F.; Zozaya, C.; Zhou, Q.; De Castro, C.; Shah, P.S. SARS-CoV-2 genome and antibodies in breastmilk: A systematic review and meta-analysis. Arch. Dis. Child. Fetal. Neonatal. Ed. 2021, 106, 514–521. [Google Scholar] [CrossRef]
- Pawar, R.; Gavade, V.; Patil, N.; Mali, V.; Girwalkar, A.; Tarkasband, V.; Loya, S.; Chavan, A.; Nanivadekar, N.; Shinde, R.; et al. Neonatal multisystem inflammatory syndrome (MIS-N) associated with prenatal maternal SARS-CoV-2: A case series. Children 2021, 8, 572. [Google Scholar] [CrossRef]
- Matyas, M.; Valeanu, M.; Hasmasanu, M.; Voina, B.; Tutu, A.; Zaharie, G.C. The Effect of Maternal SARS-CoV-2 Infection on Neonatal Outcome. Children 2023, 10, 771. [Google Scholar] [CrossRef]
- Saha, S.; Pal, P.; Mukherjee, D. Neonatal MIS-C: Managing the cytokine storm. Pediatrics 2021, 148, e2020042093. [Google Scholar] [CrossRef] [PubMed]
- Divekar, A.A.; Patamasucon, P.; Benjamin, J.S. Presumptive neonatal multisystem inflammatory syndrome in children associated with Coronavirus disease 2019. Am. J. Perinatol. 2021, 38, 632–636. [Google Scholar] [CrossRef] [PubMed]
- Shaiba, L.A.; Hadid, A.; Altirkawi, K.A.; Bakheet, H.M.; Alherz, A.M.; Hussain, S.A.; Sobaih, B.H.; Alnemri, A.M.; Almaghrabi, R.; Ahmed, M.; et al. Case Report: Neonatal multi-System inflammatory syndrome associated with SARS-CoV-2 exposure in two cases from Saudi Arabia. Front. Pediatr. 2021, 9, 652857. [Google Scholar] [CrossRef] [PubMed]
- Amonkar, P.S.; Gavhane, J.B.; Kharche, S.N.; Kadam, S.S.; Bhusare, D.B. Aortic thrombosis in a neonate with COVID-19-related fetal inflammatory response syndrome requiring amputation of the leg: A case report. Paediatr. Int. Child. Health 2021, 41, 211–216. [Google Scholar] [CrossRef]
- Kappanayil, M.; Balan, S.; Alawani, S.; Mohanty, S.; Leeladharan, S.P.; Gangadharan, S.; Jayashankar, J.P.; Jagadeesan, S.; Kumar, A.; Gupta, A.; et al. Multisystem inflammatory syndrome in a neonate, temporally associated with prenatal exposure to SARS-CoV-2: A case report. Lancet Child. Adolesc. Health 2021, 5, 304–308. [Google Scholar] [CrossRef]
- Lima, A.R.; Cardoso, C.C.; Bentim, P.R.; Voloch, C.M.; Rossi, Á.D.; da Costa, R.M.M.; da Paz, J.A.S.; Agostinho, R.F.; Figueiredo, V.R.; Júnior, J.S.; et al. Maternal SARS-CoV-2 infection associated to systemic inflammatory response and pericardial effusion in the Newborn: A case report. J. Pediatric. Infect. Dis. Soc. 2021, 10, 536–539. [Google Scholar] [CrossRef]
- Gupta, P.; Tamatam, P.R.; Dhulipudi, B.; Vardhelli, V.; Deshabhotla, S.; Oleti, T.P. Neonatal multisystem inflammatory syndrome (MIS-N) associated with maternal SARS-CoV-2 exposure. Indian J. Pediatr. 2022, 89, 827–828. [Google Scholar] [CrossRef]
- More, K.; Aiyer, S.; Goti, A.; Parikh, M.; Sheikh, S.; Patel, G.; Kallem, V.; Soni, R.; Kumar, P. Multisystem inflammatory syndrome in neonates (MIS-N) associated with SARS-CoV2 infection: A case series. Eur. J. Pediatr. 2022, 181, 1883–1898. [Google Scholar] [CrossRef]
- Chakravarty, S.; Gupta, V.; Gupta, A.; Nishu Sain, K.; Valjiyani, S. Neonatal Multisystem Inflammatory Syndrome (MIS-N). J. Biomed. Res. Environ. Sci. 2022, 3, 174–176. [Google Scholar]
- Shinde, M.D.; Khamkar, A.M.; Pote, P.D.; Suryawanshi, P.B. Fetal inflammatory response syndrome associated with SARS-CoV-2 exposure in utero. Pediatr. Oncall J. 2021, 19. [Google Scholar] [CrossRef]
- Amulya, G.A.-O.; Kaur, A.; Sharma, M. Multisystem Inflammatory Syndrome in a neonate with prenatal exposure to COVID-19. Indian J. Pediatr. 2022, 89, 314. [Google Scholar] [CrossRef]
- Nitya, U.S.; Devassy, B.M.; Joseph, S.; Anila, A.P.; George, R.; Sreenivasan, V.K. Intrauterine onset of multisystem inflammatory syndrome in a neonate temporally associated with maternal COVID-19. Indian J. Rheumatol. 2022, 17, 289–293. [Google Scholar]
- Harish, J.; Tambekar Satish, D.; Ashtekar Shishir, P. Mirgunde, Swati Khot, Shrikant Mane, Neonatal multisystem inflammatory syndrome associated with prenatal maternal SARS-CoV-2 exposure: A case series. Medip Acad. Int. J. Contemp. Pediatr. 2022, 9, 381–386. [Google Scholar]
- Sojisirikul, N.; Lapphra, K.; Ngerncham, S.; Charuvanij, S.; Durongpisitkul, K.; Curlin, M.E.; Chokephaibulkit, K. Neonatal Multisystem Inflammatory Syndrome (MIS-N): The first case report in Thailand. COVID 2022, 2, 1265–1269. [Google Scholar] [CrossRef]
- Kaushik, A.; Gupta, S.; Sood, M.; Sharma, S.; Verma, S. A systematic review of multisystem inflammatory syndrome in children associated with SARS-Cov-2 infection. Pediatr. Infect. Dis. J. 2020, 39, e340–e346. [Google Scholar] [CrossRef] [PubMed]
- Chinniah, K.; Bhimma, R.; Naidoo, K.L.; Archary, M.; Jeena, P.; Hoosen, E.; Singh, S.; Lawler, M.; Naby, F.; Masekela, R. Multisystem inflammatory syndrome in children associated with SARS-CoV-2 infection in Kwazulu-Natal, South Africa. Pediatr. Infect. Dis. J. 2023, 42, e9–e14. [Google Scholar] [CrossRef] [PubMed]
- Mohsin, S.S.; Abbas, Q.; Chowdhary, D.; Khalid, F.; Sheikh, A.S.; Ali Khan, Z.G.; Aslam, N.; Bhatti, O.A.; Inam, M.; Saleem, A.F.; et al. Multisystem inflammatory syndrome (MIS-C) in Pakistani children: A description of the phenotypes and comparison with historical cohorts of children with Kawasaki disease and myocarditis. PLoS ONE 2021, 16, e0253625. [Google Scholar] [CrossRef]
- Nayak, S.; Panda, P.C.; Biswal, B.; Agarwalla, S.K.; Satapathy, A.K.; Jena, P.K.; Gulla, K.M.; Rath, D.; Mahapatra, A.; Mishra, P.; et al. Eastern India collaboration on Multisystem inflammatory syndrome in children (EICOMISC): A multicenter observational study of 134 cases. Front. Pediatr. 2022, 10, 834039. [Google Scholar] [CrossRef] [PubMed]
- Wróblewska-Seniuk, K.; Basiukajć, A.; Wojciechowska, D.; Telge, M.; Miechowicz, I.; Mazela, J. Clinical Characteristics of Newborns Born to Mothers with COVID-19. J. Clin. Med. 2021, 10, 4383. [Google Scholar] [CrossRef]
- Moza, A.; Duica, F.; Antoniadis, P.; Bernad, E.S.; Lungeanu, D.; Craina, M.; Bernad, B.C.; Paul, C.; Muresan, C.; Nitu, R.; et al. Outcome of Newborns with Confirmed or Possible SARS-CoV-2 Vertical Infection—A Scoping Review. Diagnostics 2023, 13, 245. [Google Scholar] [CrossRef]
- Pawłowska, M.; Pokorska-Śpiewak, M.; Talarek, E.; Mania, A.; Hasiec, B.; Żwirek-Pytka, E.; Stankiewicz, M.; Stani, M.; Frańczak-Chmura, P.; Szenborn, L.; et al. Clinical Course and Severity of COVID-19 in 940 Infants with and without Comorbidities Hospitalized in 2020 and 2021: The Results of the National Multicenter Database SARSTer-PED. J. Clin. Med. 2023, 12, 2479. [Google Scholar] [CrossRef]
- McCarthy, J.; Liu, D.; Kaskel, F. The Need for Life-Course Study of Children Born to Mothers with Prior COVID-19 Infection. JAMA Pediatr. 2021, 175, 1097–1098. [Google Scholar] [CrossRef]
- Edlow, A.G.; Castro, V.M.; Shook, L.L.; Kaimal, A.J.; Perlis, R.H. Neurodevelopmental outcomes at 1 year in infants of mothers who tested positive for SARS-CoV-2 during pregnancy. JAMA Netw. Open 2002, 5, e2215787. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Case Number | 1 | 2 | 3 |
|---|---|---|---|
| Admission | April 2022 | June 2021 | December 2021 |
| Age at admission (days) | 5 | 25 | 25 |
| Birth | natural | natural | C-section |
| Gestational age (weeks) | 39 | 39 | 39 |
| Birth weight (g) | 3400 | 3100 | 3620 |
| APGAR score | 9 | 9 | 10 |
| Maternal COVID-19 infection disease severity | mild | mild | Severe (fatal) |
| Feeding | breastfeeding | mixed feeding | formula |
| Symptoms onset before admission (days) | 1 | 7 | 4 |
| Signs and symptoms | |||
| Fever | <3 days | <3 days | <3 days |
| other | Drowsiness, apathy | bloody diarrheic stools | Cough, rhinorrhea, mild respiratory distress |
| Inflammation biomarkers | |||
| CRP (mg/dL) | 0.48 | 0.26 | 2.1 |
| ESR (mm/h) | - | - | 50 |
| Fibrinogen (mg/dL) | 590 | 506 | - |
| Ferritin (µg/L) | 460 | 246 | 174.5 |
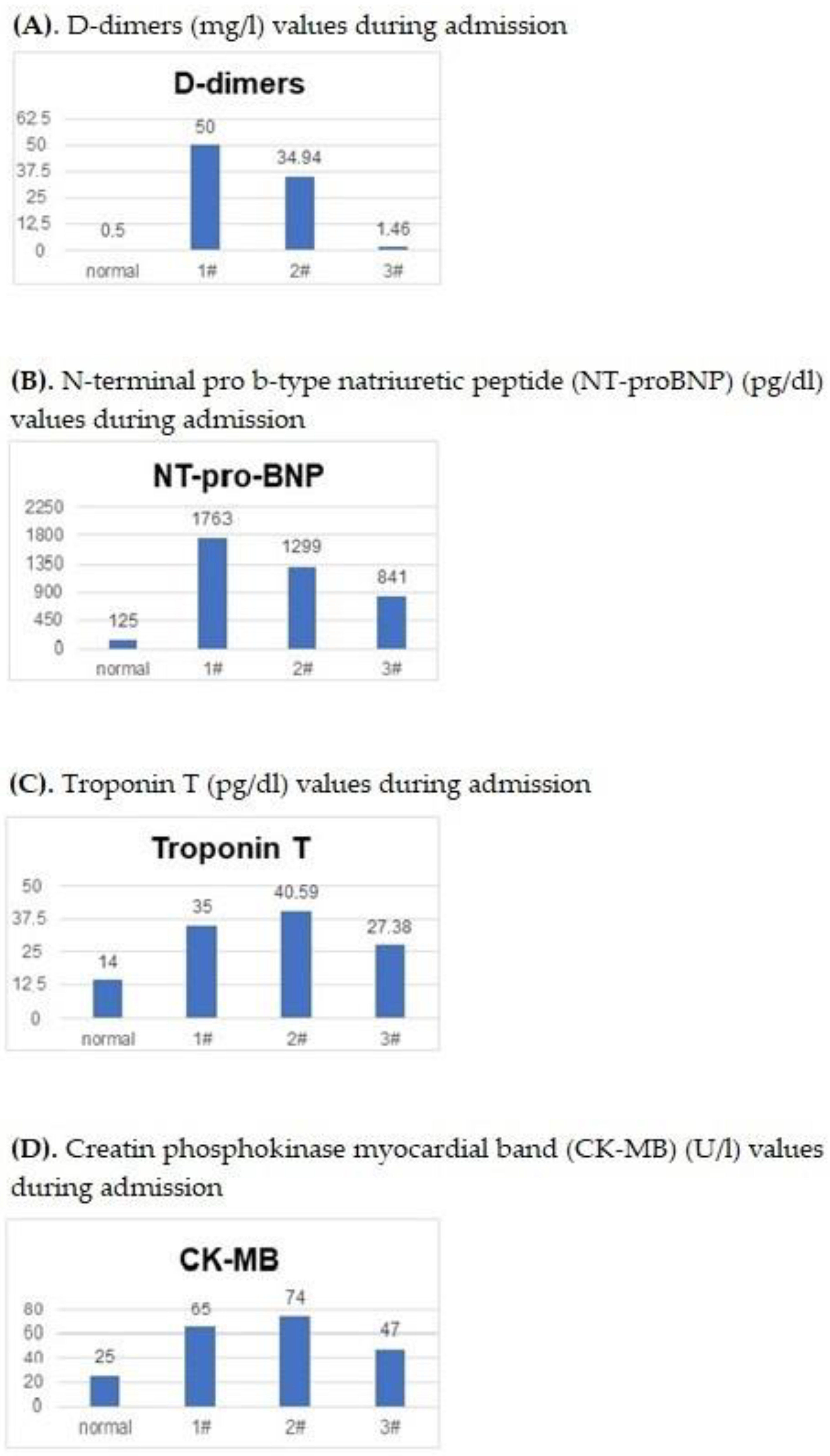
| D-dimers (mg/L) | 50 | 34.94 | 1.46 |
| Myocardial biomarkers | |||
| NT-pro-BNP (pg/dL) | 1763 | 1299 | 841 |
| Troponin T (pg/dL) | 35 | 40.59 | 27.38 |
| CK-MB (U/L) | 65 | 74 | 47 |
| Cultures | |||
| Blood | negative | negative | negative |
| Urine | negative | negative | negative |
| Stool | negative | negative | negative |
| Nasal swab | negative | not performed | negative |
| Throat swab | negative | not performed | negative |
| Ultrasound | |||
| Abdominal | normal | normal | hydronephrosis |
| Echocardiography | patent foramen ovale | atrial septal defect | - |
| Transfontanellar ultrasound | normal | normal | normal |
| Treatment | |||
| Intravenous Immunoglobulins | yes | no | no |
| Antibiotics | ampicillin | ampicillin | ampicillin + gentamicin |
| Corticosteroids | methylprednisolone; hydrocortisone hemi succinate | no | no |
| Hospitalization days | 14 | 7 | 7 |
| Follow-up | |||
| D-dimers (mg/L) | 50 | 0.71 | not done |
| NT-pro-BNP (pg/dL) | 322 | 352 | not done |
| Troponin T (pg/dL) | 35 | 37.25 | not done |
| CK-MB(U/L) | 49 | not done | not done |
| CRP (mg/dL) | 0.4 | 0.45 | not done |
| Ferritin (mg/dL) | Not performed | 162 | not done |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terciu, M.; Luca, I.; Panait, E.; Leibovitz, E.; Mitrica, M.; Popovici, B.; Ilea, A.; Falup-Pecurariu, O.G. Early Outcome of Multisystem Inflammatory Syndrome in Neonates Diagnosed following Prenatal Maternal COVID-19 Infection: A Three-Case Series. Pediatr. Rep. 2023, 15, 591-598. https://doi.org/10.3390/pediatric15040054
Terciu M, Luca I, Panait E, Leibovitz E, Mitrica M, Popovici B, Ilea A, Falup-Pecurariu OG. Early Outcome of Multisystem Inflammatory Syndrome in Neonates Diagnosed following Prenatal Maternal COVID-19 Infection: A Three-Case Series. Pediatric Reports. 2023; 15(4):591-598. https://doi.org/10.3390/pediatric15040054
Chicago/Turabian StyleTerciu, Maria, Ioana Luca, Emilia Panait, Eugene Leibovitz, Maria Mitrica, Bianca Popovici, Anca Ilea, and Oana Gabriela Falup-Pecurariu. 2023. "Early Outcome of Multisystem Inflammatory Syndrome in Neonates Diagnosed following Prenatal Maternal COVID-19 Infection: A Three-Case Series" Pediatric Reports 15, no. 4: 591-598. https://doi.org/10.3390/pediatric15040054