
SARS-CoV-2-Associated Multisystem Inflammatory Syndrome in Children (MIS-C): A Case Report from Iraq
Abstract
:1. Introduction
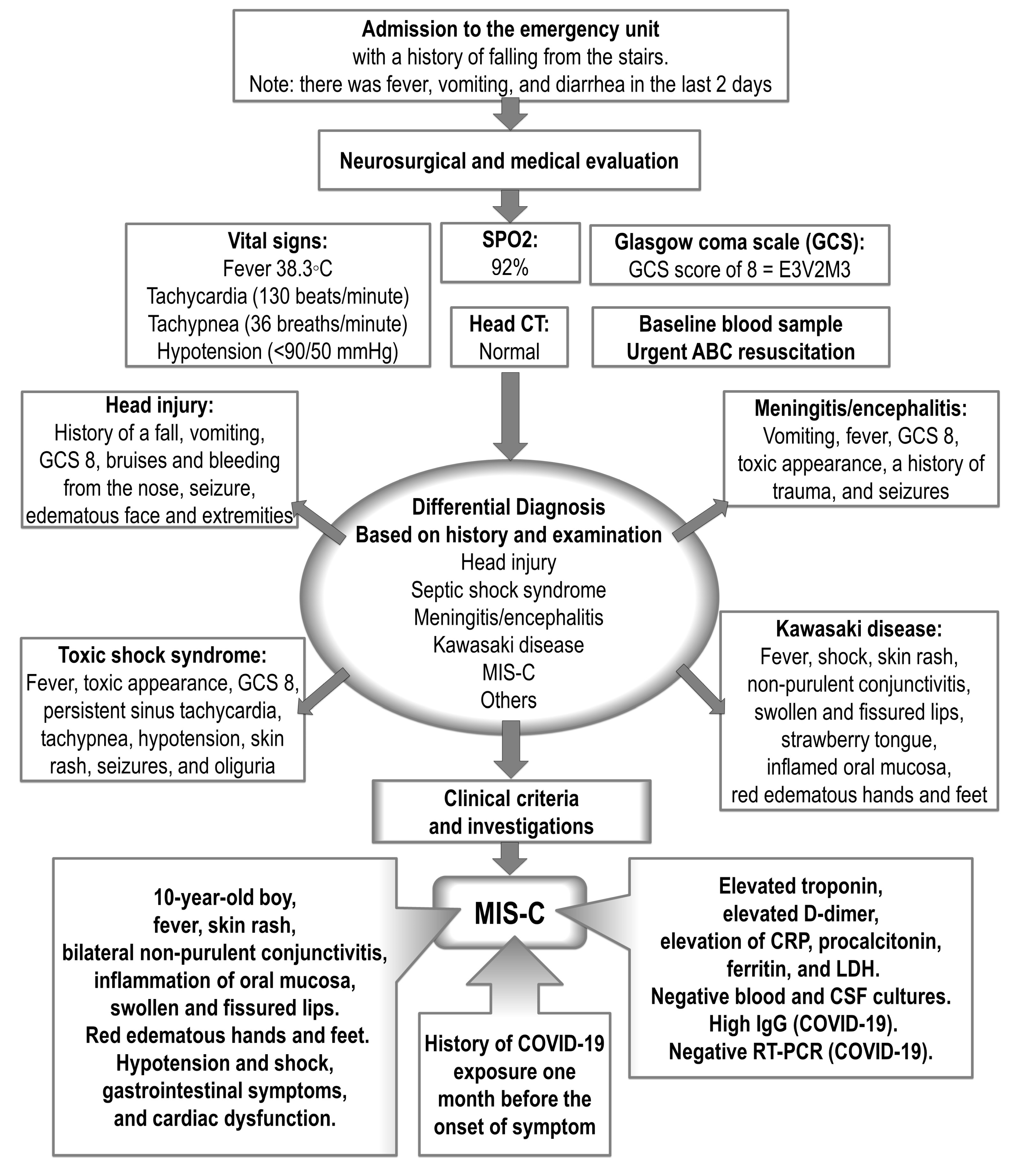
2. Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rana, R.; Tripathi, A.; Kumar, N.; Ganguly, N.K. A Comprehensive Overview on COVID-19: Future Perspectives. Front. Cell. Infect. Microbiol. 2021, 11, 744903. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.D.; Yousaf, A.R.; Bornstein, E.; Wu, M.J.; Lindsey, K.; Melgar, M.; E Oster, M.; Zambrano, L.D.; Campbell, A.P. Multisystem Inflammatory Syndrome in Children During Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Delta and Omicron Variant Circulation-United States, July 2021–January 2022. Clin. Infect. Dis. 2022, 75 (Suppl. S2), S303–S307. [Google Scholar] [CrossRef]
- Dufort, E.M.; Koumans, E.H.; Chow, E.; Rosenthal, E.M.; Muse, A.; Rowlands, J.; Barranco, M.A.; Maxted, A.M.; Rosenberg, E.S.; Easton, D.; et al. New York State and Centers for Disease Control and Prevention Multisystem Inflammatory Syndrome in Children Investigation Team. Multisystem Inflammatory Syndrome in Children in New York State. N. Engl. J. Med. 2020, 383, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Dionne, A.; Son, M.B.F.; Randolph, A.G. An Update on Multisystem Inflammatory Syndrome in Children Related to SARS-CoV-2. Pediatr. Infect. Dis. J. 2022, 41, e6–e9. [Google Scholar] [CrossRef] [PubMed]
- Molloy, E.J.; Nakra, N.; Gale, C.; Dimitriades, V.R.; Lakshminrusimha, S. Multisystem inflammatory syndrome in children (MIS-C) and neonates (MIS-N) associated with COVID-19: Optimizing definition and management. Pediatr. Res. 2023, 93, 1499–1508. [Google Scholar] [CrossRef] [PubMed]
- Wessels, P.A.; Bingler, M.A. A comparison of Kawasaki Disease and multisystem inflammatory syndrome in children. Prog. Pediatr. Cardiol. 2022, 65, 101516. [Google Scholar] [CrossRef] [PubMed]
- Council of State and Territorial Epidemiologists/CDC Surveillance Case Definition for Multisystem Inflammatory Syndrome in Children Associated with SARS-CoV-2 Infection—United States. Available online: https://stacks.cdc.gov/view/cdc/121710 (accessed on 11 July 2023).
- Lami, F.; Rashak, H.A.; Khaleel, H.A.; Mahdi, S.G.; Adnan, F.; Khader, Y.S.; A Alhilfi, R.; Lehlewa, A. Iraq experience in handling the COVID-19 pandemic: Implications of public health challenges and lessons learned for future epidemic preparedness planning. J. Public Health 2021, 43 (Suppl. S3), iii19–iii28. [Google Scholar] [CrossRef] [PubMed]
- Salih, A.F.; Hamasalih, K.; Rahman, H.S.; Mohammed, G.A. Pediatric COVID-19 infection in Sulaimaniyah Governorate, Iraq. Am. J. Otolaryngol. 2022, 43, 103199. [Google Scholar] [CrossRef] [PubMed]
- Ouldali, N.; Toubiana, J.; Antona, D.; Javouhey, E.; Madhi, F.; Lorrot, M.; Léger, P.-L.; Galeotti, C.; Claude, C.; Wiedemann, A.; et al. French COVID-19 Paediatric Inflammation Consortium. Association of Intravenous Immunoglobulins Plus Methylprednisolone vs Immunoglobulins Alone with Course of Fever in Multisystem Inflammatory Syndrome in Children. JAMA 2021, 325, 855–864. [Google Scholar] [CrossRef] [PubMed]
- Henderson, L.A.; Canna, S.W.; Friedman, K.G.; Gorelik, M.; Lapidus, S.K.; Bassiri, H.; Behrens, E.M.; Kernan, K.F.; Schulert, G.S.; Seo, P.; et al. American College of Rheumatology Clinical Guidance for Multisystem Inflammatory Syndrome in Children Associated With SARS-CoV-2 and Hyperinflammation in Pediatric COVID-19: Version 3. Arthritis Rheumatol. 2022, 74, e1–e20. [Google Scholar] [CrossRef] [PubMed]
- Piloya, T.; Nakiyingi, L.; Kimuli, I.; Kayima, J.; Lubega, J.; Sekabira, J.; Aanyu, H.T. SARS-CoV-2-Associated Multisystem Inflammatory Syndrome in a Child in Uganda: A Paediatric Experience in a Resource-Limited Setting. Case Rep. Infect. Dis. 2022, 2022, 7811891. [Google Scholar] [CrossRef] [PubMed]
- Sharp, N.; Tieves, K. Pediatric Head Trauma. J. Pediatr. Intensive Care 2015, 4, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Feldstein, L.R.; Tenforde, M.W.; Friedman, K.G.; Newhams, M.; Rose, E.B.; Dapul, H.; Soma, V.L.; Maddux, A.B.; Mourani, P.M.; Bowens, C.; et al. Overcoming COVID-19 Investigators. Characteristics and Outcomes of US Children and Adolescents with Multisystem Inflammatory Syndrome in Children (MIS-C) Compared with Severe Acute COVID-19. JAMA 2021, 325, 1074–1087. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, E.; Bamford, A.; Kenny, J.; Kaforou, M.; Jones, C.E.; Shah, P.; Ramnarayan, P.; Fraisse, A.; Miller, O.; Davies, P.; et al. PIMS-TS Study Group and EUCLIDS and PERFORM Consortia. Clinical Characteristics of 58 Children with a Pediatric Inflammatory Multisystem Syndrome Temporally Associated With SARS-CoV-2. JAMA 2020, 324, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Abrams, J.Y.; E Oster, M.; E Godfred-Cato, S.; Bryant, B.; Datta, S.D.; Campbell, A.P.; Leung, J.W.; A Tsang, C.; Pierce, T.J.; Kennedy, J.L.; et al. Factors linked to severe outcomes in multisystem inflammatory syndrome in children (MIS-C) in the USA: A retrospective surveillance study. Lancet Child Adolesc. Health 2021, 5, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Shi, D.S.; Whitaker, M.; Marks, K.J.; COVID-NET Surveillance Team. Hospitalizations of Children Aged 5-11 Years with Laboratory-Confirmed COVID-19—COVID-NET, 14 States, March 2020–February 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 574–581. [Google Scholar] [CrossRef] [PubMed]
- Iraq: WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/region/emro/country/iq (accessed on 12 August 2023).
- Lopez, A.; Patel, M.; Rayment, J.H.; Tam, H.; Roberts, A.; Laskin, S.; Tucker, L.; Biggs, C.M.; Ahmed, M.A.; Barakauskas, V.; et al. All hands on deck: A multidisciplinary approach to SARS-CoV-2-associated MIS-C. Paediatr. Child Health 2022, 27 (Suppl. S1), S53–S58. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Tests | Values | Reference Ranges | Notes | ||
|---|---|---|---|---|---|
| CBC | |||||
| Hb | 9.6 g/dL | Low | 11.5–15.5 g/dL | After 3 weeks, Hb returned to normal level | |
| Platelets | 15 × 109/L | Low | 177–381 × 109/L | After 3 weeks, platelets returned to normal level | |
| WBC | 2.4 × 109/L | Low | 4.5–13.5 × 109/L | On day 6, WBC returned to normal level | |
| Neutrophils | 67% | High | 54% | On day 4, started to improve | |
| Lymphocytes | 29% | Low | 38% | On day 4, started to improve | |
| LFT | After 3 weeks, LFT returned to normal level | ||||
| ALT | 212 U/L | High | 7–55 U/L | ||
| AST | 387 U/L | High | 8–48 U/L | ||
| LDH | 462 U/L | High | 122–222 U/L | ||
| GGT | 166 IU/L | High | 8–61 U/L | ||
| ALP | 212 U/L | High | 40–129 U/L | ||
| Albumin | 3.5 g/dL | 3.5–5 g/dL | |||
| Bilirubin (total) | 0.84 mg/dL | 0.1–1.2 mg/dL | |||
| RFT | After 3 weeks, RFT returned to normal level | ||||
| Creatinine | 1.4 mg/dL | High | 0.6–1.3 mg/dL | ||
| BUN | 50 mg/dL | High | 7–18 mg/dL | ||
| Others | |||||
| CRP | 18.3 mg/L | High | 8–10 mg/L | After 3 weeks, returned to normal level | |
| D-dimer | 5120 ng/mL * | High | <500 ng/mL | Reached the peak at day 8, then after 4 weeks returned to normal level | |
| S. ferritin | 400 ng/mL | High | 7–140 ng/mL | ||
| Troponin T | 0.44 ng/ml | High | <0.1 ng/ml | ||
| Procalcitonin | 88.3 ng/mL | High | 0.1 ng/mL | ||
| SARS-CoV-2 IgG | High | High | Negative | ||
| RT-PCR COVID-19 | Negative | Negative | |||
| Variable | CDC Defined MIS-C * | WHO Defined MIS-C ** | Our Patient (Fulfilled CDC and WHO Criteria) | |
|---|---|---|---|---|
| 1 | Age (years) | <21 | (0–19) | 10 |
| 2 | Fever | 38.0 °C or more, or a subjective fever | For 3 days or more | Fever > 38 °C for 3 days |
| 3 | Multisystem involvement (at least 2 of the following): | |||
| Shock | Hypotension or shock | Shock | |
| Erythema or edema of hands or feet, oral mucositis, drying or fissuring of the lips, strawberry tongue, conjunctivitis, or other rash | Rash or bilateral non-purulent conjunctivitis or mucocutaneous inflammation (mouth, hands, or feet) | Rash, bilateral non-purulent conjunctivitis, drying and fissuring of the lips, strawberry tongue, and red edematous hands and feet | |
| Increased troponin or left ventricular ejection fraction < 55% or coronary artery dilation, aneurysm, or ectasia | Myocardial dysfunction, pericarditis, valvulitis, or coronary abnormalities (ECG changes or elevated troponin/BNP) | Increased troponin level and ECG changes | |
| Platelets < 150,000/μL or absolute lymphocyte count < 1000/μL | Evidence of coagulopathy (increasing D-dimer and prolonged PT or PTT) | Increasing D-dimer, platelets < 150,000/μL, and absolute lymphocyte count < 1000/μL | |
| Vomiting or abdominal pain, or diarrhea | Vomiting, diarrhea, or abdominal pain | Vomiting and diarrhea, | |
| 4 | Laboratory data (evidence of systemic inflammation) | CRP 3 mg/dL or more | E.g., elevated ESR, CRP, or procalcitonin | Elevated CRP, procalcitonin, ferritin, LDH, and neutrophils |
| 5 | SARS-CoV-2 infection (any of the mentioned points) | i. Confirmation by: | Evidence through: | There was evidence of: |
| -RT-PCR |
|
| Negative SARS-CoV-2 RT-PCR | |
| -Serology |
|
| Positive serology | |
| -Antigen test |
|
| Not conducted | |
| or | ||||
| -History of contact | ii. Evidence of exposure (close contact with a confirmed or probable COVID-19 case within 60 days before hospitalization) |
| Contact with a patient with COVID-19 | |
| 6 | Absence of | A more likely alternative diagnosis | Obvious microbial causes of inflammation, including bacterial sepsis and staphylococcal/streptococcal toxic shock syndromes | No alternative plausible diagnoses and no obvious microbial cause of inflammation, including bacterial sepsis and staphylococcal/streptococcal toxic shock syndromes, were detected |
| 7 | General health status | Critical and in need of emergency setting/or resulting in death | Critical and required emergency setting |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Simaani, R.B.Y.; Al-Kzayer, L.F.Y.; Ali, K.H.; Al-Ani, M.H.; Nakazawa, Y. SARS-CoV-2-Associated Multisystem Inflammatory Syndrome in Children (MIS-C): A Case Report from Iraq. Pediatr. Rep. 2023, 15, 532-540. https://doi.org/10.3390/pediatric15030048
Al-Simaani RBY, Al-Kzayer LFY, Ali KH, Al-Ani MH, Nakazawa Y. SARS-CoV-2-Associated Multisystem Inflammatory Syndrome in Children (MIS-C): A Case Report from Iraq. Pediatric Reports. 2023; 15(3):532-540. https://doi.org/10.3390/pediatric15030048
Chicago/Turabian StyleAl-Simaani, Ruwaid Behnam Y., Lika’a Fasih Y. Al-Kzayer, Kenan Hussien Ali, Mouroge H. Al-Ani, and Yozo Nakazawa. 2023. "SARS-CoV-2-Associated Multisystem Inflammatory Syndrome in Children (MIS-C): A Case Report from Iraq" Pediatric Reports 15, no. 3: 532-540. https://doi.org/10.3390/pediatric15030048