
Leclercia adecarboxylata in Peritoneal Dialysis Patients: A Systematic Review
 , ,
, ,
Abstract
:1. Introduction
2. Case Report
3. Subjects and Methods
3.1. General Information and Literature Search Strategy
3.2. Eligibility Criteria
3.3. Information Sources and Search Strategy
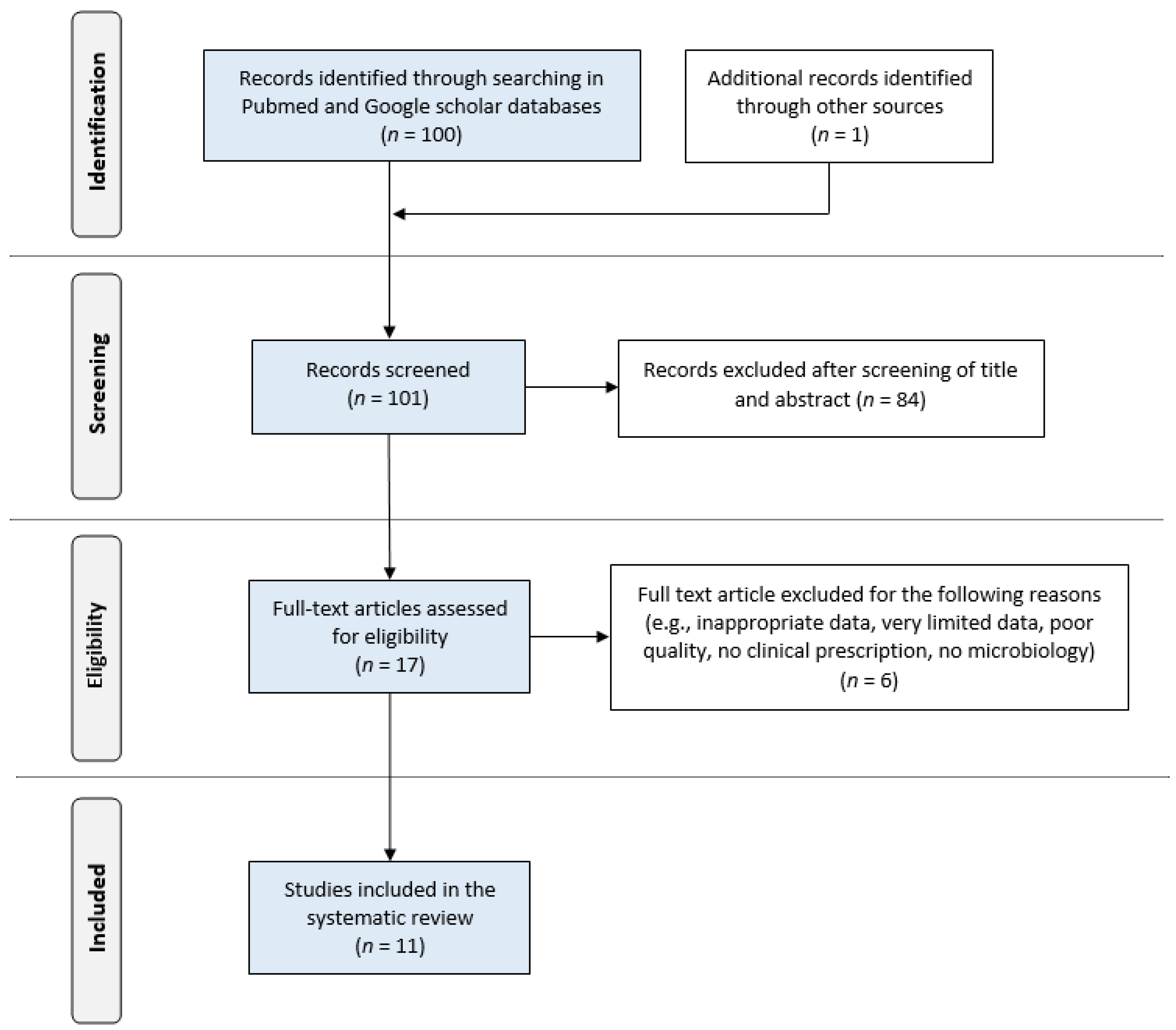
3.4. Study Selection
3.5. Data Extraction
3.6. Ethics Statement
3.7. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tamura, K.; Sakazaki, R.; Kosako, Y.; Yoshizaki, E. Leclercia adecarboxylata Gen. Nov., Comb. Nov., formerly known as Escherichia adecarboxylata. Curr. Microbiol. 1986, 13, 179–184. [Google Scholar] [CrossRef]
- Hess, B.; Burchett, A.; Huntington, M.K. Leclercia adecarboxylata in an immunocompetent patient. J. Med. Microbiol. 2008, 57, 896–898. [Google Scholar] [CrossRef]
- Zayet, S.; Lang, S.; Garnier, P.; Pierron, A.; Plantin, J.; Toko, L.; Royer, P.Y.; Villemain, M.; Klopfenstein, T.; Gendrin, V. Leclercia adecarboxylata as Emerging Pathogen in Human Infections: Clinical Features and Antimicrobial Susceptibility Testing. Pathogens. 2021, 10, 1399. [Google Scholar] [CrossRef]
- Alosaimi, R.S.; Muhmmed Kaaki, M. Catheter-Related ESBL-Producing Leclercia adecarboxylata septicemia in hemodialysis patient: An emerging pathogen? Case Rep. Infect. Dis. 2020, 2020, 7403152. [Google Scholar] [CrossRef] [PubMed]
- Li, P.K.; Chow, K.M.; Cho, Y.; Fan, S.; Figueiredo, A.E.; Harris, T.; Kanjanabuch, T.; Kim, Y.L.; Madero, M.; Malyszko, J.; et al. ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment. Perit. Dial. Int. 2022, 42, 110–153. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing, 28th ed.; CLSI Supplement M100; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Stewart, L.A.; Clarke, M.; Rovers, M.; Riley, R.D.; Simmonds, M.; Stewart, G.; Tierney, J.F.; PRISMA-IPD Development Group. Preferred reporting items for systematic review and meta-analyses of individual participant data: The PRISMA-IPD statement. JAMA 2015, 313, 1657–1665. [Google Scholar] [CrossRef]
- Hwang, H.Y.; Jeong, S.H.; Rim, H.; Rim, H.; Kim, M.H.; Jeong, T.J.; Choi, B.G. A case of Leclercia adecarboxylata isolated from dialysate in a patient with continuous ambulatory peritoneal dialysis. Korean J. Clin. Microbiol. 1998, 1, 113–116. [Google Scholar]
- Fattal, O.; Deville, J.G. Leclercia adecarboxylata peritonitis in a child receiving chronic peritoneal dialysis. Pediatr. Nephrol. 2000, 15, 186–187. [Google Scholar] [CrossRef]
- Rodríguez, J.A.; Sánchez, F.J.; Gutiérrez, N.; García, J.E.; García-Rodríguez, J.A. Bacterial peritonitis due to Leclercia adecarboxylata in a patient undergoing peritoneal dialysis. Enferm. Infecc. Microbiol. Clin. 2001, 19, 237–238. [Google Scholar] [CrossRef]
- Lee, H.N.; Park, J.W.; Kim, H.S.; Park, S.H.; Chang, J.H.; Chung, W.K.; Lee, H.H.; Seo, Y.H.; Kim, S. Peritonitis due to Leclercia adecarboxylata in a patient receiving automated peritoneal dialysis. Kidney Res. Clin. Pract. 2009, 28, 681–684. [Google Scholar]
- Lee, W.; Yi, D.Y.; Jung, B.; Huh, J.Y.; Kang, M.S.; Hong, S.G.; Hong, S.K. Two cases of independent infection by Leclercia adecarboxylata. Infect. Chemother. 2009, 41, 109–112. [Google Scholar] [CrossRef]
- Farinha, A.; Vaz, A.; Assunção, J.; Vinhas, J. Unusual bacteria causing peritonitis in peritoneal dialysis—A single centre experience. Port. J. Nephrol. Hypert. 2013, 27, 187–195. [Google Scholar]
- Chao, C.T.; Hung, P.H.; Huang, J.W.; Tsai, H.B. Cycler cassette rupture with Leclercia adecarboxylata peritoneal dialysis peritonitis. Perit. Dial. Int. 2014, 34, 131–132. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, R.; Misra, R.; Prasad, K.N.; Prasad, N. Peritonitis by Leclercia adecarboxylata in a patient with continuous ambulatory peritoneal dialysis: The first case report from India. Int. J. Res. Med. Sci. 2016, 4, 1254–1256. [Google Scholar] [CrossRef]
- Atas, D.B.; Velioglu, A.; Asicioglu, E.; Arikan, H.; Tuglular, S.; Ozener, C. Polymicrobial peritonitis with Leclercia adecarboxylata in a peritoneal dialysis patient. Saudi J. Kidney Dis. Transpl. 2017, 28, 181–182. [Google Scholar]
- Hobby, G.; Mandavilli, K.; Singh, M. A Case report of Leclercia adecarboxylata peritonitis in a peritoneal dialysis patient with review of the literature. Int. J. Nephrol. Kidney Fail. 2017, 3, 1–2. [Google Scholar] [CrossRef]
- Adapa, S.; Konala, V.M.; Nawaz, F.; Javed, T.; Dhingra, H.; Gutierrez, I.A.; Ramirez, M.L. Peritonitis from Leclercia adecarboxylata: An emerging pathogen. Clin. Case Rep. 2019, 7, 829–831. [Google Scholar] [CrossRef]
- Spiegelhauer, M.R.; Andersen, P.F.; Frandsen, T.H.; Nordestgaard, R.L.M.; Andersen, L.P. Leclercia adecarboxylata: A case report and literature review of 74 cases demonstrating its pathogenicity in immunocompromised patients. Infect. Dis. 2019, 51, 179–188. [Google Scholar] [CrossRef]
- Anuradha, M. Leclercia adecarboxylata isolation: Case reports and review. J. Clin. Diagn. Res. 2014, 8, DD3–DD4. [Google Scholar] [CrossRef]
- Feucherolles, M.; Cauchie, H.M.; Penny, C. MALDI-TOF Mass spectrometry and specific biomarkers: Potential new key for swift identification of antimicrobial resistance in foodborne pathogens. Microorganisms 2019, 7, 593. [Google Scholar] [CrossRef] [PubMed]
- Mazzariol, A.; Zuliani, J.; Fontana, R.; Cornaglia, G. Isolation from blood culture of a Leclercia adecarboxylata strain producing an SHV-12 extended-spectrum beta-lactamase. J. Clin. Microbiol. 2003, 41, 1738–1739. [Google Scholar] [CrossRef] [PubMed]
- Shin, G.W.; You, M.J.; Lee, H.S.; Lee, C.S. Catheter-related bacteremia caused by multidrug-resistant Leclercia adecarboxylata in a patient with breast cancer. J. Clin. Microbiol. 2012, 50, 3129–3132. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference, Publication Year, Language | Country | Age (y) | Gender | Vintage on PD (Months), (Etiology) | PD Method | Previous Peritonitis | |
|---|---|---|---|---|---|---|---|
| 1 | [9], 1998, (Korean) | Korea | 60 | M | NA | CAPD | NA |
| 2 | [10] *, 2000, (English) | USA | 5 | M | 9, (NA) | CDPD | 2 m previous (coagulase-negative Staphylococcus) |
| 3 | [11] *, 2001, (Spanish) | Spain | 74 | M | NA | NA | NA |
| 4 | [12] *, 2009, (Korean) | Korea | 56 | M | 24, (diabetic ESRD) | APD | No |
| 5 | [13], 2009, (Korean) | Korea | 60 | F | 7, (diabetic ESRD) | NA | No |
| 6 | [14], 2013, (English) | Portugal | 77 | F | 51, (NA) | CAPD | 1 |
| 7 | [15] *, 2014, (English) | Taiwan | 48 | F | 24, (diabetic ESRD) | APD | NA |
| 8 | [16] *, 2016, (English) | India | 38 | F | 44, (NA) | CAPD | NA |
| 9 | [17] *, 2017, (English) | Turkey | 72 | F | 60, (chronic glomerulonephritis) | CAPD | NA |
| 10 | [18] *, 2017, (English) | USA | 68 | F | 84, (diabetic ESRD) | CCPD | Multiple prior episodes of PD peritonitis |
| 11 | [19] *, 2019 (English) | USA | 48 | F | 24, (diabetic ESRD) | APD | No |
| 12 | [3] *, 2021, (English) | France | 71 | F | NA | NA | NA |
| 13 | 2022, (English) | Greece | 14.5 | M | 48, (focal segmental glomerulonephritis) | NIPD | 1st 11.5 years old, 2nd 13.5 years old (both due to Staphylococcus spp.) |
| Case | Identification Diagnostic Tool |
|---|---|
| 1 | NA |
| 2 | VITEK GN card (BioMerieux, Hazelwood, MO, USA) |
| 3 | WIDE API 32 GN (BioMerieux, Marcy l’Etoile, France) |
| 4 | VITEK-II GN card (BioMerieux, Marcy l’Etoile, France) |
| 5 | VITEK GN card (BioMerieux, Hazelwood, MO, USA) |
| 6 | NA |
| 7 | NA |
| 8 | BD Phoenix system (BD Diagnostic Systems, Sparks, MD, USA) |
| 9 | NA |
| 10 | NA |
| 11 | VITEK MS—Matrix Assisted Laser Desorption Ionization Time-of-Flight (BioMerieux, Marcy l’Etoile, France) |
| 12 | Matrix-Assisted Laser Desorption Ionization Time-of-Flight (Biotyper-Microflex, Bruker Daltonics, Bremen, Germany) |
| 13 | VITEK-II GN card (bioMérieux, Marcy l’Etoile, France) |
| Case | Treatment | Catheter Removal |
|---|---|---|
| 1 | cephalothin + amikacin/ip | No |
| 2 | ceftazidime + gentamicin/iv + ip for 10 days | No |
| 3 | NA | No |
| 4 | ceftazidime/ip for14 days | No |
| 5 | cefpiramide/ip for 12 days | No |
| 6 | ceftazidime/ip for 15 days | No |
| 7 | cefazolin/ip | No |
| 8 | tobramycin + cefazolin/ip => amikacin/ip | Yes |
| 9 | cefuroxime/ip, ciprofloxacin/pos => imipenem/iv for 21 days | No |
| 10 | vancomycin + ceftazidime/ip => ceftazidime/ip for 21 days | Yes |
| 11 | vancomycin + ceftazidime/ip => cefazolin/ip for 21 days | No |
| 12 | amoxicillin/iv | No |
| 13 | vancomycin + ceftazidime/ip => ceftazidime/ip for 21 days | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dotis, J.; Kondou, A.; Karava, V.; Sotiriou, G.; Papadopoulou, A.; Zarras, C.; Michailidou, C.; Vagdatli, E.; Printza, N. Leclercia adecarboxylata in Peritoneal Dialysis Patients: A Systematic Review. Pediatr. Rep. 2023, 15, 293-300. https://doi.org/10.3390/pediatric15020025
Dotis J, Kondou A, Karava V, Sotiriou G, Papadopoulou A, Zarras C, Michailidou C, Vagdatli E, Printza N. Leclercia adecarboxylata in Peritoneal Dialysis Patients: A Systematic Review. Pediatric Reports. 2023; 15(2):293-300. https://doi.org/10.3390/pediatric15020025
Chicago/Turabian StyleDotis, John, Antonia Kondou, Vasiliki Karava, Georgia Sotiriou, Athina Papadopoulou, Charalampos Zarras, Chrysi Michailidou, Eleni Vagdatli, and Nikoleta Printza. 2023. "Leclercia adecarboxylata in Peritoneal Dialysis Patients: A Systematic Review" Pediatric Reports 15, no. 2: 293-300. https://doi.org/10.3390/pediatric15020025