
Comparison of Antibody Persistence up to 6 Months after Additional Booster Vaccination with ChAdOx1 nCoV-19 Vaccine
 , and
, and 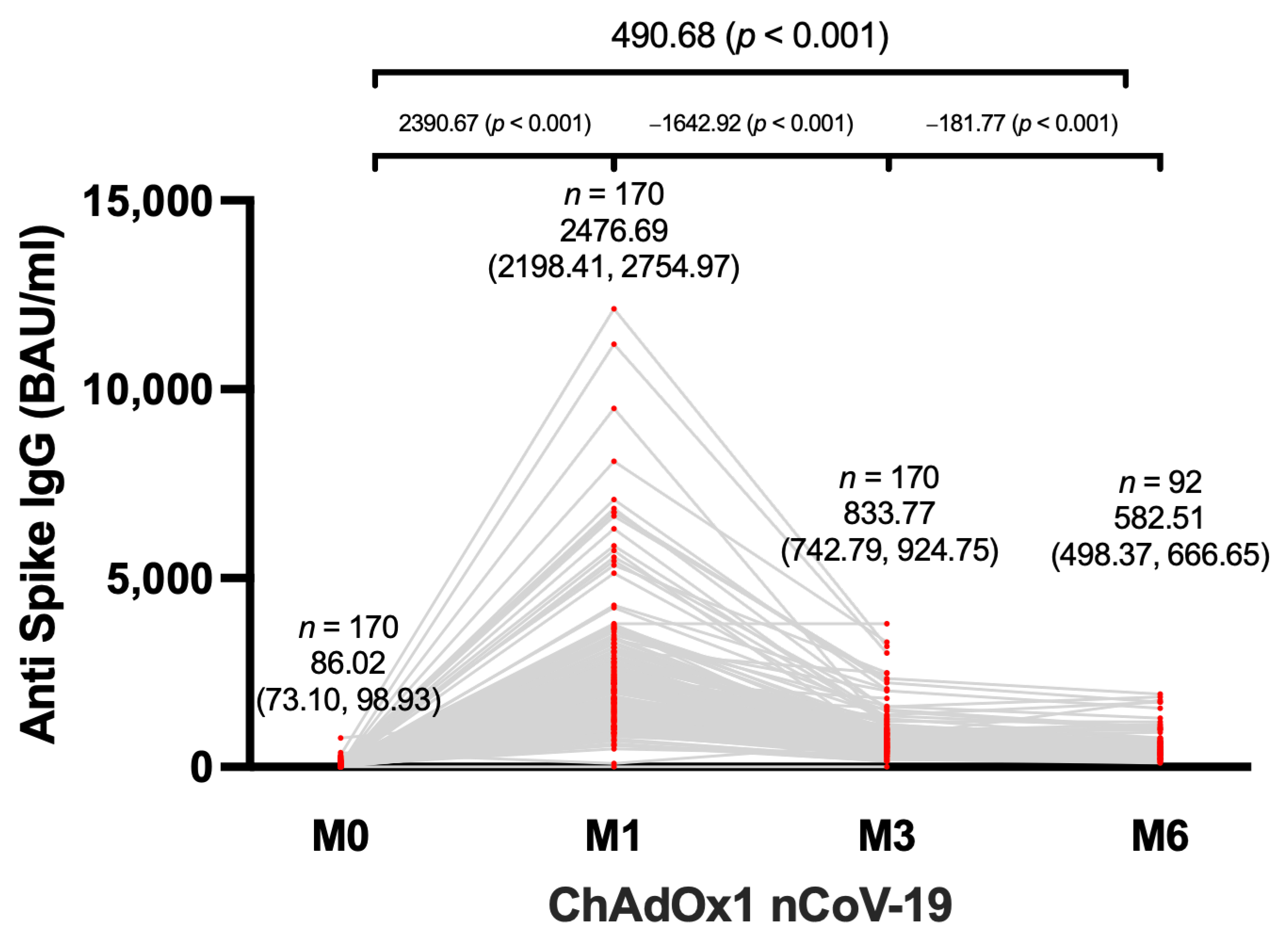{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Antibody Measurement
2.2. Statistical Analysis
2.3. Research Ethics and Trial Registration
3. Results
3.1. Characteristics of Participants
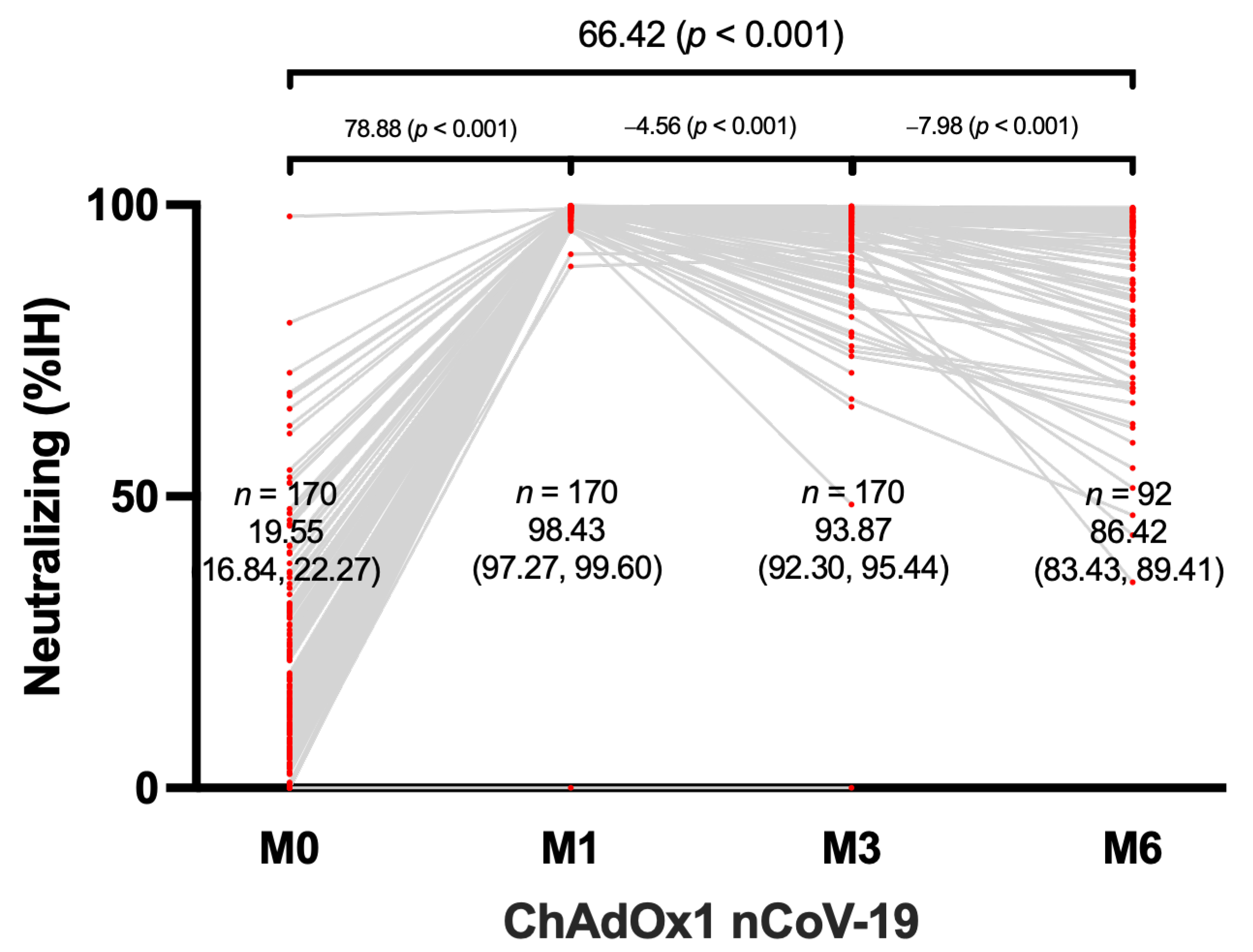
3.2. Humoral Immunogenicity
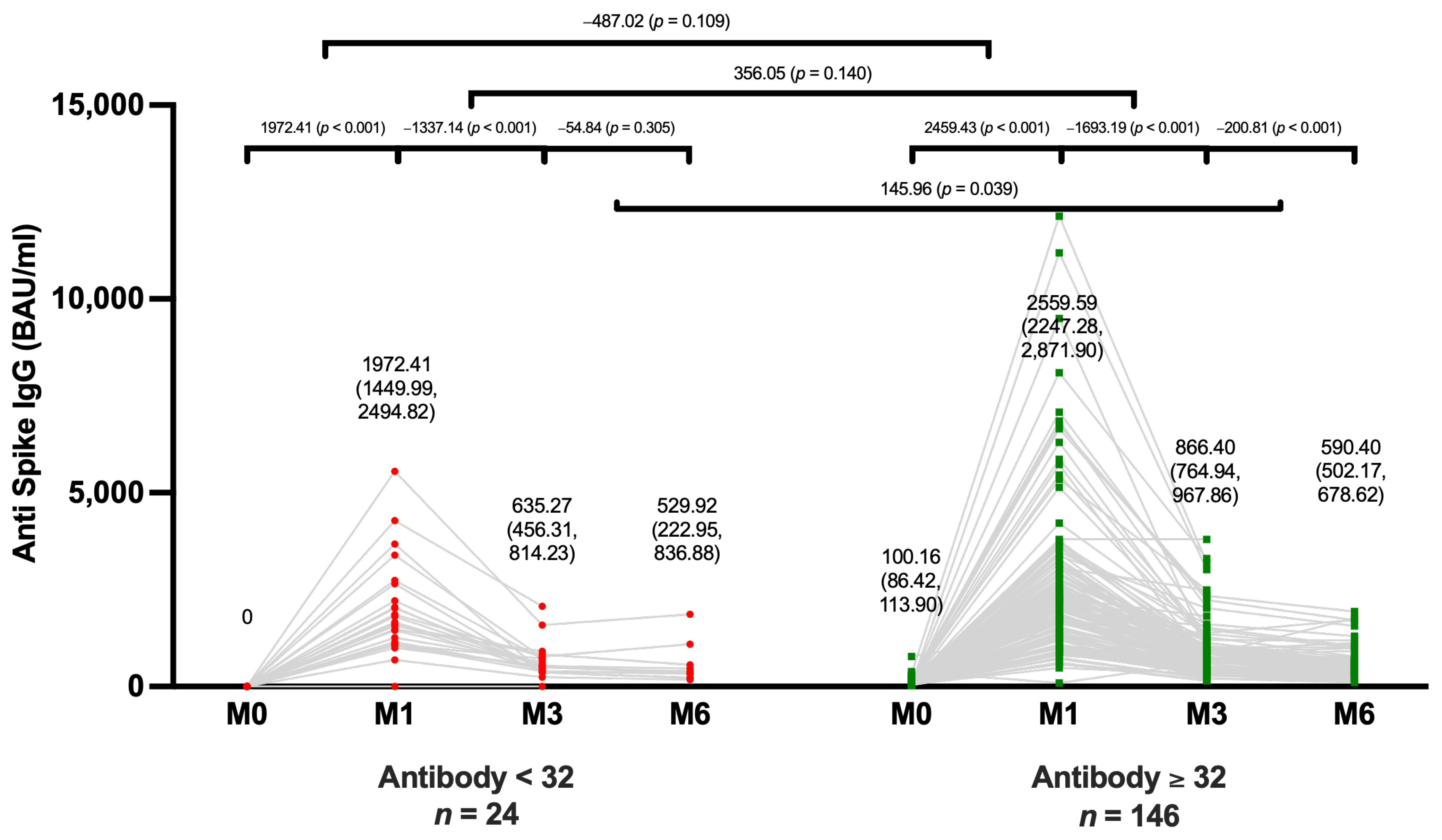
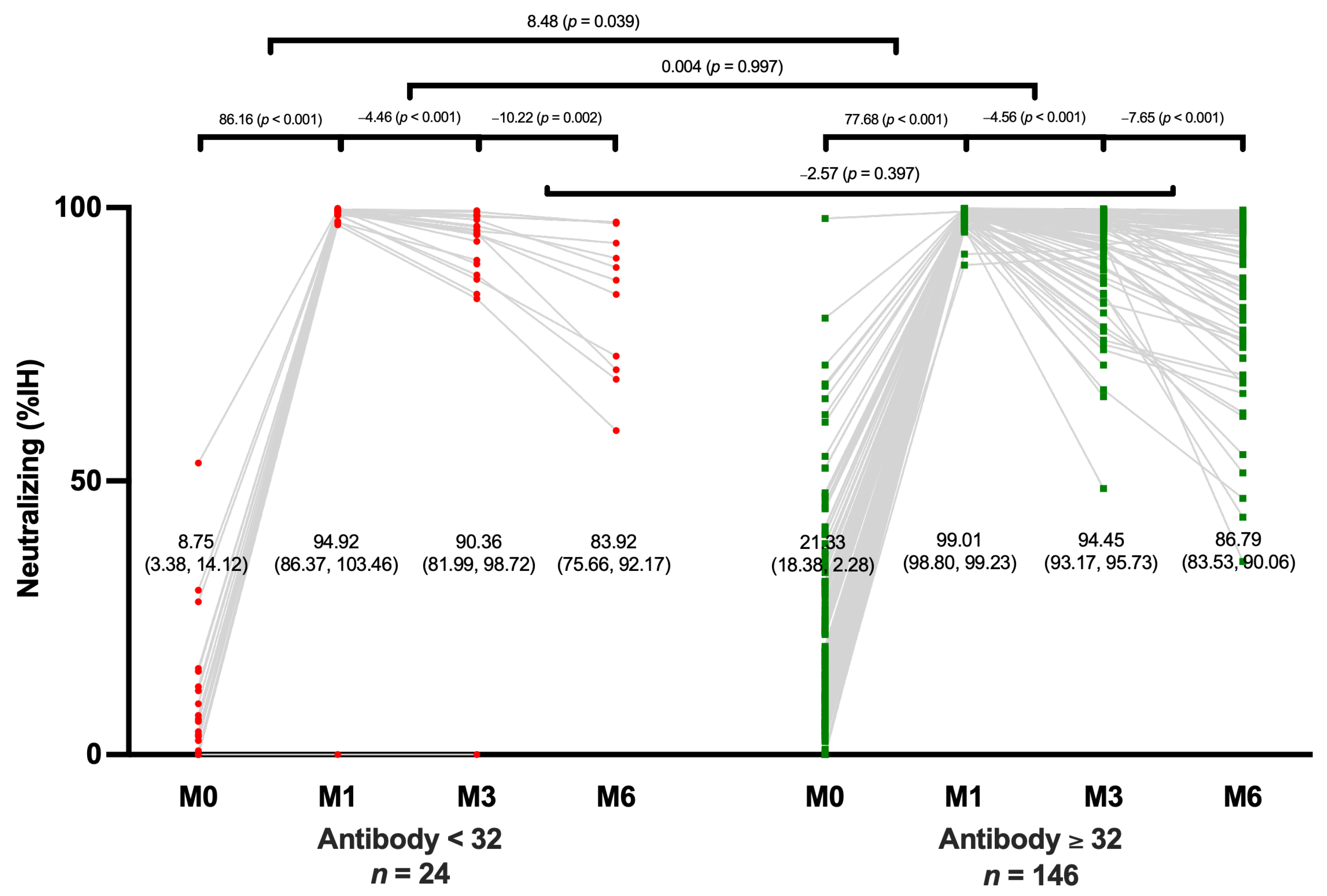
3.3. Comparisons of an Antibody Level between Positive vs. Negative IgG Subgroups
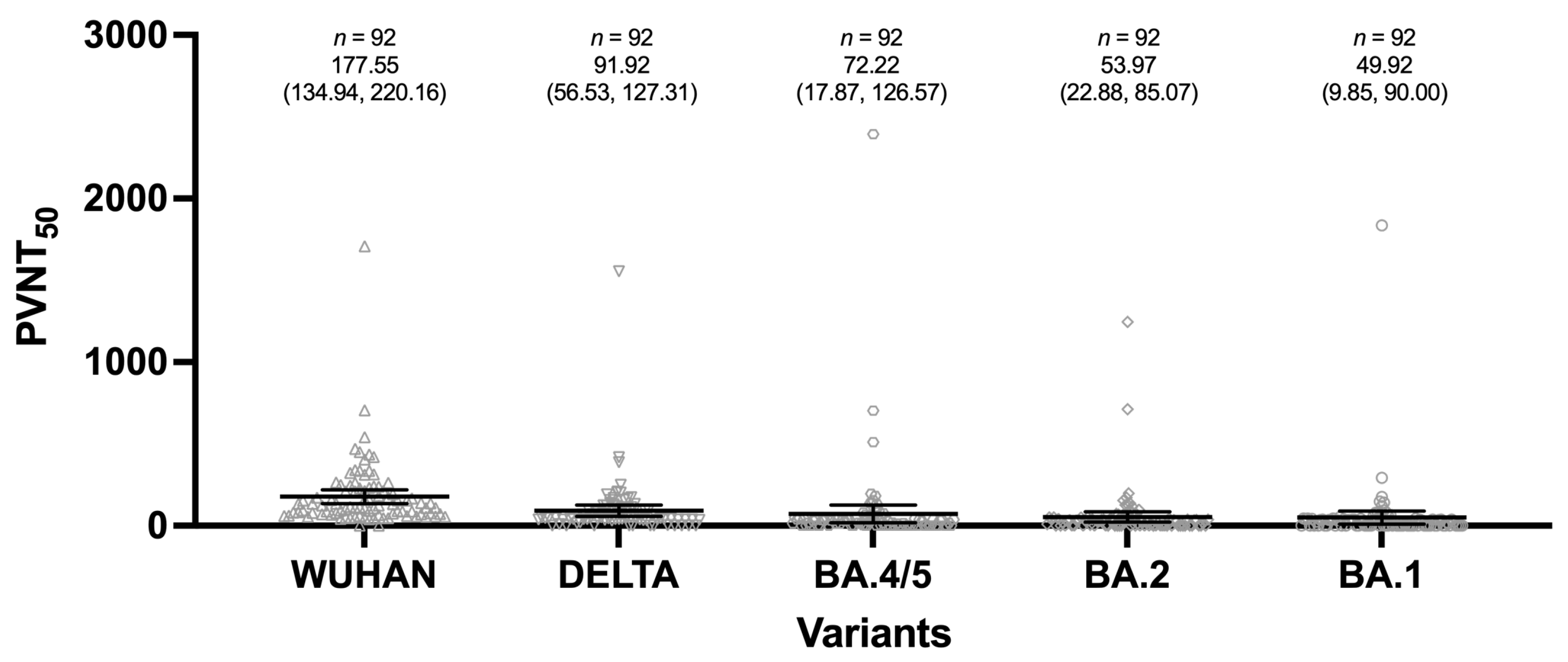
3.4. Neutralizing Antibody Responses to SARS-CoV-2 Variants 6 Months after Boosting
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fiolet, T.; Kherabi, Y.; MacDonald, C.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef] [PubMed]
- Chew, N.; Cheong, C.; Kong, G.; Phua, K.; Ngiam, J.; Tan, B.; Wang, B.; Hao, F.; Tan, W.; Han, X.; et al. An Asia-Pacific study on healthcare workers’ perceptions of, and willingness to receive, the COVID-19 vaccination. Int. J. Infect. Dis. 2021, 106, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Nopsopon, T.; Pongpirul, K.; Chotirosniramit, K.; Hiransuthikul, N. COVID-19 seroprevalence among hospital staff and preprocedural patients in Thai community hospitals: A cross-sectional study. BMJ Open 2021, 11, e046676. [Google Scholar] [CrossRef] [PubMed]
- Nopsopon, T.; Pongpirul, K.; Chotirosniramit, K.; Jakaew, W.; Kaewwijit, C.; Kanchana, S.; Hiransuthikul, N. Seroprevalence of hospital staff in a province with zero COVID-19 cases. PLoS ONE 2021, 16, e0238088. [Google Scholar] [CrossRef] [PubMed]
- Benjamanukul, S.; Traiyan, S.; Yorsaeng, R.; Vichaiwattana, P.; Sudhinaraset, N.; Wanlapakorn, N.; Poovorawan, Y. Safety and immunogenicity of inactivated COVID-19 vaccine in health care workers. J. Med. Virol. 2021, 94, 1442–1449. [Google Scholar] [CrossRef] [PubMed]
- Keskin, A.; Bolukcu, S.; Ciragil, P.; Topkaya, A. SARS-CoV-2 specific antibody responses after third CoronaVac or BNT162b2 vaccine following two-dose CoronaVac vaccine regimen. J. Med. Virol. 2022, 94, 39–41. [Google Scholar] [CrossRef] [PubMed]
- Munro, A.; Janani, L.; Cornelius, V.; Aley, P.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): A blinded, multicentre, randomised, controlled, phase 2 trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef] [PubMed]
- Flaxman, A.; Marchevsky, N.; Jenkin, D.; Aboagye, J.; Aley, P.; Angus, B.; Belij-Rammerstorfer, S.; Bibi, S.; Bittaye, M.; Cappuccini, F.; et al. Reactogenicity and immunogenicity after a late second dose or a third dose of ChAdOx1 nCoV-19 in the UK: A substudy of two randomised controlled trials (COV001 and COV002). Lancet 2021, 398, 981–990. [Google Scholar] [CrossRef] [PubMed]
- Prasithsirikul, W.; Pongpirul, K.; Nopsopon, T.; Phutrakool, P.; Pongpirul, W.; Samuthpongtorn, C.; Suwanwattana, P.; Jongkaewwattana, A. Immunogenicity of ChAdOx1 nCoV-19 Booster Vaccination Following Two CoronaVac Shots in Healthcare Workers. Vaccines 2022, 10, 217. [Google Scholar] [CrossRef] [PubMed]
- Ministry Recommends Boosters Every 4 Months. Available online: https://www.bangkokpost.com/thailand/general/2327243/ministry-recommends-boosters-every-4-months (accessed on 4 April 2023).
- Infantino, M.; Pieri, M.; Nuccetelli, M.; Grossi, V.; Lari, B.; Tomassetti, F.; Calugi, G.; Pancani, S.; Benucci, M.; Casprini, P.; et al. The WHO International Standard for COVID-19 serological tests: Towards harmonization of anti-spike assays. Int. Immunopharmacol. 2021, 100, 108095. [Google Scholar] [CrossRef] [PubMed]
- Wolter, N.; Jassat, W.; Walaza, S.; Welch, R.; Moultrie, H.; Groome, M.; Amoako, D.; Everatt, J.; Bhiman, J.; Scheepers, C.; et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: A data linkage study. Lancet 2022, 399, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Auvigne, V.; Vaux, S.; Strat, Y.; Schaeffer, J.; Fournier, L.; Tamandjou, C.; Montagnat, C.; Coignard, B.; Levy-Bruhl, D.; Parent du Châtelet, I. Severe hospital events following symptomatic infection with Sars-CoV-2 Omicron and Delta variants in France, December 2021–January 2022: A retrospective, population-based, matched cohort study. EClinicalMedicine 2022, 48, 101455. [Google Scholar] [CrossRef] [PubMed]
- Rose, W.; Raju, R.; Babji, S.; George, A.; Madhavan, R.; Leander Xavier, J.; David Chelladurai, J.; Nikitha, O.; Deborah, A.; Vijayakumar, S.; et al. Immunogenicity and safety of homologous and heterologous booster vaccination of ChAdOx1 nCoV-19 (COVISHIELD™) and BBV152 (COVAXIN®): A non-inferiority phase 4, participant and observer-blinded, randomised study. Lancet Reg. Health Southeast Asia 2023, 12, 100141. [Google Scholar] [CrossRef] [PubMed]
- Kirsebom, F.; Andrews, N.; Sachdeva, R.; Stowe, J.; Ramsay, M.; Lopez Bernal, J. Effectiveness of ChAdOx1-S COVID-19 booster vaccination against the Omicron and Delta variants in England. Nat. Commun. 2022, 13, 7688. [Google Scholar] [CrossRef] [PubMed]
- Ladyhets, B. What to Know about the Newest, Most Contagious Omicron Subvariants. Time. 15 June 2022. Available online: https://time.com/6187762/ba-4-ba-5-omicron-subvariants-symptoms-risk/ (accessed on 4 April 2023).
- Wong, M.; Dhaliwal, S.; Balakrishnan, V.; Nordin, F.; Norazmi, M.; Tye, G. Effectiveness of Booster Vaccinations on the Control of COVID-19 during the Spread of Omicron Variant in Malaysia. Int. J. Environ. Res. Public Health 2023, 20, 1647. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suwanwattana, P.; Han, M.; Nopsopon, T.; Phutrakool, P.; Samuthpongtorn, C.; Pongpirul, W.; Prasithsirikul, W.; Pongpirul, K. Comparison of Antibody Persistence up to 6 Months after Additional Booster Vaccination with ChAdOx1 nCoV-19 Vaccine. Microbiol. Res. 2023, 14, 810-818. https://doi.org/10.3390/microbiolres14020057
Suwanwattana P, Han M, Nopsopon T, Phutrakool P, Samuthpongtorn C, Pongpirul W, Prasithsirikul W, Pongpirul K. Comparison of Antibody Persistence up to 6 Months after Additional Booster Vaccination with ChAdOx1 nCoV-19 Vaccine. Microbiology Research. 2023; 14(2):810-818. https://doi.org/10.3390/microbiolres14020057
Chicago/Turabian StyleSuwanwattana, Pawita, May Han, Tanawin Nopsopon, Phanupong Phutrakool, Chatpol Samuthpongtorn, Wannarat Pongpirul, Wisit Prasithsirikul, and Krit Pongpirul. 2023. "Comparison of Antibody Persistence up to 6 Months after Additional Booster Vaccination with ChAdOx1 nCoV-19 Vaccine" Microbiology Research 14, no. 2: 810-818. https://doi.org/10.3390/microbiolres14020057