1. Introduction
Currently, more than 65 million people have been forced to leave their home countries, and 23 million are refugees and asylum seekers [
1]. Refugees and asylum seekers may hold a higher burden of communicable diseases such as tuberculosis (TB), hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV). For example, the prevalence of TB and measles among Syrian refugees and asylum seekers in host countries was found higher compared to the host population [
2]. In Europe, many communicable diseases (CDs) were reported by refugees and asylum seekers [
3,
4,
5,
6]. It was estimated that 72% of new TB cases in England are related to refugees and asylum seekers [
7]. Within refugee and asylum seeker settings, the CDs burden is mainly related to disease screening and control programs in the host and original countries. Additionally, route conditions reaching the asylum country aggravate the CDs burden [
2]. Furthermore, Asylum seekers may spend protracted periods in transit with limited access to preventative health care and poor living conditions that may magnify CD transmission. For example, alerts were raised about the health status of Syrian asylum seekers who were isolated in deserted refugee camps because of poor access to health services and unfavorable health conditions [
8]. Therefore, while the CDs burden is largely driven by refuge events and international crossing [
3], CDs burden, surveillance and control will remain a source of concern, particularly in low-burden countries managing humanitarian crises [
4,
5,
9,
10].
We aim to estimate the prevalence of TB, HBV, HCV, and HIV in refugees and asylum seekers globally by region of origin and region of destinations (asylum).
2. Materials and Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used (See
Supplementary Materials S7).
We searched four bibliographic databases for indexing articles: PubMed, EMBASE, CINAHL, and Scopus. The searches commenced on 7 July 2018 and concluded on 20 November 2020 and were then updated on 25 December 2022. No limitations were set for time or country. In all four databases, we used a two-part keyword search strategy; in the first part, related to the population, we used ‘Refugee’ and another eight related terms to indicate the population of interest. In the second part, ‘Communicable disease’ and other related terms [
9] were used. The preliminary search formula was Refugee* AND Communicable Disease (See
Supplementary Materials S1–S4).
The keyword ‘Refugee’ was defined as any term used to indicate people fleeing to a safe place, especially those who flee to a foreign country to escape danger or persecution in their own country or habitual residence because of race, religion, or political belief [
9]. ‘Communicable disease’ was defined as ‘an infectious disease transmissible (person to person) by direct or indirect contact (as by a vector)’ [
9]. The definitions of TB (active or latent), hepatitis B, hepatitis C, and HIV diseases were drawn from each reference record included in the review as described by the original author of the study. If it was not clearly mentioned, the definition of the WHO was used to resolve any confusion and have a consistent description of the included diseases.
We used ‘MESH terms’ whenever suitable to capture all relevant studies. Specific terms related to our CDs of interest were hepatitis and HIV, and sexually transmitted diseases were included (See
Supplementary Materials S1–S4). The clear status of each disease, whether it was the acute or past status of the disease, was not considered separately in this review; therefore, each included infection was analyzed based on the general status for the same disease.
Eligibility criteria (inclusion/exclusion)
Articles that fulfilled all the following characteristics were included in the systematic review.
Published, in English, specifically about ‘refugees’ and ‘asylum seekers’ of wars and conflicts.
Reported the prevalence of TB, HBV, HCV, and HIV by formal notification system diagnosis and as a systematic screening process.
Original research with a reportable prevalence denominator and numerator.
We excluded terms other than ‘Refugee’ or ‘asylum seeker’. For example, we excluded studies that referred to immigrants, migrants, or internally displaced people. Any non-empirical literature (letters to editors, commentaries, conference abstracts and transcripts, journalistic interviews, policy reports, and books) and any other studies with no full text available were also excluded. To minimize selection bias, we excluded studies conducted only for specific ages or genders such as children, pregnant women, pediatrics, or unaccompanied minors.
Study Selection (Screening Process)
The screening process conducted on all references is two-stepped:
Title and abstract screening
We used Covidence [
10], a web-based software platform, to manage title, abstract and full-text screening. All article titles and abstracts were screened according to the eligibility criteria by two reviewers (HT and SR). Judgment discrepancies in eligibility were resolved by team discussion (HT, SR, and JD) and consensus. If no clear exclusion criteria were decisive, we obtained the full text for references that were considered relevant by at least one reviewer.
Full-text screening and reading
After screening the title and abstract, we obtained full texts of included references. Independently, two reviewers (HT and SR) read the full text of the references and assessed their eligibility for inclusion. Conflicts regarding including references were resolved by discussions (HT, SR, and JD).
Data collection process (extraction)
We manually developed a data extraction sheet including the following items: study objectives (title) or research questions; years of publication; year of study; first author; population; country of origin; sampling method; sample coverage, instruments; study type; diseases under observation; sample size; prevalence; etc. (See
Supplementary Materials S5). Wherever possible, data about specific population categories (i.e., Africa or Asia) were extracted and identified as part of our population of interest. We used the authors’ definitions of each disease status as stated in the studies.
Risk of bias in individual studies (critical appraisal)
We used Hoy et al.’s tool for quality assessment [
11] to critically appraise the included studies (See
Supplementary Materials S6). The risk of bias was assessed based on the questions included in the assessment tool and based on the following process: a score of 0 was given for questions answered as yes (low risk), and a score of 1 to those answered as no (high risk); then, the total number of scores was calculated. Consequently, the risk of bias was described according to the scale by calculating points out of 10: low risk scored 0–3; moderate risk scored 4–7, and high risk scored 8–10. Unanswerable questions were titled as not applicable (
Table 1).
Prevalence records synthesis
We synthesized each prevalence record and noticed that a single study might include several prevalence records. Therefore, we extracted each prevalence record (comprised of denominator and numerator) in every included study, then assigned corresponding study information (author) for each extracted prevalence record and removed the duplicate records. We used extracted records to conduct the meta-analysis.
Meta-analysis
We used the Stata software package [
12] to measure consistency (I
2 test) and conduct a meta-analysis. We identified the numerator and denominator and conducted a random-effects meta-analysis to test the variability between included studies. We conducted pooled estimates under the supposition that each record of prevalence had dissimilar features and was measured differently. To investigate possible sources of heterogeneity, we undertook a subgroup analysis by stratifying the data by regions and CD type. We adopted the World Health Organization’s (WHO) definition of the regional grouping of countries to categorize studies by (See
Supplementary Materials S8) [
13,
14,
15].
Ethics review
Ethical clearance was not required for this systematic review.
3. Results
Study selection
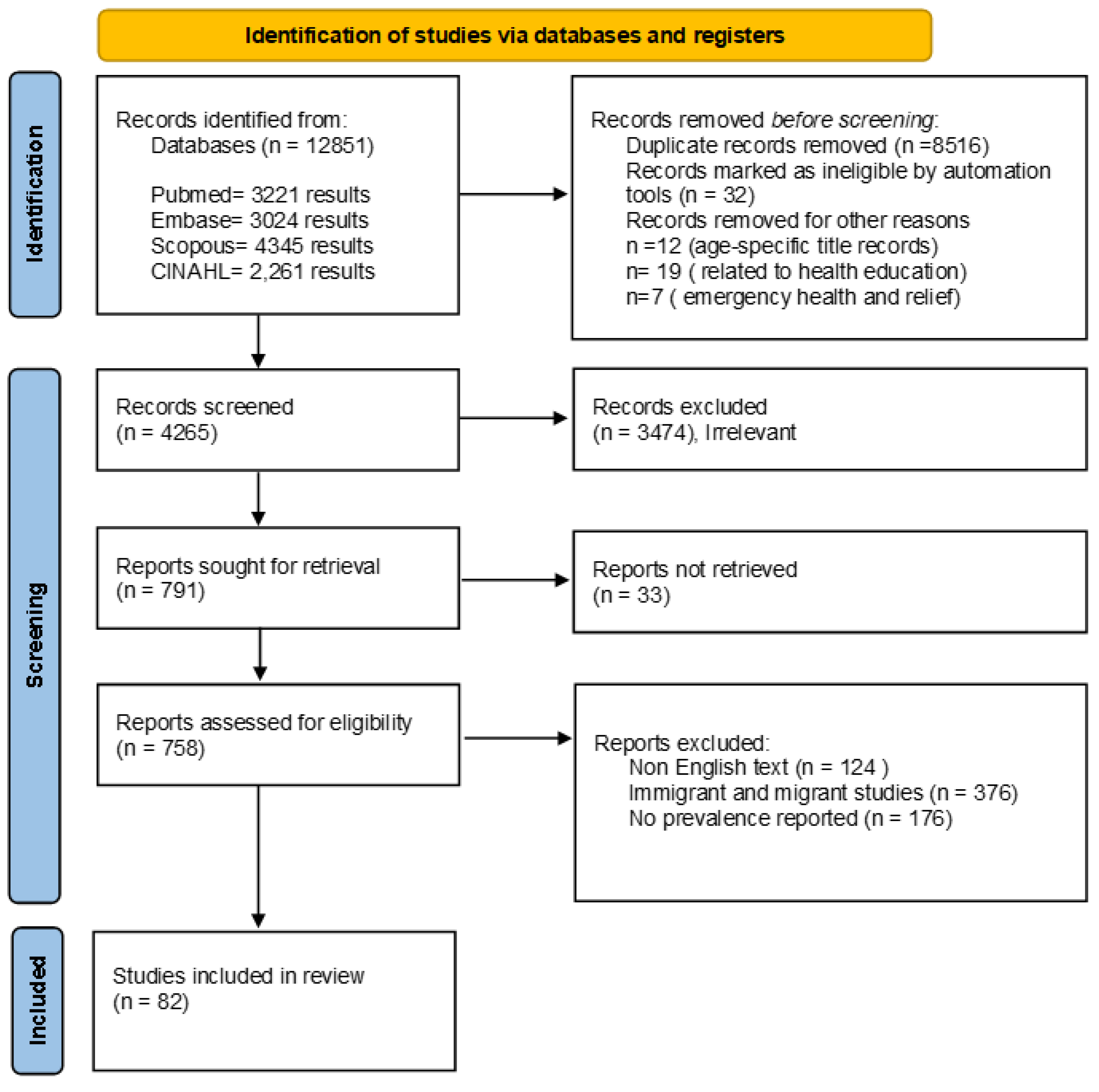
We imported 12,851 references for screening. We screened 4265 unduplicated references, from which 791 were identified for full-text review and included 82 studies ([
16,
17,
18,
19,
20,
21,
22,
23,
24,
25,
26,
27,
28,
29,
30,
31,
32,
33,
34,
35,
36,
37,
38,
39,
40,
41,
42,
43,
44,
45,
46,
47,
48,
49,
50,
51,
52,
53,
54,
55,
56,
57,
58,
59,
60,
61,
62,
63,
64,
65,
66,
67,
68,
69,
70,
71,
72,
73,
74,
75,
76,
77,
78,
79,
80,
81,
82,
83,
84,
85,
86,
87,
88,
89,
90,
91,
92,
93,
94,
95,
96]) (
Figure 1).
Study characteristics
- (A)
Study topics and record synthesis
We included 82 studies representing 279 prevalence records. Studies conducted on TB, hepatitis (B and C) and HIV were as follows: 19 (24%), 20 (24%) and 2 (2.5%), respectively; the remaining studies (50%) conducted general health screening. We extracted 122 (44%), 99 (35%), 30 (11%) and 28 (10%) prevalence records of TB, HBV, HCV, and HIV, respectively. Most of the included studies were published by the United States of America (USA), 26 (32%); Italy, 11 (13%) and Australia, 7 (9%). We adopted the WHO’s definition of the regional grouping of countries to categories studies by regions; however, 26% of the records did not report country and were therefore put in a (Not specified) category. The most frequently reported regions of origin among the overall included records (n = 279) were as follows: Asia and the Eastern Mediterranean, 103 (37%), Africa, 63 (23%) and Europe, 34 (12%). For representation’s validity, results will be discussed as regions only (
Table 2).
Meta-analysis and quality of included studies.
Generally, we found substantial variability among the included studies in terms of study objective, design, sample size, and Refugee and Asylum Seeker (RAS) regions of origin and periods (See
Supplementary Materials S9). Consequently, it was difficult to apply the quality assessment protocol to included studies because we were unable to answer three questions (Not Applicable) of the tool for 96% of the included studies (78/82). However, most studies had a low to moderate risk of bias and internal validity had a low to moderate risk of bias, while external validity had a low risk of bias. Heterogeneity was significantly high in individual estimates among all included CD studies, even after stratification, and ranged between 85 and 99%. For further information regarding the meta-analysis, please refer to the
Supplementary Material S9.
TB Prevalence
Most TB records (n = 122) were reported by the USA, 40 (33%), Australia and Germany, 14 (11%). We reported TB type as stated by the author of the included papers; however, if not specified, prevalence records were added to the ‘Unknown’ category (49%). A significant number of included papers (n = 52) did not report the used diagnostic tests to confirm TB diagnosis; however, they stated TB type. Therefore, we reported TB type as stated by the authors and did not report the diagnostic tests used because it was not comprehensively reported and was missing originally in a significant number of included studies.
Active TB
Active TB records (n = 29) were reported between the years 1981 and 2016, mostly by Germany and the United Kingdom (8/29) and in the years 2002 (9/29) and 2017 (8/29). However, the highest prevalence record of active TB (0.19) was in African RASs in Europe, and Belgium (19).
Latent TB
Latent TB records (n = 32) were reported between the years 1980 and 2018, mostly in the USA (15/32) and in the year 2009 (7/32). The highest prevalence of latent TB (0.70) was reported in Asian and Eastern Mediterranean RASs in the Western Pacific, Australia [
61]. Among all statistically significant heterogeneous estimates, latent TB in RASs from Europe was insignificantly heterogeneous and had a prevalence estimate of <0.01 (95% CI: 0.00–0.01, I
2 = 27%,
p-value = 0.25). The following
Table 3 presents the TB results.
HBV Prevalence
Included HBV records (n = 99) were reported between the years 1978 and 2018, mostly by the USA (39/99), Australia (13/99) and Italy (11/99) and in the years 2010 (15/99) and 2015 (11/99). The highest prevalence of HBV (0.48) was reported in Asian and Eastern Mediterranean RASs in the Western Pacific, Australia [
18] (
Table 4). A significant number of included papers (n = 41) did not report the used diagnostic tests to confirm HBV diagnosis. Therefore, we adopted the author’s definition of the HBV case and did not report the diagnostic tests used because it was not comprehensively reported and was missing originally in a significant number of included HBV studies.
HCV Prevalence
Included HCV records (n = 30) were reported between the years 1995 and 2018, mostly by Italy (6/30) and in the year 2015 (8/30). However, the highest prevalence record of HCV (0.31) was reported in Asian and Eastern Mediterranean RASs in Europe [
75]. Among all statistically significant heterogeneous estimates, HCV heterogeneity was insignificant in RASs in Asia and the Eastern Mediterranean and Western Pacific, with prevalence estimates of 0.03 (95% CI: 0.01–0.05, I
2 = 11%,
p-value = 0.33) and 0.02 (95% CI: 0.01–0.02, I
2 = 3%,
p-value = 0.39), respectively (
Table 5).
HIV Prevalence
Included HIV records (n = 28) were reported between the years 1995 and 2018, mostly in Italy and Germany (6/28) and in 2015 (6/28). The highest HIV prevalence (0.27) was reported in African RASs in Africa [
38] (
Table 6).
4. Discussion
This systematic review and meta-analysis include a significantly high coverage of studies (n = 82) compared to other reviews [
97,
98]. This is most likely explained due to the unrestricted search strategy conducted for this systematic review, to allow the capture of a wide range of studies from different origins and asylum countries. For example, other reviews [
7,
97] were conducted in specific settings only, such as country and time, and therefore included fewer studies. However, our review included a fewer number of studies compared to other conducted reviews that were restricted to time and location [
86]. This could be explained by the discrepancy in eligibility criteria each review undertakes and the relevance/aims of each. Therefore, the aim of this review justifies the high yet reasonable number of included studies.
The overall heterogeneity in this review is high (I
2 = 64–99) across all studies, even after stratification. This was evident in other reviews (24, 27, 28) conducted on a fewer number of studies [
98] and/or restricted to a single country and time [
97]. Heterogeneity is most likely explained as a real difference in CDs prevalence between RASs of different origin and asylum regions; as well, the epidemiologic status of CDs constantly changes over time within and between states, territories, and individuals, and like other diseases varies between regions and certain risk groups [
99]. However, compared to other reviews that reported high heterogeneity levels (97–99%), our review reported less heterogeneity across included studies when stratified by region. The sub-analysis by regions generated low heterogeneous prevalence results in three regions, as follows: latent TB prevalence in RASs from Europe (<0.00, 95% CI: 0.00–0.01, I
2 = 27.42,
p-value = 0.25), HCV prevalence in RASs in Asia and the Eastern Mediterranean (0.03, 95% CI: 0.01–0.05, I
2 = 11.70,
p-value = 0.33) and the Western Pacific (0.02, 95% CI: 0.01–0.02, I
2 = 3.75,
p-value = 0.39). Therefore, considering I
2 = 75% as a threshold for high heterogeneity, our meta-analysis showed relatively low levels of heterogeneity and might propose a promising method to direct and conduct future research in this field.
We found TB to be the most prevalent CD among RASs (19 studies and 122 records), particularly in Europe (50/122). This is consistent with other studies that reported RAS epidemiological data [
100,
101]. This might be linked to the past decade’s increase in the movement of RASs to European countries, which might be reflected in TB reporting. Since 2008, there has been a noticeable increase in the number of RASs hosted in Europe, which reached 5.2 million at the end of 2016 [
102]. Therefore, TB prevalence among RASs may be explained by the continuous implementation of TB control programs such as screening at entry, by considering TB a major global health issue and a leading cause of mortality worldwide [
97,
103], particularly among RASs and international travelers from high-TB-burden countries. These results were similarly observed in a study conducted in Europe to evaluate migrants from the sub-Saharan countries [
104]; the study found that almost 14% of the migrants had TB, which highlights again the importance of TB screening for early diagnosis and treatment in the country of asylum [
104]. Furthermore, considering the health status of the migrants by screening at entry is very important for controlling the spread of TB among the local population, particularly as migrants are usually more exposed and more vulnerable than any other populations to diseases, whether chronic or infectious, despite healthy presentation at arrival [
105].
We found differences in the prevalence ranges between active and latent TB. For example, we found a large disparity between the results of active TB between different regions, <0.01 and 0.6, which might indicate considerable variations between the included studies. However, we noticed that most of the reported prevalence is legitimately valid based on the methods used at that time. For example, the study that reported the highest active TB prevalence [
39] used a TB notification system with a sample size (n = 8293) large enough to conclude the prevalence of active TB in RASs. Although this reported prevalence is inhomogeneous and considerably higher compared to other included records in our review [
65], the results are reliable because there is a similarity in TB case notification rates between the reference country and our study in that same year. Yet, the study identifies 56 subjects lost to follow-up and assumes higher cases of active TB [
39]. On the other hand, the reported maximum prevalence of latent TB between regions ranges between 0.50 and 0.70 is more consistent and considered higher than active TB, except for the Pacific (0.04) and The Americas (<0.01) (only one record for each). This may be explained by the diagnostic and reporting difficulties of active TB compared to latent TB. A patient’s medical history and a single test, a TB skin test, may be sufficient to diagnose and report latent TB. However, more complex procedures, such as chest radiographs and microbiology tests, are needed to diagnose active TB [
106]. Therefore, most of the studies might have reported latent TB more consistently and frequently than active TB [
101]. We found that RASs from the Asia and Eastern Mediterranean region had the highest HBV prevalence among RASs. These findings are consistent with other reviews [
107,
108] that associated RASs from East Asia with higher disease risks [
107].
Based on regions of origin, HBV prevalence estimates ranged from <0.01 to 0.10. However, the highest reported HBV prevalence (0.48) was found in RASs from Asia and the Eastern Mediterranean who sought asylum in the Western Pacific, particularly Australia. These findings are most probably explained by the unprecedented refugee rates and the settling of RASs in low-HBV-burden countries such as Australia. This is further reflected in our findings in other regions such as Africa and Europe that have a comparably high prevalence: 0.37 and 0.27, respectively. Although estimated prevalence is not different among RASs by region of origin, it is subject to a high heterogeneity level (>94%) (See
Table 4).
The finding of this review suggests that RASs from high or intermediate HCV prevalence regions present a high risk for HCV infection. We found that RASs from the Asia and Eastern Mediterranean region have the highest HCV prevalence (0.31). The HCV prevalence from our review is confined within acceptable prevalence ranges reported by other studies [
98,
108,
109]. Globally, HCV prevalence is highest in Asia and the Eastern Mediterranean, Africa and Europe, ranging between 2% and 4%, but is less (<1.5%) in other regions such as Australia and The Americas. Although our findings were consistent with published regional findings, they are subject to the high heterogeneity of pooled estimates. Generally, the epidemiology of HCV is greatly variable within and between countries and regions because it is concentrated in certain risk groups that might alter over time. Therefore, the discrepancy might arise because of the wide range of HCV prevalence in individual countries in the same region [
109,
110]. In our study, the discrepancy in the reported and estimated prevalence may be due to the studies included in our review having a different risk profile of RASs, time, and characteristics of RASs.
We found that RASs from the African region reported the highest HIV prevalence (0.27). The findings are justified as most people living with HIV are in low- and middle-income countries, with an estimated 25 million living in Africa [
111]. Our review suggests that RASs from high-/intermediate-HIV-prevalence regions, such as Africa, present a high risk for HCV infection. However, while previous reviews conducted on HIV in refugee settings were unable to establish sufficient evidence of HIV transmission [
112], our results might be confounded only by the original global HIV distribution. This is further justified by the insufficient data at times of conflict and refugee crisis to conclude that RASs have a higher risk of HIV prevalence. However, our review provided HIV estimates consistent with other reviews conducted, particularly on RASs in African regions. For example, the prevalence of HIV infection ranged from 0.02 to 0.26 in RASs in African countries [
112], matching with our results that range from 0.01 to 0.27, which therefore justifies our findings.
Although there is no consensus in the literature on how RASs could impact the epidemiology of local populations, some studies have discussed the range of risks that could emerge from hosting RASs from different geographical locations with certain infectious disease epidemiology. For example, while some RASs in Europe are found healthier than local populations, they are at higher risk for the main infectious diseases such as TB, HIV, and hepatitis [
113]. This denotes that RASs could potentially be a source of infectious disease for local populations if there is direct or even indirect contact [
114]. This highlights the need for the implementation of broad migrant screening campaigns to control infectious disease transmission from such populations [
113]. On the other hand, it was found that RAS population migration has played a major role in disease transmission by starting outbreaks and increasing the prevalence and incidence of infectious diseases in the country of asylum. Moreover, the RAS population is considered a main factor in introducing infectious diseases and increasing transmission potential with local populations [
114]. For example, in North America, the role of the migrant population, such as refugees, in disease transmission ranged from incubating infections such as hepatitis A, reactivating latent diseases such as TB, or bearing an increased burden of the diseases [
114]. This highlights the challenges that might be faced by local health authorities and the need to manage illnesses and diseases attributed to global factors that are beyond the national disease control strategies and management plans. The type of risk that emerges from the RAS populations will have effects that grow in clinical, control and management nature, which will identify RASs as an important risk group that continuously poses new challenges as more RASs arrive from new geographical regions with variable infectious disease epidemiology and demography [
115].
Limitations
Several limitations were observed in our review. Adjusting for RASs’ characteristics was practically challenging and was therefore reflected in homogeneity levels and findings [
96,
98,
106]. For example, we attempted to report countries of origin/asylum; however, we noticed discrepancies across the literature regarding countries/regions reported without standard geographical classification. Therefore, we chose to report our results according to the WHO’s geo-regional definitions. Overall, 25% did not report geographical origin and were therefore grouped as ‘Not specified’. Failure to report geographical regions affected the validity of the findings and the homogeneity. Additionally, prevalence records were not always reported clearly by the authors and needed manual calculation. RAS definitions were not clear and were indistinguishable from similar populations such as migrants [
7]. This led to the exclusion of many studies that did not clearly define RASs, and therefore a loss of data [
7]. Additionally, studies were not always disease-specific but presented a general description of CDs (n = 40/82). For example, 62/122 (51%) of TB records failed to specify the TB type (active or latent). The overall quality of the risk of bias assessment is affected by including a wide range of studies and study designs [
89,
96].
This review did not provide a separate analysis of each disease status, i.e., whether acute or past, but each included infection was analyzed based on the general status for the same disease. This could have created minor discrepancy in the results compared to other studies that considered the disease status as active vs. latent, for example [
116]. Consequently, the results of this review might be subject to a bias and inaccuracies in the pooled prevalence [
117]. However, considering the aim of this review, this expected bias might have little effect on looking at the overall estimates of the diseases in refugee populations at the countries of asylum, although estimating the status of each disease precisely would provide more confidence and rigor to the review.




{kind=link}