
Hepatitis B Vaccination in Advanced Chronic Kidney Disease: A Quality Improvement Project at a Veteran Affairs Chronic Kidney Disease Clinic

 ,
,
Abstract
:1. Introduction
2. Patient and Methods
2.1. Patient Cohort
2.2. Vaccination
2.3. Statistical Methods
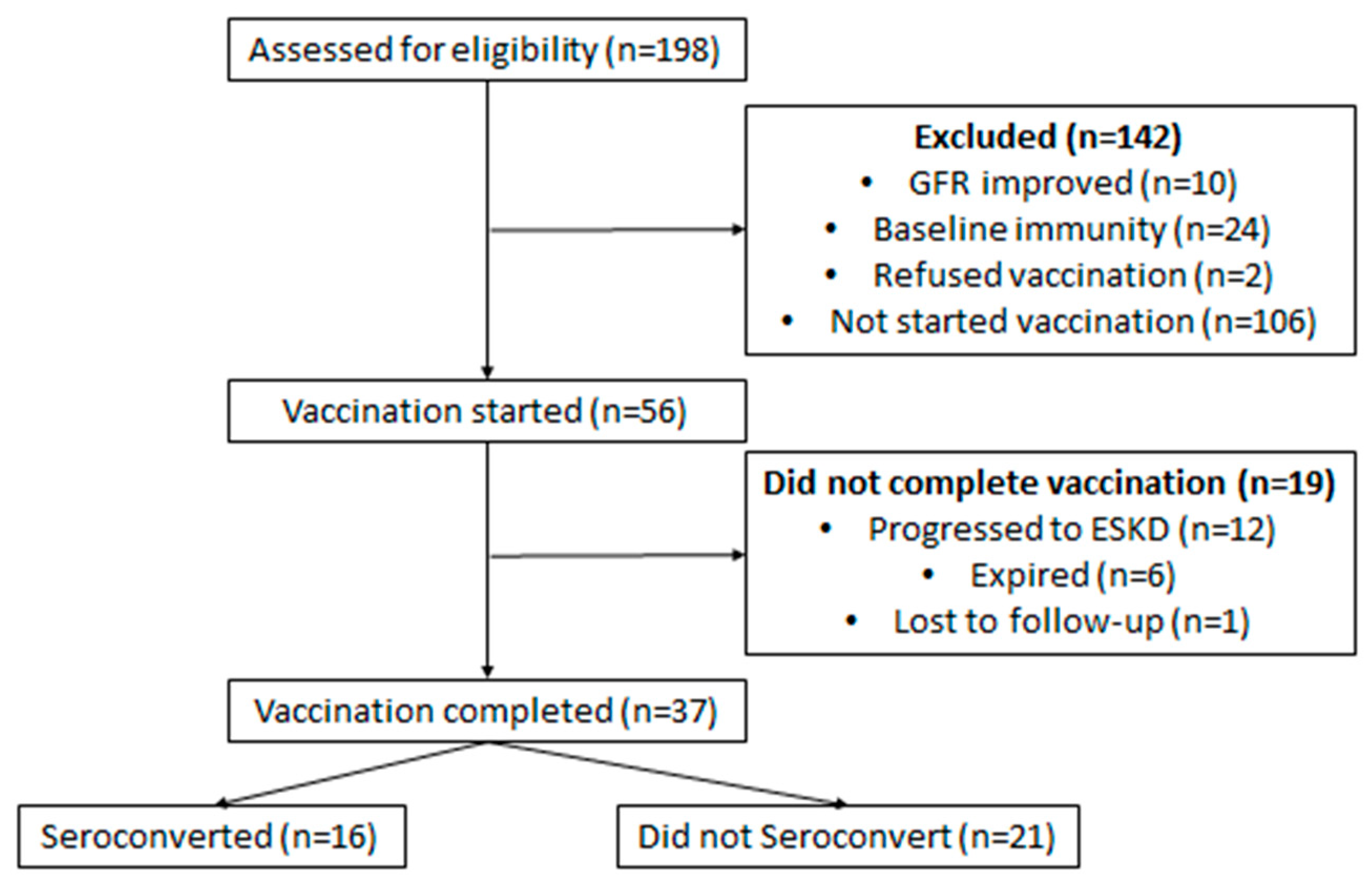
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Figure Legends
References
- Somi, M.H.; Hajipour, B. Improving hepatitis B vaccine efficacy in end-stage renal diseases patients and role of adjuvants. ISRN Gastroenterol. 2012, 2012, 960413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burdick, R.A.; Bragg-Gresham, J.L.; Woods, J.D.; Hedderwick, S.A.; Kurokawa, K.; Combe, C.; Saito, A.; Labrecque, J.; Port, F.K.; Young, E.W. Patterns of hepatitis B prevalence and seroconversion in hemodialysis units from three continents: The DOPPS. Kidney Int. 2003, 63, 2222–2229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maisonneuve, P.; Agodoa, L.; Gellert, R.; Stewart, J.H.; Buccianti, G.; Lowenfels, A.B.; Wolf, R.A.; Jones, E.; Dsiney, A.P.S.; Briggs, D.; et al. Cancer in patients on dialysis for end-stage renal disease: An international collaborative study. Lancet 1999, 354, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Pol, S.; Samuel, D.; Cadranel, J.; Legendre, C.; Bismuth, H.; Bréchot, C.; Kreis, H. Hepatitis and solid organ transplantation. Transplant. Proc. 2000, 32, 454–457. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.R.; Alter, M.J.; Tokars, J.I. Protective effect of hepatitis B vaccine in chronic hemodialysis patients. Am. J. Kidney Dis. 1999, 33, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Grzegorzewska, A.E. Hepatitis B vaccination in chronic kidney disease: Review of evidence in non-dialyzed patients. Hepat. Mon. 2012, 12, e7359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghadiani, M.H.; Besharati, S.; Mousavinasab, N.; Jalalzadeh, M. Response rates to HB vaccine in CKD stages 3-4 and hemodialysis patients. J. Res. Med. Sci. 2012, 17, 527–533. [Google Scholar]
- Shepard, C.W.; Simard, E.P.; Finelli, L.; Fiore, A.E.; Bell, B.P. Hepatitis B virus infection: Epidemiology and vaccination. Epidemiol. Rev. 2006, 28, 112–125. [Google Scholar] [CrossRef] [PubMed]
- Alter, M.J.; Arduino, M.J.; Lyerla, H.C.; Miller, E.R.; Tokars, J.J. Recommendations for preventing transmission of infections among chronic hemodialysis patients. MMWR Recomm. Rep. 2001, 50, 1–43. [Google Scholar] [PubMed]
- Lok, A.S.; McMahon, B.J.; Brown, R.S., Jr.; Wong, J.B.; Ahmed, A.T.; Farah, W.; Almasri, J.; Alahdab, F.; Benkhadra, K.; Mouchli, M.A.; et al. Antiviral therapy for chronic hepatitis B viral infection in adults: A systematic review and meta-analysis. Hepatology 2016, 63, 284–306. [Google Scholar] [CrossRef] [PubMed]
- Grzegorzewska, A.E. Hepatitis B vaccination in chronic kidney disease patients: A call for novel vaccines. Expert Rev. Vaccines 2014, 13, 1317–1326. [Google Scholar] [CrossRef] [PubMed]
- Lacson, E.; Teng, M.; Ong, J.; Vienneau, L.; Ofsthun, N.; Lazarus, J.M. Antibody response to Engerix-B and Recombivax-HB hepatitis B vaccination in end-stage renal disease. Hemodial. Int. 2005, 9, 367–975. [Google Scholar] [CrossRef] [PubMed]
- Mulley, W.R.; Le, S.T.; Ives, K.E. Primary seroresponses to double-dose compared with standard-dose hepatitis B vaccination in patients with chronic kidney disease: A systematic review and meta-analysis. Nephrol. Dial. Transpl. 2017, 32, 136–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engel, A.L.; Sun, G.C.; Gad, E.; Rastetter, L.R.; Strobe, K.; Yang, Y.; Dang, Y.; Disis, M.L.; Lu, H. Protein-bound polysaccharide activates dendritic cells and enhances OVA-specific T cell response as vaccine adjuvant. Immunobiology 2013, 218, 1468–1476. [Google Scholar] [CrossRef] [Green Version]
- Grzegorzewska, A.E. Prophylactic vaccinations in chronic kidney disease: Current status. Hum. Vaccines Immunother. 2015, 11, 2599–2605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yousaf, F.; Gandham, S.; Galler, M.; Spinowitz, B.; Charytan, C. Systematic review of the efficacy and safety of intradermal versus intramuscular hepatitis B vaccination in end-stage renal disease population unresponsive to primary vaccination series. Ren. Fail. 2015, 37, 1080–1088. [Google Scholar] [PubMed]
- Hung, I.F.; Yap, D.Y.; Yip, T.P.; Zhang, R.R.; To, K.K.; Chan, K.H.; Tang, S.C.; Lui, S.L.; Levin, Y.; Kochba, E.; et al. A Double-blind, Randomized Phase 2 Controlled Trial of Intradermal Hepatitis B Vaccination With a Topical Toll-like Receptor 7 Agonist Imiquimod, in Patients on Dialysis. Clin. Infect. Dis. 2021, 73, e304–e311. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, M.; Shalchiantabrizi, P.; Dadgarmoghaddam, M.; Ahmady-Simab, S.; Behjati, A.; Salari, M. The Effect of Oral Levamisole Co-administration on the Level of Immune Response to Hepatitis B Vaccine in Healthy Individuals: A Randomized Clinical Trial. Iran J. Allergy Asthma Immunol. 2017, 16, 219–227. [Google Scholar] [PubMed]
- Kosmadakis, G.; Albaret, J.; Correia, E.D.C.; Somda, F.; Aguilera, D. Vaccination practices in dialysis patients: A narrative review. Semin. Dial. 2018, 31, 507–518. [Google Scholar] [CrossRef] [PubMed]
- Haddiya, I. Current Knowledge of Vaccinations in Chronic Kidney Disease Patients. Int. J. Nephrol. Renovasc. Dis. 2020, 13, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, F.; Ramezani, M.; Razeghi, E.; Ranjbarnovin, N.; Khazaeipour, Z. A randomized controlled trial of two schedules of hepatitis B vaccination in predialysed chronic renal failure patients. Hepat. Mon. 2012, 12, 344–348. [Google Scholar] [CrossRef] [Green Version]
- Fabrizi, F.; Cerutti, R.; Nardelli, L.; Tripodi, F.; Messa, P. HBV vaccination with Fendrix is effective and safe in pre-dialysis CKD population. Clin. Res. Hepatol. Gastroenterol. 2020, 44, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Makidon, P.E.; Smith, D.M.; Groom, J.V., II; Cao, Z.; Landers, J.J.; Baker, J.R., Jr. Effect of Chronic Uremia on the Cell Surface Expression of B7 Family Costimulatory Molecules in an HLA-A2 Transgenic Mouse Model of Chronic Kidney Disease. Comp. Med. 2015, 65, 308–314. [Google Scholar] [PubMed]
- Alavian, S.M.; Tabatabaei, S.V. The effect of diabetes mellitus on immunological response to hepatitis B virus vaccine in individuals with chronic kidney disease: A meta-analysis of current literature. Vaccine 2010, 28, 3773–3777. [Google Scholar] [CrossRef] [PubMed]
- Udomkarnjananun, S.; Takkavatakarn, K.; Praditpornsilpa, K.; Nader, C.; Eiam-Ong, S.; Jaber, B.L.; Susantitaphong, P. Hepatitis B virus vaccine immune response and mortality in dialysis patients: A meta-analysis. J. Nephrol. 2020, 33, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Zitt, E.; Sprenger-Mähr, H.; Knoll, F.; Neyer, U.; Lhotta, K. Vitamin D deficiency is associated with poor response to active hepatitis B immunisation in patients with chronic kidney disease. Vaccine 2012, 30, 931–935. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Converters N = 16 | Non-Converters N = 21 | p-Value |
|---|---|---|---|
| Age–Median (25th, 75th) | 69 (58, 75) | 71 (69, 77) | 0.1203 |
| GFR–Median (25th, 75th) | 18.5 (15, 23) | 24 (16, 25) | 0.2070 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hettenbaugh, J.; Mullane, R.; Gillispie, G.; Shostrom, V.; Flores, L.; Fillaus, J.A.; Florescu, M.C.; Murcek, D.; Tendulkar, K.K. Hepatitis B Vaccination in Advanced Chronic Kidney Disease: A Quality Improvement Project at a Veteran Affairs Chronic Kidney Disease Clinic. Infect. Dis. Rep. 2021, 13, 1036-1042. https://doi.org/10.3390/idr13040094
Hettenbaugh J, Mullane R, Gillispie G, Shostrom V, Flores L, Fillaus JA, Florescu MC, Murcek D, Tendulkar KK. Hepatitis B Vaccination in Advanced Chronic Kidney Disease: A Quality Improvement Project at a Veteran Affairs Chronic Kidney Disease Clinic. Infectious Disease Reports. 2021; 13(4):1036-1042. https://doi.org/10.3390/idr13040094
Chicago/Turabian StyleHettenbaugh, Jacob, Ryan Mullane, Gayle Gillispie, Valerie Shostrom, Linda Flores, Jennifer A. Fillaus, Marius C. Florescu, Denise Murcek, and Ketki K. Tendulkar. 2021. "Hepatitis B Vaccination in Advanced Chronic Kidney Disease: A Quality Improvement Project at a Veteran Affairs Chronic Kidney Disease Clinic" Infectious Disease Reports 13, no. 4: 1036-1042. https://doi.org/10.3390/idr13040094