
Terlipressin for the Prevention and Treatment of Renal Decline in Hepatorenal Syndrome: A Drug Profile

Abstract
:1. Introduction
2. Treatment of Hepatorenal Syndrome
3. Vasopressin: Background
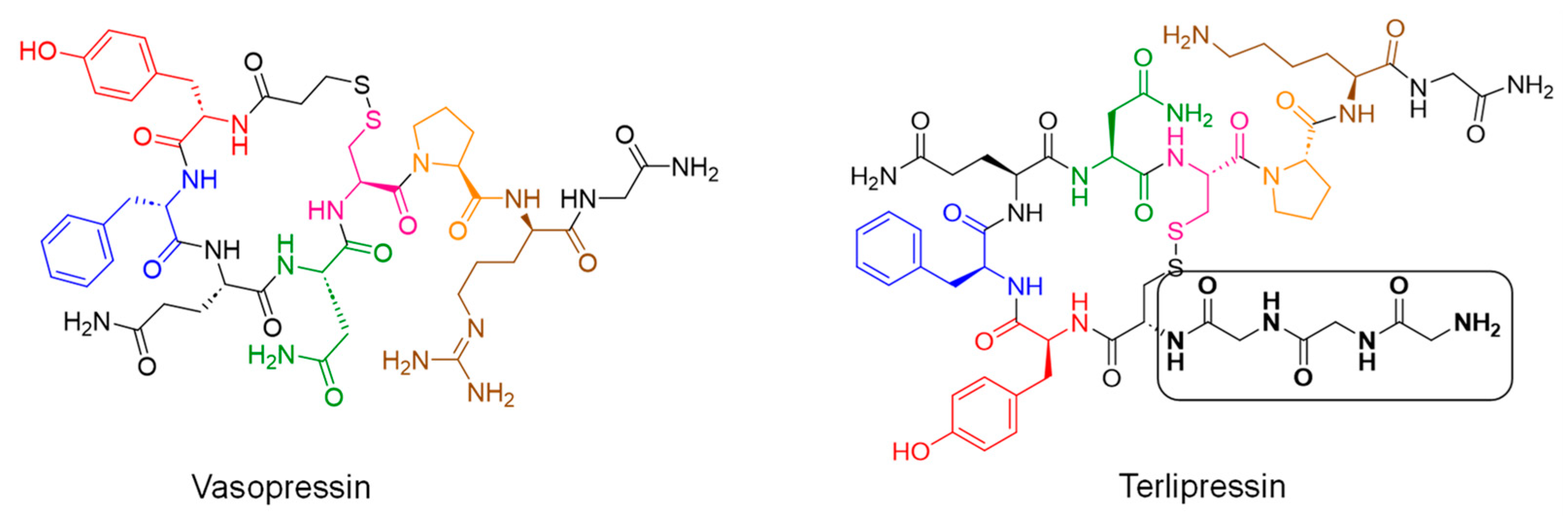
4. Terlipressin: Chemistry
5. Terlipressin: Mechanism of Action
6. Terlipressin: Pharmacokinetics
7. Terlipressin: Clinical Trials
8. Terlipressin: Tolerability and Pharmacovigilance
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ginès, P.; Schrier, R.W. Renal failure in cirrhosis. N. Engl. J. Med. 2009, 361, 1279–1290. [Google Scholar] [CrossRef] [PubMed]
- Ginès, P.; Guevara, M.; Arroyo, V.; Rodés, J. Hepatorenal syndrome. Lancet 2003, 362, 1819–1827. [Google Scholar] [CrossRef] [PubMed]
- Wadei, H.M.; Mai, M.L.; Ahsan, N.; Gonwa, T.A. Hepatorenal syndrome: Pathophysiology and management. Clin. J. Am. Soc. Nephrol. 2006, 1, 1066–1079. [Google Scholar] [CrossRef] [PubMed]
- Mindikoglu, A.L.; Pappas, S.C. New Developments in Hepatorenal Syndrome. Clin. Gastroenterol. Hepatol. 2018, 16, 162–177.e1. [Google Scholar] [CrossRef] [PubMed]
- Ginès, A.; Escorsell, A.; Ginès, P.; Saló, J.; Jiménez, W.; Inglada, L.; Navasa, M.; Clària, J.; Rimola, A.; Arroyo, V.; et al. Incidence, predictive factors, and prognosis of the hepatorenal syndrome in cirrhosis with ascites. Gastroenterology 1993, 105, 229–236. [Google Scholar] [CrossRef]
- Akriviadis, E.; Botla, R.; Briggs, W.; Han, S.; Reynolds, T.; Shakil, O. Pentoxifylline improves short-term survival in severe acute alcoholic hepatitis: A double-blind, placebo-controlled trial. Gastroenterology 2000, 119, 1637–1648. [Google Scholar] [CrossRef]
- Arroyo, V.; Gines, P.; Gerbes, A.L.; Dudley, F.J.; Gentilini, P.; Laffi, G.; Reynolds, T.B.; Ring-Larsen, H.; Schölmerich, J. Definition and diagnostic criteria of refractory ascites and hepatorenal syndrome in cirrhosis. International Ascites Club. Hepatology 1996, 23, 164–176. [Google Scholar] [CrossRef]
- Baldus, W.P.; Feicher, R.N.; Summerskill, W.H. The kidney in cirrhosis: I. Clinical and biochemical features of azotemia in hepatic failure. Ann. Intern. Med. 1964, 60, 353–365. [Google Scholar] [CrossRef]
- Esrailian, E.; Pantangco, E.R.; Kyulo, N.L.; Hu, K.Q.; Runyon, B.A. Octreotide/Midodrine therapy significantly improves renal function and 30-day survival in patients with type 1 hepatorenal syndrome. Dig. Dis. Sci. 2007, 52, 742–748. [Google Scholar] [CrossRef]
- Salerno, F.; Gerbes, A.; Ginès, P.; Wong, F.; Arroyo, V. Diagnosis, prevention and treatment of hepatorenal syndrome in cirrhosis. Gut 2007, 56, 1310–1318. [Google Scholar] [CrossRef]
- Biggins, S.W.; Angeli, P.; Garcia-Tsao, G.; Ginès, P.; Ling, S.C.; Nadim, M.K.; Wong, F.; Kim, W.R. Diagnosis, Evaluation, and Management of Ascites, Spontaneous Bacterial Peritonitis and Hepatorenal Syndrome: 2021 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2021, 74, 1014–1048. [Google Scholar] [CrossRef]
- Subedi, A.; Suresh Kumar, V.C.; Sharma Subedi, A.; Sapkota, B. A Review of Hepatorenal Syndrome. Cureus 2021, 13, e16084. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.S.; Tan, J.C.; Kim, W.R. Management of renal failure in end-stage liver disease: A critical appraisal. Liver Transpl. 2016, 22, 1710–1719. [Google Scholar] [CrossRef] [PubMed]
- Amini, M.; Runyon, B.A. Alcoholic hepatitis 2010: A clinician’s guide to diagnosis and therapy. World J. Gastroenterol. 2010, 16, 4905–4912. [Google Scholar] [CrossRef] [PubMed]
- Garg, H.; Sarin, S.K.; Kumar, M.; Garg, V.; Sharma, B.C.; Kumar, A. Tenofovir improves the outcome in patients with spontaneous reactivation of hepatitis B presenting as acute-on-chronic liver failure. Hepatology 2011, 53, 774–780. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Linganna, M. Diagnosis and management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome. Cleve Clin J Med. 2023, 90, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Kam, P.C.; Williams, S.; Yoong, F.F. Vasopressin and terlipressin: Pharmacology and its clinical relevance. Anaesthesia 2004, 59, 993–1001. [Google Scholar] [CrossRef]
- Kulkarni, A.V.; Arab, J.P.; Premkumar, M.; Benitez, C.; Tirumalige Ravikumar, S.; Kumar, P.; Sharma, M.; Reddy, D.N.; Simonetto, D.A.; Rao, P.N. Terlipressin has stood the test of time: Clinical overview in 2020 and future perspectives. Liver Int. 2020, 40, 2888–2905. [Google Scholar] [CrossRef]
- Anonymous. Terlipressin Acetate. Am. J. Health Syst. Pharm. 2023, 80, e10–e11. [Google Scholar] [CrossRef]
- Ryan, L.; Attridge, R.L.; Moote, R.; Miller, M.L. Chapter 9. Portal Hypertension and Cirrhosis. In Internal Medicine: A Guide to Clinical Therapeutics; Attridge, R.L., Miller, M.L., Moote, R., Ryan, L., Eds.; McGraw Hill: New York, NY, USA, 2013; Available online: https://accesspharmacy.mhmedical.com/Content.aspx?bookid=565§ionid=42003718 (accessed on 4 August 2023).
- Mukhtar, N.A.; Khalili, M. Liver Disease. In Pathophysiology of Disease: An Introduction to Clinical Medicine, 8th ed.; Hammer, G.D., McPhee, S.J., Eds.; McGraw Hill: New York, NY, USA, 2019; Available online: https://accesspharmacy.mhmedical.com/content.aspx?bookid=2468§ionid=198222693 (accessed on 4 August 2023).
- Boone, M.; Deen, P.M. Physiology and pathophysiology of the vasopressin-regulated renal water reabsorption. Pflugers Arch. 2008, 456, 1005–1024. [Google Scholar] [CrossRef]
- Matok, I.; Vard, A.; Efrati, O.; Rubinshtein, M.; Vishne, T.; Leibovitch, L.; Adam, M.; Barzilay, Z.; Paret, G. Terlipressin as rescue therapy for intractable hypotension due to septic shock in children. Shock 2005, 23, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Pesaturo, A.B.; Jennings, H.R.; Voils, S.A. Terlipressin: Vasopressin analog and novel drug for septic shock. Ann. Pharmacother. 2006, 40, 2170–2177. [Google Scholar] [CrossRef] [PubMed]
- The U.S. Food and Drug Administration Label for TERLIVAZ (Terlipressin) for Injection, for Intravenous Use. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/022231s000lbl.pdf (accessed on 24 November 2022).
- Klein, M.; Weksler, N.; Borer, A.; Koyfman, L.; Kesslin, J.; Gurman, G.M. Terlipressin facilitates transport of septic patients treated with norepinephrine. Isr. Med. Assoc. J. 2006, 8, 691–693. [Google Scholar]
- Sanyal, A.J.; Boyer, T.; Garcia–Tsao, G.; Regenstein, F.; Rossaro, L.; Appenrodt, B.; Blei, A.; Gülberg, V.; Sigal, S.; Teuber, P. A randomized, prospective, double-blind, placebo-controlled trial of terlipressin for type 1 hepatorenal syndrome. Gastroenterology 2008, 134, 1360–1368. [Google Scholar] [CrossRef]
- Wong, F.; Pappas, S.C.; Curry, M.P.; Reddy, K.R.; Rubin, R.A.; Porayko, M.K.; Gonzalez, S.A.; Mumtaz, K.; Lim, N.; Simonetto, D.A.; et al. Terlipressin plus Albumin for the Treatment of Type 1 Hepatorenal Syndrome. N. Engl. J. Med. 2021, 384, 818–828. [Google Scholar] [CrossRef] [PubMed]
- Narahara, Y.; Kanazawa, H.; Sakamoto, C.; Maruyama, H.; Yokosuka, O.; Mochida, S.; Uemura, M.; Fukui, H.; Sumino, Y.; Matsuzaki, Y.; et al. The efficacy and safety of terlipressin and albumin in patients with type 1 hepatorenal syndrome: A multicenter, open-label, explorative study. J. Gastroenterol. 2012, 47, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Terlivaz® (Terlipressin) for Injection Prescribing Information. Available online: https://www.terlivaz.com/assets/pdf/Terlivaz-USPI_04_2023.pdf (accessed on 4 August 2023).
- Piano, S.; Gambino, C.; Vettore, E.; Calvino, V.; Tonon, M.; Boccagni, P.; Gringeri, E.; Germani, G.; Burra, P.; Cillo, U.; et al. Response to Terlipressin and Albumin Is Associated with Improved Liver Transplant Outcomes in Patients with Hepatorenal Syndrome. Hepatology 2021, 73, 1909–1919. [Google Scholar] [CrossRef]
- Moreau, R.; Durand, F.; Poynard, T.; Duhamel, C.; Cervoni, J.; Ichaï, P.; Abergel, A.; Halimi, C.; Pauwels, M.; Bronowicki, J.; et al. Terlipressin in patients with cirrhosis and type 1 hepatorenal syndrome: A retrospective multicenter study. Gastroenterology 2002, 122, 923–930. [Google Scholar] [CrossRef]
- Solanki, P.; Chawla, A.; Garg, R.; Gupta, R.; Jain, M.; Sarin, S.K. Beneficial effects of terlipressin in hepatorenal syndrome: A prospective, randomised placebo-controlled clinical trial. J. Gastroenterol. Hepatol. 2003, 18, 152–156. [Google Scholar] [CrossRef]
- Neri, S.; Pulvirenti, D.; Malaguarnera, M.; Cosimo, B.M.; Bertino, G.; Ignaccolo, L.; Siringo, S.; Castellino, P. Terlipressin and albumin in patients with cirrhosis and type I hepatorenal syndrome. Dig. Dis. Sci. 2008, 53, 830–835. [Google Scholar] [CrossRef]
- Sharma, P.; Kumar, A.; Shrama, B.C.; Sarin, S.K. An open label, pilot, randomised controlled trial of noradrenaline versus terlipressin in the treatment of type 1 hepatorenal syndrome and predictors of response. Am. J. Gastroenterol. 2008, 103, 1689–1697. [Google Scholar] [CrossRef] [PubMed]
- Nazar, A.; Pereira, G.H.; Guevara, M.; Martín-Llahi, M.; Pepin, M.-N.; Marinelli, M.; Solá, E.; Baccaro, M.E.; Terra, C.; Arroyo, V.; et al. Predictors of response to therapy with terlipressin and albumin in patients with cirrhosis and type 1 hepatorenal syndrome. Hepatology 2010, 51, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.; Ghosh, S.; Singh, B.; Kumar, P.; Sharma, N.; Bhalla, A.; Sharma, A.K.; Choudhary, N.S.; Chawla, Y.; Nain, C.K. Noradrenaline vs. terlipressin in the treatment of hepatorenal syndrome: A randomised study. J. Hepatol. 2012, 56, 1293–1298. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Choudhary, N.S.; Sharma, A.K.; Singh, B.; Kumar, P.; Agarwal, R.; Sharma, N.; Bhalla, A.; Chawla, Y.K.; Singh, V. Noradrenaline vs. terlipressin in the treatment of type 2 hepatorenal syndrome: A randomised pilot study. Liver Int. 2013, 33, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Cavallin, M.; Kamath, P.S.; Merli, M.; Fasolato, S.; Toniutto, P.; Salerno, F.; Bernardi, M.; Romanelli, R.G.; Colletta, C.; Salinas, F.; et al. Terlipressin plus albumin versus midodrine and octreotide plus albumin in the treatment of hepatorenal syndrome: A randomised trial. Hepatology 2015, 62, 567–574. [Google Scholar] [CrossRef]
- Goyal, O.; Sidhu, S.S.; Sehgal, N.; Puri, S. Noradrenaline is as effective as terlipressin in hepatorenal syndrome type 1: A prospective randomised trial. J. Assoc. Physicians India. 2016, 64, 30–35. [Google Scholar] [PubMed]
- Sanyal, A.J.; Boyer, T.D.; Frederick, R.T.; Wong, F.; Rossaro, L.; Araya, V.; Vargas, H.E.; Reddy, K.R.; Pappas, S.C.; Teuber, P.; et al. Reversal of hepatorenal syndrome type 1 with terlipressin plus albumin vs. placebo plus albumin in a pooled analysis of the OT-0401 and REVERSE randomised clinical studies. Aliment. Pharmacol. Ther. 2017, 45, 1390–1402. [Google Scholar] [CrossRef]
- Saif, R.U.; Dar, H.A.; Sofi, S.M.; Andrabi, M.S.; Javid, G.; Zargar, S.A. Noradrenaline versus terlipressin in the management of type 1 hepatorenal syndrome: A randomised controlled study. Indian. J. Gastroenterol. 2018, 37, 424–429. [Google Scholar] [CrossRef]
- Uriz, J.; Ginès, P.; Cárdenas, A.; Sort, P.; Jiménez, W.; Salmerón, J.M.; Bataller, R.; Mas, A.; Navasa, M.; Arroyo, V.; et al. Terlipressin plus albumin infusion: An effective and safe therapy of hepatorenal syndrome. J. Hepatol. 2000, 33, 43–48. [Google Scholar] [CrossRef]
- Ortega, R.; Gines, P.; Uriz, J.; Cárdenas, A.; Calahorra, B.; De Las Heras, D.; Guevara, M.; Bataller, R.; Jiménez, W.; Arroyo, V.; et al. Terlipressin therapy with and without albumin for patients with hepatorenal syndrome: Results of a prospective, nonrandomised study. Hepatology 2002, 36 Pt 1, 941–948. [Google Scholar]
- Alessandria, C.; Ottobrelli, A.; Debernardi-Venon, W.; Todros, L.; Cerenzia, M.T.; Martini, S.; Balzola, F.; Morgando, A.; Rizzetto, M.; Marzano, A. Noradrenalin vs. terlipressin in patients with hepatorenal syndrome: A prospective, randomised, unblinded, pilot study. J. Hepatol. 2007, 47, 499–505. [Google Scholar] [CrossRef]
- Martín-Llahí, M.; Pépin, M.N.; Guevara, M.; Díaz, F.; Torre, A.; Monescillo, A.; Soriano, G.; Terra, C.; Fábrega, E.; Arroyo, V.; et al. Terlipressin and albumin vs. albumin in patients with cirrhosis and hepatorenal syndrome: A randomised study. Gastroenterology 2008, 134, 1352–1359. [Google Scholar] [CrossRef]
- Nguyen-Tat, M.; Jäger, J.; Rey, J.W.; Nagel, M.; Labenz, C.; Wörns, M.-A.; Galle, P.R.; Marquardt, J.U. Terlipressin and albumin combination treatment in patients with hepatorenal syndrome type 2. United Eur. Gastroenterol. J. 2019, 7, 529–537. [Google Scholar] [CrossRef]
- Wong, F.; Curry, M.P.; Reddy, K.R.; Rubin, R.A.; Porayko, M.K.; Gonzalez, S.A.; Mumtaz, K.; Lim, N.; Simonetto, D.A.; Sharma, P.; et al. The CONFIRM study: A North American randomised controlled trial (RCT) of terlipressin plus albumin for the treatment of hepatorenal syndrome type 1 (HRS-1). Hepatology 2019, 70, 1480A–1481A. [Google Scholar]
- Moore, K.; Jamil, K.; Verleger, K.; Luo, L.; Kebede, N.; Heisen, M.; Corman, S.; Leonardi, R.; Bakker, R.; Maï, C.; et al. Real-world treatment patterns and outcomes using terlipressin in 203 patients with the hepatorenal syndrome. Aliment. Pharmacol. Ther. 2020, 52, 351–358. [Google Scholar] [CrossRef]
- Sridharan, K.; Sivaramakrishnan, G. Vasoactive agents for hepatorenal syndrome: A mixed treatment comparison network meta-analysis and trial sequential analysis of randomized clinical trials. J. Gen. Intern. Med. 2018, 33, 97–102. [Google Scholar] [CrossRef]
- Best, L.M.; Freeman, S.C.; Sutton, A.J.; Cooper, N.J.; Tng, E.L.; Csenar, M.; Hawkins, N.; Pavlov, C.S.; Davidson, B.R.; Thorburn, D.; et al. Treatment for hepatorenal syndrome in people with decompensated liver cirrhosis: A network meta-analysis. Cochrane Database Syst. Rev. 2019, 9, CD013103. [Google Scholar] [CrossRef]
- Nanchal, R.S.; Warrillow, S. Terlipressin: Leading the Water to the Thirsty. Crit. Care Med. 2022, 50, 1533–1535. [Google Scholar] [CrossRef]
- Rodríguez, E.; Elia, C.; Solà, E.; Barreto, R.; Graupera, I.; Andrealli, A.; Pereira, G.; Poca, M.; Sánchez, J.; Guevara, M.; et al. Terlipressin and albumin for type-1 hepatorenal syndrome associated with sepsis. J. Hepatol. 2014, 60, 955–961. [Google Scholar] [CrossRef]
- Belcher, J.M. Good Enough? Terlipressin, Hepatorenal Syndrome, and the Usage of RRT. Kidney360 2023, 4, 1011–1013. [Google Scholar] [CrossRef]
- Carter, J.A.; Huang, X.; Jamil, K.; Corman, S.; Ektare, V.; Niewoehner, J. Cost-effectiveness of terlipressin for hepatorenal syndrome: The United States hospital perspective. J. Med. Econ. 2023, 1–19. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study No. of Participants | Dose of Terlipressin | Comparator | Reversal and Survival Benefit with Terlipressin | Ref. |
|---|---|---|---|---|
| HRS-AKI | ||||
| Moreau R et al. (2002), N = 99 | 3.2 ± 1.3 mg/day infusion | None | 64% reversal | [32] |
| Solanki P et al. (2003), N = 12 in each group | 1 mg every 12 h | Placebo | 41.67% reversal and survival benefit on day 15 | [33] |
| Neri S et al. (2008), N = 26 in each group | 1 mg every 8 h for 5 days, then 0.5 mg every 8 h for 2 weeks with albumin | Albumin | 80% reversal (vs. 19%) | [34] |
| Sharma P et al. (2008), N = 20 in each group | 0.5 mg every 6 h. increasing every third day (in case of no response) to 2 mg every 6 h | Noradrenaline/albumin | 50% reversal in each group Survival was similar on day 15 | [35] |
| Nazar A et al. (2010), N = 39 | 0.5 to 1 mg every 4 h for 3 days. The dose increased to 2 mg every 4 h with albumin if sCr had not decreased >25% | None | 46% reversal | [36] |
| Singh V et al. (2012), N = 23 in each group | 0.5 mg every 6 h. increasing every third day (in case of no response) to 2 mg every 6 h | Noradrenaline/albumin | 39% reversal (vs. 43.4%) Survival was similar in both groups | [37] |
| Ghosh S et al. (2013), N = 23 in each group | 0.5 mg every 6 h, increasing every third day when no response achieved to 2 mg every 6 h with albumin | Noradrenaline/albumin | 74% reversal (vs. 74%) No survival benefit | [38] |
| Cavallin M et al. (2015), N = 27 in terlipressin and 22 in the other group | 3 mg infusion for 24 h, increased to 12 mg over 24 h if no response achieved with albumin | Midodrine/octreotide/ albumin | 70.4% reversal (vs. 28.6%) No survival benefits | [39] |
| Goyal O et al. (2016), N = 41 | 0.5–2 mg every 6 h with albumin | Noradrenaline/albumin | 45% reversal (vs. 47.6%) | [40] |
| Sanyal A et al. (2017), N = 308 patients (terlipressin = 153; placebo = 155) | 1 mg every 6 h. Dose doubled to 2 mg every 6 h when no significant improvement achieved | Placebo | 27% reversal (vs. 14%) Survival benefit on day 90 | [41] |
| Saif RU et al. (2018), N = 30 in each group | 0.5 mg every 6 h with maximum dose of 4 mg every 6 h with albumin | Noradrenaline/albumin | 57% reversal (vs. 53%) No survival benefit | [42] |
| Wong F et al. (2021), N = 300 (199 were assigned to the terlipressin + albumin group and 101 to the placebo + albumin group) | 1 mg of terlipressin was administered IV every 5.5 to 6.5 h. Patient could receive up to 2 mg every 6 h on day 4 if no sufficient response achieved | Placebo/albumin | (1) 32% verified reversal (vs. 17%) (2) Reversal without renal replacement therapy by day 30 was 34% (vs. 17%) (3) Reversal among patients with systemic inflammatory response syndrome was 37% (vs. 6%) (4) 26% verified reversal (vs. 17%) without recurrence by day 30 (5) At day 90, liver transplantations had been performed in 23% (vs. 29%) and death occurred in 51% (vs. 45%) | [28] |
| HRS-AKI and HRS-NAKI | ||||
| Uriz J et al. (2000), N = 9 | 0.5 mg every 4 h. Increased every third day to 1 mg every 4 h and 2 mg every 4 h if no adequate response | None | 78% reversal | [43] |
| Ortega R et al. (2002), N = 21 patients (five were HRS-NAKI) | 0.5–2 mg every 4 h with albumin | None | 57% reversal (vs. 10%) | [44] |
| Alessandria C et al. (2007), N = 22 (12 in terlipressin group) | 1–2 mg every four hours | Noradrenaline/albumin | 83% reversal (vs. 70%) No survival benefit | [45] |
| Martin-Llahi M et al. (2008), N = 23 in each group | 1 mg every 4 h for 3 days. If no adequate response, the dose was increased to 2 mg every 4 h | Albumin | 43.5% reversal (vs. 8.7%) No survival benefit at day 90 | [46] |
| Nguyen-Tat M et al. (2019), N = 106 | 4 mg/day IV infusion | None | 46–48% reversal | [47] |
| Adverse Event | Placebo % | Terlipressin % |
|---|---|---|
| Abdominal pain | 6.1 | 19.5 |
| Nausea | 10.1 | 16.0 |
| Respiratory failure | 7.1 | 15.5 |
| Diarrhea | 7.1 | 13.0 |
| Dyspnea | 5.1 | 12.5 |
| Fluid overload | 3.0 | 8.5 |
| Pleural effusion | 0 | 5.5 |
| Sepsis | 1.0 | 5.5 |
| Bradycardia | 0 | 5.0 |
| Ischemia-related events (skin discoloration, cyanosis, ischemia, and intestinal ischemia) | 0 | 4.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayyad, A.; Al-Horani, R.A. Terlipressin for the Prevention and Treatment of Renal Decline in Hepatorenal Syndrome: A Drug Profile. Gastroenterol. Insights 2023, 14, 420-430. https://doi.org/10.3390/gastroent14040031
Ayyad A, Al-Horani RA. Terlipressin for the Prevention and Treatment of Renal Decline in Hepatorenal Syndrome: A Drug Profile. Gastroenterology Insights. 2023; 14(4):420-430. https://doi.org/10.3390/gastroent14040031
Chicago/Turabian StyleAyyad, Ahlam, and Rami A. Al-Horani. 2023. "Terlipressin for the Prevention and Treatment of Renal Decline in Hepatorenal Syndrome: A Drug Profile" Gastroenterology Insights 14, no. 4: 420-430. https://doi.org/10.3390/gastroent14040031