
Blood-Based Non-Invasive Tests of Hepatic Fibrosis in Autoimmune Hepatitis: Application among Selected Patients Leads to Higher Accuracy
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Autoimmune hepatitis. J. Hepatol. 2015, 63, 971–1004.
- Muratori, P.; Carbone, M.; Stangos, G.; Perini, L.; Lalanne, C.; Ronca, V.; Cazzagon, N.; Bianchi, G.; Lenzi, M.; Floreani, A.; et al. Clinical and prognostic implications of acute onset of Autoimmune Hepatitis: An Italian multicentre study. Dig. Liver Dis. 2018, 50, 698–702. [Google Scholar] [CrossRef] [PubMed]
- West, J.; Card, T.R. Reduced mortality rates following elective percutaneous liver biopsies. Gastroenterology 2010, 139, 1230–1237. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Liu, D.; Cui, J.; Sha, Y.; Zhou, H.; Tang, N.; Wang, N.; Huang, A.; Xia, J. Diagnostic accuracy of red blood cell distribution width to platelet ratio for predicting staging liver fibrosis in chronic liver disease patients: A systematic review and meta-analysis. Medicine 2019, 98, e15096. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Yang, Z.; Zhou, J.; Zeng, N.; He, Z.; Zhan, S.; Jia, J.; You, H. Systematic review: Diagnostic accuracy of non-invasive tests for staging liver fibrosis in autoimmune hepatitis. Hepatol. Int. 2019, 13, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Sheng, L.; Bao, H.; Chen, X.; Guo, C.; Li, H.; Ma, X.; Qiu, D.; Hua, J. Evaluation of transient elastography in assessing liver fibrosis in patients with autoimmune hepatitis. J. Gastroenterol. Hepatol. 2017, 32, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Yada, N.; Sakurai, T.; Minami, T.; Arizumi, T.; Takita, M.; Hagiwara, S.; Ida, H.; Ueshima, K.; Nishida, N.; Kudo, M. Influence of Liver Inflammation on Liver Stiffness Measurement in Patients with Autoimmune Hepatitis Evaluation by Combinational Elastography. Oncology 2017, 92 (Suppl. S1), 10–15. [Google Scholar] [CrossRef] [PubMed]
- Swets, J.A. Measuring the accuracy of diagnostic systems. Science 1988, 240, 1285–1293. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver; List of panel members (alphabetical order); Berzigotti, A.; Boursier, J.; Castera, L.; Cazzagon, N.; Friedrich-Rust, M.; Petta, S.; Thiele, M.; Tsochatzis, E. Easl Clinical Practice Guidelines (Cpgs) On Non-Invasive Tests For Evaluation Of Liver Disease Severity And Prognosis-2020 Update. J. Hepatol. 2021; 3, 659–689. [Google Scholar]
- Montano-Loza, A.J.; Thandassery, R.B.; Czaja, A.J. Targeting Hepatic Fibrosis in Autoimmune Hepatitis. Dig. Dis. Sci. 2016, 61, 3118–3139. [Google Scholar] [PubMed]
- Hartl, J.; Ehlken, H.; Sebode, M.; Peiseler, M.; Krech, T.; Zenouzi, R.; von Felden, J.; Weiler-Normann, C.; Schramm, C.; Lohse, A.W. Usefulness of biochemical remission and transient elastography in monitoring disease course in autoimmune hepatitis. J. Hepatol. 2018, 68, 754–763. [Google Scholar] [CrossRef] [PubMed]
- Hartl, J.; Denzer, U.; Ehlken, H.; Zenouzi, R.; Peiseler, M.; Sebode, M.; Hübener, S.; Pannicke, N.; Weiler-Normann, C.; Quaas, A.; et al. Transient elastography in autoimmune hepatitis: Timing determines the impact of inflammation and fibrosis. J. Hepatol. 2016, 65, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Xiao, G.; Yang, J.; Yan, L. Comparison of diagnostic accuracy of aspartate aminotransferase to platelet ratio index and fibrosis-4 index for detecting liver fibrosis in adult patients with chronic hepatitis B virus infection: A systemic review and meta-analysis. Hepatology 2015, 61, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Vilar-Gomez, E.; Chalasani, N. Non-invasive assessment of non-alcoholic fatty liver disease: Clinical prediction rules and blood-based biomarkers. J. Hepatol. 2018, 68, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.S.; Yamada, G.; Vuppalanchi, R.; Van Natta, M.; Loomba, R.; Guy, C.; Brandman, D.; Tonascia, J.; Chalasani, N.; Neuschwander-Tetri, B.; et al. NASH Clinical Research Network. Diagnostic Accuracy of Noninvasive Fibrosis Models to Detect Change in Fibrosis Stage. Clin. Gastroenterol. Hepatol. 2019, 17, 1877–1885.e5. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, A.C.; El-Bacha, I.; Vianna, M.V.; Parise, E.R. Utility and limitations of APRI and FIB4 to predict staging in a cohort of nonselected outpatients with hepatitis C. Ann. Hepatol. 2016, 15, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Zheng, L.; Hu, L.; Zhou, H.; Yu, L.; Liang, W. Transient Elastography (FibroScan) Performs Better Than Non-Invasive Markers in Assessing Liver Fibrosis and Cirrhosis in Autoimmune Hepatitis Patients. Med. Sci. Monit. 2017, 23, 5106–5112. [Google Scholar] [CrossRef] [PubMed]
- Sheptulina, A.; Shirokova, E.; Nekrasova, T.; Blum, H.; Ivashkin, V. Platelet count to spleen diameter ratio non-invasively identifies severe fibrosis and cirrhosis in patients with autoimmune hepatitis. J. Gastroenterol. Hepatol. 2016, 31, 1956–1962. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Cao, J.; Zhong, Z.; Guo, Z.; Jiang, Y.; Bai, Y.; Xu, J. Noninvasive indicators predict advanced liver fibrosis in autoimmune hepatitis patients. J. Clin. Lab. Anal. 2019, 33, e22922. [Google Scholar] [CrossRef] [PubMed]
- Kruger, F.C.; Daniels, C.R.; Kidd, M.; Swart, G.; Brundyn, K.; van Rensburg, C.; Kotze, M. APRI: A simple bedside marker for advanced fibrosis that can avoid liver biopsy in patients with NAFLD/NASH. South Afr. Med. J. 2011, 101, 477–480. [Google Scholar]
- Boursier, J.; de Ledinghen, V.; Zarski, J.P.; Rousselet, M.C.; Sturm, N.; Foucher, J.; Leroy, V.; Fouchard-Hubert, I.; Bertrais, S.; Gallois, Y.; et al. A new combination of blood test and fibroscan for accurate non-invasive diagnosis of liver fibrosis stages in chronic hepatitis C. Am. J. Gastroenterol. 2011, 106, 1255–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Missing | Ishak 0–3 | Ishak ≥ 4 | p-Value | |
|---|---|---|---|---|
| (n = 95) | (n = 27) | |||
| Age | 0 | 47.0 (31.0–57.5) | 57.0 (42.0–60.5) | 0.099 |
| WBC | 16 | 5.90 (5.05–7.60) | 5.46 (4.37–6.78) | 0.127 |
| Neutrophil | 20 | 3.14 (2.59–4.05) | 2.63 (2.05–3.82) | 0.095 |
| Lymphocyte | 20 | 1.95 (1.50–2.54) | 2.05 (1.49–2.39) | 0.684 |
| RBC | 18 | 4.60 (4.23–4.87) | 4.50 (4.24–4.87) | 0.846 |
| Hb | 16 | 13.40 (12.60–14.50) | 12.90 (12.10–14.20) | 0.279 |
| MCV | 21 | 89.00 (84.78–91.83) | 88.10 (85.80–91.00) | 0.962 |
| PC | 17 | 245.50 (187.00–290.00) | 177.00 (130.00–222.00) | <0.001 |
| RDW | 40 | 13.90 (13.40–15.00) | 14.10 (13.90–16.75) | 0.027 |
| MPV | 46 | 9.20 (8.20–11.00) | 9.60 (8.85–10.70) | 0.579 |
| AST | 2 | 254.00 (95.00–739.00) | 488.00 (279.00–982.50) | 0.044 |
| AST/ULN | 2 | 7.00 (2.70–20.10) | 13.00 (7.50–23.70) | 0.077 |
| ALT | 2 | 434.00 (124.00–962.00) | 650.00 (317.50–986.00) | 0.341 |
| ALT/ULN | 2 | 11.22 (3.00–27.00) | 14.00 (8.15–23.90) | 0.704 |
| GGT | 9 | 79.50 (29.75–137.00) | 151.00 (68.00–190.00) | 0.014 |
| ALP | 14 | 132.50 (81.25–219.25) | 172.00 (127.25–238.25) | 0.165 |
| Albumin | 14 | 40.00 (36.85–42.00) | 36.00 (34.53–39.00) | 0.003 |
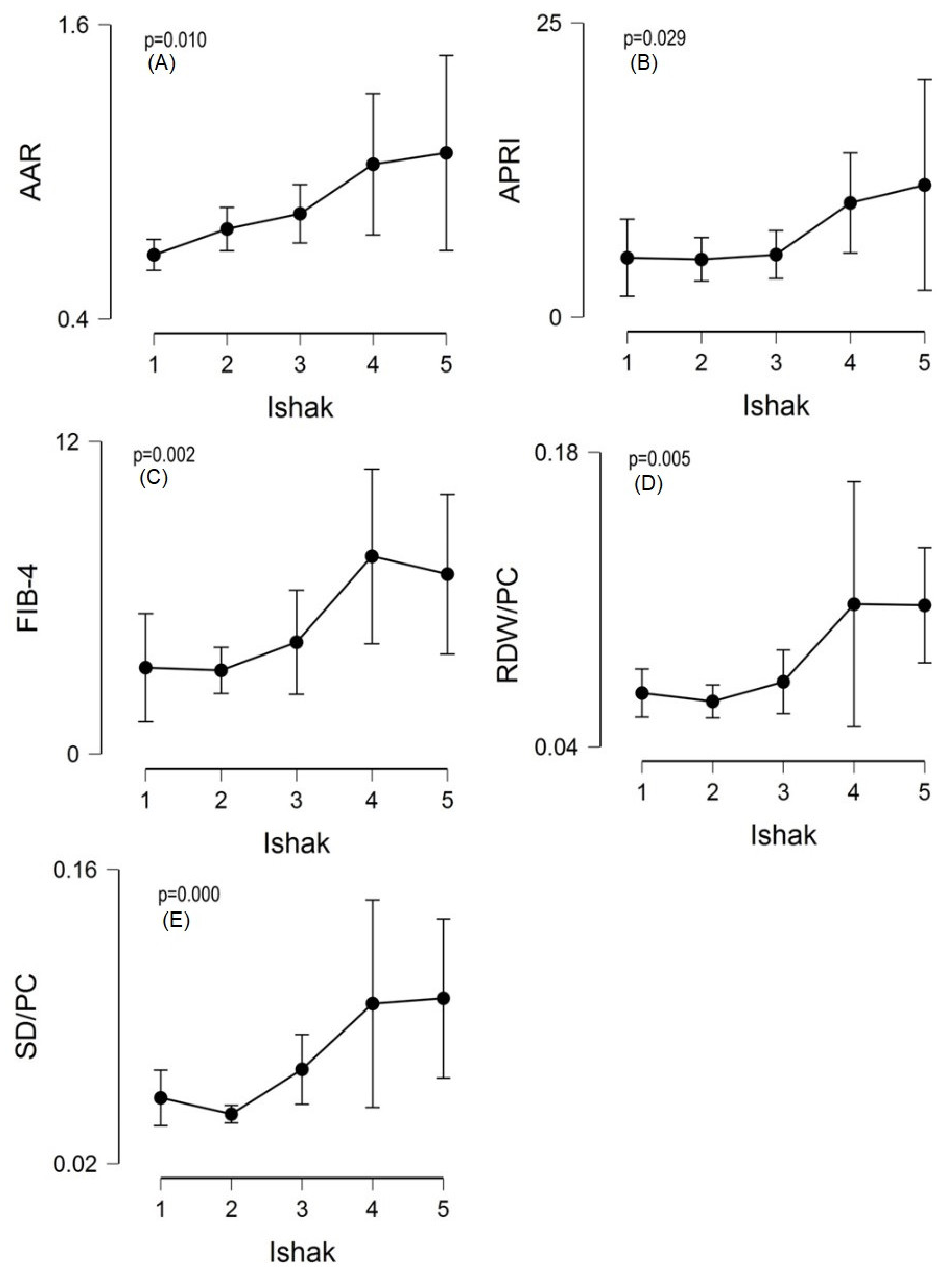
| SD | 21 | 11.00 (10.00–12.50) | 13.80 (12.70–14.53) | <0.001 |
| FIB–4 | 17 | 2.21 (1.21–4.53) | 6.17 (3.32–11.03) | <0.001 |
| APRI | 17 | 0.04 (0.01–0.11) | 0.11 (0.05–0.12) | 0.002 |
| AAR | 17 | 0.70 (0.59–0.89) | 0.97 (0.71–1.24) | 0.002 |
| RDW/PC | 20 | 0.06 (0.05–0.08) | 0.09 (0.06–0.13) | <0.001 |
| SD/PC | 29 | 0.04 (0.04–0.06) | 0.08 (0.06–0.10) | <0.001 |
| Test | Population | AUC | 95% CI | Z | p-Value |
|---|---|---|---|---|---|
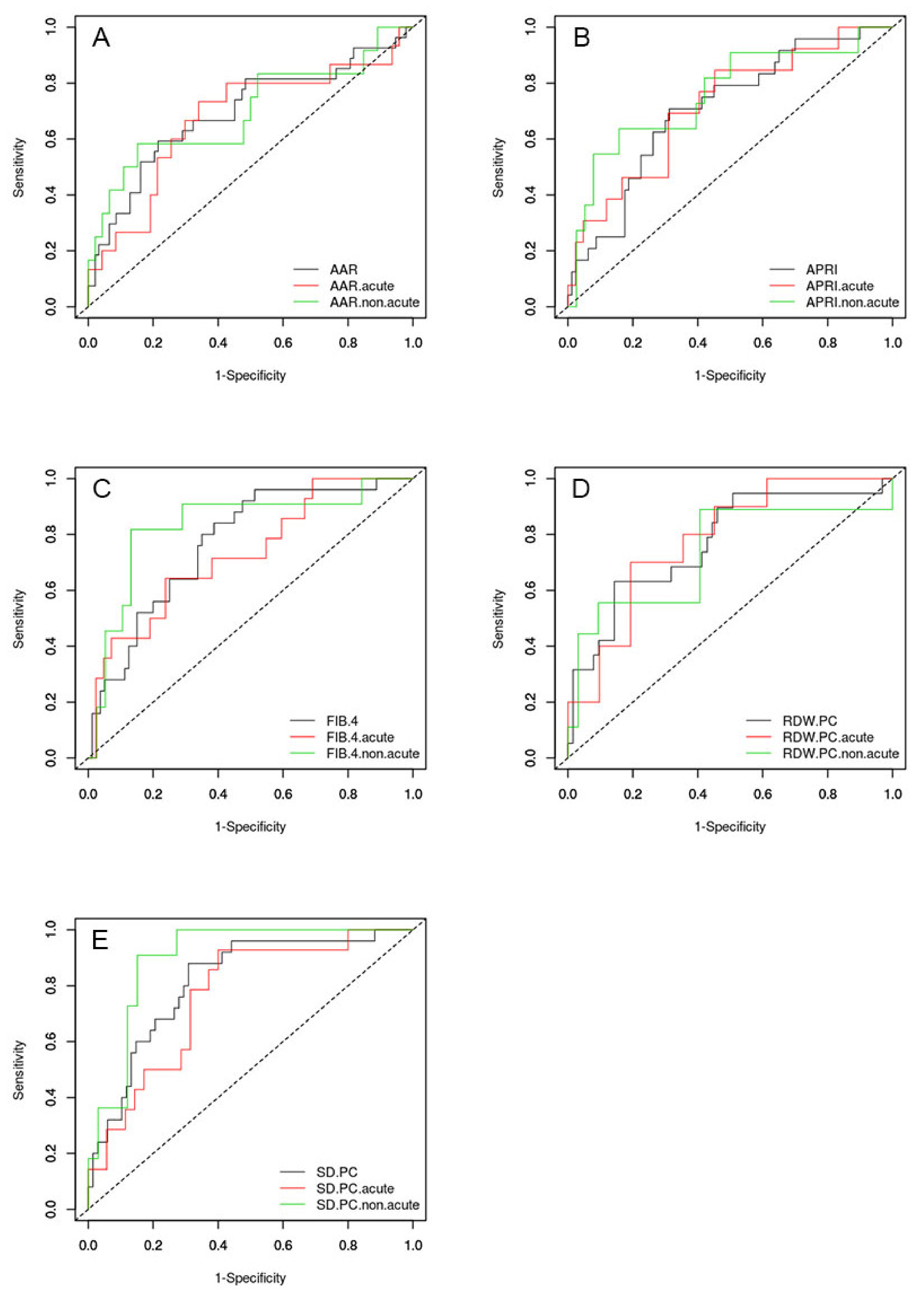
| FIB-4 | All patients (n = 105) | 0.770 | (0.670–0.870) | 5298.42 | <0.001 |
| Acute (n = 56) | 0.724 | (0.567–0.881) | 2792.685 | 0.005 | |
| Non-acute (n = 49) | 0.834 | (0.679–0.990) | 4206.383 | <0.001 | |
| APRI | All patients (n = 105) | 0.708 | (0.592–0.823) | 3.522 | <0.001 |
| Acute (n = 56) | 0.716 | (0.553–0.879) | 2.605 | 0.009 | |
| Non-acute (n = 49) | 0.758 | (0.579–0.938) | 2.816 | 0.005 | |
| AAR | All patients (n = 120) | 0.694 | (0.568–0.819) | 3022.145 | 0.003 |
| Acute (n = 62) | 0.674 | (0.500–0.848) | 1958.879 | 0.050 | |
| Non-acute (n = 58) | 0.697 | (0.500–0.894) | 1969.192 | 0.049 | |
| RDW/PC | All patients (n = 82) | 0.768 | (0.640–0.896) | 4114.128 | <0.001 |
| Acute (n = 41) | 0.773 | (0.614–0.933) | 3362.831 | 0.001 | |
| Non-acute (n = 41) | 0.733 | (0.506–0.959) | 201.469 | 0.044 | |
| SD/PC | All patients (n = 93) | 0.814 | (0.719–0.909) | 6478.971 | <0.001 |
| Acute (n = 49) | 0.754 | (0.606–0.902) | 3371.503 | 0.001 | |
| Non-acute (n = 44) | 0.902 | (0.814–0.990) | 8988.844 | <0.001 |
| Test | Population | Cut-Off | Sensitivity | Specificity | PPV | NPV | LR pos | LR neg |
|---|---|---|---|---|---|---|---|---|
| FIB-4 | All patients | 2.000 | 0.960 | 0.487 | 0.369 | 0.975 | 1.873 | 0.082 |
| Non-acute | 3.300 | 0.818 | 0.872 | 0.643 | 0.944 | 6.382 | 0.209 | |
| Acute | 6.200 | 0.643 | 0.756 | 0.474 | 0.861 | 2.636 | 0.472 | |
| APRI | All patients | 6.044 | 0.708 | 0.688 | 0.405 | 0.887 | 2.267 | 0.424 |
| Non-acute | 3.422 | 0.636 | 0.842 | 0.538 | 0.889 | 4.03 | 0.432 | |
| Acute | 7.232 | 0.846 | 0.548 | 0.367 | 0.92 | 1.87 | 0.281 | |
| AAR | All patients | 0.930 | 0.593 | 0.787 | 0.444 | 0.871 | 2.785 | 0.518 |
| Non-acute | 0.934 | 0.583 | 0.848 | 0.5 | 0.886 | 3.833 | 0.491 | |
| Acute | 0.825 | 0.733 | 0.66 | 0.407 | 0.886 | 2.154 | 0.404 | |
| RDW/PC | All patients | 0.087 | 0.632 | 0.859 | 0.571 | 0.887 | 4.491 | 0.429 |
| Non-acute | 0.061 | 0.889 | 0.594 | 0.381 | 0.95 | 2.188 | 0.187 | |
| Acute | 0.087 | 0.700 | 0.800 | 0.538 | 0.889 | 3.5 | 0.375 | |
| SD/PC | All patients | 0.054 | 0.880 | 0.691 | 0.512 | 0.94 | 2.85 | 0.174 |
| Non-acute | 0.062 | 0.909 | 0.853 | 0.667 | 0.967 | 6.182 | 0.107 | |
| Acute | 0.045 | 0.929 | 0.588 | 0.481 | 0.952 | 2.255 | 0.121 |
| NIT | Article Type | CLD | N | AUC | Cut-Off | Diagnostic Accuracy |
|---|---|---|---|---|---|---|
| FIB-4 [13] | Metanalysis | CHB | 3139 | 0.80 (0.74–0.91) | 0.5 | SE 73%, SP 55% |
| FIB-4 [14] | Review | NAFLD | 686 | 0.80–0.86 | 1.3 | NPV 90–95% |
| 3.25 | PPV 75% | |||||
| FIB-4 [15] | Retrospective multicenter | NAFLD | 1904 | NR | 1.37 | SE 75%, SP 71% |
| FIB-4 [16] | Retrospective monocentric | CHC | 798 | 0.84 | NR | NR |
| FIB-4 [17] | Retrospective monocentric | AIH | 108 | 0.64 (0.53–0.74) | 3.21 | SE 24%, SP 78% |
| FIB-4 [18] | Retrospective monocentric | AIH | 76 | 0.74 (0.62–0.86) | 2.37 | SE 74%, SP 71% |
| FIB-4 [5] | Metanalysis | AIH | 421 | 0.76 (0.72–0.79) | NR | SE 60%, SP 76% |
| FIB-4 [19] | Retrospective monocentric | AIH | 45 | 0.76 (0.61–0.90) | 2.26 | SE 77%, SP 74% |
| RDW/PC [4] | Metanalysis | Various | 1489 | 0.83 (±0.03) | 0.07 | SE 78%, SP 70% |
| RDW/PC [19] | Retrospective monocentric | AIH | 45 | 0.79 (0.65–0.92) | 0.24 | SE 86%, SP 61% |
| AAR [15] | Retrospective multicentre | NAFLD | 1904 | 0.68 (0.66–0.71) | 0.85 | SE 54%, SP 73% |
| AAR [19] | Retrospective monocentric | AIH | 45 | 0.71 (0.56–0.86) | 0.77 | SE 82%, SP 57% |
| AAR [18] | Retrospective monocentric | AIH | 76 | 0.73 (0.61–0.85) | 1.0 | SE 59%, SP 71% |
| AAR [14] | Review | NAFLD | 174 | 0.83–0.90 | 0.8 | NPV 93%, PPV 44% |
| AAR [5] | Metanalysis | AIH | 252 | 0.73 (0.69–0.76) | NR | SE 84%, SP 64% |
| APRI [16] | Retrospective monocentric | CHC | 798 | 0.82 | NR | NR |
| APRI [13] | Metanalysis | CHB | 3139 | 0.76 (0.68–0.87) | NR | NR |
| APRI [20] | Retrospective monocentric | NAFLD | 111 | 0.85 | 0.98 | SE 75%, SP 86% |
| APRI [14] | Review | NAFLD | 175 | 0.56–0.67 | 1 | NPV 84%, PPV 37% |
| APRI [15] | Retrospective multicentre | NAFLD | 1904 | NR | 0.84 | SE 75%, SP 65% |
| APRI [5] | Metanalysis | AIH | 506 | 0.74 (0.70–0.78) | NR | SE 72%, SP 64% |
| APRI [17] | Retrospective monocentric | AIH | 108 | 0.65 (0.54–0.75) | 2.13 | SE 43%, SP 89% |
| APRI [18] | Retrospective monocentric | AIH | 76 | 0.71 (0.58–0.83) | 0.84 | SE 83%, SP 63% |
| SD/PC [18] | Retrospective monocentric | AIH | 76 | 0.88 (0.80–0.97) | 0.001 | SE 88%, SP 85% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferronato, M.; Lenzi, M.; Muratori, P.; Muratori, L. Blood-Based Non-Invasive Tests of Hepatic Fibrosis in Autoimmune Hepatitis: Application among Selected Patients Leads to Higher Accuracy. Gastroenterol. Insights 2022, 13, 286-295. https://doi.org/10.3390/gastroent13030029
Ferronato M, Lenzi M, Muratori P, Muratori L. Blood-Based Non-Invasive Tests of Hepatic Fibrosis in Autoimmune Hepatitis: Application among Selected Patients Leads to Higher Accuracy. Gastroenterology Insights. 2022; 13(3):286-295. https://doi.org/10.3390/gastroent13030029
Chicago/Turabian StyleFerronato, Marco, Marco Lenzi, Paolo Muratori, and Luigi Muratori. 2022. "Blood-Based Non-Invasive Tests of Hepatic Fibrosis in Autoimmune Hepatitis: Application among Selected Patients Leads to Higher Accuracy" Gastroenterology Insights 13, no. 3: 286-295. https://doi.org/10.3390/gastroent13030029