
Twelve-Month Results from a Prospective Clinical Study Evaluating the Efficacy and Safety of Cellular Bone Allograft in Subjects Undergoing Lumbar Spinal Fusion
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design and Treatment
2.3. Assessments
2.4. Statistical Analysis
3. Results
3.1. Subject Demographics and Surgical Procedure
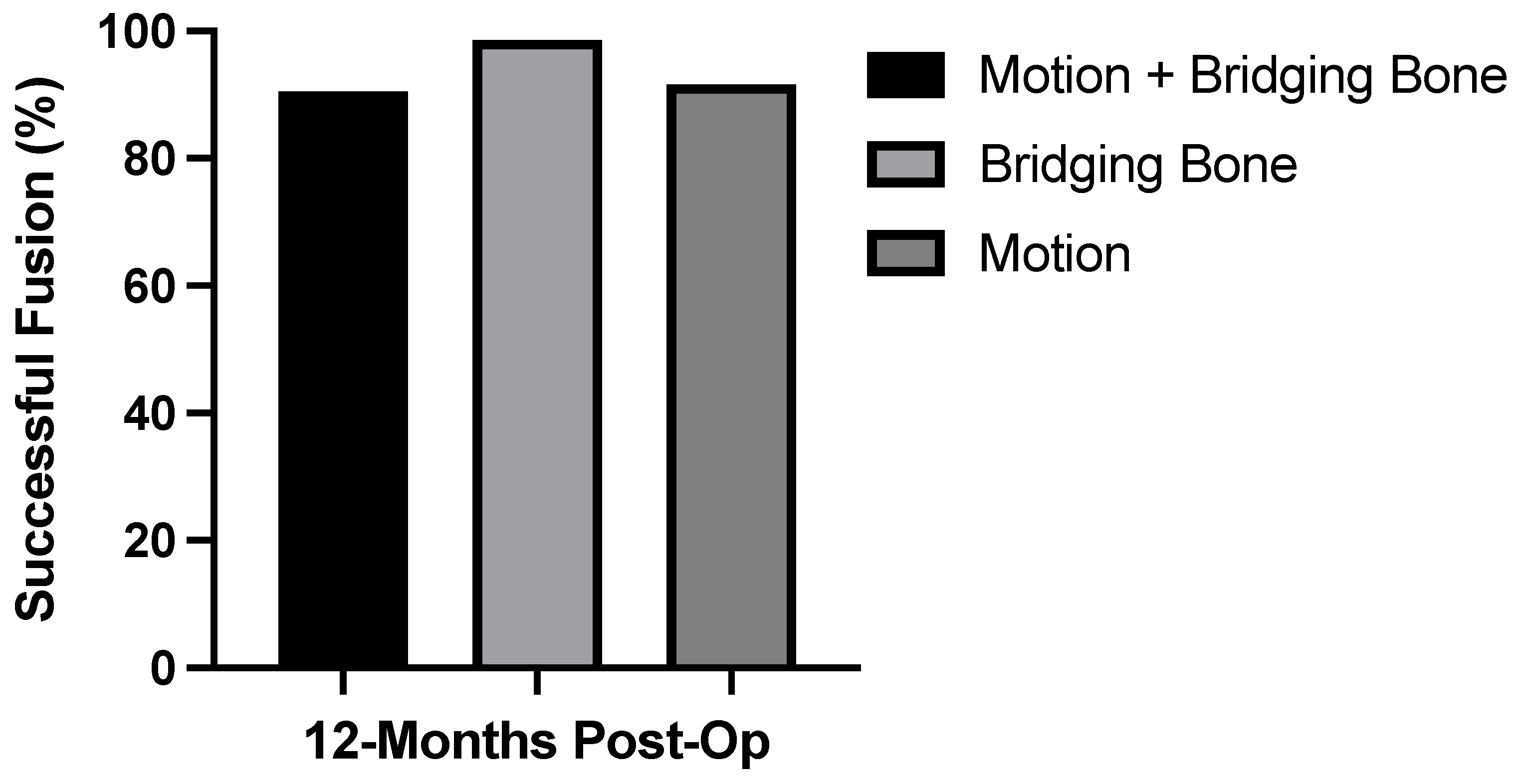
3.2. Radiographic Fusion Outcomes
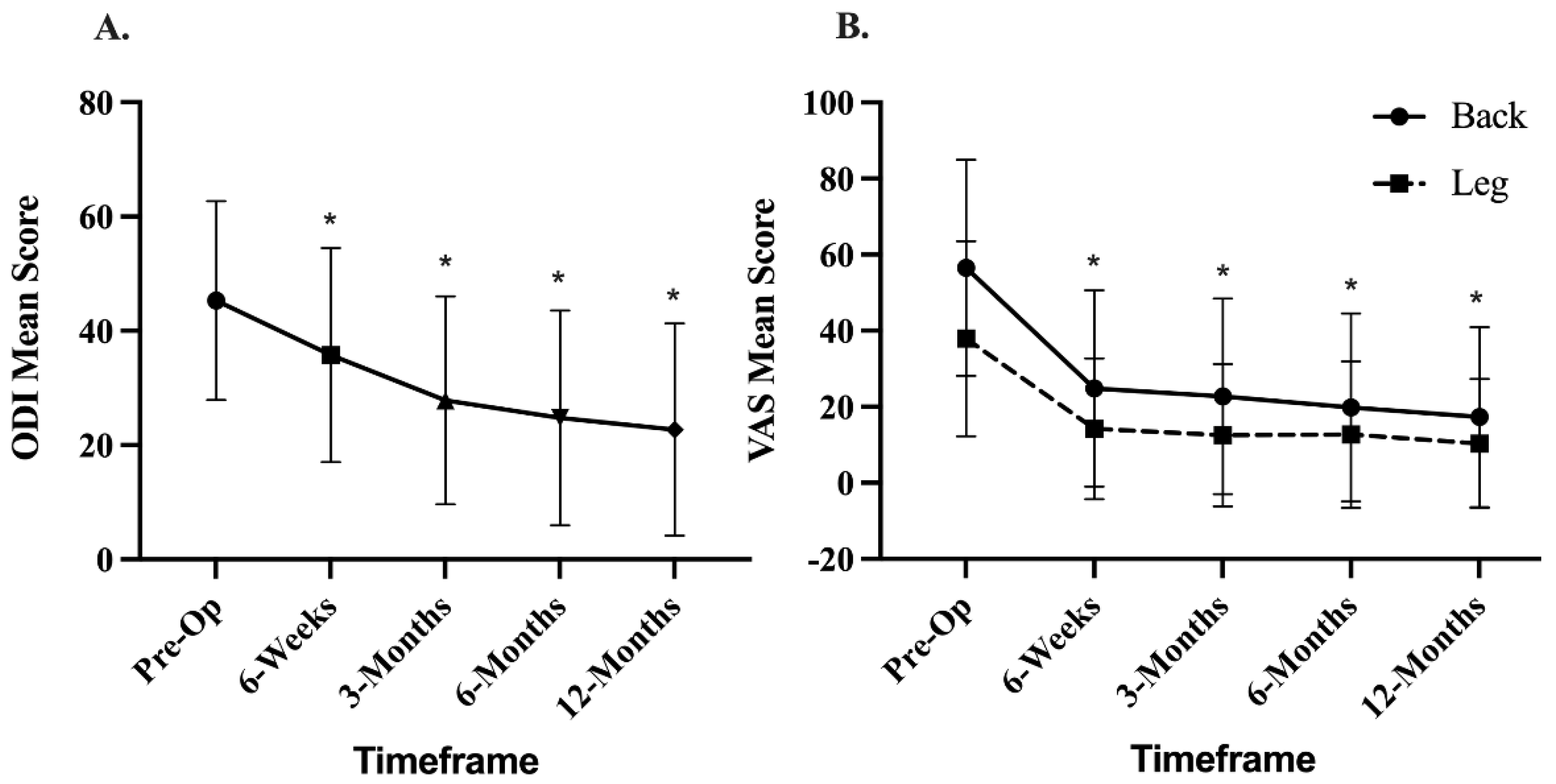
3.3. Clinical Outcomes
3.4. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lykissas, M.G.; Aichmair, A. Current concepts on spinal arthrodesis in degenerative disorders of the lumbar spine. World J. Clin. Cases 2013, 1, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.N.; Cammisa, F.P., Jr.; Sandhu, H.S.; Diwan, A.D.; Girardi, F.P.; Lane, J.M. The Biology of Bone Grafting. J. Am. Acad. Orthop. Surg. 2005, 13, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Park, J.J.; Hershman, S.H.; Kim, Y. Updates in the use of bone grafts in the lumbar spine. Bull. Hosp. Jt. Dis. 2013, 71, 39–48. [Google Scholar]
- Sheha, E.D.; Meredith, D.S.; Shifflett, G.D.; Bjerke, B.T.; Iyer, S.; Shue, J.; Nguyen, J.; Huang, R.C. Postoperative pain following posterior iliac crest bone graft harvesting in spine surgery: A prospective, randomized trial. Spine J. 2018, 18, 986–992. [Google Scholar] [CrossRef] [PubMed]
- Boone, D.W. Complications of iliac crest graft and bone grafting alternatives in foot and ankle surgery. Foot Ankle Clin. 2003, 8, 1–14. [Google Scholar] [CrossRef]
- Katz, M.; Ooms, M.; Heitzer, M.; Peters, F.; Winnand, P.; Kniha, K.; Möhlhenrich, S.; Hölzle, F.; Knobe, M.; Modabber, A. Postoperative Morbidity and Complications in Elderly Patients after Harvesting of Iliac Crest Bone Grafts. Medicina 2021, 57, 759. [Google Scholar] [CrossRef]
- Ahlmann, E.; Patzakis, M.; Roidis, N.; Shepherd, L.; Holtom, P. Comparison of Anterior and Posterior Iliac Crest Bone GRAFTS in Terms of Harvest-Site Morbidity and Functional Outcomes. J. Bone Jt. Surg. 2002, 84, 716–720. [Google Scholar] [CrossRef]
- Gruskay, J.A.; Basques, B.A.; Bohl, D.D.; Webb, M.L.; Grauer, J.N. Short-Term Adverse Events, Length of Stay, and Readmission After Iliac Crest Bone Graft for Spinal Fusion. Spine 2014, 39, 1718–1724. [Google Scholar] [CrossRef]
- Fernyhough, J.C.; Schimandle, J.J.; Weigel, M.C.; Edwards, C.C.; Levine, A.M. Chronic Donor Site Pain Complicating Bone Graft Harvesting from the Posterior Iliac Crest for Spinal Fusion. Spine 1992, 17, 1474–1480. [Google Scholar] [CrossRef]
- Fowler, B.L.; Dall, B.; Rowe, D.E. Complications associated with harvesting autogenous iliac bone graft. Am. J. Orthop. 1995, 24, 895–903. [Google Scholar]
- Arrington, E.D.; Smith, W.J.; Chambers, H.G.; Bucknell, A.L.; Davino, N.A. Complications of Iliac Crest Bone Graft Harvesting. Clin. Orthop. Relat. Res. 1996, 329, 300–309. [Google Scholar] [CrossRef]
- Goulet, J.A.; Senunas, L.E.; DeSilva, G.L.; Greenfield, M.L.V.H. Autogenous Iliac Crest Bone Graft: Complications and Functional Assessment. Clin. Orthop. Relat. Res. 1997, 339, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Younger, E.M.; Chapman, M.W. Morbidity at Bone Graft Donor Sites. J. Orthop. Trauma 1989, 3, 192–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, B.; Jenis, L.G. Carrier materials for spinal fusion. Spine J. 2005, 5, S224–S230. [Google Scholar] [CrossRef]
- Buser, Z.; Brodke, D.S.; Youssef, J.A.; Meisel, H.-J.; Myhre, S.L.; Hashimoto, R.; Park, J.-B.; Yoon, S.T.; Wang, J.C. Synthetic bone graft versus autograft or allograft for spinal fusion: A systematic review. J. Neurosurg. Spine 2016, 25, 509–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; Powers, R.M., Jr.; Wolfinbarger, L., Jr. Effect(s) of the demineralization process on the osteoinductivity of demineralized bone matrix. J. Periodontol. 1997, 68, 1085–1092. [Google Scholar] [CrossRef] [PubMed]
- Turonis, J.W.; McPherson, J.C.; Cuenin, M.F.; Hokett, S.D.; Peacock, M.E.; Sharawy, M. The Effect of Residual Calcium in Decalcified Freeze-dried Bone Allograft in a Critical-sized Defect in the Rattus norvegicus Calvarium. J. Oral Implant. 2006, 32, 55–62. [Google Scholar] [CrossRef]
- Ammerman, J.M.; Libricz, J.; Ammerman, M.D. The role of Osteocel Plus as a fusion substrate in minimally invasive instrumented transforaminal lumbar interbody fusion. Clin. Neurol. Neurosurg. 2013, 115, 991–994. [Google Scholar] [CrossRef]
- Tohmeh, A.G.; Watson, B.; Tohmeh, M.; Zielinski, X.J. Allograft Cellular Bone Matrix in Extreme Lateral Interbody Fusion: Preliminary Radiographic and Clinical Outcomes. Sci. World J. 2012, 2012, 263637. [Google Scholar] [CrossRef] [Green Version]
- Elgafy, H.; Wetzell, B.; Gillette, M.; Semaan, H.; Rowland, A.; Balboa, C.A.; Mierzwa, T.A.; McLean, J.B.; Dorsch, K.; Moore, M.A. Lumbar spine fusion outcomes using a cellular bone allograft with lineage-committed bone-forming cells in 96 patients. BMC Musculoskelet. Disord. 2021, 22, 699. [Google Scholar] [CrossRef]
- Hall, J.F.; McLean, J.B.; Jones, S.M.; Moore, M.A.; Nicholson, M.D.; Dorsch, K.A. Multilevel instrumented posterolateral lumbar spine fusion with an allogeneic cellular bone graft. J. Orthop. Surg. Res. 2019, 14, 372–379. [Google Scholar] [CrossRef]
- Reisener, M.-J.; Pumberger, M.; Shue, J.; Girardi, F.P.; Hughes, A.P. Trends in lumbar spinal fusion—A literature review. J. Spine Surg. 2020, 6, 752–761. [Google Scholar] [CrossRef] [PubMed]
- Martin, B.I.; Mirza, S.K.; Spina, N.; Spiker, W.R.; Lawrence, B.; Brodke, D.S. Trends in Lumbar Fusion Procedure Rates and Associated Hospital Costs for Degenerative Spinal Diseases in the United States, 2004 to 2015. Spine 2019, 44, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Debono, B.; Lonjon, G.; Alvarez, L.; Kerever, S.; Guiot, B.; Eicker, S.; Hamel, O.; Ringel, F. Indication Variability in Degenerative Lumbar Spine Surgery: A Four-nation Survey. Spine 2018, 43, 185–192. [Google Scholar] [CrossRef]
- Lee, S.C.; Chen, J.F.; Wu, C.T.; Lee, S.T. In situ local autograft for instrumented lower lumbar or lumbosacral posterolateral fusion. J. Clin. Neurosci. 2009, 16, 37–43. [Google Scholar] [CrossRef]
- Sengupta, D.K.; Truumees, E.; Patel, C.K.; Kazmierczak, C.; Hughes, B.; Elders, G.; Herkowitz, H.N. Outcome of Local Bone Versus Autogenous Iliac Crest Bone Graft in the Instrumented Posterolateral Fusion of the Lumbar Spine. Spine 2006, 31, 985–991. [Google Scholar] [CrossRef]
- Ohtori, S.; Koshi, T.; Yamashita, M.; Takaso, M.; Yamauchi, K.; Inoue, G.; Suzuki, M.; Orita, S.; Eguchi, Y.; Ochiai, N.; et al. Single-level instrumented posterolateral fusion versus non-instrumented anterior interbody fusion for lumbar spondylolisthesis: A prospective study with a 2-year follow-up. J. Orthop. Sci. 2011, 16, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Inage, K.; Ohtori, S.; Koshi, T.; Suzuki, M.; Takaso, M.; Yamashita, M.; Yamauchi, K.; Inoue, G.; Orita, S.; Eguchi, Y.; et al. One, two-, and three-level instrumented posterolateral fusion of the lumbar spine with a local bone graft: A prospective study with a 2-year follow-up. Spine 2011, 36, 1392–1396. [Google Scholar] [CrossRef]
- Han, S.; Park, B.; Lim, J.-W.; Youm, J.-Y.; Choi, S.-W.; Kim, D.H.; Ahn, D.K. Comparison of Fusion Rate between Demineralized Bone Matrix versus Autograft in Lumbar Fusion: Meta-Analysis. J. Korean Neurosurg. Soc. 2020, 63, 673–680. [Google Scholar] [CrossRef]
- Kang, J.; An, H.; Hilibrand, A.; Yoon, S.T.; Kavanagh, E.; Boden, S. Grafton and Local Bone Have Comparable Outcomes to Iliac Crest Bone in Instrumented Single-Level Lumbar Fusions. Spine 2012, 37, 1083–1091. [Google Scholar] [CrossRef]
- Abou-Madawi, A.M.; Ali, S.H.; Abdelmonem, A.M. Local Autograft Versus Iliac Crest Bone Graft PSF-Augmented TLIF in Low-Grade Isthmic and Degenerative Lumbar Spondylolisthesis. Glob. Spine J. 2022, 12, 70–78. [Google Scholar] [CrossRef]
- Peppers, T.A.; Bullard, D.E.; Vanichkachorn, J.S.; Stanley, S.K.; Arnold, P.M.; Waldorff, E.I.; Hahn, R.; Atkinson, B.L.; Ryaby, J.T.; Linovitz, R.J. Prospective clinical and radiographic evaluation of an allogeneic bone matrix containing stem cells (Trinity Evolution(R) Viable Cellular Bone Matrix) in patients undergoing two-level anterior cervical discectomy and fusion. J. Orthop. Surg. Res. 2017, 12, 67. [Google Scholar] [CrossRef]
- Vanichkachorn, J.; Peppers, T.; Bullard, D.; Stanley, S.K.; Linovitz, R.J.; Ryaby, J.T. A prospective clinical and radiographic 12-month outcome study of patients undergoing single-level anterior cervical discectomy and fusion for symptomatic cervical degenerative disc disease utilizing a novel viable allogeneic, cancellous, bone matrix (trinity evolution™) with a comparison to historical controls. Eur. Spine J. 2016, 25, 2233–2238. [Google Scholar] [PubMed] [Green Version]
- Musante, D.B.; Firtha, M.E.; Atkinson, B.L.; Hahn, R.; Ryaby, J.T.; Linovitz, R.J. Clinical evaluation of an allogeneic bone matrix containing viable osteogenic cells in patients undergoing one- and two-level posterolateral lumbar arthrodesis with decompressive laminectomy. J. Orthop. Surg. Res. 2016, 11, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darveau, S.C.; Leary, O.P.; Persad-Paisley, E.M.; Shaaya, E.A.; Oyelese, A.A.; Fridley, J.S.; Sampath, P.; Camara-Quintana, J.Q.; Gokaslan, Z.L.; Niu, T. Existing clinical evidence on the use of cellular bone matrix grafts in spinal fusion: Updated systematic review of the literature. Neurosurg. Focus 2021, 50, E12. [Google Scholar] [CrossRef] [PubMed]
- Copay, A.G.; Glassman, S.D.; Subach, B.R.; Berven, S.; Schuler, T.C.; Carreon, L.Y. Minimum clinically important difference in lumbar spine surgery patients: A choice of methods using the Oswestry Disability Index, Medical Outcomes Study questionnaire Short Form 36, and Pain Scales. Spine J. 2008, 8, 968–974. [Google Scholar] [CrossRef]
- Glassman, S.D.; Copay, A.G.; Berven, S.H.; Polly, D.W.; Subach, B.R.; Carreon, L.Y. Defining Substantial Clinical Benefit Following Lumbar Spine Arthrodesis. J. Bone Jt. Surg. 2008, 90, 1839–1847. [Google Scholar] [CrossRef]
- Niu, S.; Anastasio, A.T.; Faraj, R.R.; Rhee, J.M. Evaluation of Heterotopic Ossification After Using Recombinant Human Bone Morphogenetic Protein-2 in Transforaminal Lumbar Interbody Fusion: A Computed Tomography Review of 996 Disc Levels. Glob. Spine J. 2020, 10, 280–285. [Google Scholar] [CrossRef]
- Kasis, A.G.; Jensen, C.; Dharmadhikari, R.; Emmerson, B.R.; Mawdsley, M. Novel bone grafting technique in stand-alone ALIF procedure combining allograft and autograft (‘Northumbria Technique’)—Fusion rate and functional outcomes in 100 consecutive patients. Eur. Spine J. 2021, 30, 1296–1302. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Subjects (N = 201) |
|---|---|
| Age (years), Mean (Range) | 60.2 ± 11.5 (28–82) |
| Female; Male, n (%) | 124 (61.7); 77 (38.3) |
| BMI, Mean (Range) | 30.6 ± 6.5 kg/m2 (18.0–51.4) |
| Smoker, n (%) | 31 (15.4) |
| Diabetes, n (%) | 41 (20.4) |
| Osteoporosis, n (%) | 15 (7.5) |
| Total Subjects N | Fusion Success N (%) | |
|---|---|---|
| Level | ||
| 1 Level | 141 | 128 (90.8) |
| 2 Level | 57 | 52 (91.2) |
| 3 Level | 1 | 1 (100.0) |
| 4 Level | 2 | 1 (50.0) |
| Surgical Approach | ||
| Anterior Lumbar Interbody Fusion (ALIF) | 49 | 40 (81.6) |
| Posterior Lumbar Interbody Fusion (TLIF/PLIF) | 86 | 80 (93.0) |
| Lateral or Oblique Lateral Lumbar Interbody Fusion (OLIF/XLIF/LLIF/DLIF) | 53 | 50 (94.3) |
| Posterolateral Lumbar Fusion (PLF) | 13 | 12 (92.3) |
| Risk Factor | Fusion Success | p-Value |
|---|---|---|
| BMI ≥ 30 | 93.4% (n = 107) | 0.1324 |
| Smoking | 87. 1% (n = 31) | 0.5036 |
| Age + 65 | 88.1% (n = 84) | 0.3140 |
| Diabetes | 85.3% (n = 41) | 0.2037 |
| Osteoporosis | 80.0% (n = 15) | 0.1567 |
| Multiple Risk Factors | 90.5% (n = 106) | 0.4970 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wind, J.; Park, D.; Lansford, T.; Nunley, P.; Peppers, T.; Russo, A.; Hassanzadeh, H.; Sembrano, J.N.; Yoo, J.; Sales, J. Twelve-Month Results from a Prospective Clinical Study Evaluating the Efficacy and Safety of Cellular Bone Allograft in Subjects Undergoing Lumbar Spinal Fusion. Neurol. Int. 2022, 14, 875-883. https://doi.org/10.3390/neurolint14040070
Wind J, Park D, Lansford T, Nunley P, Peppers T, Russo A, Hassanzadeh H, Sembrano JN, Yoo J, Sales J. Twelve-Month Results from a Prospective Clinical Study Evaluating the Efficacy and Safety of Cellular Bone Allograft in Subjects Undergoing Lumbar Spinal Fusion. Neurology International. 2022; 14(4):875-883. https://doi.org/10.3390/neurolint14040070
Chicago/Turabian StyleWind, Joshua, Daniel Park, Todd Lansford, Pierce Nunley, Timothy Peppers, Anthony Russo, Hamid Hassanzadeh, Jonathan N. Sembrano, Jung Yoo, and Jonathan Sales. 2022. "Twelve-Month Results from a Prospective Clinical Study Evaluating the Efficacy and Safety of Cellular Bone Allograft in Subjects Undergoing Lumbar Spinal Fusion" Neurology International 14, no. 4: 875-883. https://doi.org/10.3390/neurolint14040070