
Pharmacokinetic Modeling of Bepotastine for Determination of Optimal Dosage Regimen in Pediatric Patients with Allergic Rhinitis or Urticaria
 , , , , and
, , , , and
Abstract
:1. Introduction
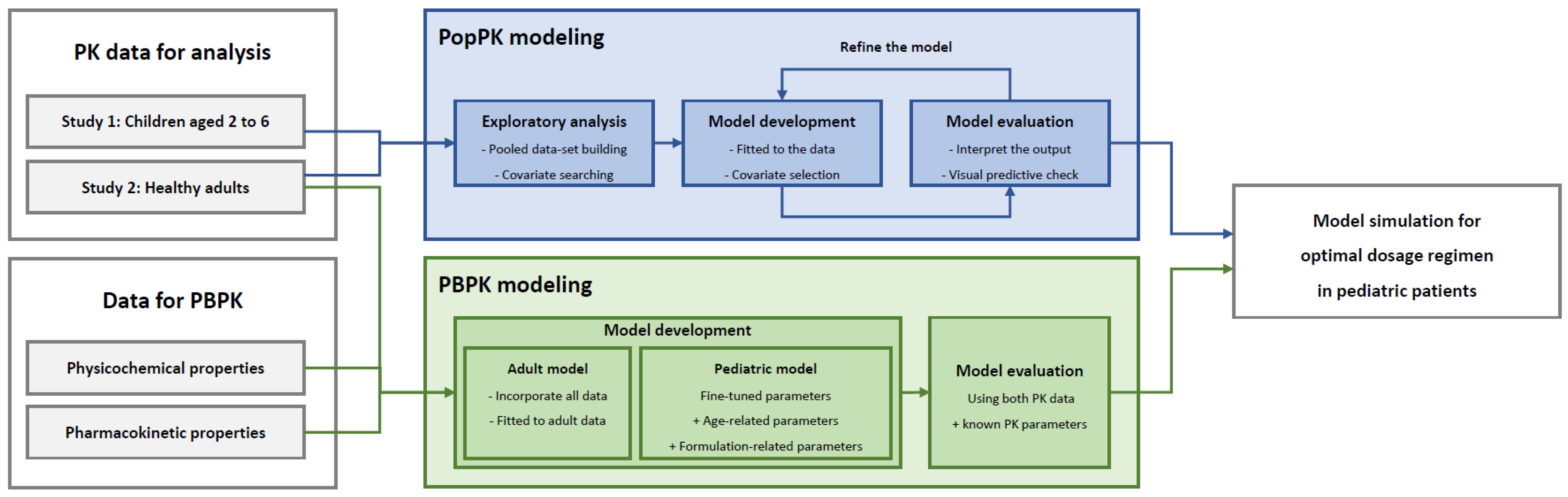
2. Materials and Methods
2.1. Data Collection
2.2. PopPK Model Development
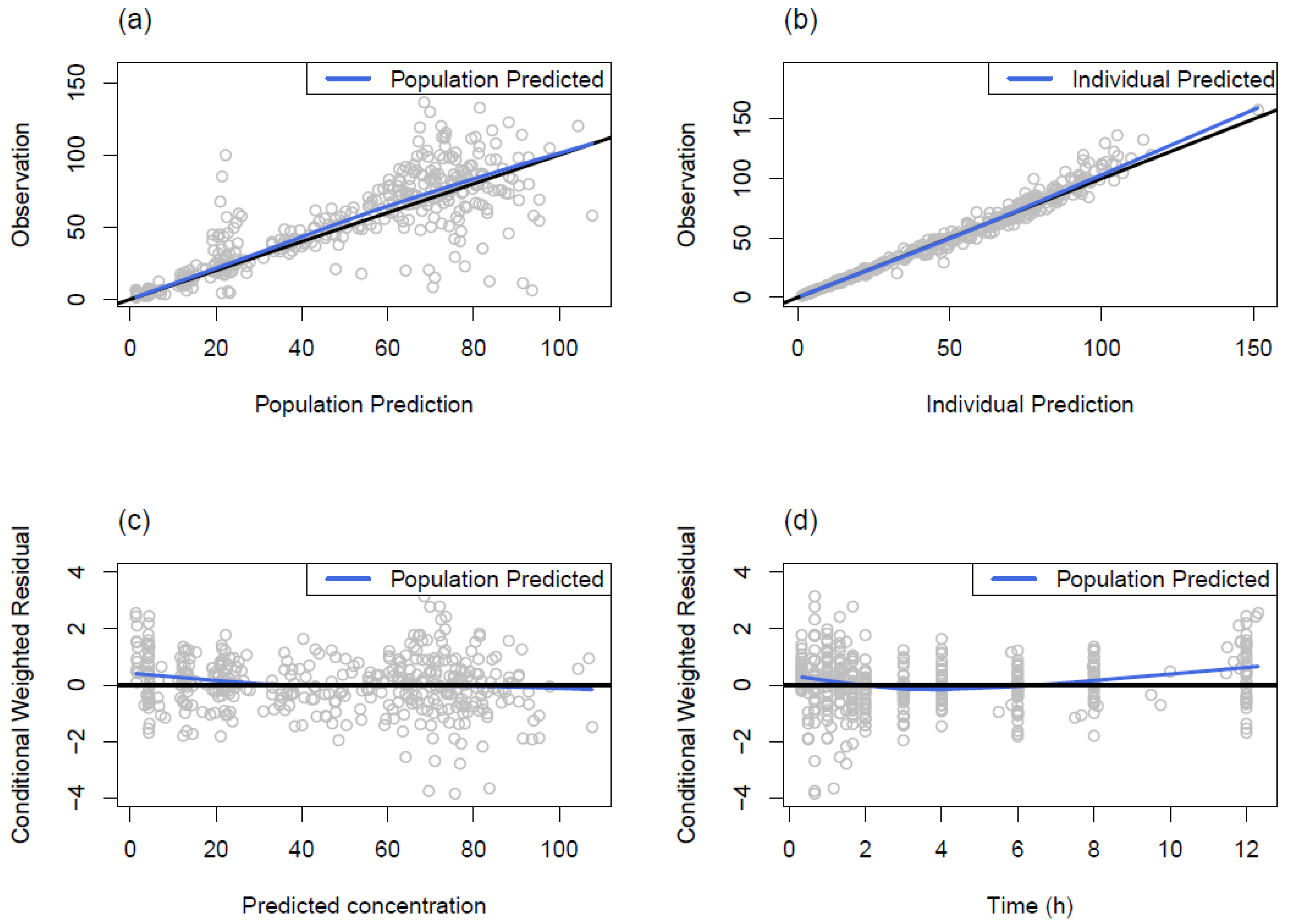
2.3. PopPK Model Evaluation
2.4. PopPK Model Simulation
2.5. PBPK Model Development
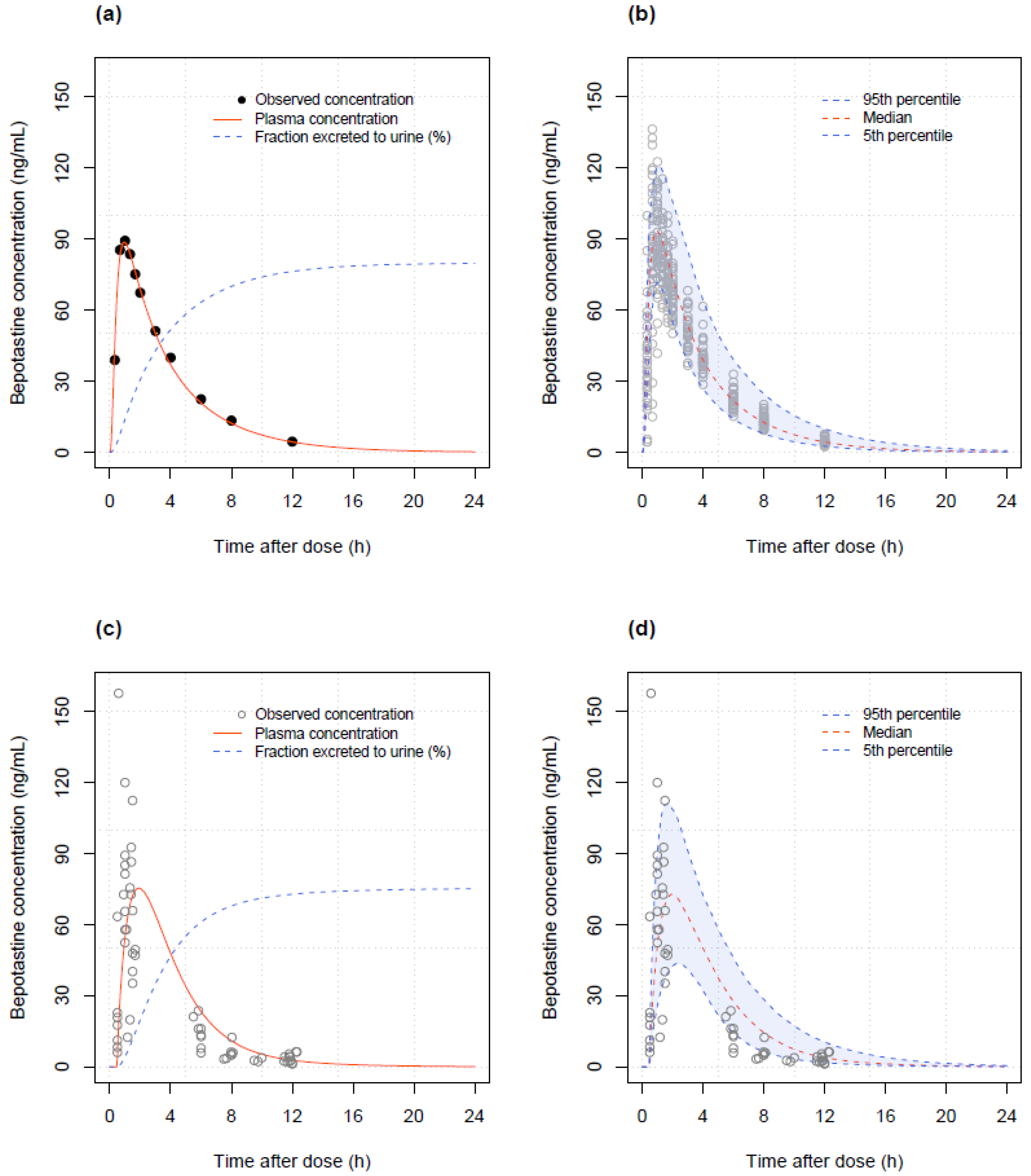
2.6. PBPK Model Evaluation
2.7. PBPK Model Simulation
3. Results
3.1. PopPK Model
3.2. PopPK Model Simulation
3.3. PBPK Model
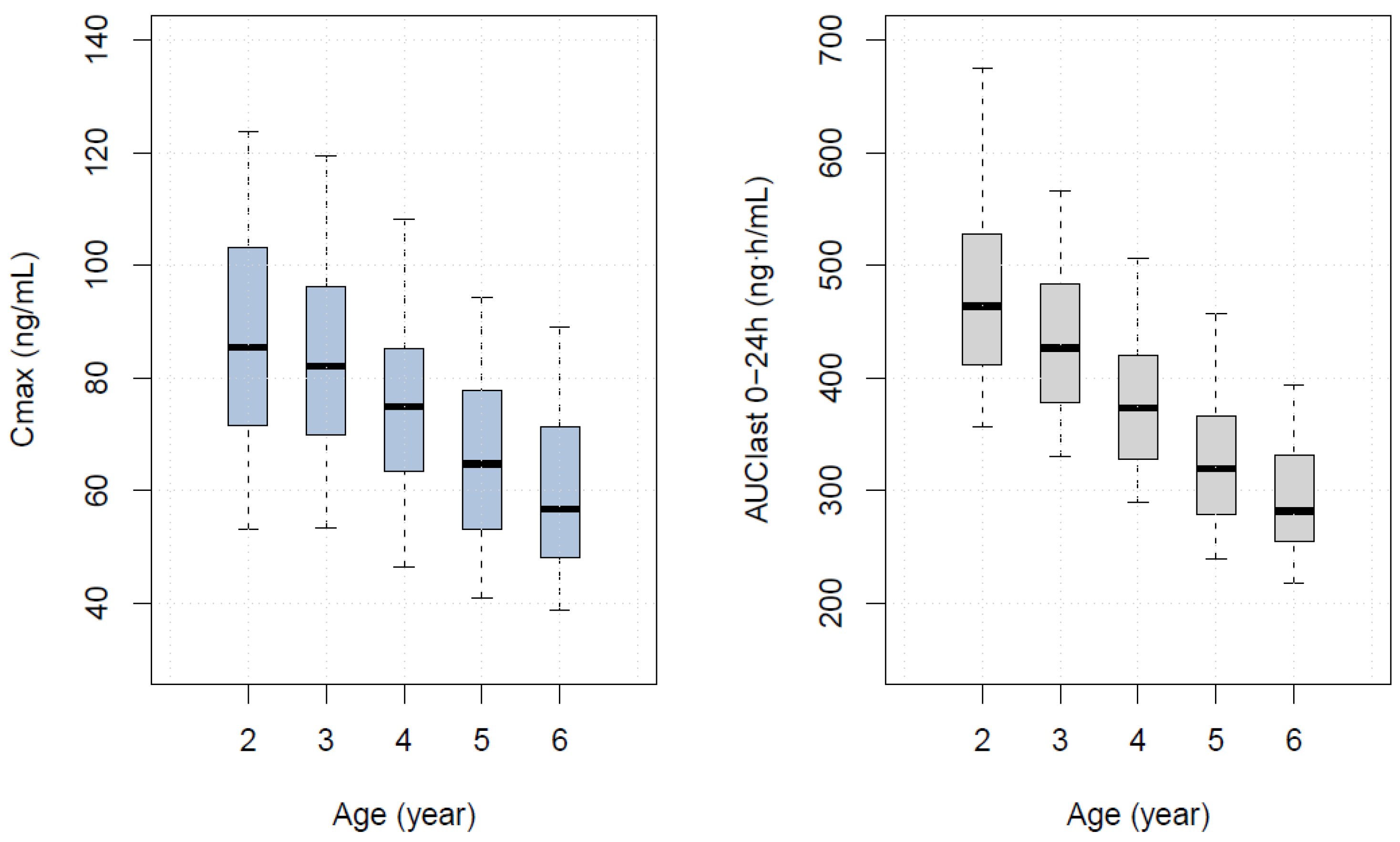
3.4. PBPK Model Simulation
3.5. Comparison of Predictive Performance of Two Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Simons, F.E.; Simons, K.J. Histamine and H1-antihistamines: Celebrating a century of progress. J. Allergy Clin. Immunol. 2011, 128, 1139–1150.e1134. [Google Scholar] [CrossRef]
- Ohashi, R.; Kamikozawa, Y.; Sugiura, M.; Fukuda, H.; Yabuuchi, H.; Tamai, I. Effect of p-glycoprotein on intestinal absorption and brain penetration of antiallergic agent bepotastine besilate. Drug Metab. Dispos. 2006, 34, 793–799. [Google Scholar] [CrossRef]
- Tanizaki, H.; Ikoma, A.; Fukuoka, M.; Miyachi, Y.; Kabashima, K. Effects of bepotastine and fexofenadine on histamine-induced flare, wheal and itch. Int. Arch. Allergy Immunol. 2012, 158, 191–195. [Google Scholar] [CrossRef]
- Abelson, M.B.; Torkildsen, G.L.; Williams, J.I.; Gow, J.A.; Gomes, P.J.; McNamara, T.R.; Bepotastine Besilate Ophthalmic Solutions Clinical Study Group. Time to onset and duration of action of the antihistamine bepotastine besilate ophthalmic solutions 1.0% and 1.5% in allergic conjunctivitis: A phase iii, single-center, prospective, randomized, double-masked, placebo-controlled, conjunctival allergen challenge assessment in adults and children. Clin. Ther. 2009, 31, 1908–1921. [Google Scholar] [PubMed]
- Bepreve Prescribing Information. Available online: https://www.bausch.com/globalassets/pdf/packageinserts/pharma/bepreve-prescribing-info.pdf (accessed on 10 January 2024).
- Review Reports: Talion Tablets. Available online: https://www.pmda.go.jp/english/review-services/reviews/approved-information/drugs/0001.html (accessed on 10 January 2024).
- Greiner, A.N.; Hellings, P.W.; Rotiroti, G.; Scadding, G.K. Allergic rhinitis. Lancet 2011, 378, 2112–2122. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, B.F. Urticaria: Impact on quality of life and economic cost. Immunol. Allergy Clin. N. Am. 2014, 34, 89–104. [Google Scholar] [CrossRef]
- Okubo, K.; Ichimura, M.; Koyama, T.; Susuta, Y.; Izaki, H. Double-blind placebo-controlled study of bepotastine besilate in pediatric patients with perennial allergic rhinitis. Expert Opin. Pharmacother. 2015, 16, 2395–2408. [Google Scholar] [CrossRef] [PubMed]
- Mould, D.R.; Upton, R.N. Basic concepts in population modeling, simulation, and model-based drug development. CPT Pharmacomet. Syst. Pharmacol. 2012, 1, e6. [Google Scholar] [CrossRef]
- Stockmann, C.; Barrett, J.S.; Roberts, J.K.; Sherwin, C. Use of modeling and simulation in the design and conduct of pediatric clinical trials and the optimization of individualized dosing regimens. CPT Pharmacomet. Syst. Pharmacol. 2015, 4, 630–640. [Google Scholar] [CrossRef] [PubMed]
- Bonate, P.L.; Wang, T.; Passier, P.; Bagchus, W.; Burt, H.; Lupfert, C.; Abla, N.; Kovac, J.; Keiser, J. Extrapolation of praziquantel pharmacokinetics to a pediatric population: A cautionary tale. J. Pharmacokinet. Pharmacodyn. 2018, 45, 747–762. [Google Scholar] [CrossRef] [PubMed]
- Maharaj, A.R.; Edginton, A.N. Physiologically based pharmacokinetic modeling and simulation in pediatric drug development. CPT Pharmacomet. Syst. Pharmacol. 2014, 3, e150. [Google Scholar] [CrossRef]
- Ince, I.; Dallmann, A.; Frechen, S.; Coboeken, K.; Niederalt, C.; Wendl, T.; Block, M.; Meyer, M.; Eissing, T.; Burghaus, R.; et al. Predictive performance of physiology-based pharmacokinetic dose estimates for pediatric trials: Evaluation with 10 bayer small-molecule compounds in children. J. Clin. Pharmacol. 2021, 61 (Suppl. S1), S70–S82. [Google Scholar] [CrossRef]
- Peters, S.A. Physiologically-Based Pharmacokinetic (pbpk) Modeling and Simulations: Principles, Methods, and Applications in the Pharmaceutical Industry, 1st ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2012. [Google Scholar]
- Holford, N.; Heo, Y.A.; Anderson, B. A pharmacokinetic standard for babies and adults. J. Pharm. Sci. 2013, 102, 2941–2952. [Google Scholar] [CrossRef] [PubMed]
- Dash, S.; Murthy, P.N.; Nath, L.; Chowdhury, P. Kinetic modeling on drug release from controlled drug delivery systems. Acta Pol. Pharm. 2010, 67, 217–223. [Google Scholar] [PubMed]
- Thelen, K.; Coboeken, K.; Willmann, S.; Burghaus, R.; Dressman, J.B.; Lippert, J. Evolution of a detailed physiological model to simulate the gastrointestinal transit and absorption process in humans, part 1: Oral solutions. J. Pharm. Sci. 2011, 100, 5324–5345. [Google Scholar] [CrossRef] [PubMed]
- Kuepfer, L.; Niederalt, C.; Wendl, T.; Schlender, J.F.; Willmann, S.; Lippert, J.; Block, M.; Eissing, T.; Teutonico, D. Applied concepts in pbpk modeling: How to build a pbpk/pd model. CPT Pharmacomet. Syst. Pharmacol. 2016, 5, 516–531. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Lennernas, H.; Welage, L.S.; Barnett, J.L.; Landowski, C.P.; Foster, D.; Fleisher, D.; Lee, K.D.; Amidon, G.L. Comparison of human duodenum and caco-2 gene expression profiles for 12,000 gene sequences tags and correlation with permeability of 26 drugs. Pharm. Res. 2002, 19, 1400–1416. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.I.; Gow, J.A.; Klier, S.M.; McCue, S.L.; Salapatek, A.M.; McNamara, T.R. Non-clinical pharmacology, pharmacokinetics, and safety findings for the antihistamine bepotastine besilate. Curr. Med. Res. Opin. 2010, 26, 2329–2338. [Google Scholar] [CrossRef]
- Shentu, J.; Zhou, H.; Hu, X.; Wu, G.; Wu, L.; Zhu, M.; Zhai, Y.; Zheng, Y.; Liu, J. Comparative fasting bioavailability of 2 bepotastine formulations in healthy male chinese volunteers: An open-label, randomized, single-dose, 2-way crossover study. Clin. Ther. 2014, 36, 579–585. [Google Scholar] [CrossRef]
- Rowland, M.; Tozer, T.N. Clinical Pharmacokinetics and Pharmacodynamics: Concepts and Applications, 4th ed.; Wolters kluwer, Health/Lippincott William & Wilkins: Philadelphia, PA, USA, 2011; p. 67. [Google Scholar]
- Kim, J.H.; Yun, S.; Hwang, S.S.; Shim, J.O.; Chae, H.W.; Lee, Y.J.; Lee, J.H.; Kim, S.C.; Lim, D.; Yang, S.W.; et al. The 2017 korean national growth charts for children and adolescents: Development, improvement, and prospects. Korean J. Pediatr. 2018, 61, 135–149. [Google Scholar] [CrossRef]
- Cho, K.H.; Choi, H.G. Development of novel bepotastine salicylate salt bioequivalent to the commercial bepotastine besilate in beagle dogs. Drug Dev. Ind. Pharm. 2013, 39, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.A.; Park, J.Y. Pharmacokinetic comparisons of bepotastine besilate and bepotastine salicylate in healthy subjects. Clin. Drug Investig. 2013, 33, 913–919. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.K.; Sahu, A.; Wani, A.A.; Bharatam, P.V.; Chakraborti, A.K.; Giri, S.; Singh, S. Characterization of photodegradation products of bepotastine besilate and in silico evaluation of their physicochemical, absorption, distribution, metabolism, excretion and toxicity properties. J. Pharm. Sci. 2020, 109, 1883–1895. [Google Scholar] [CrossRef] [PubMed]
- Tucker, G.T. Measurement of the renal clearance of drugs. Br. J. Clin. Pharmacol. 1981, 12, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Verbeeck, R.K. Pharmacokinetics and dosage adjustment in patients with hepatic dysfunction. Eur. J. Clin. Pharmacol. 2008, 64, 1147–1161. [Google Scholar] [CrossRef]
- Pasko, P.; Rodacki, T.; Domagala-Rodacka, R.; Palimonka, K.; Marcinkowska, M.; Owczarek, D. Second generation H1–antihistamines interaction with food and alcohol—A systematic review. Biomed. Pharmacother. 2017, 93, 27–39. [Google Scholar] [CrossRef]
- Anderson, B.J.; Holford, N.H. Tips and traps analyzing pediatric pk data. Paediatr. Anaesth. 2011, 21, 222–237. [Google Scholar] [CrossRef]
- Back, H.M.; Lee, J.B.; Han, N.; Goo, S.; Jung, E.; Kim, J.; Song, B.; An, S.H.; Kim, J.T.; Rhie, S.J.; et al. Application of size and maturation functions to population pharmacokinetic modeling of pediatric patients. Pharmaceutics 2019, 11, 259. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study 1 (Adults, n = 32) | Study 2 (Children, n = 30) | |||
|---|---|---|---|---|
| Variables | Mean (SD) | Median (Min–Max) | Mean (SD) | Median (Min–Max) |
| Age (years) | 24.97 (4.02) | 24 (19–37) | 4.33 (1.24) | 5 (2–6) |
| Weight (kg) | 70.95 (8.04) | 70.8 (56.8–89.6) | 18.90 (3.78) | 17.8 (13–26) |
| Creatinine (mg/dL) | 0.87 (0.10) | 0.85 (0.69–1.10) | 0.38 (0.07) | 0.36 (0.28–0.52) |
| eGFR (mL/min/1.73 m2) | 109.3 (13.30) | 112.0 (80–133) | 119.4 (16.15) | 121.5 (90–152) |
| Gender (n,%) | Male (32, 100) | Female (0, 0) | Male (19, 63) | Female (11, 37) |
| Structural Parameters | Inter-Individual Variability (IIV) | |||
|---|---|---|---|---|
| Parameter | Estimate (%RSE) | Parameter | Estimate (%RSE) | Shrinkage (%) |
| KA (h−1) | 4.21 (5) | IIV of KA (CV%) | 112.7 (13) | 17.2 |
| CL (L/h) | 28.0 (4) | IIV of CL (CV%) | 22.5 (12) | 14.5 |
| V (L) | 103.0 (5) | IIV of V (CV%) | 22.0 (21) | 17.8 |
| ALAG (h) | 0.27 (5) | IIV of ALAG | 32.4 (20) | 21.3 |
| Exponent of CL | 0.75 fixed | CORR of CL-V | 0.65 (25) | |
| Exponent of V | 1.0 fixed | CORR of CL-ALAG | 0.47 (18) | |
| Residual variability | ||||
| Proportional error | 10.3 (9) | Additive error | 0.1 fixed | |
| Body Weight (kg) | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Recommended dose based on | Cmax | 1.6 | 1.7 | 1.9 | 2.0 | 2.1 | 2.3 | 2.4 | 2.6 | 2.7 | 2.9 | 3.0 |
| AUClast | 2.3 | 2.5 | 2.7 | 2.8 | 3.0 | 3.1 | 3.3 | 3.5 | 3.6 | 3.8 | 3.9 | |
| Body weight (kg) | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | |
| Recommended dose based on | Cmax | 3.2 | 3.3 | 3.4 | 3.6 | 3.7 | 3.9 | 4.0 | 4.1 | 4.3 | 4.4 | 4.6 |
| AUClast | 4.0 | 4.2 | 4.3 | 4.5 | 4.6 | 4.8 | 4.9 | 5.0 | 5.2 | 5.3 | 5.4 | |
| Parameter | Initial Value | Final Values | References |
|---|---|---|---|
| Physico-chemical properties | |||
| Molecular weight (g/mol) | 388.88 | DrugBank | |
| LogP | 0.55 | Chemaxon (in silico) | |
| pKa | 4.10/9.39 | Chemaxon (in silico) | |
| Fraction unbound | 0.45 | Talion label [6], NIH (NCATS) | |
| Water Solubility (mg/mL) | 40.2 | Paper (in vitro) [25] | |
| Pharmacokinetic properties | |||
| Absorption | |||
| Intestinal permeability (cm/s) | 5.0 × 10−4 | 3.04 × 10−4 | Paper (in vitro/in vivo) [20], fitted to data |
| Weibull absorption | (Tablet, Dry syrup) | Parameter identification by PK-Sim | |
| Dissolution time (min) | 85, 32.63 | ||
| Lag time (min) | 0, 28.40 | ||
| Dissolution shape | 0.84, 0.55 | ||
| Distribution | |||
| P-gp (ABCB1), Km (umol/L) | 1.25 | Paper (in vivo) [2] | |
| P-gp (ABCB1), Kcat (1/s) | 6.47 | 5.41 | Paper (in vivo) [2] Parameter identification by PK-Sim |
| Blood to plasma ratio † | 0.69 | Calculated by PK-Sim | |
| Partition coefficient † | 0.32 | Calculated by PK-Sim | |
| Elimination | |||
| Tubular secretion (L/min) | 0.7 | 1.33/* 0.67 | Fitted to data |
| CYP-related parameters | None | DrugBank, Bepreve label [5] |
| PK Parameters | ||
|---|---|---|
| Age (Year) | AUClast (H·ng/mL) (5th Percentile–95th Percentile) | Cmax (ng/mL) (5th Percentile–95th Percentile) |
| 2 | 463.67 (355.96–675.47) | 85.46 (53.11–123.77) |
| 3 | 426.64 (329.97–566.67) | 82.08 (53.40–119.54) |
| 4 | 373.38 (289.31–506.73) | 74.88 (46.50–108.20) |
| 5 | 319.45 (239.37–456.62) | 64.70 (40.80–94.42) |
| 6 | 281.81 (217.15–393.55) | 56.68 (38.84–88.98) |
| Age (Year) | * Weight (kg) Median (5th Percentile–95th Percentile) | Based on AUClast | Based on Cmax | ||
|---|---|---|---|---|---|
| PBPK | PopPK † | PBPK | PopPK † | ||
| 2 | 14.0 (13.1–15.4) | 2.4 | 3.0 | 3.1 | 2.1 |
| 3 | 14.4 (13.4–16.4) | 2.7 | 3.0 | 3.3 | 2.2 |
| 4 | 15.9 (14.2–18.6) | 3.0 | 3.3 | 3.5 | 2.4 |
| 5 | 17.9 (15.8–20.8) | 3.5 | 3.6 | 4.1 | 2.7 |
| 6 | 19.6 (17.0–23.2) | 4.0 | 3.8 | 4.7 | 3.0 |
| Number of Samples | PopPK | PBPK | † p-Value | |
|---|---|---|---|---|
| Prediction error | 60 (Total) | 750.6 ± 1574.8 | 725.0 ± 2533.1 | 0.95 |
| 30 (Absorption period) | 1489.0 ± 1979.1 | 1427.8 ± 3468.6 | 0.93 | |
| 30 (Elimination period) | 12.2 ± 17.5 | 22.0 ± 39.3 | 0.22 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, S.; Jin, B.H.; Kim, C.O.; Park, K.; Park, M.S.; Chae, D. Pharmacokinetic Modeling of Bepotastine for Determination of Optimal Dosage Regimen in Pediatric Patients with Allergic Rhinitis or Urticaria. Pharmaceutics 2024, 16, 334. https://doi.org/10.3390/pharmaceutics16030334
Yoon S, Jin BH, Kim CO, Park K, Park MS, Chae D. Pharmacokinetic Modeling of Bepotastine for Determination of Optimal Dosage Regimen in Pediatric Patients with Allergic Rhinitis or Urticaria. Pharmaceutics. 2024; 16(3):334. https://doi.org/10.3390/pharmaceutics16030334
Chicago/Turabian StyleYoon, Sukyong, Byung Hak Jin, Choon Ok Kim, Kyungsoo Park, Min Soo Park, and Dongwoo Chae. 2024. "Pharmacokinetic Modeling of Bepotastine for Determination of Optimal Dosage Regimen in Pediatric Patients with Allergic Rhinitis or Urticaria" Pharmaceutics 16, no. 3: 334. https://doi.org/10.3390/pharmaceutics16030334