
Influence of Photosensitizer on Photodynamic Therapy for Peri-Implantitis: A Systematic Review

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Information
2.3. Search Algorithms
2.4. Studys Selection
2.5. Data Extraction
2.6. Risk of Bias in Individual Studies
3. Results
3.1. Study Characteristics and Results of Individual Studies
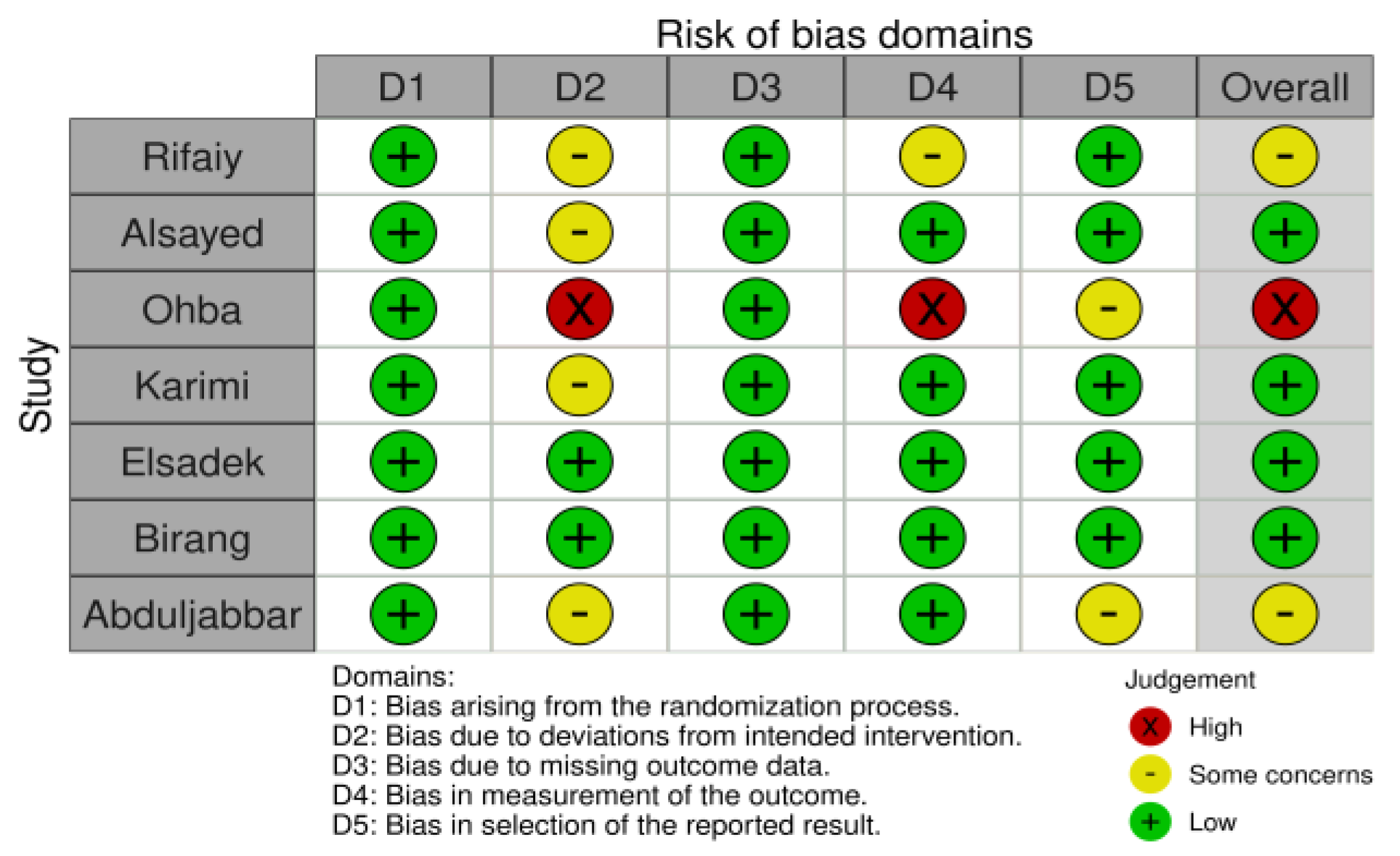
3.2. Risk of Bias
3.3. Certainty of Evidence
3.4. Photosensitizers
4. Discussion
4.1. Sounding Depth Index
4.2. Gingival Bleeding Index
4.3. Plaque Index
4.4. Microbiological Analyzes
4.5. Comparative Results
4.6. Efficacy of PDT in Smoking Patients
4.7. Efficacy of PDT in Diabetic Patients
4.8. Side Effects and Safety
4.9. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Berglundh, T.; Persson, L.; Klinge, B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J. Clin. Periodontol. 2002, 29, 197–212. [Google Scholar] [CrossRef]
- Almohareb, T.; Alhamoudi, N.; Al Deeb, M.; Bin-Shuwaish, M.S.; Mokeem, S.A.; Saad Shafqat, S.; Vohra, F.; Abduljabbar, T. Clinical efficacy of photodynamic therapy as an adjunct to mechanical debridement in the treatment of per-implantitis with abscess. Photodiagnosis Photodyn. Ther. 2020, 30, 101750. [Google Scholar] [CrossRef]
- Diaz, P.; Gonzalo, E.; Villagra, L.J.G.; Miegimolle, B.; Suarez, M.J. What is the prevalence of peri-implantitis? A systematic review and meta-analysis. BMC Oral Health 2022, 22, 449. [Google Scholar] [CrossRef]
- Ahmed, P.; Bukhari, I.A.; Albaijan, R.; Sheikh, S.A.; Vohra, F. The effectiveness of photodynamic and antibiotic gel therapy as an adjunct to mechanical debridement in the treatment of peri-implantitis among diabetic patients. Photodiagnosis Photodyn. Ther. 2020, 32, 102077. [Google Scholar] [CrossRef]
- Sanhueza, C.; Hermosilla, J.; Klein, C.; Chaparro, A.; Valdivia-Gandur, I.; Beltrán, V.; Acevedo, F. Osteoinductive Electrospun Scaffold Based on PCL-Col as a Regenerative Therapy for Peri-Implantitis. Pharmaceutics 2023, 15, 1939. [Google Scholar] [CrossRef]
- Parlar, A.; Bosshardt, D.D.; Çetiner, D.; Schafroth, D.; Ünsal, B.; Haytaç, C.; Lang, N.P. Effects of decontamination and implant surface characteristics on re-osseointegration following treatment of peri-implantitis. Clin. Oral Implant. Res. 2009, 20, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Mulla, M.; Mulla, M.; Hegde, S.; Koshy, A.V. In vitro assessment of the effect of probiotic lactobacillus reuteri on peri-implantitis microflora. BMC Oral Health 2021, 21, 408. [Google Scholar] [CrossRef] [PubMed]
- Socransky, S.S.; Haffajee, A.D. Periodontal microbial ecology. Periodontol. 2000 2005, 38, 135–187. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A. Microbiology and antimicrobial therapy of peri-implantitis. Periodontol. 2000 2002, 28, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.-L. Peri-implantitis. J. Clin. Periodontol. 2018, 45, S246—S266. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A.; Lang, N.P. Microbial aspects of implant dentistry. Periodontol. 2000 1994, 4, 74–80. [Google Scholar] [CrossRef]
- Persson, G.R.; Renvert, S. Cluster of Bacteria Associated with Peri-Implantitis. Clin. Implant Dent. Relat. Res. 2013, 16, 783–793. [Google Scholar] [CrossRef]
- Eick, S.; Markauskaite, G.; Nietzsche, S.; Laugisch, O.; Salvi, G.E.; Sculean, A. Effect of photoactivated disinfection with a light-emitting diode on bacterial species and biofilms associated with periodontitis and peri-implantitis. Photodiagnosis Photodyn. Ther. 2013, 10, 156–167. [Google Scholar] [CrossRef]
- Genco, R.; Kornman, K.; Williams, R.; Offenbacher, S.; Zambon, J.J.; Ishikawa, I.; Listgarten, M.; Michalowicz, B.; Page, R.; Schenkein, H.; et al. Periodontal diseases: Pathogenesis and microbial factors. J. Am. Dent. Assoc. 1998, 129, 58-S–62-S. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Nguyen, K.-A.; Potempa, J. Dichotomy of gingipains action as virulence factors: From cleaving substrates with the precision of a surgeon’s knife to a meat chopper-like brutal degradation of proteins. Periodontol. 2000 2010, 54, 15–44. [Google Scholar] [CrossRef] [PubMed]
- Potempa, J.; Sroka, A.; Imamura, T.; Travis, J. Gingipains, the Major Cysteine Proteinases and Virulence Factors of Porphyromonas gingivalis: Structure, Function and Assembly of Multidomain Protein Complexes. Curr. Protein Pept. Sci. 2003, 4, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, S.; Berglundh, T.; Genco, R.; Aass, A.M.; Demirel, K.; Derks, J.; Figuero, E.; Giovannoli, J.L.; Goldstein, M.; Lambert, F.; et al. Primary prevention of peri-implantitis: Managing peri-implant mucositis. J. Clin. Periodontol. 2015, 42, S152—S157. [Google Scholar] [CrossRef] [PubMed]
- Henderson, B.; Nair, S.P.; Ward, J.M.; Wilson, M. Molecular Pathogenicity of the Oral Opportunistic PathogenActinobacillus actinomycetemcomitans. Annu. Rev. Microbiol. 2003, 57, 29–55. [Google Scholar] [CrossRef] [PubMed]
- Shibli, J.A.; Melo, L.; Ferrari, D.S.; Figueiredo, L.C.; Faveri, M.; Feres, M. Composition of supra- and subgingival biofilm of subjects with healthy and diseased implants. Clin. Oral Implant. Res. 2008, 19, 975–982. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Persson, G.R.; Pirih, F.Q.; Camargo, P.M. Peri-implant health, peri-implant mucositis, and peri-implantitis: Case definitions and diagnostic considerations. J. Clin. Periodontol. 2018, 45, S278–S285. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L.J.A.; Salvi, G.E. Peri-implant mucositis. J. Clin. Periodontol. 2018, 45, S237–S245. [Google Scholar] [CrossRef] [PubMed]
- Zitzmann, N.U.; Abrahamsson, I.; Berglundh, T.; Lindhe, J. Soft tissue reactions to plaque formation at implant abutments with different surface topography. J. Clin. Periodontol. 2002, 29, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.O.; Takenaka-Martinez, S.; Cota, L.O.M.; Ferreira, S.D.; Silva, G.L.M.; Costa, J.E. Peri-implant disease in subjects with and without preventive maintenance: A 5-year follow-up. J. Clin. Periodontol. 2011, 39, 173–181. [Google Scholar] [CrossRef]
- Sahrmann, P.; Gilli, F.; Wiedemeier, D.B.; Attin, T.; Schmidlin, P.R.; Karygianni, L. The Microbiome of Peri-Implantitis: A Systematic Review and Meta-Analysis. Microorganisms 2020, 8, 661. [Google Scholar] [CrossRef]
- Mongardini, C.; Pilloni, A.; Farina, R.; Di Tanna, G.; Zeza, B. Adjunctive efficacy of probiotics in the treatment of experimental peri-implant mucositis with mechanical and photodynamic therapy: A randomized, cross-over clinical trial. J. Clin. Periodontol. 2017, 44, 410–417. [Google Scholar] [CrossRef]
- Castano, A.P.; Demidova, T.N.; Hamblin, M.R. Mechanisms in photodynamic therapy: Part one—Photosensitizers, photochemistry and cellular localization. Photodiagnosis Photodyn. Ther. 2004, 1, 279–293. [Google Scholar] [CrossRef] [PubMed]
- Konopka, K.; Goslinski, T. Photodynamic Therapy in Dentistry. J. Dent. Res. 2007, 86, 694–707. [Google Scholar] [CrossRef]
- Dalvi, S.; Benedicenti, S.; Sălăgean, T.; Bordea, I.R.; Hanna, R. Effectiveness of Antimicrobial Photodynamic Therapy in the Treatment of Periodontitis: A Systematic Review and Meta-Analysis of In Vivo Human Randomized Controlled Clinical Trials. Pharmaceutics 2021, 13, 836. [Google Scholar] [CrossRef]
- Silva, T.; Lunardi, A.J.L.; Barros, A.C.S.M.; Mandetta, A.R.H.; Grudzien, E.; San-Martín, M.; Horliana, A.C.R.T.; Bussadori, S.K.; Motta, L.J. Application of Photodynamic Therapy in Pediatric Dentistry: Literature Review. Pharmaceutics 2023, 15, 2335. [Google Scholar] [CrossRef]
- Zeza, B.; Farina, R.; Pilloni, A.; Mongardini, C. Clinical outcomes of experimental gingivitis and peri-implant mucositis treatment with professionally administered plaque removal and photodynamic therapy. Int. J. Dent. Hyg. 2017, 16, e58–e64. [Google Scholar] [CrossRef]
- Alresayes, S.; Al Deeb, M.; Mokeem, S.A.; Al-Hamoudi, N.; Ahmad, P.; Al-Aali, K.A.; Vohra, F.; Abduljabbar, T. Influence of body fat in patients with dental implant rehabilitation treated with adjunctive photodynamic therapy. Photodiagnosis Photodyn. Ther. 2020, 31, 101831. [Google Scholar] [CrossRef]
- Lang, N.P.; Berglundh, T. Periimplant diseases: Where are we now?—Consensus of the Seventh European Workshop on Periodontology. J. Clin. Periodontol. 2011, 38, 178–181. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- A Declaração PRISMA 2020: Diretriz Atualizada Para Relatar Revisões Sistemáticas*. Available online: https://iris.paho.org/handle/10665.2/56882 (accessed on 11 October 2023).
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; Hooft, L.; et al. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies. JAMA 2018, 319, 388. [Google Scholar] [CrossRef]
- Birang, E.; Talebi Ardekani, M.R.; Rajabzadeh, M.; Sarmadi, G.; Birang, R.; Gutknecht, N. Evaluation of Effectiveness of Photodynamic Therapy With Low-level Diode Laser in Nonsurgical Treatment of Peri-implantitis. J. Lasers Med. Sci. 2017, 8, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Abduljabbar, T. Effect of mechanical debridement with adjunct antimicrobial photodynamic therapy in the treatment of peri-implant diseases in type-2 diabetic smokers and non-smokers. Photodiagnosis Photodyn. Ther. 2017, 17, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Al Rifaiy, M.Q.; Qutub, O.A.; Alasqah, M.N.; Al-Sowygh, Z.H.; Mokeem, S.A.; Alrahlah, A. Effectiveness of adjunctive antimicrobial photodynamic therapy in reducing peri -implant inflammatory response in individuals vaping electronic cigarettes: A randomized controlled clinical trial. Photodiagnosis Photodyn. Ther. 2018, 22, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Alsayed, H.; Bukhari, I.A.; Alsaif, R.; Vohra, F. Efficacy of indocyanine green and methylene blue mediated-photodynamic therapy on peri-implant outcomes among diabetics with peri-implant mucositis. Photodiagnosis Photodyn. Ther. 2023, 42, 103344. [Google Scholar] [CrossRef] [PubMed]
- Elsadek, M.F. Effectiveness of two photosensitizer-mediated photodynamic therapy for treating moderate peri-implant infections in type-II diabetes mellitus patients: A randomized clinical trial. Photodiagnosis Photodyn. Ther. 2023, 43, 103643. [Google Scholar] [CrossRef] [PubMed]
- Ohba, S.; Sato, M.; Noda, S.; Yamamoto, H.; Egahira, K.; Asahina, I. Assessment of safety and efficacy of antimicrobial photodynamic therapy for peri-implant disease. Photodiagnosis Photodyn. Ther. 2020, 31, 101936. [Google Scholar] [CrossRef] [PubMed]
- Karimi, M.R.; Hasani, A.; Khosroshahian, S. Efficacy of Antimicrobial Photodynamic Therapy as an Adjunctive to Mechanical Debridement in the Treatment of Peri-implant Diseases: A Randomized Controlled Clinical Trial. J. Lasers Med. Sci. 2016, 7, 139–145. [Google Scholar] [CrossRef]
- CONSORT 2010 Explanation and Elaboration: Updated Guidelines for Reporting Parallel Group Randomised Trials. Available online: https://pubmed.ncbi.nlm.nih.gov/20346624/ (accessed on 16 November 2023).
- Schnemann, H.J.; Oxman, A.D.; Vist, G.E.; Higgins, J.P.; Deeks, J.J.; Glasziou, P.; Guyatt, G.H. Interpreting Results and Drawing Conclusions. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Ltd.: Chichester, UK, 2008; pp. 359–387. [Google Scholar] [CrossRef]
- Aabed, K.; Moubayed, N.; BinShabaib, M.S.; ALHarthi, S.S. Is a single session of antimicrobial photodynamic therapy as an adjuvant to non-surgical scaling and root planing effective in reducing periodontal inflammation and subgingival presence of Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans in patients with periodontitis? Photodiagnosis Photodyn. Ther. 2022, 38, 102847. [Google Scholar] [CrossRef]
- Abdellatif, H.M.; Ali, D.; Divakar, D.D.; BinShabaib, M.S.; ALHarthi, S.S. Periodontal status and whole salivary adipokines after scaling and root planing with and without adjunct antimicrobial photodynamic therapy in obese patients with periodontitis. Photodiagnosis Photodyn. Ther. 2022, 40, 103112. [Google Scholar] [CrossRef] [PubMed]
- Abduljabbar, T. Effect of mechanical debridement with and without adjunct antimicrobial photodynamic therapy in the treatment of peri-implant diseases in prediabetic patients. Photodiagnosis Photodyn. Ther. 2017, 17, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Afrasiabi, S.; Partoazar, A.; Chiniforush, N.; Goudarzi, R. The Potential Application of Natural Photosensitizers Used in Antimicrobial Photodynamic Therapy against Oral Infections. Pharmaceuticals 2022, 15, 767. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.R.; Kamran, M.A.; Suleman, G.; Sharif, R.A.; Alamrey, A.A.M.; Sulaiman, S.A. Novel use of chloro-aluminum phthalocyanine assisted photodynamic therapy helps in periimplant healing among smoking patients. Photodiagnosis Photodyn. Ther. 2022, 41, 103193. [Google Scholar] [CrossRef]
- Al Amri, M.D.; Kellesarian, S.V.; Ahmed, A.; Al-Kheraif, A.A.; Romanos, G.E.; Javed, F. Efficacy of periimplant mechanical debridement with and without adjunct antimicrobial photodynamic therapy in patients with type 2 diabetes mellitus. Photodiagnosis Photodyn. Ther. 2016, 14, 166–169. [Google Scholar] [CrossRef]
- Al Deeb, M.; Alresayes, S.; Mokeem, S.A.; Alhenaki, A.M.; AlHelal, A.; Vohra, F.; Abduljabbar, T. Clinical peri-implant health and biological bone marker levels in tobacco users treated with photodynamic therapy. Photodiagnosis Photodyn. Ther. 2020, 31, 101821. [Google Scholar] [CrossRef] [PubMed]
- Al Deeb, M.; Alresayes, S.; Mokeem, S.A.; Alhenaki, A.M.; AlHelal, A.; Shafqat, S.S.; Vohra, F.; Abduljabbar, T. Clinical and immunological peri-implant parameters among cigarette and electronic smoking patients treated with photochemotherapy: A randomized controlled clinical trial. Photodiagnosis Photodyn. Ther. 2020, 31, 101800. [Google Scholar] [CrossRef] [PubMed]
- Al-Khureif, A.A.; Mohamed, B.A.; Siddiqui, A.Z.; Hashem, M.; Khan, A.A.; Divakar, D.D. Clinical, host-derived immune biomarkers and microbiological outcomes with adjunctive photochemotherapy compared with local antimicrobial therapy in the treatment of peri-implantitis in cigarette smokers. Photodiagnosis Photodyn. Ther. 2020, 30, 101684. [Google Scholar] [CrossRef]
- Herbert, D.; Thomas, M.; Stefan, W.; Marco, K.; Anton, S. Nonsurgical Antimicrobial Photodynamic Therapy in Moderate vs Severe Peri-Implant Defects: A Clinical Pilot Study. Quintessenz Verlags-GmbH, 15 de julho de 2013. Available online: https://www.quintessence-publishing.com/deu/de/article/840668/quintessence-international/2013/08/nonsurgical-antimicrobial-photodynamic-therapy-in-moderate-vs-severe-peri-implant-defects-a-clinical-pilot-study (accessed on 16 November 2023).
- Dörtbudak, O.; Haas, R.; Bernhart, T.; Mailath-Pokorny, G. Lethal photosensitization for decontamination of implant surfaces in the treatment of peri-implantitis. Clin. Oral Implant. Res. 2001, 12, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Albaker, A.M.; ArRejaie, A.S.; Alrabiah, M.; Al-Aali, K.A.; Mokeem, S.; Alasqah, M.N.; Vohra, F.; Abduljabbar, T. Effect of antimicrobial photodynamic therapy in open flap debridement in the treatment of peri-implantitis: A randomized controlled trial. Photodiagnosis Photodyn. Ther. 2018, 23, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Harmouche, L.; Courval, A.; Mathieu, A.; Petit, C.; Huck, O.; Severac, F.; Davideau, J.-L. Impact of tooth-related factors on photodynamic therapy effectiveness during active periodontal therapy: A 6-months split-mouth randomized clinical trial. Photodiagnosis Photodyn. Ther. 2019, 27, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Javed, F.; BinShabaib, M.S.; Alharthi, S.S.; Qadri, T. Role of mechanical curettage with and without adjunct antimicrobial photodynamic therapy in the treatment of peri-implant mucositis in cigarette smokers: A randomized controlled clinical trial. Photodiagnosis Photodyn. Ther. 2017, 18, 331–334. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author/Study Design | Clinical Parameters | Photosensitizer/Intervention | Results |
|---|---|---|---|
| Birang et al., (2017) [36] STUDY DESIGN n = 20, 10 M/10 F20 to 67 years old MI = 36.6 ± 9.7 years
Lasertherapy × PDT in individuals with primary peri-implantitis Follow-up: 6 weeks and 3 months | Probing pocket depth (PPD), papilla bleeding index (BOP), modified plaque index (PI) COLLECTION POINTS Collection points: distobuccal (DV), mesiobuccal (MV), distolingual (DL), mesiolingual (ML) Collection: initial, 6 weeks and 3 months | EmunDo INTERVENTION Initial—manual debridement (DM) with ultrasound (US) and DM with plastic curette, sodium bicarbonate jet in G1 and G2 G1—US + DM + PDT with EmunDo 90 s + irrigation with 0.9% saline solution + transgingival irradiation 30 s/300 mW + intra-pocket irradiation 30 s/300 mW + elimination of intra-pocket granulation tissue 30 s/300 mW 15 days—repeat the initial intervention Instructions for participants: Oral hygiene guidance (OHG) | G1 and G2 showed statistically significant improvements in bleeding on probing (p < 0.001), probing pocket depth (PPD) (p = 0.006) and modified plaque index (p < 0.001), without significant differences between the groups. Two groups (p > 0.05) and P. gingivalis (p = 0.015) in the control group significantly decreased. Laser therapy only significantly decreased P. gingivalis (p = 0.015) and differences in A. actinomycetemcomitans were threshold significant (p = 0.061). PDT significantly decreased A. actinomycetemcomitans (p = 0.022), T. forsythia (p = 0.038) and P. gingivalis (p= 0.050). Mann-Whitney test revealed no significant difference in changes in bacterial counts before and after treatment between treatment modalities (A. actinomycetemcomitans p = 0.846, P. gingival p = 0.503, P. intermediate p = 0.682, T. denticola p = 0.399 and T. forsythia p = 0.199) |
| Abduljabbar (2017) [37] STUDY DESIGN n = 64, all men
| BO, PD ≥ 4 mm COLLECTION POINTS DV, MV, DL, ML, V, P/L | Phenothiazine chloride INTERVENTION DM with US + adjuvant PDT with phenothiazine chloride 120 s + pocket irrigation with 3% hydrogen peroxide + irradiation with 600 nm/100 mW diode laser for 10 s in a single session + high-power liquid chromatography (HbA1c) at baseline and after 6 months (G1 + G2) Instructions to participants not reported | At baseline, BOP and PD ≥ 4 mm were comparable between subjects in groups 1 and 2. At 6-month follow-up, there was no statistically significant difference in BOP and PD ≥ 4 mm between patients in groups 1 and 2 compared to respective baseline values. HbA1c levels were comparable in all groups at all time intervals. HbA1c at baseline and 6 months later—G1—9.3% (start)/8.4 (6 months)—G2—8.7% (start)/8.4 (6 months)—BOP—G1—53, 3 ± 4.2% (start)/48.2 ± 3.6% (6 months)—G2—35.2 ± 3.1% (start)/33.1 ± 2.4% (6 months)—PD—G1—26.2 ± 3.7% (start)/25.1 ± 0.8% (6 months)—G2—29.5 ± 3.7% (start)/25.5 ± 1.4% (6 months) |
| Author/Study Design | Clinical Parameters | Photosensitizer/Intervention | Results |
|---|---|---|---|
| Al Rifaiy et al., (2018) [38] STUDY DESIGN n = 38, all men
| IP, BOP, PD COLLECTION POINTS DV, MV, DL, ML, buccal(V), palatal/lingual (P/L) | Methylene blue (TB) 0.005% INTERVENTION G1—DM + PDT with TB applied to the periodontal pocket with a 10 s wait + 60 s irradiation with a 670 nm/150 mW diode laser in a single application G2—DM with plastic curette Instructions for participants: OHG, guidelines for quitting smoking | Start—PI, BOP and peri-implant PD comparable between G1 and 2. After 12 weeks, statistically significant reduction in PI (p < 0.001) and PD (p < 0.001) between G1 and G2 patients compared to baseline. Significant reduction in IP (p < 0.001) and PD (p < 0.001) for G1 compared to G2 at 12 weeks. There was no statistically significant difference for BOP between groups at follow-up |
| Alsayed et al., (2023) [39] STUDY DESIGN n = 60, 35 M/25 F
Follow-up for 3 months | IP, PD, BOP, crest bone level (CBL) COLLECTION POINTS DV, MV, DL, ML, V, P/L CBL collection by bitewing digital radiographs | Indocyanine green (ICG) and methylene blue (MB) INTERVENTION G1—DM with plastic curette G2—DM + PDT with ICG 1 mg/mL, 60 s wait + irrigation (saline solution) + irradiation: (a) photobiomodulation tip in the 30 s papilla (6J), (b) tip of the bulb in the 10 s palatine groove and sulcus bottom lingual to coronal (4J), 810 nm/200 mW (continuous mode), single application G3—DM + PDT with MB, 60 s wait + irrigation (saline solution) + irradiation with 670 nm/140 mW (21 Jcm2), single application Instructions for participants: OHG, guidelines for using mouthwash with chlorhexidine gluconate (0.12%), twice a day, 60 s, to avoid the consumption of anti-inflammatories during the study | Mean changes between baseline and 3-month follow-up in peri-implant clinical-radiographic parameters were significantly different between control (PI: 12.42 ± 21.80%; BOP: 12.10 ± 19.30%; PD: 0.45 ± 0.41 mm; CBL:1.10 ± 1.02 mm) and test groups (ICG-mediated PDT [PI: 26.55 ± 25.80%; BOP: 28.77 ± 29.24%; PD: 0.84 ± 0.62 mm; CBL: 1.98 ± 1.85 mm] and MB-mediated PDT [PI: 27.24 ± 26.15%; BOP: 27.71 ± 28.16%; PD: 0.85 ± 0.63 mm; CBL: 1.95 ± 1.80 mm]); comparable differences observed in peri-implant PI, BOP, PD and CBL between G2 and G3 participants (p > 0.05). The proportions of T. forsythia were significantly reduced in G2 (4.78 × 104 CFU/mL) and G3 (4.76 × 104 CFU/mL) as compared to G1 (−4.40 × 103 CFU/mL) at 3-month follow-up (p = 0.02). No statistically significant differences were observed between the study groups in relation to the proportions of the other target bacteria species evaluated. For IL-6 (G 1: 210 ± 108; G2: 298 ± 165; G3: 277 ± 121 pg/mL; p = 0.03), IL-1β (G1: 101 ± 95; G2: 84 ± 98; G3: 86 ± 74 pg/mL; p = 0.02) and TNF-α (G1: 36 ± 121; G2: 385 ± 210; G3: 366 ± 198 pg/mL; p = 0.03) at PISF levels, a statistically significant reduction at the 3-month follow-up. |
| Elsadek (2023) [40] STUDY DESIGN n = 38
Follow-up: 3 months and 6 months | Plaque scores (PS), peri-implant probing scores (PPS), bleeding scores (BS), estimated peri-implant bone loss (PIBL) linearly from 2 mm below the abutment interface to the most level of the crest of the bone. COLLECTION POINTS Three lingual and three buccal surfaces. | G1—Indocyanine green solution (ICG) 1 mg/mL/G2—methylthionine chloride (MTC) INTERVENTION G1—DM with US and scaling and root planing with curette + PDT with ICG with a wait of 60 s + irradiation 810/300 mW, with a fluence of 56 Jcm2 pulsed mode 30 s with continuous vertical movement, single application G2—DM with US and scaling and root planing with curette + PDT with MTC waiting for 60 s + removal of excess dye gently + irradiation with a 660 ± 10 nm/100 mW diode laser with the tip inserted into the depth of the pocket and moved circumferentially around the implant, 120 s/location. Each irradiation point about 0.4 cm2, radiant exposure 30 Jcm2, irradiance 0.25 Wcm2 1 point every 3 mm, single application Instructions to participants not reported | Significant reduction for PS, BS and PPS in all groups tested at each follow-up visit compared to baseline values (p < 0.05). Substantial decrease in PIBL in all patients in the group at the 6-month follow-up compared to the 3-month follow-up (p < 0.05). Levels of IL-6 and TNF-α, substantial reduction in all study groups up to 6 months from their initial scores (p < 0.05). No changes in AGEs levels were observed in any group at any of the visits (p > 0.05). |
| Author/Study Design | Clinical Parameters | Photosensitizer/Intervention | Results |
|---|---|---|---|
| Ohba et al., (2020) [41] STUDY DESIGN n = 21 implants
Follow-up for 7 ± 2 days | Pus discharge volume, BOP, IP COLLECTION POINTS Not mentioned | Toluidine blue (TB) 0.1 mg/mL INTERVENTION TB 0.1 mg/mL with 630 nm LED (620–640 nm), in two applications in the same session G1—irrigation with 5 mL saline solution G2—irrigation with 5 mL saline solution + PDT with TB 0.1 mg/mL without waiting time + irradiation with 630 nm LED (620–640 nm buccal/labial and lingual/palatal sides 30 s + irrigation with 5 mL of solution saline. Repeat the procedure once more, in the same session. Evaluations in 7 ± 2 days Instructions to participants not reported | Pus discharge decreased in 7 of 12 implants (58.3%) in G2 and in 2 of 13 implants (15.4%) in G1. Fisher’s exact test—PDT resulted in a statistically significant decrease in pus discharge compared to irrigation alone (p = 0.0414)” |
| Karimi et al., (2016) [42] STUDY DESIGN n = 30 implants, 10 individuals 2 M and 8 F
G2—DM + PDT/MI = 52.8 years Randomized clinical trial Follow-up for 3 months | Gingival index (GI), BP, PD, MR, clinical attachment loss (CAL) COLLECTION POINTS PPD and CAL DV, MV, DL, ML, V, P/L, buccal and lingual | Toluidine blue (TB) 0.01% INTERVENTION TB 0.01% 180 s with 630 diode laser nm/2.00 mW/cm2 in single application G1—DM with plastic curette + irrigation of the pocket with sterile saline solution G2—DM with plastic curette + irrigation of the pocket with sterile saline solution + PDT with TB waiting time 180 s + irradiation in 6 niches, for 20 s each (total 120 s). Instructions for participants: Individualized OHG, depending on the type of prosthesis Clinical parameters measured immediately before treatment and re-evaluated 1.5 and 3 months after treatment, using a plastic probe | Significant differences in PPD, CAL, BOP, and GI at each time point between the two groups. There were no statistically significant changes in relation to any of the control group parameters. Complete resolution of BOP within 3 months achieved in 100% of test implants. At 1.5 and 3 months, there were differences in the mean probing depth and CAL gain measurements in the implants in the test group |
| Author, Year | Reason for Exclusion |
|---|---|
| 1. Aabed et al., 2022 [45] | 1 |
| 2. Abdellatif et al., 2022 [46] | 1 |
| 3. Abduljabbar, 2017 [47] | 2 |
| 4. Afrasiabi et al., 2022 [48] | 3 |
| 5. Ahmed et al., 2022 [49] | 4 |
| 6. Ahmed et al., 2020 [4] | 5 |
| 7. Al Amri et al., 2016 [50] | 6 |
| 8. Al Deeb et al., 2020 [51] | 6 |
| 9. Al Deeb et al., 2020 [52] | 7 |
| 10. Al-Khureif et al., 2020 [53] | 5 |
| 11. Herbert et al., 2013 [54] | 10 |
| 12. Dörtbudak et al., 2001 [55] | 8 |
| 13. Albaker et al., 2018 [56] | 9 |
| 14. Harmouche et al., 2019 [57] | 1 |
| 15. Javed et al., 2017 [58] | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schweigert, T.B.M.O.; Afonso, J.P.R.; da Palma, R.K.; Oliveira-Silva, I.; Silva, C.H.M.; Jirjos, E.I.; Freitas Júnior, W.R.; Insalaco, G.; Guedes, O.A.; Oliveira, L.V.F. Influence of Photosensitizer on Photodynamic Therapy for Peri-Implantitis: A Systematic Review. Pharmaceutics 2024, 16, 307. https://doi.org/10.3390/pharmaceutics16030307
Schweigert TBMO, Afonso JPR, da Palma RK, Oliveira-Silva I, Silva CHM, Jirjos EI, Freitas Júnior WR, Insalaco G, Guedes OA, Oliveira LVF. Influence of Photosensitizer on Photodynamic Therapy for Peri-Implantitis: A Systematic Review. Pharmaceutics. 2024; 16(3):307. https://doi.org/10.3390/pharmaceutics16030307
Chicago/Turabian StyleSchweigert, Thaís B. M. O., João P. R. Afonso, Renata K. da Palma, Iransé Oliveira-Silva, Carlos H. M. Silva, Elias Ilias Jirjos, Wilson Rodrigues Freitas Júnior, Giuseppe Insalaco, Orlando A. Guedes, and Luís V. F. Oliveira. 2024. "Influence of Photosensitizer on Photodynamic Therapy for Peri-Implantitis: A Systematic Review" Pharmaceutics 16, no. 3: 307. https://doi.org/10.3390/pharmaceutics16030307