

Drug Exposure and Susceptibility of Pyrazinamide Correlate with Treatment Response in Pyrazinamide-Susceptible Patients with Multidrug-Resistant Tuberculosis
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. MDR-TB Treatment and Information Collection
2.3. Drug Susceptibility Testing
2.4. Drug Exposure
2.5. Definitions of Treatment Response and Main Variables
2.6. Statistical Analyses
3. Results
3.1. Study Population
3.2. Pyrazinamide Exposure and Susceptibility
3.3. Treatment Responses
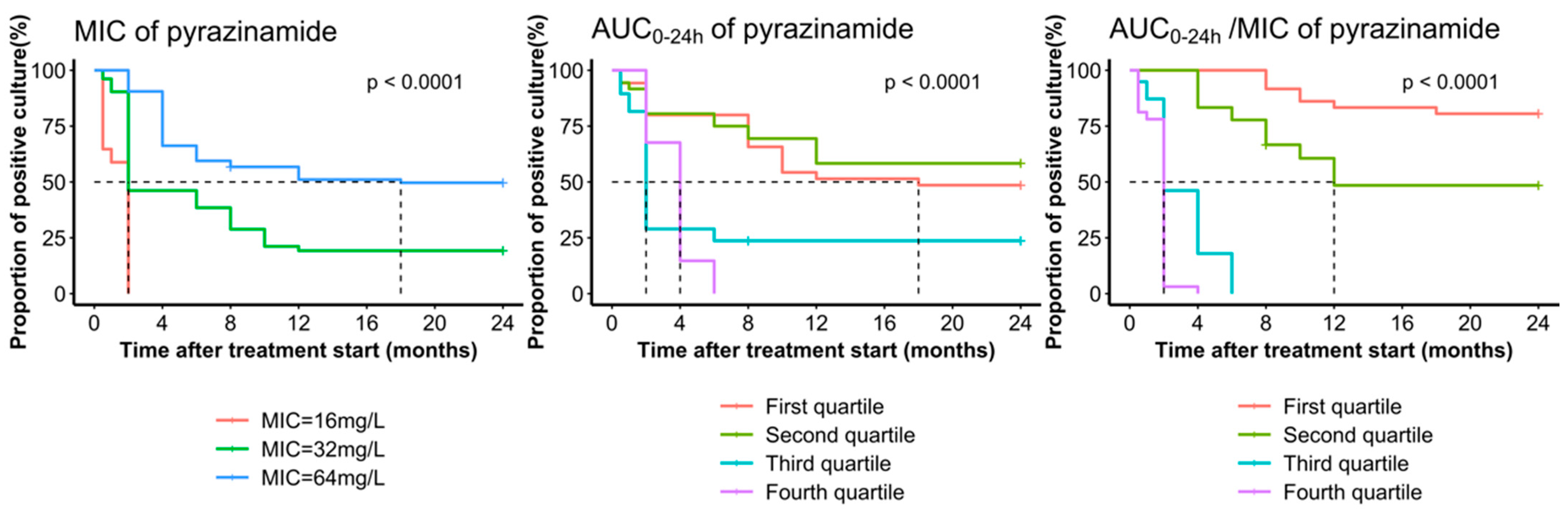
3.4. The Correlation between Exposure and Susceptibility of Pyrazinamide and Treatment Responses
3.5. CART Analysis of Pyrazinamide Exposure/Susceptibility Target
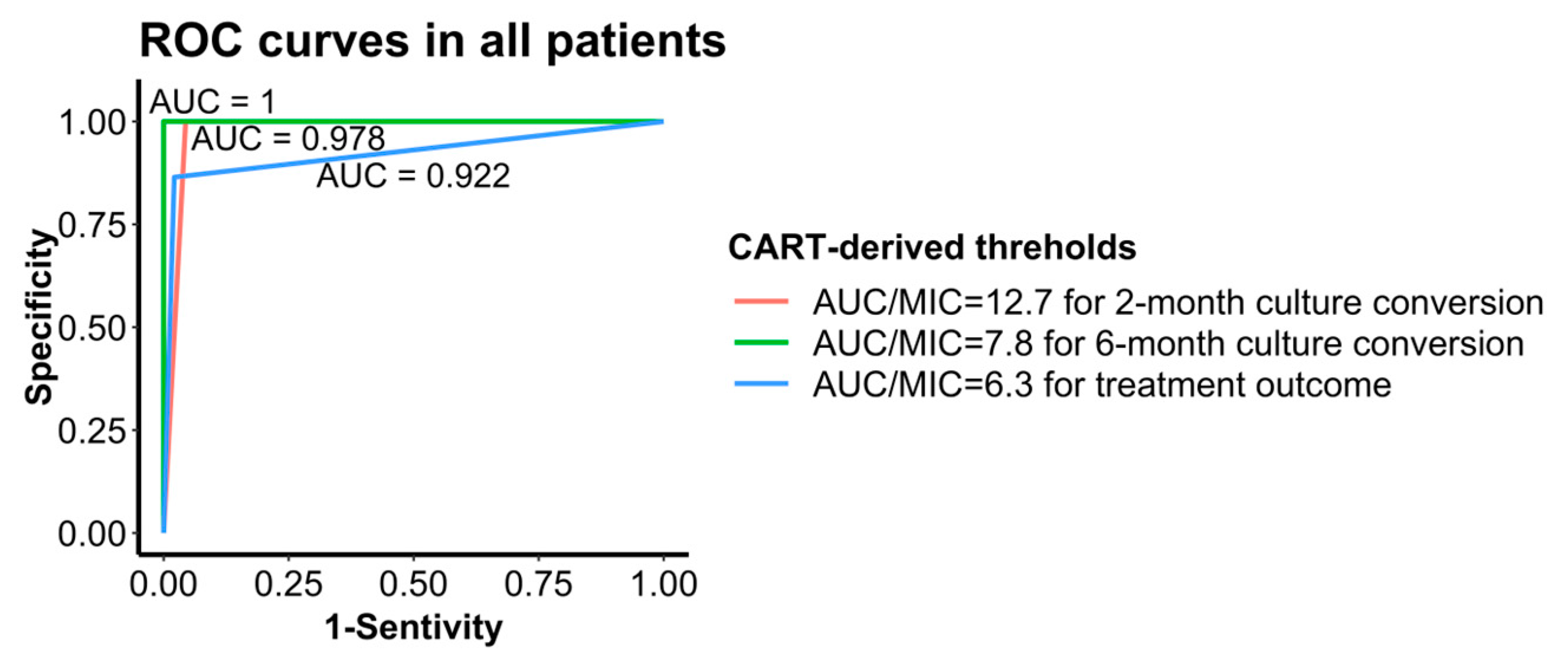
3.6. CART-Derived Threshold Performance Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bagcchi, S. WHO’s Global Tuberculosis Report 2022. Lancet Microbe 2023, 4, e20. [Google Scholar] [CrossRef]
- Aguilar Diaz, J.M.; Abulfathi, A.A.; Te Brake, L.H.; van Ingen, J.; Kuipers, S.; Magis-Escurra, C.; Raaijmakers, J.; Svensson, E.M.; Boeree, M.J. New and Repurposed Drugs for the Treatment of Active Tuberculosis: An Update for Clinicians. Respiration 2023, 102, 83–100. [Google Scholar] [CrossRef]
- World Health Organization. WHO Treatment Guidelines for Drug-Resistant Tuberculosis; 2016 update; World Health Organization: Geneva, Switzerland, 2016; ISBN 978-92-4-154963-9. [Google Scholar]
- World Health Organization. WHO Consolidated Guidelines on Tuberculosis: Module 4: Treatment: Drug-Resistant Tuberculosis Treatment; World Health Organization: Geneva, Switzerland, 2020; ISBN 978-92-4-000704-8. [Google Scholar]
- Zhang, Y.; Yew, W.W.; Barer, M.R. Targeting Persisters for Tuberculosis Control. Antimicrob. Agents Chemother. 2012, 56, 2223–2230. [Google Scholar] [CrossRef]
- Zhang, N.; Savic, R.M.; Boeree, M.J.; Peloquin, C.A.; Weiner, M.; Heinrich, N.; Bliven-Sizemore, E.; Phillips, P.P.J.; Hoelscher, M.; Whitworth, W.; et al. Optimising Pyrazinamide for the Treatment of Tuberculosis. Eur. Respir. J. 2021, 58, 2002013. [Google Scholar] [CrossRef]
- Sun, F.; Li, Y.; Chen, Y.; Guan, W.; Jiang, X.; Wang, X.; Ren, P.; Li, J.; Shi, J.; He, G.; et al. Introducing Molecular Testing of Pyrazinamide Susceptibility Improves Multidrug-Resistant Tuberculosis Treatment Outcomes: A Prospective Cohort Study. Eur. Respir. J. 2019, 53, 1801770. [Google Scholar] [CrossRef]
- Forsman, L.D.; Jonsson, J.; Wagrell, C.; Werngren, J.; Mansjö, M.; Wijkander, M.; Groenheit, R.; Hammar, U.; Giske, C.G.; Schön, T.; et al. Minimum Inhibitory Concentrations of Fluoroquinolones and Pyrazinamide Susceptibility Correlate to Clinical Improvement in Multidrug-Resistant Tuberculosis Patients: A Nationwide Swedish Cohort Study Over 2 Decades. Clin. Infect. Dis. 2019, 69, 1394–1402. [Google Scholar] [CrossRef]
- Zheng, X.; Davies Forsman, L.; Bao, Z.; Xie, Y.; Ning, Z.; Schön, T.; Bruchfeld, J.; Xu, B.; Alffenaar, J.-W.; Hu, Y. Drug Exposure and Susceptibility of Second-Line Drugs Correlate with Treatment Response in Patients with Multidrug-Resistant Tuberculosis: A Multicentre Prospective Cohort Study in China. Eur. Respir. J. 2022, 59, 2101925. [Google Scholar] [CrossRef]
- Alsultan, A.; Savic, R.; Dooley, K.E.; Weiner, M.; Whitworth, W.; Mac Kenzie, W.R.; Peloquin, C.A. Population Pharmacokinetics of Pyrazinamide in Patients with Tuberculosis. Antimicrob. Agents Chemother. 2017, 61, e02625-16. [Google Scholar] [CrossRef]
- Xavier, R.M.; Sharumathi, S.M.; Kanniyappan Parthasarathy, A.; Mani, D.; Mohanasundaram, T. Limited Sampling Strategies for Therapeutic Drug Monitoring of Anti-Tuberculosis Medications: A Systematic Review of Their Feasibility and Clinical Utility. Tuberculosis 2023, 141, 102367. [Google Scholar] [CrossRef]
- Donald, P.R.; Maritz, J.S.; Diacon, A.H. Pyrazinamide Pharmacokinetics and Efficacy in Adults and Children. Tuberculosis 2012, 92, 1–8. [Google Scholar] [CrossRef]
- Pasipanodya, J.G.; McIlleron, H.; Burger, A.; Wash, P.A.; Smith, P.; Gumbo, T. Serum Drug Concentrations Predictive of Pulmonary Tuberculosis Outcomes. J. Infect. Dis. 2013, 208, 1464–1473. [Google Scholar] [CrossRef]
- Kuhlin, J.; Davies Forsman, L.; Mansjö, M.; Jonsson Nordvall, M.; Wijkander, M.; Wagrell, C.; Jonsson, J.; Groenheit, R.; Werngren, J.; Schön, T.; et al. Genotypic Resistance of Pyrazinamide but Not Minimum Inhibitory Concentration Is Associated with Longer Time to Sputum Culture Conversion in Patients with Multidrug-Resistant Tuberculosis. Clin. Infect. Dis. 2021, 73, e3511–e3517. [Google Scholar] [CrossRef]
- Chang, K.C.; Yew, W.W.; Zhang, Y. Pyrazinamide Susceptibility Testing in Mycobacterium Tuberculosis: A Systematic Review with Meta-Analyses. Antimicrob. Agents Chemother. 2011, 55, 4499–4505. [Google Scholar] [CrossRef]
- Whitfield, M.G.; Soeters, H.M.; Warren, R.M.; York, T.; Sampson, S.L.; Streicher, E.M.; van Helden, P.D.; van Rie, A. A Global Perspective on Pyrazinamide Resistance: Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0133869. [Google Scholar] [CrossRef]
- Daneau, G.; Gumusboga, M.; De Rijk, P.; Trebucq, A.; Rigouts, L.; Van Deun, A.; de Jong, B.C. The Majority of Patients with Multidrug-Resistant Tuberculosis in Sub-Saharan Africa Present a Concomitant Resistance to Pyrazinamide. Int. J. Mycobacteriol. 2016, 5 (Suppl. S1), S46–S47. [Google Scholar] [CrossRef]
- Shi, D.; Zhou, Q.; Xu, S.; Zhu, Y.; Li, H.; Xu, Y. Pyrazinamide Resistance and pncA Mutation Profiles in Multidrug Resistant Mycobacterium Tuberculosis. Infect. Drug Resist. 2022, 15, 4985–4994. [Google Scholar] [CrossRef]
- Peloquin, C. The Role of Therapeutic Drug Monitoring in Mycobacterial Infections. Microbiol. Spectr. 2017, 5. [Google Scholar] [CrossRef]
- Verbeeck, R.K.; Günther, G.; Kibuule, D.; Hunter, C.; Rennie, T.W. Optimizing Treatment Outcome of First-Line Anti-Tuberculosis Drugs: The Role of Therapeutic Drug Monitoring. Eur. J. Clin. Pharmacol. 2016, 72, 905–916. [Google Scholar] [CrossRef]
- Chigutsa, E.; Pasipanodya, J.G.; Visser, M.E.; van Helden, P.D.; Smith, P.J.; Sirgel, F.A.; Gumbo, T.; McIlleron, H. Impact of Nonlinear Interactions of Pharmacokinetics and MICs on Sputum Bacillary Kill Rates as a Marker of Sterilizing Effect in Tuberculosis. Antimicrob. Agents Chemother. 2014, 59, 38–45. [Google Scholar] [CrossRef]
- Zheng, X.; Bao, Z.; Forsman, L.D.; Hu, Y.; Ren, W.; Gao, Y.; Li, X.; Hoffner, S.; Bruchfeld, J.; Alffenaar, J.-W. Drug Exposure and Minimum Inhibitory Concentration Predict Pulmonary Tuberculosis Treatment Response. Clin. Infect. Dis. 2021, 73, e3520–e3528. [Google Scholar] [CrossRef]
- Springer, B.; Lucke, K.; Calligaris-Maibach, R.; Ritter, C.; Böttger, E.C. Quantitative Drug Susceptibility Testing of Mycobacterium Tuberculosis by Use of MGIT 960 and EpiCenter Instrumentation. J. Clin. Microbiol. 2009, 47, 1773–1780. [Google Scholar] [CrossRef]
- Mustazzolu, A.; Iacobino, A.; Giannoni, F.; Piersimoni, C.; Italian Multicentre Study on Resistance to Antituberculosis Drugs (SMIRA) Group; Fattorini, L. Improved Bactec MGIT 960 Pyrazinamide Test Decreases Detection of False Mycobacterium Tuberculosis Pyrazinamide Resistance. J. Clin. Microbiol. 2017, 55, 3552–3553. [Google Scholar] [CrossRef]
- World Health Organization. Technical Manual for Drug Susceptibility Testing of Medicines Used in the Treatment of Tuberculosis; World Health Organization: Geneva, Switzerland, 2018; ISBN 978-92-4-151484-2. [Google Scholar]
- Alsultan, A.; Peloquin, C.A. Therapeutic Drug Monitoring in the Treatment of Tuberculosis: An Update. Drugs 2014, 74, 839–854. [Google Scholar] [CrossRef]
- Zheng, X.; Jongedijk, E.M.; Hu, Y.; Kuhlin, J.; Zheng, R.; Niward, K.; Paues, J.; Xu, B.; Davies Forsman, L.; Schön, T.; et al. Development and Validation of a Simple LC-MS/MS Method for Simultaneous Determination of Moxifloxacin, Levofloxacin, Prothionamide, Pyrazinamide and Ethambutol in Human Plasma. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2020, 1158, 122397. [Google Scholar] [CrossRef]
- World Health Organization. Definitions and Reporting Framework for Tuberculosis; World Health Organization: Geneva, Switzerland, 2013; ISBN 978-92-4-150534-5. [Google Scholar]
- Linh, N.N.; Viney, K.; Gegia, M.; Falzon, D.; Glaziou, P.; Floyd, K.; Timimi, H.; Ismail, N.; Zignol, M.; Kasaeva, T.; et al. World Health Organization Treatment Outcome Definitions for Tuberculosis: 2021 Update. Eur. Respir. J. 2021, 58, 2100804. [Google Scholar] [CrossRef]
- Chakraborthy, A.; Shivananjaiah, A.J.; Ramaswamy, S.; Chikkavenkatappa, N. Chest X Ray Score (Timika Score): An Useful Adjunct to Predict Treatment Outcome in Tuberculosis. Adv. Respir. Med. 2018, 86, 205–210. [Google Scholar] [CrossRef]
- Rudolf, F.; Lemvik, G.; Abate, E.; Verkuilen, J.; Schön, T.; Gomes, V.F.; Eugen-Olsen, J.; Østergaard, L.; Wejse, C. TBscore II: Refining and Validating a Simple Clinical Score for Treatment Monitoring of Patients with Pulmonary Tuberculosis. Scand. J. Infect. Dis. 2013, 45, 825–836. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number (%) |
|---|---|
| Area | |
| Guangzhou, China | 43 (30.1) |
| Henan, China | 50 (35.0) |
| Jiangsu, China | 50 (35.0) |
| Age (years) | 43.3 ± 10.4 |
| Male | 84 (58.7) |
| Weight (kg) | 58.0 (50.0–69.0) |
| BMI (kg/m2) | 20.9 ± 2.7 |
| Current smoker | 82 (57.3) |
| Diabetes mellitus type II | 27 (18.9) |
| Pulmonary cavities | 54 (37.8) |
| Extensive pulmonary disease (Timika score ≥ 71) | 0 (0.0) |
| Severe disease (TB score ≥ 8) | 31 (21.7) |
| Culture time to positivity (days) | 11.9 ± 3.3 |
| Drug intake | |
| moxifloxacin (400 mg, once daily) | 136 (95.1) |
| linezolid (600 mg, once daily) | 106 (74.1) |
| bedaquiline (400 mg, once daily) | 35 (24.5) |
| Clofazimine (100 mg, once daily) a | 109 (76.2) |
| Cycloserine (500 mg, once daily) | 129 (90.1) |
| P-aminosalicylic acid (3.3–6.6 g, twice a day) | 9 (6.3) |
| Prothionamide (600 mg, three times a day) | 41 (28.7) |
| pyrazinamide (1500 mg, three times a day) | 143 (100.0) |
| Ethambutol (750 mg, once daily) | 7 (4.9) |
| Pyrazinamide dosage (mg/kg) | 26.9 ± 5.7 |
| Using five effective drugs b | 143 (100.0) |
| Group A drugs c | |
| moxifloxacin + bedaquiline + linezolid | 35 (24.5) |
| moxifloxacin + linezolid | 64 (44.8) |
| moxifloxacin | 37 (25.9) |
| linezolid | 7 (4.9) |
| Two-month culture conversion | 52 (36.4) |
| Six-month culture conversion | 79 (55.2) |
| Time to culture conversion (months) | 6 (2–24) |
| Treatment outcome d | |
| Success | 96 (67.1) |
| Failure | 47 (32.9) |
| Treatment Regimen | Two-Month Culture Conversion | Six-Month Culture Conversion | Treatment Outcome | Time to Culture Conversion | ||||
|---|---|---|---|---|---|---|---|---|
| Negative No. (%) a | Adjusted RR b (95% CI) | Negative No. (%) a | Adjusted RR b (95% CI) | Success No. (%) a | Adjusted RR b (95% CI) | Month Median (IQR) | Adjusted HR b (95% CI) | |
| All patients | 52 (36.4) | 1.1 (1.09–1.20) | 79 (55.2) | 1.1 (1.06–1.16) | 96 (67.1) | 1.07 (1.03–1.10) | 6 (2–24) | 1.18 (1.14–1.23) |
| MFX + LZD + BDQ | 23 (65.7) | 1.1 (1.03–1.12) | 29 (82.9) | 1.05 (1.02–1.08) | 30 (85.7) | 1.04 (1.01–1.07) | 2 (2–4) | 1.12 (1.05–1.21) |
| MFX + LZD | 20 (31.3) | 1.5 (1.31–1.62) | 34 (53.1) | 1.2 (1.14–1.26) | 46 (71.9) | 1.1 (1.05–1.12) | 6 (2–24) | 1.6 (1.44–1.86) |
| MFX | 9 (24.3) | 3.0 (2.03–4.22) | 12 (32.4) | 1.4 (1.26–1.65) | 16 (43.2) | 1.2 (1.06–1.26) | 24 (3–24) | 2.2 (1.44–3.40) |
| LZD | 0 (0.0) | 1.0 (0.79–1.25) c | 4 (57.1) | 21.0 (17.84–24.63) | 4 (57.1) | 21.0 (17.84–24.63) | 6 (4–24) | 153 (23.57–1036) |
| CART-Derived Threshold | Sputum Culture Conversion/Treatment Outcome | Time to Culture Conversion | ||||
|---|---|---|---|---|---|---|
| Success/negative No. (%) a | RR (95% CI) | Adjusted RR b (95% CI) | Month Median (IQR) | HR (95% CI) | Adjusted HR b (95% CI) | |
| Two-month | ||||||
| AUC0–24h/MIC ≤ 12.8 c | 1 (1.1) | 1 | 1 | 24 (6–24) | 1 | 1 |
| AUC0–24h/MIC > 12.8 c | 51 (92.7) | 81.6 (11.6–573.6) | 77.8 (10.7–564.3) | 2 (2–2) | 20.4 (11.8–35.3) | 24.7 (12.9–47.3) |
| Six-month | ||||||
| AUC0–24h/MIC ≤ 8.5 d | 1 (1.5) | 1 | 1 | 24 (12–24) | 1 | 1 |
| AUC0–24h/MIC > 8.5 d | 78 (100.0) | 65.0 (9.3–454.5) | 67.8 (10.5–436.5) | 2 (2–4) | 302.5 (40.2–2273.1) | 334.2 (43.4–2576.3) |
| Treatment outcome | ||||||
| AUC0–24h/MIC ≤ 6.3 | 13 (22.0) | 1 | 1 | 24 (18–24) | 1 | 1 |
| AUC0–24h/MIC > 6.3 | 83 (98.8) | 4.5 (2.8–7.3) | 4.2 (2.6–6.9) | 2 (2–4) | 28.2 (14.5–55.2) | 30.6 (14.5–64.8) |
| Treatment Regimen | AUC0–24h/MIC = 6.3 (for Treatment Outcome) | AUC0–24h/MIC = 7.8 (for Six-Month Culture Conversion) | AUC0–24h/MIC = 12.7 (for Two-Month Culture Conversion) |
|---|---|---|---|
| MFX + LZD + BDQ | 1.000 | 1.000 | 1.000 |
| MFX + LZD | 0.874 | 1.000 | 0.966 |
| MFX | 0.875 | 1.000 | 1.000 |
| LZD | / | 1.000 | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dong, S.; Shao, G.; Davies Forsman, L.; Wang, S.; Wang, S.; Cao, J.; Bao, Z.; Bruchfeld, J.; Alffenaar, J.-W.C.; Liu, J.; et al. Drug Exposure and Susceptibility of Pyrazinamide Correlate with Treatment Response in Pyrazinamide-Susceptible Patients with Multidrug-Resistant Tuberculosis. Pharmaceutics 2024, 16, 144. https://doi.org/10.3390/pharmaceutics16010144
Dong S, Shao G, Davies Forsman L, Wang S, Wang S, Cao J, Bao Z, Bruchfeld J, Alffenaar J-WC, Liu J, et al. Drug Exposure and Susceptibility of Pyrazinamide Correlate with Treatment Response in Pyrazinamide-Susceptible Patients with Multidrug-Resistant Tuberculosis. Pharmaceutics. 2024; 16(1):144. https://doi.org/10.3390/pharmaceutics16010144
Chicago/Turabian StyleDong, Shulan, Ge Shao, Lina Davies Forsman, Sainan Wang, Shanshan Wang, Jiayi Cao, Ziwei Bao, Judith Bruchfeld, Jan-Willem C. Alffenaar, Jia Liu, and et al. 2024. "Drug Exposure and Susceptibility of Pyrazinamide Correlate with Treatment Response in Pyrazinamide-Susceptible Patients with Multidrug-Resistant Tuberculosis" Pharmaceutics 16, no. 1: 144. https://doi.org/10.3390/pharmaceutics16010144