
A Bilayer Microarray Patch (MAP) for HIV Pre-Exposure Prophylaxis: The Role of MAP Designs and Formulation Composition in Enhancing Long-Acting Drug Delivery
 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Strategies to Improve MAP Delivery Efficiency via Refinement of MAP Designs
2.3. Strategies to Enhance MAP Delivery Efficiency via Fabrication of Improved Bilayer MAPs
2.4. MAP Characterization
2.4.1. Determination of CAB Na MAP Drug Content
2.4.2. Assessment of CAB Na MAP Mechanical Properties
2.5. Ex Vivo Drug Deposition Studies
2.6. In Vivo Drug Deposition and Pharmacokinetic Studies
2.6.1. Rat Dose Calculation
2.6.2. In Vivo Study Design and Experimental Procedure
2.7. Pharmaceutical Analysis
2.7.1. Preparation of Drug-Containing Samples from the In Vitro Studies for Drug Analysis
2.7.2. Preparation of Skin Tissue Samples from Ex Vivo Studies for Drug Analysis
2.7.3. Preparation of Plasma Samples from In Vivo Studies for Drug Analysis
2.8. Pharmacokinetic Parameter Calculation
2.9. Statistical Analysis
3. Results and Discussion
3.1. Characterization of MAP Designs for Improved Insertion and Drug Delivery Performance
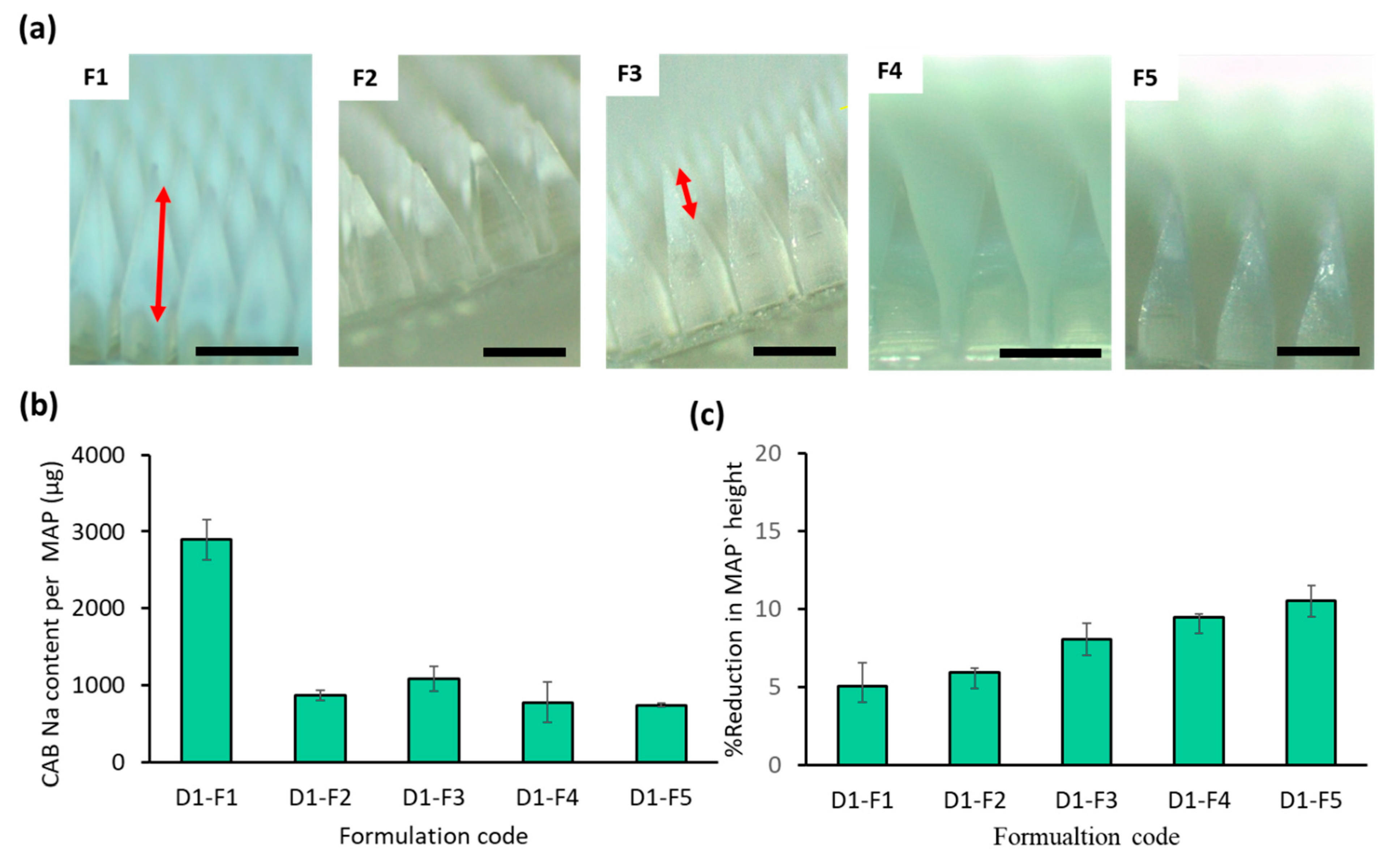
3.2. Improving the MAP Formulation to Enhance MAP Delivery Efficiency
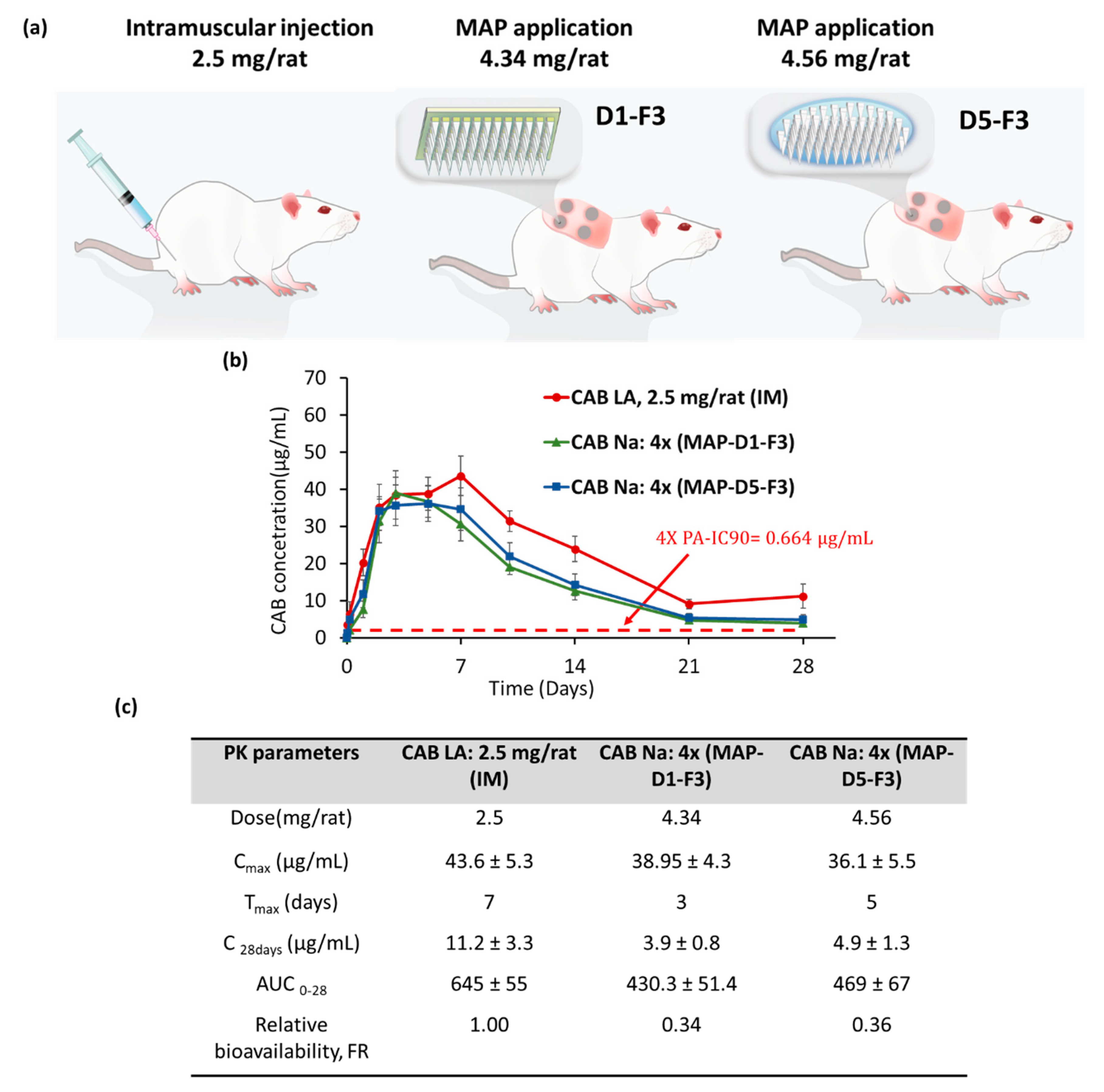
3.3. In Vivo Pharmacokinetic Studies: Combination MAP Designs/Hydrogel Formulation to Enhance MAP Delivery Efficiency
3.4. In Vivo Pharmacokinetic Studies: Repeated Dosing of D1 and D5 Using F3
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Girum, T.; Wasie, A.; Worku, A. Trend of HIV/AIDS for the Last 26 Years and Predicting Achievement of the 90–90-90 HIV Prevention Targets by 2020 in Ethiopia: A Time Series Analysis. BMC Infect. Dis. 2020, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Barré-Sinoussi, F.; Chermann, J.C.; Rey, F.; Nugeyre, M.T.; Chamaret, S.; Gruest, J.; Dauguet, C.; Axler-Blin, C.; Vézinet-Brun, F.; Rouzioux, C.; et al. Isolation of a T-Lymphotropic Retrovirus from a Patient at Risk for Acquired Immune Deficiency Syndrome (AIDS). Science 1983, 220, 868–871. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 HIV Collaborators. Global, Regional, and National Incidence, Prevalence, and Mortality of HIV, 1980–2017, and Forecasts to 2030, for 195 Countries and Territories: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors Study 2017. Lancet HIV 2019, 6, 831–859. [Google Scholar] [CrossRef]
- Gottlieb, M.S.; Schroff, R.; Schanker, H.M.; Weisman, J.D.; Fan, P.T.; Wolf, R.A.; Saxon, A. Pneumocystis Carinii Pneumonia and Mucosal Candidiasis in Previously Healthy Homosexual Men. Evidence of a New Acquired Cellular Immunodeficiency. J. Urol. 1982, 128, 444. [Google Scholar] [CrossRef]
- UNAIDS. Danger: Unaids Global Aids Update; UNAIDS: Geneva, Switzerland, 2022. [Google Scholar]
- Sidebottom, D.; Ekström, A.M.; Strömdahl, S. A Systematic Review of Adherence to Oral Pre-Exposure Prophylaxis for HIV—How Can We Improve Uptake and Adherence? BMC Infect. Dis. 2018, 18, 581. [Google Scholar] [CrossRef]
- Venkatesan, P. Long-Acting Injectable ART for HIV: A (Cautious) Step Forward. Lancet Microbe 2022, 3, e94. [Google Scholar] [CrossRef]
- WHO. Recommends the Dapivirine Vaginal Ring as a New Choice for HIV Prevention for Women at Substantial Risk of HIV Infection. Available online: https://www.who.int/news/item/26-01-2021-who-recommends-the-dapivirine-vaginal-ring-as-a-new-choice-for-hiv-prevention-for-women-at-substantial-risk-of-hiv-infection (accessed on 3 November 2023).
- Paik, J. Lenacapavir: First Approval. Drugs 2022, 82, 1499–1504. [Google Scholar] [CrossRef]
- Pons-Faudoa, F.P.; Sizovs, A.; Di Trani, N.; Paez-Mayorga, J.; Bruno, G.; Rhudy, J.; Manohar, M.; Gwenden, K.; Martini, C.; Chua, C.Y.X.; et al. 2-Hydroxypropyl-β-cyclodextrin-enhanced pharmacokinetics of cabotegravir from a nanofluidic implant for HIV pre-exposure prophylaxis. J. Control Release 2019, 306, 89–96. [Google Scholar] [CrossRef]
- Pons-Faudoa, F.P.; Di Trani, N.; Capuani, S.; Campa-Carranza, J.N.; Nehete, B.; Sharma, S.; Shelton, K.A.; Bushman, L.R.; Abdelmawla, F.; Williams, M.; et al. Long-acting refillable nanofluidic implant confers protection against SHIV infection in nonhuman primates. Sci. Transl. Med. 2023, 15, eadg2887. [Google Scholar] [CrossRef]
- Massud, I.; Krovi, A.; Nishiura, K.; Ruone, S.; Li, L.; Holder, A.; Gary, J.; Mills, P.; Mitchell, J.; Khalil, G.; et al. Safety and efficacy of a biodegradable implant releasing tenofovir alafenamide for vaginal protection in a macaque model. J. Antimicrob. Chemother. 2022, 77, 2964–2971. [Google Scholar] [CrossRef]
- Palanee-Phillips, T.; Baum, M.M.; Moss, J.A.; Clark, M.R.; Nuttall, J.; Romano, J.W. Drug-releasing vaginal rings for HIV/STI and pregnancy prevention: A review of recent advances and clinical applications. Expert Opin. Drug Deliv. 2022, 19, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Mgodi, N.M.; Murewanhema, G. Advancing the Use of Long-Acting Extended Delivery Formulations for HIV Prevention in Sub-Saharan Africa: Challenges, Opportunities, and Advancing the Use of Long-Acting Extended Delivery Formulations for HIV Prevention in Sub-Saharan Africa: Challeng. J. Int. AIDS Soc. 2023, 26, e26115. [Google Scholar] [CrossRef] [PubMed]
- Tekko, I.A.; Vora, L.K.; Volpe-zanutto, F.; Moffatt, K.; Jarrahian, C.; Mccarthy, H.O.; Donnelly, R.F. Novel Bilayer Microarray Patch-Assisted Long-Acting Micro-Depot Cabotegravir Intradermal Delivery for HIV Pre-Exposure Prophylaxis. Adv. Funct. Mater. 2022, 32, 2106999. [Google Scholar] [CrossRef]
- Moffatt, K.; Tekko, I.A.; Vora, L.; Volpe-Zanutto, F.; Hutton, A.R.J.; Mistilis, J.; Jarrahian, C.; Akhavein, N.; Weber, A.D.; McCarthy, H.O.; et al. Development and Evaluation of Dissolving Microarray Patches for Co-Administered and Repeated Intradermal Delivery of Long-Acting Rilpivirine and Cabotegravir Nanosuspensions for Paediatric HIV Antiretroviral Therapy. Pharm. Res. 2022, 40, 1673–1696. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Vora, L.K.; Tekko, I.A.; Volpe-zanutto, F.; Peng, K.; Paredes, A.J.; Mccarthy, H.O.; Donnelly, R.F. Development of Dissolving Microneedles for Intradermal Delivery of the Long-Acting Antiretroviral Drug Bictegravir. Int. J. Pharm. 2023, 642, 123108. [Google Scholar] [CrossRef] [PubMed]
- Paredes, A.J.; Ramöller, I.K.; Mckenna, P.E.; Abbate, M.T.A.; Volpe-zanutto, F.; Vora, L.K.; Kilbourne-brook, M.; Jarrahian, C.; Moffatt, K.; Zhang, C.; et al. Microarray Patches: Breaking down the Barriers to Contraceptive Care and HIV Prevention for Women across the Globe. Adv. Drug Deliv. Rev. 2021, 173, 331–348. [Google Scholar] [CrossRef] [PubMed]
- Sabri, A.H.; Kim, Y.; Marlow, M.; Scurr, D.J.; Segal, J.; Banga, A.K.; Kagan, L.; Bong, J. Intradermal and Transdermal Drug Delivery Using Microneedles—Fabrication, Performance Evaluation and Application to Lymphatic Delivery. Adv. Drug Deliv. Rev. 2019, 153, 195–215. [Google Scholar] [CrossRef]
- Sabri, A.; Ogilvie, J.; Abdulhamid, K.; Shpadaruk, V.; McKenna, J.; Segal, J.; Scurr, D.J.; Marlow, M. Expanding the Applications of Microneedles in Dermatology. Eur. J. Pharm. Biopharm. 2019, 140, 121–140. [Google Scholar] [CrossRef]
- Ramöller, I.K.; Volpe-Zanutto, F.; Vora, L.K.; Abbate, M.T.A.; Hutton, A.R.J.; McKenna, P.E.; Peng, K.; Tekko, I.A.; Sabri, A.; McAlister, E.; et al. Intradermal delivery of the antiretroviral drugs cabotegravir and rilpivirine by dissolving microarray patches: Investigation of lymphatic uptake. J. Control Release 2024, 366, 548–566. [Google Scholar] [CrossRef]
- Tekko, I.; Vora, L.; McCrudden, M.T.C.; Jarrahian, C.; Rein-Weston, A.; Zehrung, D.; Giffen, P.; McCarthy, H.O.; Donnelly, R.F. Novel Dissolving Bilayer Microarray Patches as a Minimally Invasive, Efficient Intradermal Delivery System for a Long-Acting Cabotegravir Nanosuspension. In Proceedings of the 2019 Controlled Release Society Annual Meeting & Exposition, Valencia, Spain, 21–24 July 2019. [Google Scholar]
- Cordeiro, A.S.; Tekko, I.A.; Jomaa, M.H.; Vora, L.; McAlister, E.; Volpe-Zanutto, F.; Nethery, M.; Baine, P.T.; Mitchell, N.; McNeill, D.W.; et al. Two-Photon Polymerisation 3D Printing of Microneedle Array Templates with Versatile Designs: Application in the Development of Polymeric Drug Delivery Systems. Pharm. Res. 2020, 37, 174. [Google Scholar] [CrossRef]
- Larrañeta, E.; Lutton, R.E.M.; Woolfson, A.D.; Donnelly, R.F. Microneedle Arrays as Transdermal and Intradermal Drug Delivery Systems: Materials Science, Manufacture and Commercial Development. Mater. Sci. Eng. R Rep. 2016, 104, 1–32. [Google Scholar] [CrossRef]
- Tekko, I.A.; Permana, A.; Vora, L.; Hatahet, T.; Mccarthy, H.O.; Donnelly, R.F. Localised and Sustained Intradermal Delivery of Methotrexate Using Nanocrystal-Loaded Microneedle Arrays: Potential for Enhanced Treatment of Psoriasis. Eur. J. Pharm. Sci. 2020, 152, 105469. [Google Scholar] [CrossRef] [PubMed]
- Volpe-Zanutto, F.; Vora, L.K.; Tekko, I.A.; McKenna, P.E.; Permana, A.D.; Sabri, A.H.; Anjani, Q.K.; McCarthy, H.O.; Paredes, A.J.; Donnelly, R.F. Hydrogel-Forming Microarray Patches with Cyclodextrin Drug Reservoirs for Long-Acting Delivery of Poorly Soluble Cabotegravir Sodium for HIV Pre-Exposure Prophylaxis. J. Control Release 2022, 348, 771–785. [Google Scholar] [CrossRef]
- Zhang, Y.; Huo, M.; Zhou, J.; Xie, S. PKSolver: An Add-in Program for Pharmacokinetic and Pharmacodynamic Data Analysis in Microsoft Excel. Comput. Methods Programs Biomed. 2010, 99, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Herkenne, C.; Naik, A.; Kalia, Y.N.; Hadgraft, J.; Guy, R.H. Pig Ear Skin Ex Vivo as a Model for in Vivo Dermatopharmacokinetic Studies in Man. Pharm. Res. 2006, 23, 1850–1856. [Google Scholar] [CrossRef]
- Makvandi, P.; Kirkby, M.; Hutton, A.R.J.; Shabani, M.; Yiu, C.K.Y.; Baghbantaraghdari, Z.; Jamaledin, R.; Carlotti, M.; Mazzolai, B.; Mattoli, V.; et al. Engineering Microneedle Patches for Improved Penetration: Analysis, Skin Models and Factors Affecting Needle Insertion; Springer: Singapore, 2021; Volume 13, ISBN 0123456789. [Google Scholar]
- Anjani, Q.K.; Hidayat, A.; Sabri, B.; Moreno-castellanos, N.; Utomo, E.; Cárcamo-martínez, Á.; Domínguez-robles, J.; Ahmadi, L.; Wardoyo, H.; Donnelly, R.F. Soluplus®-Based Dissolving Microarray Patches Loaded with Colchicine: Towards a Minimally Invasive Treatment and Management of Gout. Biomater. Sci. 2022, 10, 5838–5855. [Google Scholar] [CrossRef] [PubMed]
- Kurnia, Q.; Hidayat, A.; Sabri, B.; Domínguez-robles, J.; Donnelly, R.F. Metronidazole Nanosuspension Loaded Dissolving Microarray Patches: An Engineered Composite Pharmaceutical System for the Treatment of Skin and Soft Tissue Infection. Biomater. Adv. 2022, 140, 213073. [Google Scholar] [CrossRef]
- Levintova, Y.; Plakogiannis, F.M.; Bellantone, R.A. An Improved in Vitro Method for Measuring Skin Permeability That Controls Excess Hydration of Skin Using Modified Franz Diffusion Cells. Int. J. Pharm. 2011, 419, 96–106. [Google Scholar] [CrossRef]
- Nguyen, V.T.T.; Darville, N.; Vermeulen, A. Pharmacokinetics of Long-Acting Aqueous Nano-/Microsuspensions After Intramuscular Administration in Different Animal Species and Humans—A Review. AAPS J. 2023, 25, 4. [Google Scholar] [CrossRef]
- Kovač, L.; Časar, Z.; Trdan Lušin, T.; Roškar, R. Development of an Analytical Method for Determination of Related Substances and Degradation Products of Cabotegravir Using Analytical Quality by Design Principles. ACS Omega 2022, 7, 8896–8905. [Google Scholar] [CrossRef]
- Carter, N.W.; Rector, F.C.; Campion, D.S.; Seldin, D.W. Measurement of Intracellular PH of Skeletal Muscle with PH-Sensitive Glass Microelectrodes. J. Clin. Investig. 1967, 46, 920–933. [Google Scholar] [CrossRef]
- Paredes, A.J.; Volpe-Zanutto, F.; Vora, L.K.; Tekko, I.A.; Permana, A.D.; Picco, C.J.; McCarthy, H.O.; Donnelly, R.F. Systemic Delivery of Tenofovir Alafenamide Using Dissolving and Implantable Microneedle Patches. Mater. Today Bio 2022, 13, 100217. [Google Scholar] [CrossRef] [PubMed]
- Vora, L.K.; Donnelly, R.F.; Larrañeta, E.; González-Vázquez, P.; Thakur, R.R.S.; Vavia, P.R. Novel Bilayer Dissolving Microneedle Arrays with Concentrated PLGA Nano-Microparticles for Targeted Intradermal Delivery: Proof of Concept. J. Control Release 2017, 265, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Sabri, A.H.; Cater, Z.; Ogilvie, J.; Scurr, D.J.; Marlow, M.; Segal, J. Characterisation of Mechanical Insertion of Commercial Microneedles. J. Drug Deliv. Sci. Technol. 2020, 58, 101766. [Google Scholar] [CrossRef]
- Donnelly, R.F.; Garland, M.J.; Morrow, D.I.J.; Migalska, K.; Raghu, T.; Singh, R.; Majithiya, R.; Woolfson, A.D. Optical Coherence Tomography Is a Valuable Tool in the Study of the Effects of Microneedle Geometry on Skin Penetration Characteristics and In-Skin Dissolution. J. Control. Release 2010, 147, 333–341. [Google Scholar] [CrossRef]
- Gachigua, S.G.; Karuga, R.; Ngunjiri, A.; Jarrahian, C.; Coffey, P.S.; Kilbourne-Brook, M.; Otiso, L. Microarray Patch for HIV Prevention and as a Multipurpose Prevention Technology to Prevent HIV and Unplanned Pregnancy: An Assessment of Potential Acceptability, Usability, and Programmatic Fit in Kenya. Front. Reprod. Health 2023, 5, 1125159. [Google Scholar] [CrossRef]
- Kinvig, H.; Rajoli, R.K.R.; Pertinez, H.; Vora, L.K.; Volpe-Zanutto, F.; Donnelly, R.F.; Rannard, S.; Flexner, C.; Siccardi, M.; Owen, A. Physiologically Based Pharmacokinetic Modelling of Cabotegravir Microarray Patches in Rats and Humans. Pharmaceutics 2023, 15, 2709. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Code | Design | Length (µm) | Base Width (µm) | Interspacing (µm) | Array Size (cm2) |
|---|---|---|---|---|---|
| MAP-D1 | 16 × 16 (256) Cuboidal base/pyramidal tips | 900 | 300 | 100 | 0.5 |
| MAP-D2 | 11 × 11 (121) Cuboidal base/pyramidal tips | 900 | 300 | 300 | 0.5 |
| MAP-D3 | 16 × 16 (256) Full conical | 900 | 300 | 100 | 0.5 |
| MAP-D4 | 16 × 16 (256) Full pyramidal | 900 | 300 | 100 | 0.5 |
| MAP-D5 | 24 × 25 (600) Full pyramidal | 700 | 300 | 50 | 0.75 |
| MAP-D6 | 9 × 9 Cuboidal base/pyramidal tips | 1150 | 500 | 300 | 0.5 |
| Formulation Code | |||||
|---|---|---|---|---|---|
| Composition | F1 | F2 * | F3 | F4 | F5 |
| CAB Na, g | 0.84 | 0.84 | 0.84 | 0.84 | 0.84 |
| PVA (10 kDa) gel (40%w/w), g | 0.6 | 0.6 | 0.6 | 0.6 | 0.6 |
| PVP K29-32 gel (40%w/w), g | 0.6 | 0.6 | 0.6 | 0.6 | 0.6 |
| Water, mL | 1.0 | 1.0 | 1.5 | 2.0 | 2.5 |
| Cohort | Administration Route/Array Design/Dosing Regimen | Study Objective | Rat Weight | Number of MAPs or Injection/Rat | Total Dose/Rat (mg) | Study Period (Days) |
|---|---|---|---|---|---|---|
| 1 | Intradermal/Single dose | Drug deposition | 228 ± 8 | 2 × 50 µL | 2.6 mg | 1 |
| 2 | MAP-D1-F1/Single dose | 236 ± 4 | 4 MAP | 10.9 mg | 1 | |
| 3 | MAP-D2-F1/Single dose | 222 ± 4 | 4 MAP | 4.4 mg | 1 | |
| 4 | MAP-D3-F1/Single dose | 224 ± 9 | 4 MAP | 7.2 mg | 1 | |
| 5 | MAP-D4-F1/Single dose | 215 ± 3 | 4 MAP | 7.04 mg | 1 | |
| 6 | MAP-D5-F1/Single dose | 217 ± 7 | 4 MAP | 13.1 mg | 1 | |
| 7 | MAP-D6-F1/Single dose | 215 ± 6 | 4 MAP | 11.5 mg | 1 | |
| 8 | MAP-D1-F3/Single dose | 207 ± 5 | 4 MAP | 4.3 mg | 1 | |
| 9 | MAP-D4-F3/Single dose | 209 ± 21 | 4 MAP | 2.9 mg | 1 | |
| 10 | MAP-D5-F3/Single dose | 210 ± 12 | 4 MAP | 4.6 mg | 1 | |
| 11 | IM/Single dose | Single dose PK study | 218 ± 11 | 50 µL | 2.5 mg | 28 |
| 12 | MAP-D1-F3/Single dose | 212 ± 8 | 4 MAP | 4.3 mg | 28 | |
| 13 | MAP-D5-F3/Single dose | 200 ± 6 | 4 MAP | 4.6 mg | 28 | |
| 14 | LD: IM MD: IM | Repeated dose PK study | 259 ± 24 | LD: 50 µL MD: 50 µL | LD: 2.5 mg MD: weekly 1.25 mg | 42 |
| 15 | LD: IM MD: MAP | 274 ± 29 | LD: 50 µL MD: 4 MAP | LD: 2.5 mg MD: weekly 4.3 mg | 42 | |
| 16 | LD: MAP MD: MAP | 269 ±30 | LD: 4 MAP MD: 4 MAP | LD: 4.3 mg MD: weekly 4.3 mg | 42 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vora, L.K.; Tekko, I.A.; Zanutto, F.V.; Sabri, A.; Choy, R.K.M.; Mistilis, J.; Kwarteng, P.; Jarrahian, C.; McCarthy, H.O.; Donnelly, R.F. A Bilayer Microarray Patch (MAP) for HIV Pre-Exposure Prophylaxis: The Role of MAP Designs and Formulation Composition in Enhancing Long-Acting Drug Delivery. Pharmaceutics 2024, 16, 142. https://doi.org/10.3390/pharmaceutics16010142
Vora LK, Tekko IA, Zanutto FV, Sabri A, Choy RKM, Mistilis J, Kwarteng P, Jarrahian C, McCarthy HO, Donnelly RF. A Bilayer Microarray Patch (MAP) for HIV Pre-Exposure Prophylaxis: The Role of MAP Designs and Formulation Composition in Enhancing Long-Acting Drug Delivery. Pharmaceutics. 2024; 16(1):142. https://doi.org/10.3390/pharmaceutics16010142
Chicago/Turabian StyleVora, Lalitkumar K., Ismaiel A. Tekko, Fabiana Volpe Zanutto, Akmal Sabri, Robert K. M. Choy, Jessica Mistilis, Priscilla Kwarteng, Courtney Jarrahian, Helen O. McCarthy, and Ryan F. Donnelly. 2024. "A Bilayer Microarray Patch (MAP) for HIV Pre-Exposure Prophylaxis: The Role of MAP Designs and Formulation Composition in Enhancing Long-Acting Drug Delivery" Pharmaceutics 16, no. 1: 142. https://doi.org/10.3390/pharmaceutics16010142