
Safety Evaluation and Population Pharmacokinetics of Camostat Mesylate and Its Major Metabolites Using a Phase I Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethics
2.3. Blood Sampling
2.4. Bioanalysis
2.5. Statistical Analysis of PK and Safety
2.6. Population PK Model Development
2.7. Simulations
3. Results
3.1. Population
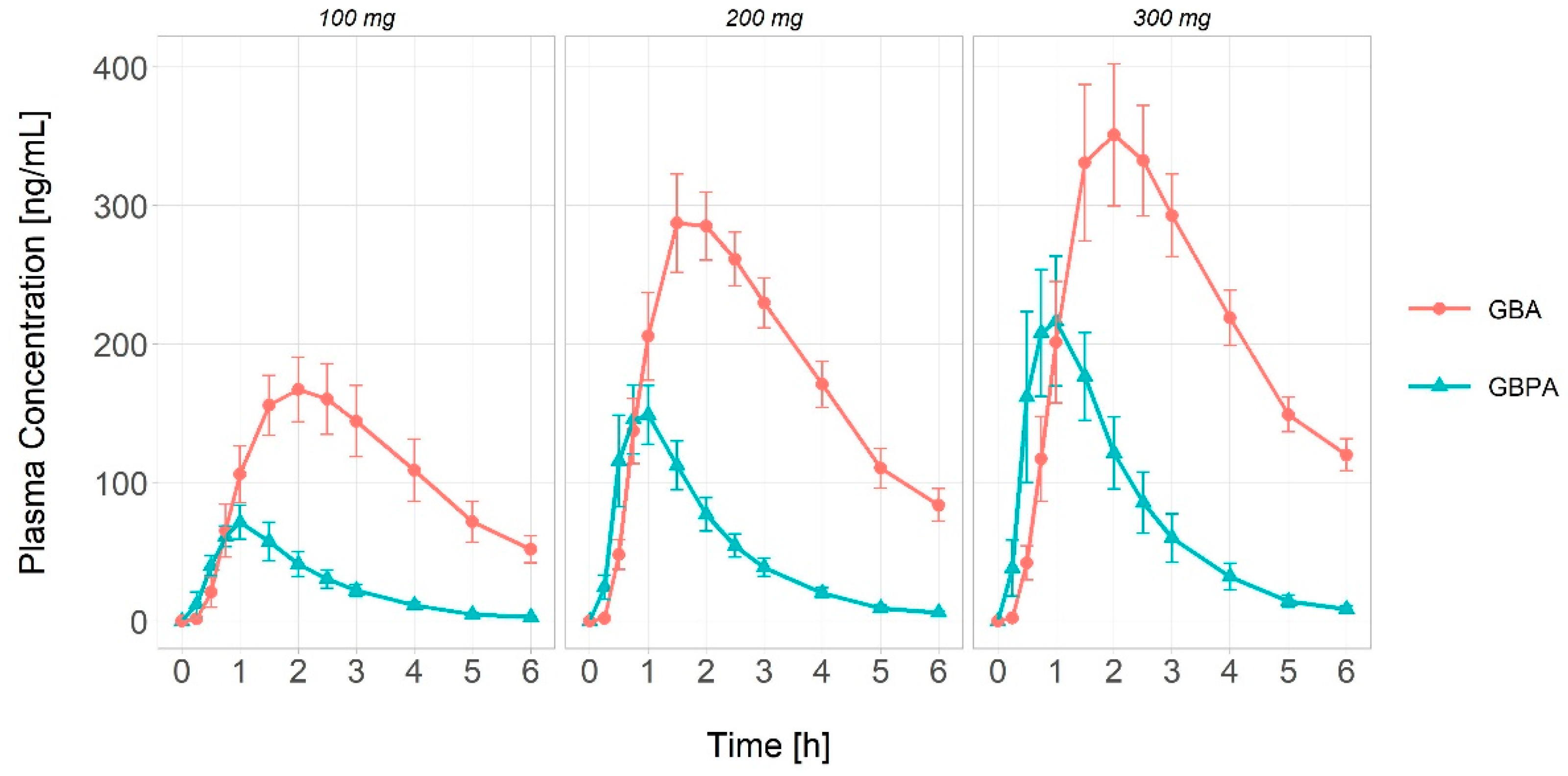
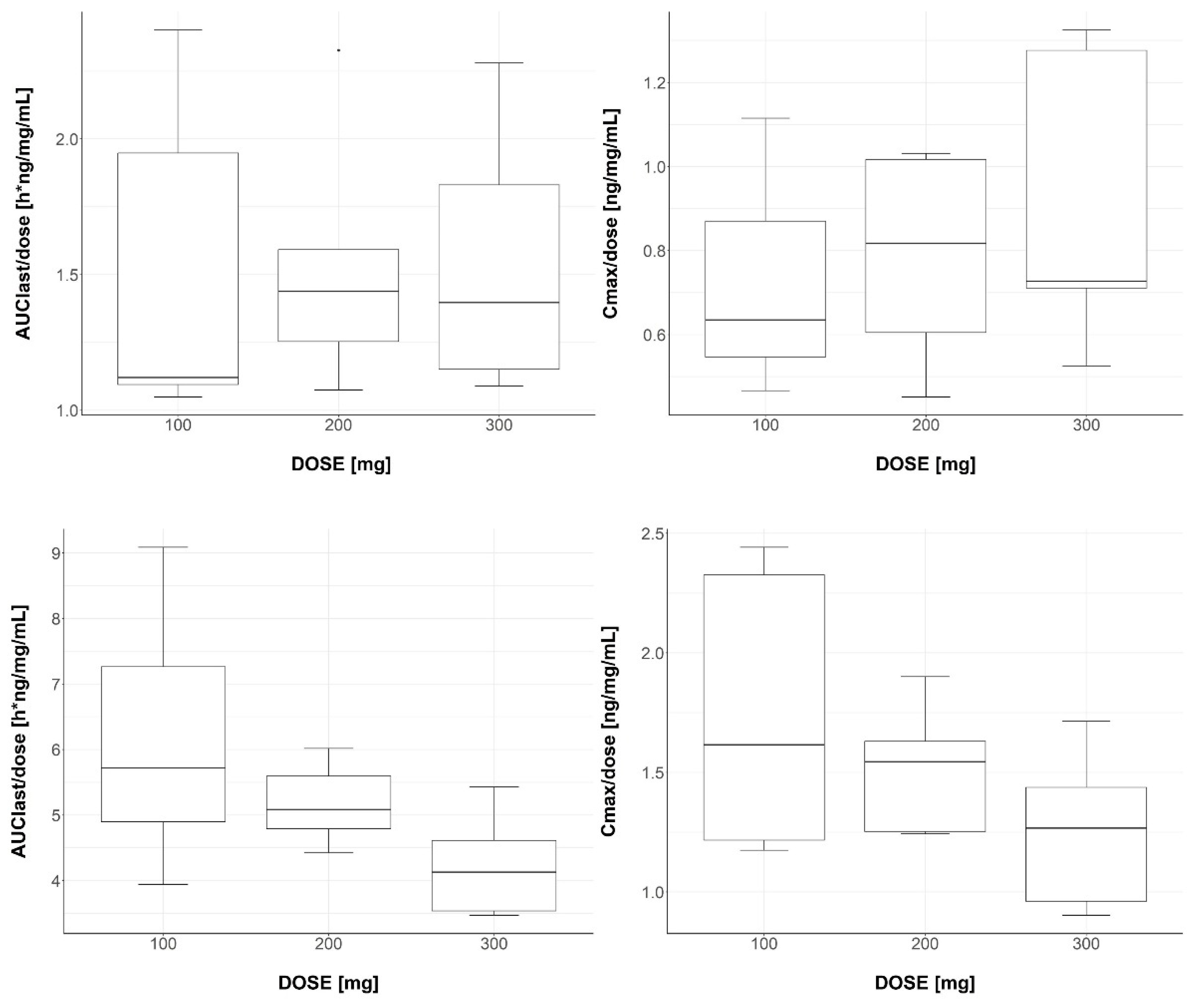
3.2. Pharmacokinetic Analysis
3.3. Safety Analysis
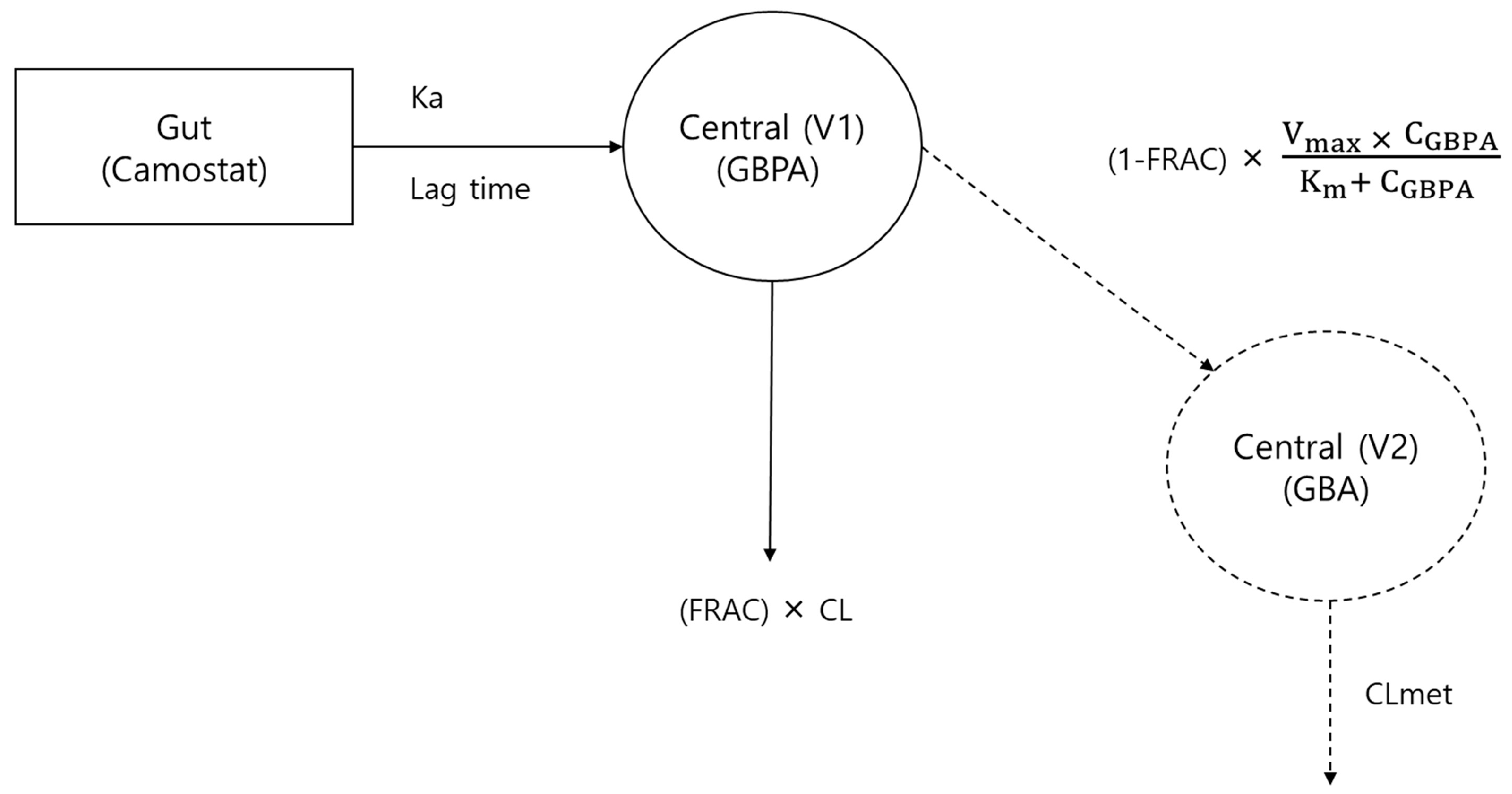
3.4. Population PK Model Development
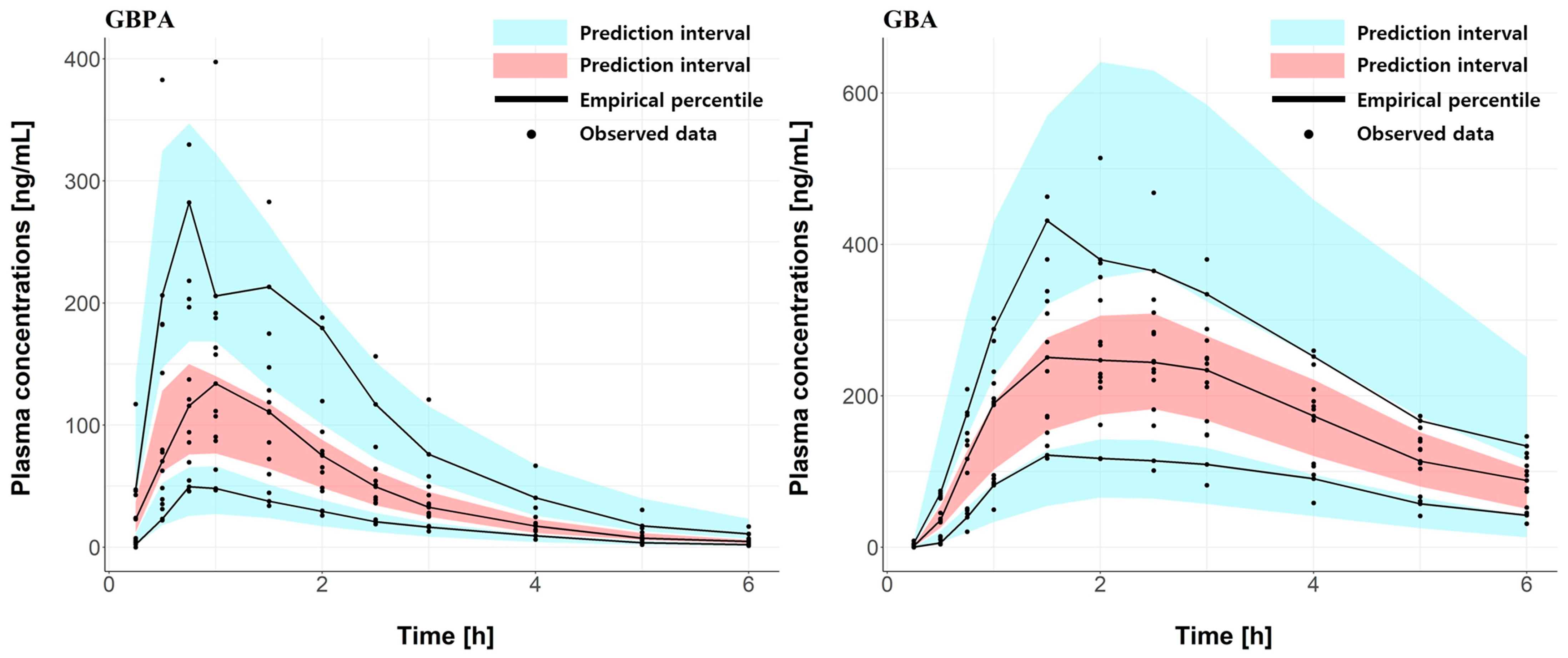
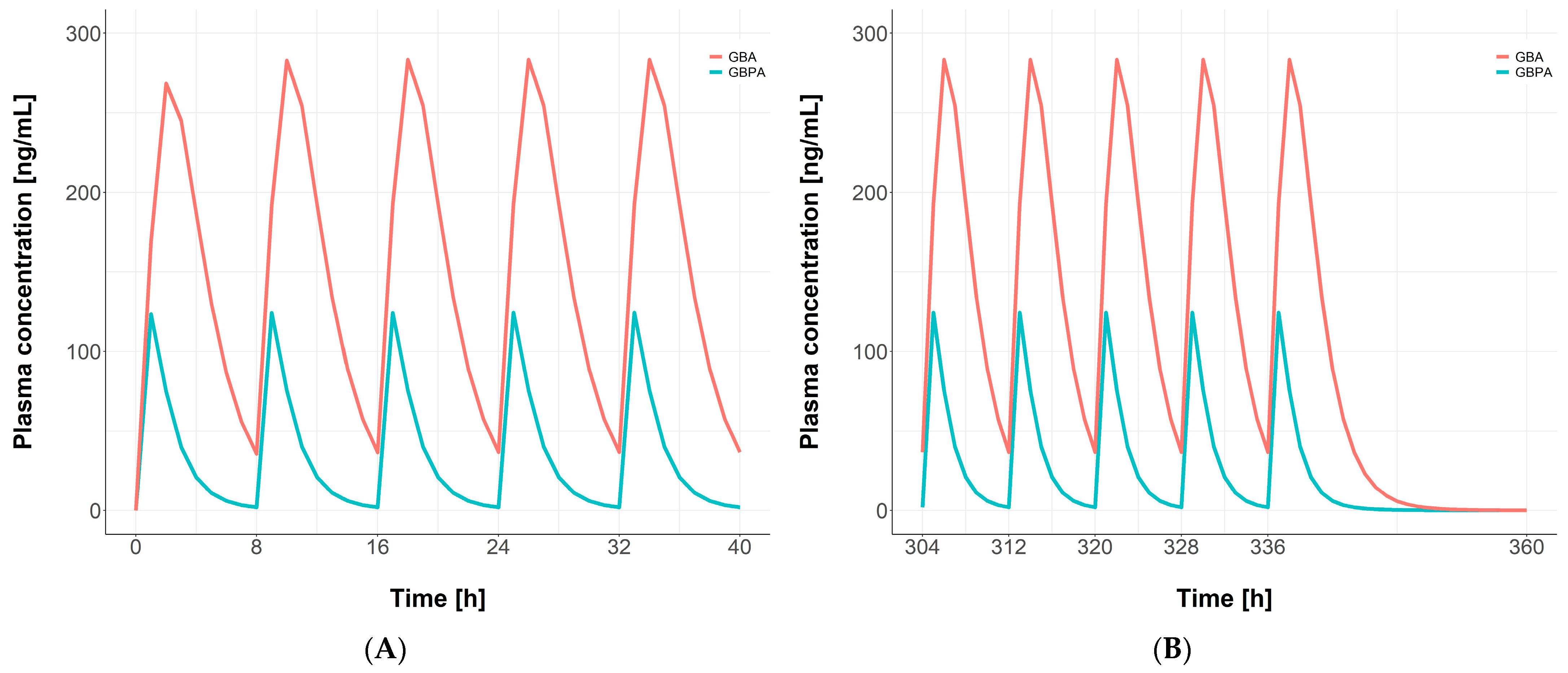
3.5. Simulations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The Socio-Economic Implications of the Coronavirus Pandemic (COVID-19): A Review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Satsangi, S.; Gupta, N.; Kodan, P. Current and New Drugs for COVID-19 Treatment and Its Effects on the Liver. J. Clin. Transl. Hepatol. 2021, 9, 436. [Google Scholar] [CrossRef] [PubMed]
- Serafin, M.B.; Bottega, A.; Foletto, V.S.; da Rosa, T.F.; Hörner, A.; Hörner, R. Drug Repositioning Is an Alternative for the Treatment of Coronavirus COVID-19. Int. J. Antimicrob. Agents 2020, 55, 105969. [Google Scholar] [CrossRef] [PubMed]
- Malik, P.; Jain, S.; Jain, P.; Kumawat, J.; Dwivedi, J.; Kishore, D. A Comprehensive Update on the Structure and Synthesis of Potential Drug Targets for Combating the Coronavirus Pandemic Caused by SARS-CoV-2. Arch. Pharm. 2022, 355, 2100382. [Google Scholar] [CrossRef]
- Hoffmann, M.; Hofmann-Winkler, H.; Smith, J.C.; Krüger, N.; Arora, P.; Sørensen, L.K.; Søgaard, O.S.; Hasselstrøm, J.B.; Winkler, M.; Hempel, T. Camostat Mesylate Inhibits SARS-CoV-2 Activation by TMPRSS2-Related Proteases and Its Metabolite GBPA Exerts Antiviral Activity. eBioMedicine 2021, 65, 103255. [Google Scholar] [CrossRef]
- Hoffmann, M.; Schroeder, S.; Kleine-Weber, H.; Müller, M.A.; Drosten, C.; Pöhlmann, S. Nafamostat Mesylate Blocks Activation of SARS-CoV-2: New Treatment Option for COVID-19. Antimicrob. Agents Chemother. 2020, 64, e00754-20. [Google Scholar] [CrossRef]
- Zhou, Y.; Vedantham, P.; Lu, K.; Agudelo, J.; Carrion, R.; Nunneley, J.W.; Barnard, D.; Pöhlmann, S.; McKerrow, J.H.; Renslo, A.R.; et al. Protease Inhibitors Targeting Coronavirus and Filovirus Entry. Antiviral Res. 2015, 116, 76–84. [Google Scholar] [CrossRef]
- Jilg, N.; Chew, K.W.; Giganti, M.J.; Daar, E.S.; Wohl, D.A.; Javan, A.C.; Kantor, A.; Moser, C.; Coombs, R.W.; Neytman, G. One Week of Oral Camostat Versus Placebo in Non-Hospitalized Adults with Mild-to-Moderate COVID-19: A Randomized Controlled Phase 2 Trial. Clin. Infect. Dis. 2023, ciad342. [Google Scholar] [CrossRef]
- Chupp, G.; Spichler-Moffarah, A.; Søgaard, O.S.; Esserman, D.; Dziura, J.; Danzig, L.; Chaurasia, R.; Patra, K.P.; Salovey, A.; Nunez, A. A Phase 2 Randomized, Double-Blind, Placebo-Controlled Trial of Oral Camostat Mesylate for Early Treatment of COVID-19 Outpatients Showed Shorter Illness Course and Attenuation of Loss of Smell and Taste. medRxiv 2022. [Google Scholar] [CrossRef]
- Gunst, J.D.; Staerke, N.B.; Pahus, M.H.; Kristensen, L.H.; Bodilsen, J.; Lohse, N.; Dalgaard, L.S.; Brønnum, D.; Fröbert, O.; Hønge, B. Efficacy of the TMPRSS2 Inhibitor Camostat Mesilate in Patients Hospitalized with Covid-19-a Double-Blind Randomized Controlled Trial. eClinicalMedicine 2021, 35, 100849. [Google Scholar] [CrossRef]
- Breining, P.; Frølund, A.L.; Højen, J.F.; Gunst, J.D.; Staerke, N.B.; Saedder, E.; Cases-Thomas, M.; Little, P.; Nielsen, L.P.; Søgaard, O.S. Camostat Mesylate against SARS-CoV-2 and COVID-19—Rationale, Dosing and Safety. Basic Clin. Pharmacol. Toxicol. 2021, 128, 204–212. [Google Scholar] [CrossRef]
- Kinoshita, T.; Shinoda, M.; Nishizaki, Y.; Shiraki, K.; Hirai, Y.; Kichikawa, Y.; Tsushima, K.; Sinkai, M.; Komura, N.; Yoshida, K. A Multicenter, Double-Blind, Randomised, Parallel-Group, Placebo-Controlled Study to Evaluate the Efficacy and Saafety of Camostat Mesilate in Patients with COVID-19 (CANDLE Study). BMC Med. 2022, 20, 342. [Google Scholar] [CrossRef]
- Tobback, E.; Degroote, S.; Buysse, S.; Delesie, L.; Van Dooren, L.; Vanherrewege, S.; Barbezange, C.; Hutse, V.; Romano, M.; Thomas, I. Efficacy and Safety of Camostat Mesylate in Early COVID-19 Disease in an Ambulatory Setting: A Randomized Placebo-Controlled Phase II Trial. Int. J. Infect. Dis. 2022, 122, 628–635. [Google Scholar] [CrossRef]
- Choi, J.-P.; Kim, H.-J.; Han, J.; Park, S.; Han, J. Foistar® (Camostat Mesylate) Associated with the Significant Decrease in CRP Levels Compared to Kaletra®(Lopinavir/Ritonavir) Treatment in Korean Mild COVID-19 Pneumonic Patients. medrxiv 2020. [Google Scholar] [CrossRef]
- Khatri, M.; Mago, P. Nitazoxanide/Camostat Combination for COVID-19: An Unexplored Potential Therapy. Chem. Biol. Lett. 2020, 7, 192–196. [Google Scholar]
- Bittmann, S.; Weissenstein, A.; Villalon, G.; Moschuring-Alieva, E.; Luchter, E. Simultaneous Treatment of COVID-19 with Serine Protease Inhibitor Camostat and/or Cathepsin l Inhibitor? J. Clin. Med. Res. 2020, 12, 320. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, L.K.; Hasselstrøm, J.B.; Gunst, J.D.; Søgaard, O.S.; Kjolby, M. Determination of Camostat and Its Metabolites in Human Plasma–Preservation of Samples and Quantification by a Validated UHPLC-MS/MS Method. Clin. Biochem. 2021, 96, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Reckh, K.; Weidenbach, H.; Weidenbach, F.; Mutter, R.; Adler, G. Hepatic and Pancreatic Metabolism and Biliary Excretion of the Protease Inhibitor Camostat Mesilate. Int. J. Pancreatol. 1991, 10, 197–205. [Google Scholar] [CrossRef]
- Midgley, I.; Hood, A.J.; Proctor, P.; Chasseaud, L.F.; Irons, S.R.; Cheng, K.N.; Brindley, C.J.; Bonn, R. Metabolic Fate of 14C-Camostat Mesylate in Man, Rat and Dog after Intravenous Administration. Xenobiotica 1994, 24, 79–92. [Google Scholar] [CrossRef]
- Kosinsky, Y.; Peskov, K.; Stanski, D.R.; Wetmore, D.; Vinetz, J. Semi-Mechanistic Pharmacokinetic-Pharmacodynamic Model of Camostat Mesylate-Predicted Efficacy against SARS-CoV-2 in COVID-19. Microbiol. Spectr. 2022, 10, e02167-21. [Google Scholar] [CrossRef]
- Peiffer, A.L.; Garlick, J.M.; Wu, Y.; Soellner, M.B.; Brooks III, C.L.; Mapp, A.K. TMPRSS2 Inhibitor Discovery Facilitated through an in Silico and Biochemical Screening Platform. ACS Med. Chem. Lett. 2023, 14, 860–866. [Google Scholar] [CrossRef]
- Ramjee, M.K.; Henderson, I.M.; McLoughlin, S.B.; Padova, A. The Kinetic and Structural Characterization of the Reaction of Nafamostat with Bovine Pancreatic Trypsin. Thromb. Res. 2000, 98, 559–569. [Google Scholar] [CrossRef] [PubMed]
- Sun, G.; Sui, Y.; Zhou, Y.; Ya, J.; Yuan, C.; Jiang, L.; Huang, M. Structural Basis of Covalent Inhibitory Mechanism of TMPRSS2-Related Serine Proteases by Camostat. J. Virol. 2021, 95, e00861-21. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; An, L.; Zhang, L.; Wang, R.; Tian, Y.; Zhang, Z. Identification of Impurities in Nafamostat Mesylate Using HPLC-IT-TOF/MS: A Series of Double-Charged Ions. J. Pharm. Anal. 2020, 10, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.P.; Vandenhende, F.R.; DeSante, K.A.; Farid, N.A.; Welch, P.A.; Callaghan, J.T.; Forgue, S.T. Confidence Interval Criteria for Assessment of Dose Proportionality. Pharm. Res. 2000, 17, 1278–1283. [Google Scholar] [CrossRef] [PubMed]
- Sukarnjanaset, W.; Wattanavijitkul, T.; Jarurattanasirikul, S. Evaluation of FOCEI and SAEM Estimation Methods in Population Pharmacokinetic Analysis Using NONMEM® across Rich, Medium, and Sparse Sampling Data. Eur. J. Drug Metab. Pharmacokinet. 2018, 43, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Metzler, C.M.; Tong, D.D.M. Computational Problems of Compartment Models with Michaelis-Menten-type Elimination. J. Pharm. Sci. 1981, 70, 733–737. [Google Scholar] [CrossRef]
- Keizer, R.J.; Karlsson, M.O.; Hooker, A. Modeling and Simulation Workbench for NONMEM: Tutorial on Pirana, PsN, and Xpose. CPT Pharmacomet. Syst. Pharmacol. 2013, 2, 1–9. [Google Scholar] [CrossRef]
- Thai, H.-T.; Mentré, F.; Holford, N.H.; Veyrat-Follet, C.; Comets, E. Evaluation of Bootstrap Methods for Estimating Uncertainty of Parameters in Nonlinear Mixed-Effects Models: A Simulation Study in Population Pharmacokinetics. J. Pharmacokinet. Pharmacodyn. 2014, 41, 15–33. [Google Scholar] [CrossRef]
- Kim, Y.-S.; Jeon, S.-H.; Kim, J.; Koh, J.H.; Ra, S.W.; Kim, J.W.; Kim, Y.; Kim, C.K.; Shin, Y.C.; Kang, B.D. A Double-Blind, Randomized, Placebo-Controlled, Phase II Clinical Study To Evaluate the Efficacy and Safety of Camostat Mesylate (DWJ1248) in Adult Patients with Mild to Moderate COVID-19. Antimicrob. Agents Chemother. 2023, 67, e00452-22. [Google Scholar] [CrossRef]
- Sai, J.K.; Suyama, M.; Kubokawa, Y.; Matsumura, Y.; Inami, K.; Watanabe, S. Efficacy of Camostat Mesilate against Dyspepsia Associated with Non-Alcoholic Mild Pancreatic Disease. J. Gastroenterol. 2010, 45, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Kitagawa, J.; Arai, H.; Iida, H.; Mukai, J.; Furukawa, K.; Ohtsu, S.; Nakade, S.; Hikima, T.; Haranaka, M.; Uemura, N. A Phase I Study of High Dose Camostat Mesylate in Healthy Adults Provides a Rationale to Repurpose the TMPRSS2 Inhibitor for the Treatment of COVID-19. Clin. Transl. Sci. 2021, 14, 1967–1976. [Google Scholar] [CrossRef] [PubMed]
- Low Risk of the TMPRSS2 Inhibitor Camostat Mesylate and Its Metabolite GBPA to Act as Perpetrators of Drug-Drug Interactions—ScienceDirect. Available online: https://www.sciencedirect.com/science/article/pii/S0009279721000648?via%3Dihub (accessed on 17 March 2023).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Statistics | |||
|---|---|---|---|---|
| 100 mg | 200 mg | 300 mg | ||
| Sex, n (%) | Male | 5 (100) | 5 (100) | 5 (100) |
| Female | 0 (0) | 0 (0) | 0 (0) | |
| Age (years) | 26.8 (6.34) | 29.0 (5.56) | 28.0 (5.34) | |
| Weight (kg) | 70.1 (10.9) | 68.5 (10.9) | 74.5 (16.0) | |
| Height (cm) | 173.1 (7.19) | 172.8 (5.53) | 175.4 (6.97) | |
| BMI (kg/m2) | 23.3 (2.60) | 22.9 (2.93) | 24.0 (3.96) | |
| AST (IU/L) | 17.4 (4.56) | 16.6 (4.72) | 13.6 (6.27) | |
| ALT (IU/L) | 24.2 (8.76) | 24.8 (12.5) | 21.8 (12.3) | |
| eGFR (mL/min/1.73 m2) | 99.2 (10.7) | 113.8 (31.8) | 93.8 (15.3) | |
| Albumin (g/dL) | 4.42 (0.21) | 4.50 (0.12) | 4.58 (0.29) | |
| GBPA | GBA | |||||
|---|---|---|---|---|---|---|
| 100 mg | 200 mg | 300 mg | 100 mg | 200 mg | 300 mg | |
| Half-life (h) | 1.012 (0.122) | 1.034 (0.083) | 1.002 (0.058) | 1.942 (0.377) | 1.954 (0.565) | 2.407 (1.089) |
| Cmax (ng/mL) | 72.68 (26.42) | 156.8 (50.85) | 273.9 (108.8) | 175.5 (60.07) | 302.9 (55.26) | 376.9 (101.1) |
| AUClast (h × ng/mL) | 152.3 (63.68) | 307.4 (96.45) | 464.8 (150.5) | 618.2 (203.0) | 1036 (126.7) | 1270 (243.6) |
| AUCinf (h × ng/mL) | 156.5 (63.68) | 316.9 (100.1) | 477.5 (156.0) | 762.8 (242.9) | 1268 (194.5) | 1710 (268.3) |
| CL/F (L/h) | 141.7 (43.51) | 158.8 (27.88) | 179.6 (31.73) | 718.6 (247.5) | 675.1 (179.6) | 680.4 (202.9) |
| Vd (h) | 1046 (69.5) | 1006 (286.8) | 977.8 (265.4) | 404.5 (163.5) | 437.8 (86.23) | 604.8 (207.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, G.; Moon, H.-k.; Kim, T.; Yun, S.-h.; Yun, H.-y.; Hong, J.H.; Kim, D.-D. Safety Evaluation and Population Pharmacokinetics of Camostat Mesylate and Its Major Metabolites Using a Phase I Study. Pharmaceutics 2023, 15, 2357. https://doi.org/10.3390/pharmaceutics15092357
Kim G, Moon H-k, Kim T, Yun S-h, Yun H-y, Hong JH, Kim D-D. Safety Evaluation and Population Pharmacokinetics of Camostat Mesylate and Its Major Metabolites Using a Phase I Study. Pharmaceutics. 2023; 15(9):2357. https://doi.org/10.3390/pharmaceutics15092357
Chicago/Turabian StyleKim, Gwanyoung, Hyun-ki Moon, Taeheon Kim, So-hye Yun, Hwi-yeol Yun, Jang Hee Hong, and Dae-Duk Kim. 2023. "Safety Evaluation and Population Pharmacokinetics of Camostat Mesylate and Its Major Metabolites Using a Phase I Study" Pharmaceutics 15, no. 9: 2357. https://doi.org/10.3390/pharmaceutics15092357