
Evaluation of Two Osmosis-Based Methods for the Preparation of Drug Delivery Systems Based on Red Blood Cells
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
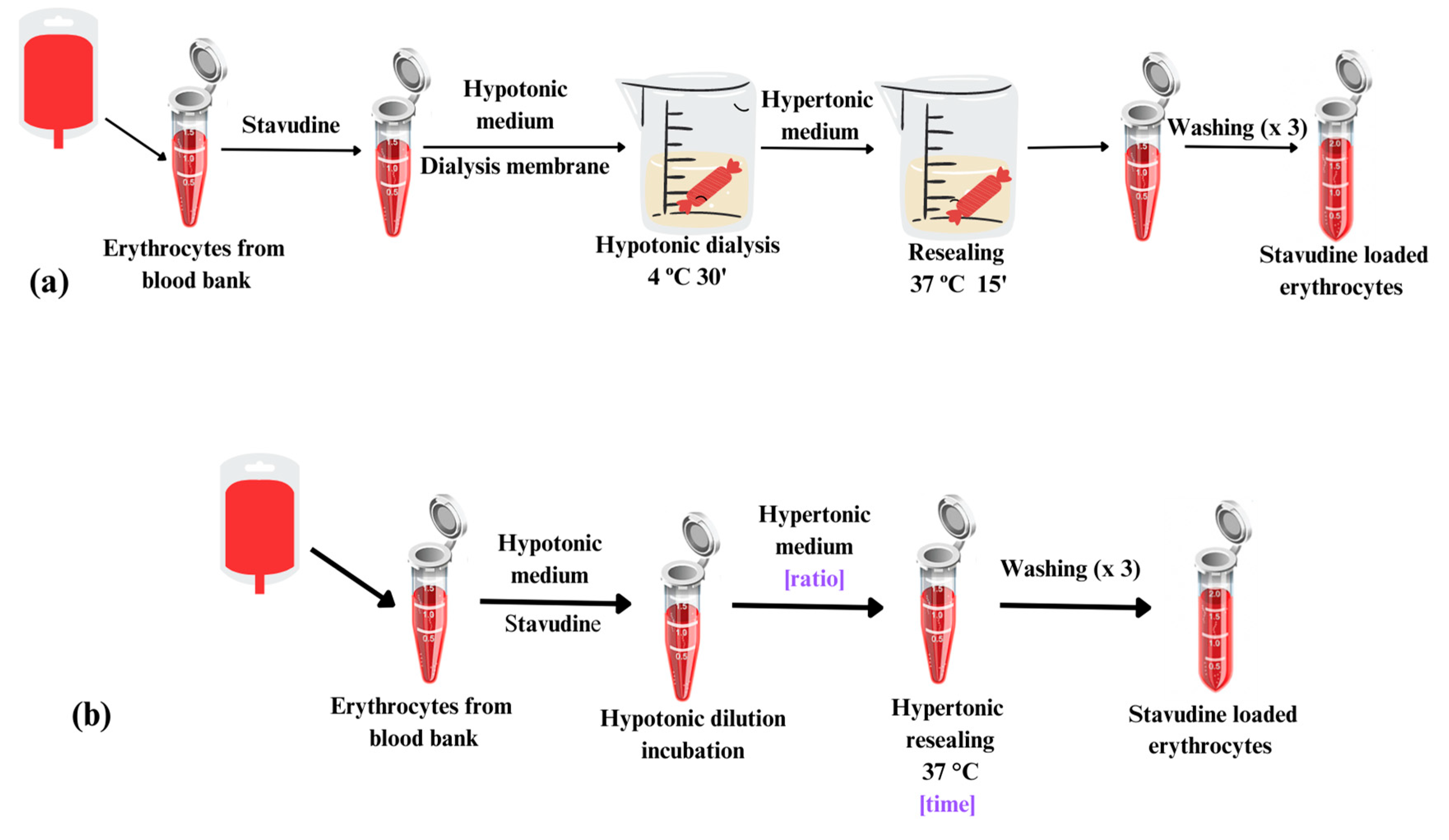
2.1. Loading Methods
2.2. Drug Encapsulation
2.3. Stavudine Quantification
2.4. Osmotic Fragility
2.5. Hematological Parameters
2.6. Microscopic Analysis
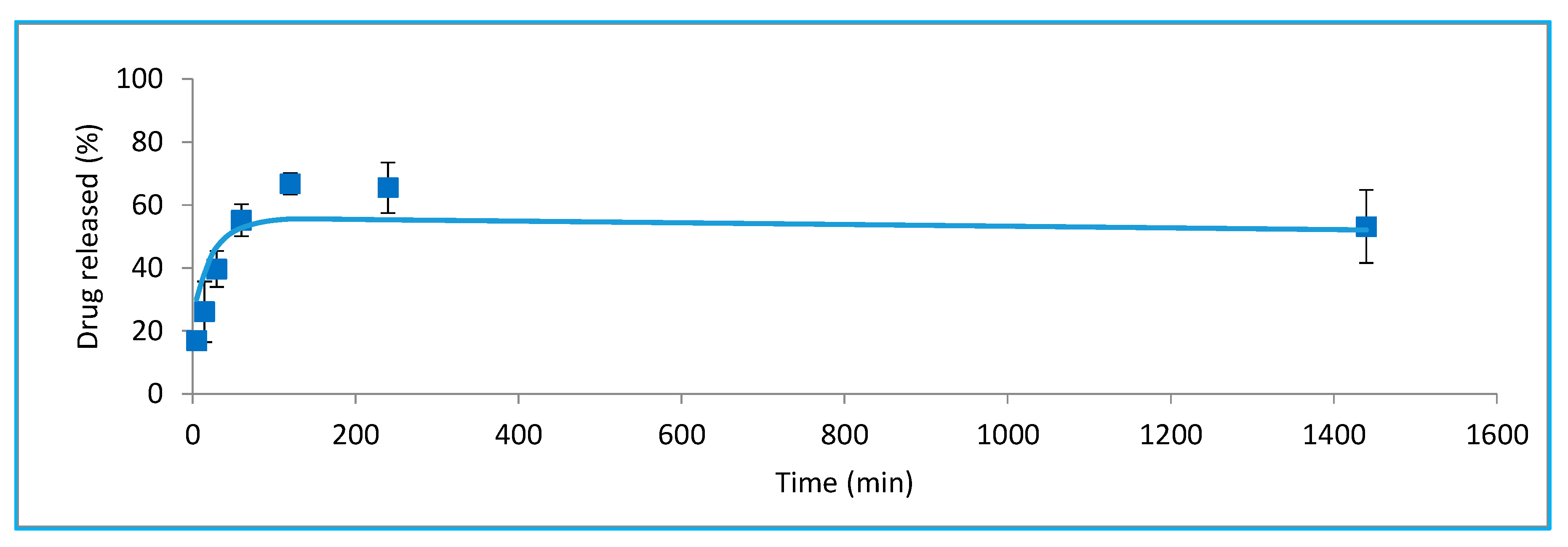
2.7. In Vitro Release
2.8. Statistical Analysis
3. Results and Discussion
3.1. Optimization of Resealing Conditions
3.1.1. Stavudine Encapsulation
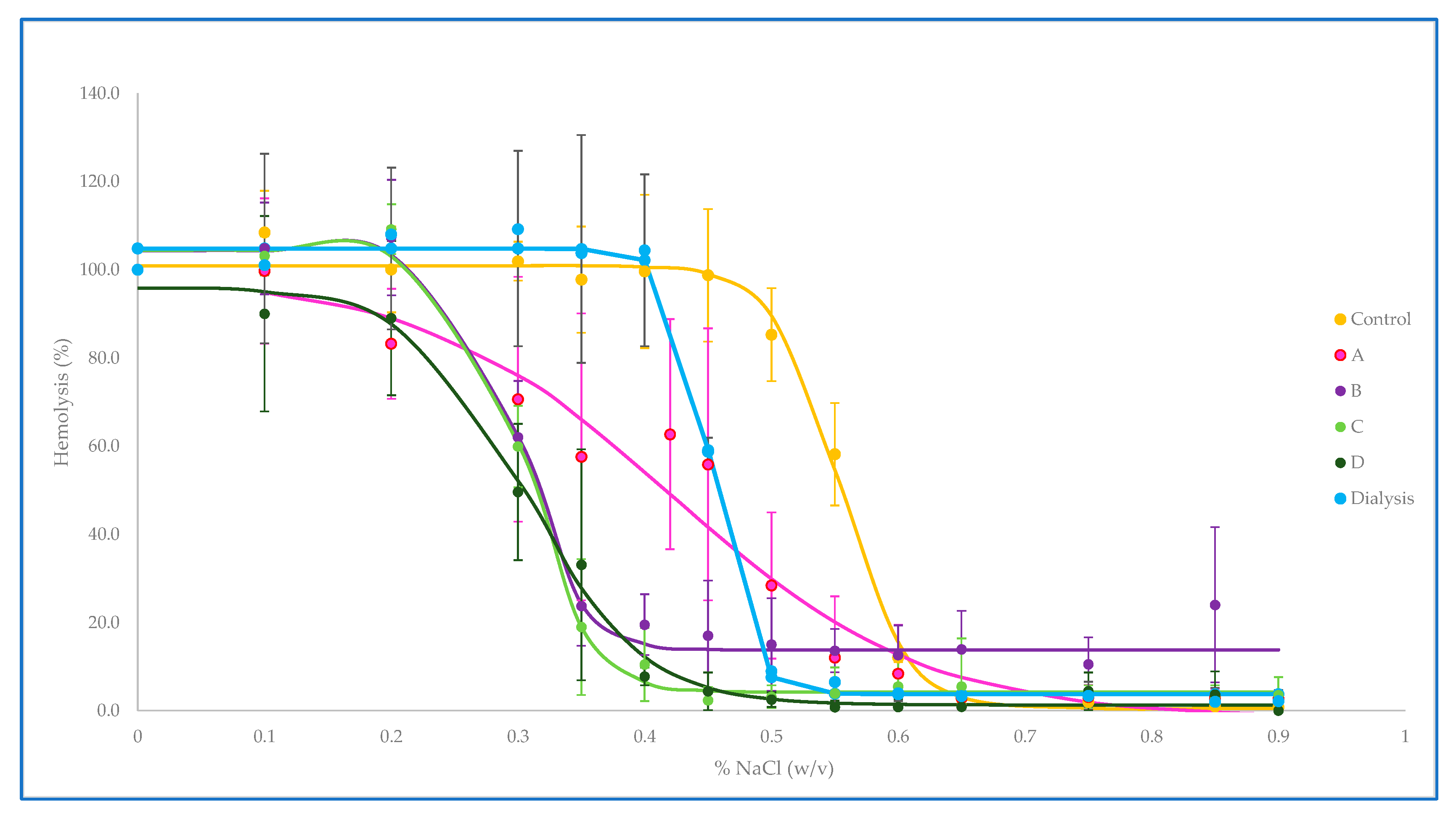
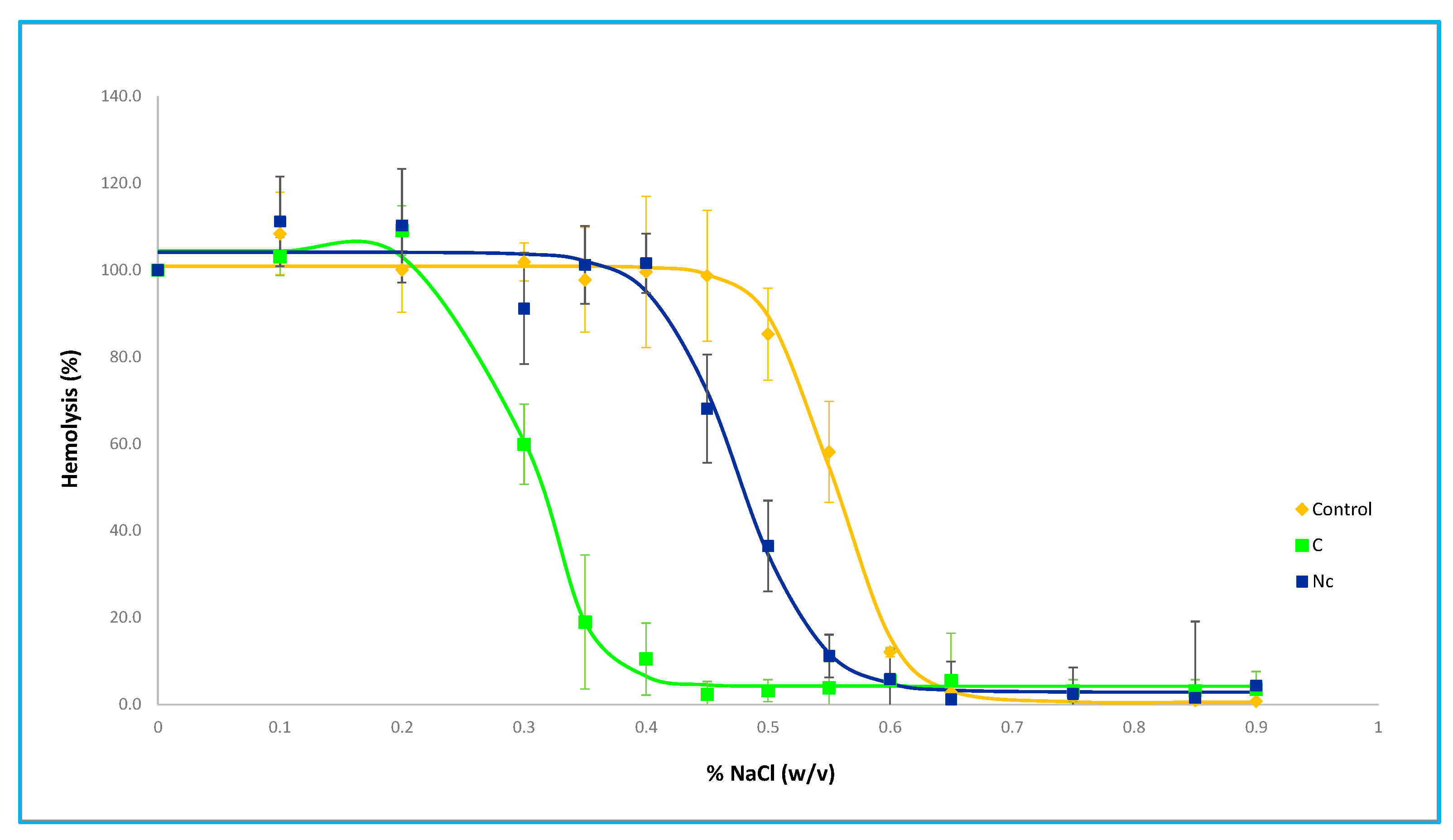
3.1.2. Osmotic Fragility
3.1.3. Hematological Parameters
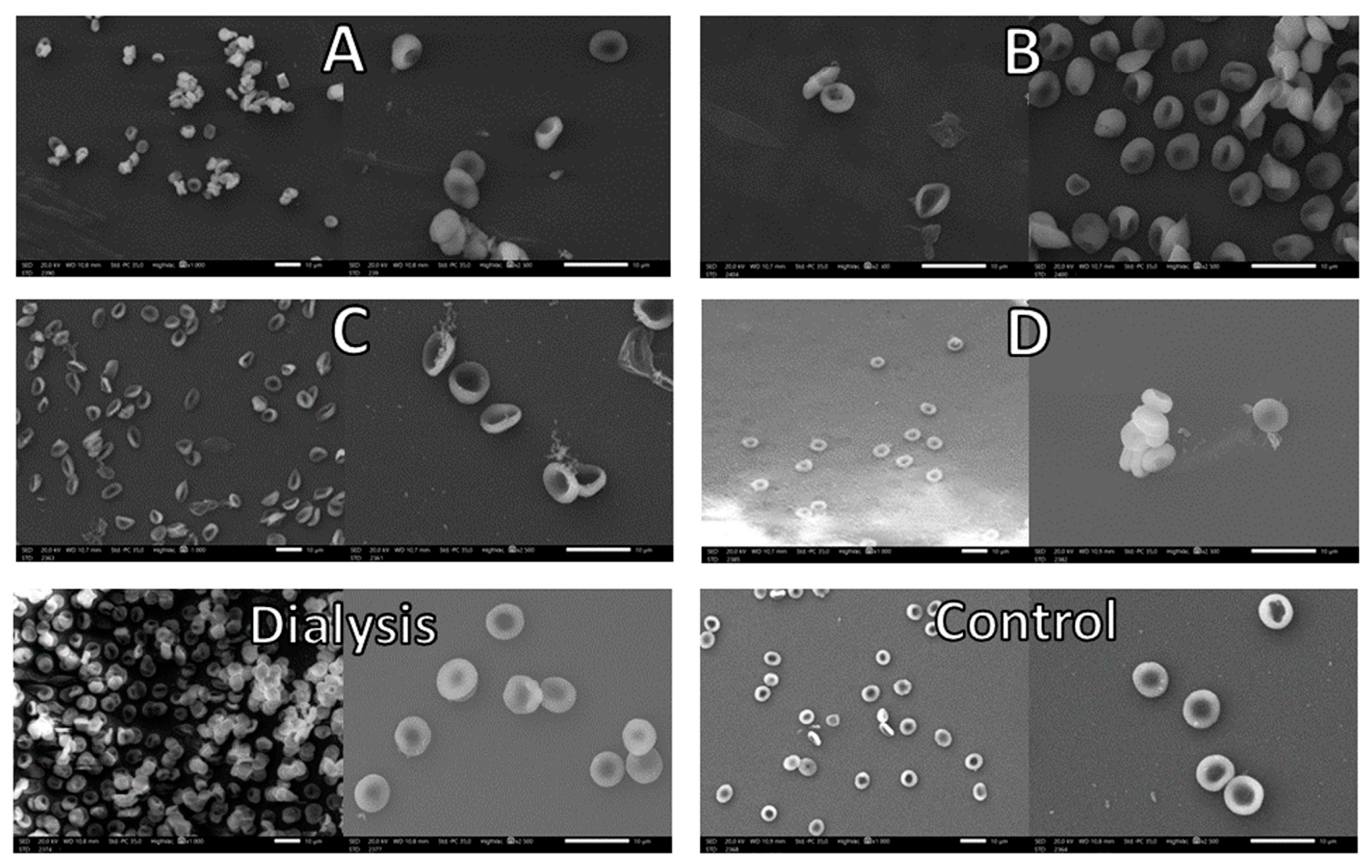
3.1.4. Morphology
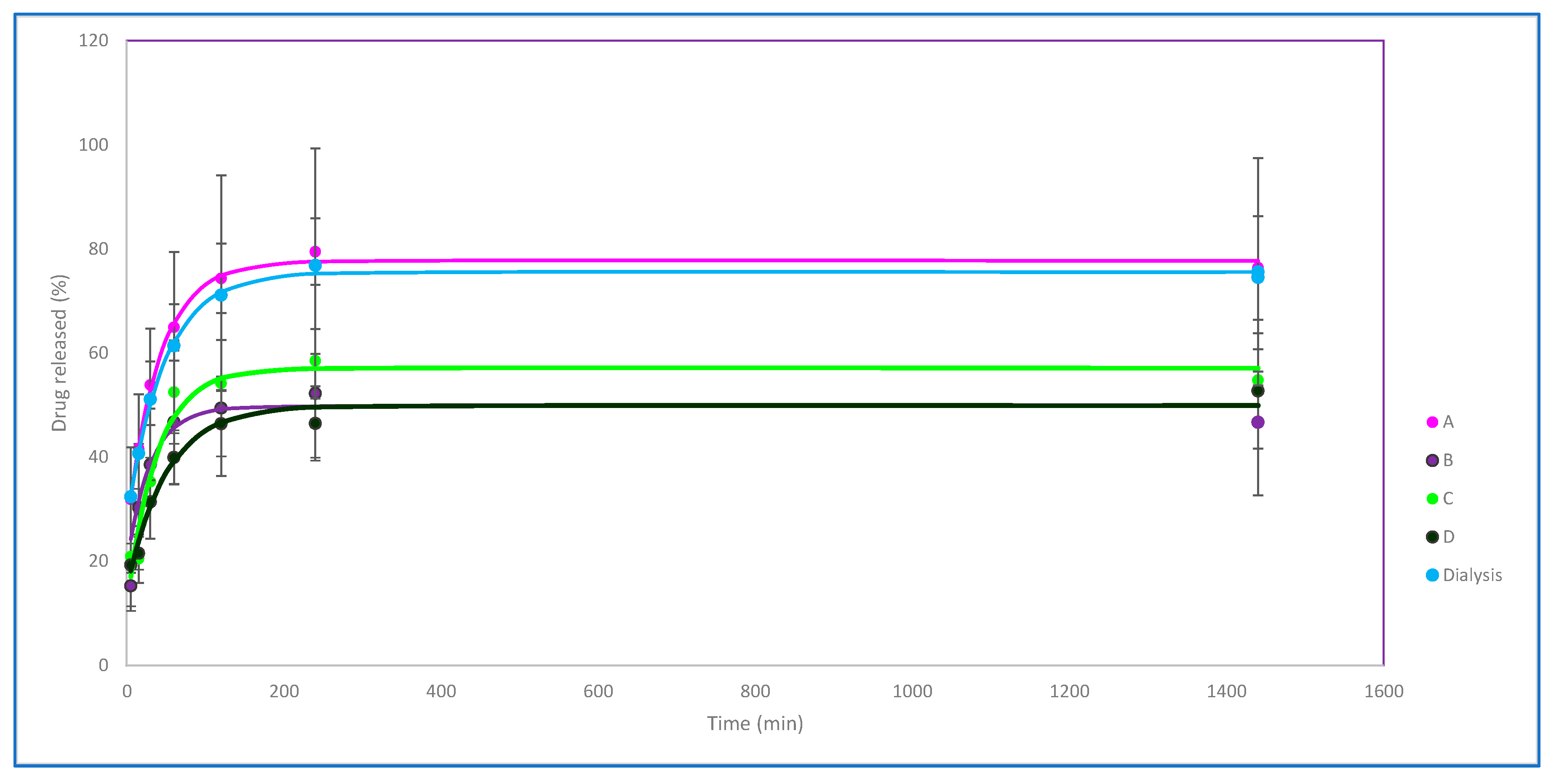
3.1.5. In Vitro Release
3.2. Comparative Analysis of Simplified Hypoosmotic Buffer Results
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sun, Y.; Su, J.; Liu, G.; Chen, J.; Zhang, X.; Zhang, R.; Jiang, M.; Qiu, M. Advances of blood cell-based drug delivery systems. Eur. J. Pharm. Sci. 2017, 96, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Han, K.; Ma, S.; Qi, X.; Guo, L.; Li, X. Blood cells as supercarrier systems for advanced drug delivery. Med. Drug Discov. 2022, 13, 100119. [Google Scholar] [CrossRef]
- Dong, H.; Tu, T.; Jiang, Y.; Yuan, Y.; Peng, F.; Deng, Y.; Ren, C.; Liu, C. Erythrocyte-based Drug Delivery: How Far from Clinical Application? Curr. Drug Deliv. 2023, 21, 52–64. [Google Scholar] [CrossRef] [PubMed]
- Rossi, L.; Pierigè, F.; Aliano, M.P.; Magnani, M. Ongoing Developments and Clinical Progress in Drug-Loaded Red Blood Cell Technologies. BioDrugs 2020, 34, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Millán, C.G.; Castañeda, A.Z.; Marinero, M.L.S.; Lanao, J.M. Factors associated with the performance of carrier erythrocytes obtained by hypotonic dialysis. Blood Cells Mol. Dis. 2004, 33, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Koleva, L.; Bovt, E.; Ataullakhanov, F.; Sinauridze, E. Erythrocytes as Carriers: From Drug Delivery to Biosensors. Pharmaceutics 2020, 12, 276. [Google Scholar] [CrossRef] [PubMed]
- López, S.C.B.; Meissner, K.E. Characterization of carrier erythrocytes for biosensing applications. J. Biomed. Opt. 2017, 22, 91510. [Google Scholar] [CrossRef] [PubMed]
- Hamidi, M.; Tajerzadeh, H. Carrier Erythrocytes: An Overview. Drug Deliv. 2003, 10, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.; Wu, T.; Zhang, D.; Zhang, Z. Cell or Cell Membrane-Based Drug Delivery Systems. Theranostics 2015, 5, 863–881. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Ye, J.; Wang, Y.; Liu, Q.; Chung, H.S.; Kwon, Y.M.; Shin, M.C.; Lee, K.; Yang, V.C. Cell-penetrating peptides meditated encapsulation of protein therapeutics into intact red blood cells and its application. J. Control. Release 2014, 176, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Rao, L.; Cai, B.; Bu, L.-L.; Liao, Q.-Q.; Guo, S.-S.; Zhao, X.-Z.; Dong, W.-F.; Liu, W. Microfluidic Electroporation-Facilitated Synthesis of Erythrocyte Membrane-Coated Magnetic Nanoparticles for Enhanced Imaging-Guided Cancer Therapy. ACS Nano 2017, 11, 3496–3505. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Raza, F.; Liu, Y.; Wei, Y.; Rong, R.; Zheng, M.; Yuan, W.; Su, J.; Qiu, M. Clinical progress and advanced research of red blood cells based drug delivery system. Biomaterials 2021, 279, 121202. [Google Scholar] [CrossRef] [PubMed]
- Millán, C.G.; Castañeda, A.Z.; López, F.G.; Marinero, M.L.S.; Lanao, J.M.; Arévalo, M. Encapsulation and In Vitro Evaluation of Amikacin-Loaded Erythrocytes. Drug Deliv. 2005, 12, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Millán, C.G.; Bax, B.E.; Castañeda, A.Z.; Marinero, M.L.S.; Lanao, J.M. In vitro studies of amikacin-loaded human carrier erythrocytes. Transl. Res. 2008, 152, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Zazo, H.; Colino, C.I.; Gutiérrez-Millán, C.; Cordero, A.A.; Bartneck, M.; Lanao, J.M. Physiologically Based Pharmacokinetic (PBPK) Model of Gold Nanoparticle-Based Drug Delivery System for Stavudine Biodistribution. Pharmaceutics 2022, 14, 406. [Google Scholar] [CrossRef] [PubMed]
- Briones, E.; Colino, C.I.; Millán, C.G.; Lanao, J.M. Increasing the selectivity of amikacin in rat peritoneal macrophages using carrier erythrocytes. Eur. J. Pharm. Sci. 2009, 38, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Coker, S.A.; Szczepiorkowski, Z.M.; Siegel, A.H.; Ferrari, A.; Mambrini, G.; Anand, R.; Hartman, R.D.; Benatti, L.; Dumont, L.J. A Study of the Pharmacokinetic Properties and the In Vivo Kinetics of Erythrocytes Loaded with Dexamethasone Sodium Phosphate in Healthy Volunteers. Transfus. Med. Rev. 2018, 32, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Qiu, M.; Guo, P.; Lian, Y.; Xu, E.; Su, J. Autologous Red Blood Cell Delivery of Betamethasone Phosphate Sodium for Long Anti-Inflammation. Pharmaceutics 2018, 10, 286. [Google Scholar] [CrossRef] [PubMed]
- Millán, C.G.; Castañeda, A.Z.; López, F.G.; Marinero, M.L.S.; Lanao, J.M. Pharmacokinetics and biodistribution of amikacin encapsulated in carrier erythrocytes. J. Antimicrob. Chemother. 2008, 61, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Robert, M.; Laperrousaz, B.; Piedrahita, D.; Gautier, E.-F.; Nemkov, T.; Dupuy, F.; Nader, E.; Salnot, V.; Mayeux, P.; D’Alessandro, A.; et al. Multiparametric characterization of red blood cell physiology after hypotonic dialysis based drug encapsulation process. Acta Pharm. Sin. B 2022, 12, 2089–2102. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Resealing Conditions | Ratio (v:v) | Time (min) |
|---|---|---|
| A | 1:0.5 | 15 |
| B | 1:1.5 | 15 |
| C | 1:0.5 | 30 |
| D | 1:1.5 | 30 |
| Concentration (mg/mL) * | Efficiency (%) | Encapsulated Drug per Cell Number (mg/×1010 Cells) | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| A | 0.28 | 0.10 | 26.11 | 9.73 | 0.33 | 0.20 |
| B | 0.28 | 0.14 | 24.81 | 14.67 | 0.68 | 0.16 |
| C | 0.63 | 0.16 | 32.86 | 12.60 | 1.64 | 0.41 |
| D | 0.29 | 0.12 | 29.80 | 8.49 | 0.60 | 0.17 |
| Dialysis | 0.40 | 0.22 | 19.04 | 7.17 | 0.66 | 0.59 |
| Control | A | B | C | D | Dialysis |
|---|---|---|---|---|---|
| 0.55 | 0.42 | 0.31 | 0.31 | 0.30 | 0.46 |
| Control | Control Erythrocytes | A | B | C | D | Dialysis |
|---|---|---|---|---|---|---|
| Hematocrit (%) | 47.23 ± 3.45 | 63.73 ± 2.50 | 69.53 ± 2.25 | 69.27 ± 0.64 | 66.73 ± 6.71 | 62.00 ± 5.24 |
| HGB (g/dL) | 15.63 ± 0.92 | 21.53 ± 1.03 | 23.53 ± 1.33 | 23.27 ± 0.64 | 22.4 ± 2.90 | 20.20 ± 1.91 |
| RBCS (number/μL) | 5.12 × 106 ±4.17 × 105 | 7.11 × 106 ±2.91 × 105 | 7.79 × 106 ±3.19 × 105 | 7.69 × 106 ±1.86 × 105 | 7.47 × 106 ±7.91 × 105 | 7.21 × 106 ±5.34 × 105 |
| RDW * | 13.70 ± 0.26 | 13.40 ± 0.50 | 13.13 ± 0.12 | 13.47 ± 0.93 | 13.40 ± 0.30 | 17.40 ± 0.70 |
| MCV (fL) * | 92.30 ± 1.42 | 89.69 ± 0.32 | 89.32 ± 0.76 | 90.14 ± 1.33 | 89.33 ± 0.48 | 85.99 ± 1.24 |
| HCM (pg) * | 30.55 ± 1.14 | 30.29 ± 0.27 | 30.21 ± 0.47 | 30.27 ± 0.23 | 30.02 ± 0.73 | 28.00 ± 0.73 |
| CHCM (g/dL) | 33.10 ± 0.80 | 33.78 ± 0.42 | 33.83 ± 0.81 | 33.59 ± 0.64 | 33.60 ± 0.99 | 32.57 ± 0.95 |
| Control | A | B | C | D | Dialysis |
|---|---|---|---|---|---|
| 6.64 ± 0.45 | 5.59 ± 0.61 | 6.29 ± 0.52 | 6.68 ± 0.69 | 5.99 ± 0.53 | 6.00 ± 0.36 |
| Control | Control Erythrocytes | C | Nc |
|---|---|---|---|
| Hematocrit (%) * | 47.23 ± 3.45 | 69.27 ± 0.64 | 65.00 ± 1.261 |
| HGB (g/dL) * | 15.63 ± 0.92 | 23.27 ± 0.64 | 21.50 ± 0.38 |
| RBCS (number/µL) | 5.12 × 106 ±4.17 × 105 | 7.69 × 106 ±1.86 × 105 | 7.74 × 106 ±1.45 × 105 |
| RDW | 13.70 ± 0.26 | 13.47 ± 0.93 | 16.45 ± 0.33 |
| VCM (fL) * | 92.30 ± 1.42 | 90.14 ± 1.33 | 84.03 ± 0.06 |
| HCM (pg) * | 30.55 ± 1.14 | 30.27 ± 0.23 | 27.80 ± 0.06 |
| CHCM (g/dL) | 33.10 ± 0.80 | 33.59 ± 0.64 | 33.08 ± 010 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutierrez-Millan, C.; Barez Diaz, C.; Alvarez Vizan, L.; Colino, C.I. Evaluation of Two Osmosis-Based Methods for the Preparation of Drug Delivery Systems Based on Red Blood Cells. Pharmaceutics 2023, 15, 2281. https://doi.org/10.3390/pharmaceutics15092281
Gutierrez-Millan C, Barez Diaz C, Alvarez Vizan L, Colino CI. Evaluation of Two Osmosis-Based Methods for the Preparation of Drug Delivery Systems Based on Red Blood Cells. Pharmaceutics. 2023; 15(9):2281. https://doi.org/10.3390/pharmaceutics15092281
Chicago/Turabian StyleGutierrez-Millan, Carmen, Celia Barez Diaz, Lydia Alvarez Vizan, and Clara I. Colino. 2023. "Evaluation of Two Osmosis-Based Methods for the Preparation of Drug Delivery Systems Based on Red Blood Cells" Pharmaceutics 15, no. 9: 2281. https://doi.org/10.3390/pharmaceutics15092281