

A Study on Pharmacokinetics of Acetylsalicylic Acid Mini-Tablets in Healthy Adult Males—Comparison with the Powder Formulation
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
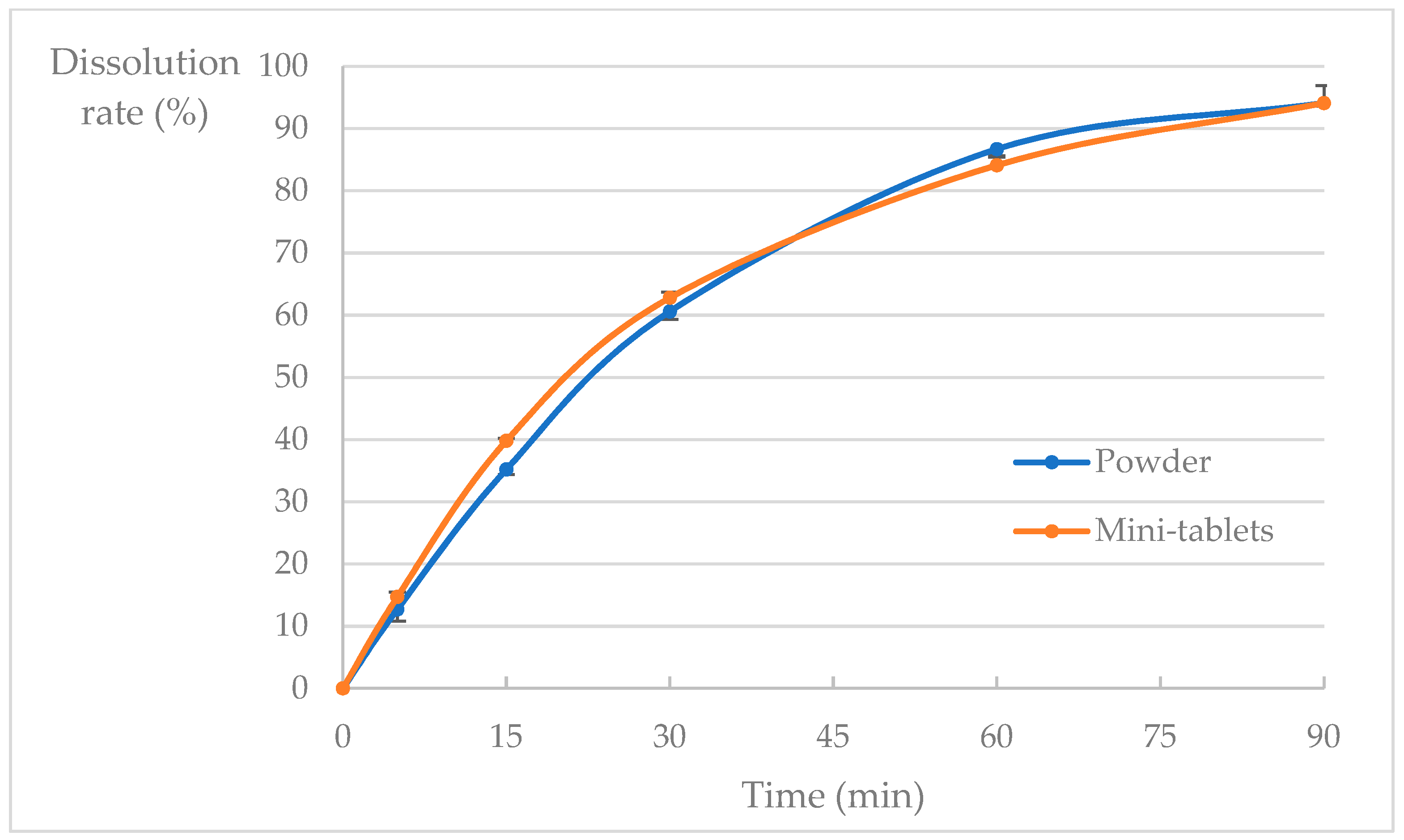
2.1. Dissolution Test
2.1.1. Test Method
- Test formulation: Acetylsalicylic acid mini-tablets.
- The paddle method (50 rpm; JP 1st fluid, pH 1.2, 900 mL; 37 ± 0.5 °C) was employed according to the JP guidance using the dissolution tester NTR-6400A (Toyama Sangyo Co., Osaka, Japan). Aliquots were sampled at 5, 15, 30, 60, and 90 min using the autosampler SAS-6000 (Toyama Sangyo Co., Osaka, Japan). The dissolution profile similarity was determined following the bioequivalence guidelines for generic drugs based on the following criteria when the standard drug product did not dissolve an average of ≥85% of the standard drug product within 30 min: when the average dissolution rate of the standard formulation is ≥85% at the specified test time, the average dissolution rate of the test formulation is within ±15% of the average dissolution rate of the standard formulation at two appropriate time points around 40% and 85%, or the f2 function value is ≥42.
2.1.2. Preparation and Storage of Acetylsalicylic Acid Powder
2.1.3. Preparation and Storage of Acetylsalicylic Acid Mini-Tablets
- Acetylsalicylic acid powder (50 g) was measured and placed in a plastic bag #1.
- Crystalline cellulose (10 g), corn starch (10 g), and mannitol (27 g) were introduced to a separate plastic bag #2, and put into plastic bag #1 containing acetylsalicylic acid.
- The mouth of the plastic bag #1 was closed after allowing the entry of sufficient air. The bag was rotated 200 times manually to thoroughly mix the powders.
- Magnesium stearate (3 g) was added to plastic bag #1 containing the powder mixed with acetylsalicylic acid, crystal cellulose, and mannitol.
- The mouth of the plastic bag was closed after allowing the entry of sufficient air. The bag was rotated 200 times by hand to thoroughly mix the powders.
- The mixed powder was visually inspected for foreign substances; if any foreign substance was identified, they were removed, or a fresh batch was initiated.
- The tablets were placed on a sieve, vibrated to shake off the adhering powder, and temporarily stored with a desiccant in an aluminum bag with a zip-lock cover lid.
- Ten mini-tablets were counted and divided into pile packers. The tablets were stored in an aluminum bag with a zipper, together with a desiccant, in an investigational drug control room, with constant temperature and humidity.
2.2. Subjects
2.3. Eligibility
2.3.1. Inclusion Criteria
- Age: Participants must be ≥20 ≤45 years old when providing consent.
- Gender: Male.
- The ability to provide consent, comply with the study rules, undergo a preliminary examination as specified in the research protocol, and report any subjective symptoms.
- Deemed eligible for participation by the principal investigator or sub-investigator based on the preliminary examination outlined in the research protocol.
2.3.2. Exclusion Criteria
- People with a medical history that may affect the evaluation and safety of the study, including drug abuse/dependence, alcohol abuse/dependence, or heart, liver, kidney, lung, eye, and blood diseases.
- People with a history or current presence of peptic ulcer.
- People with a bleeding tendency.
- People with aspirin-induced asthma.
- People taking medications (including dietary supplements) that may affect the evaluation and safety of the study.
- People with a history of drug allergies.
- People with excessive alcohol intake (inability to maintain abstinence from alcohol intake during the study period).
- People who have participated in another clinical research study within the past three months.
- People deemed ineligible by the principal investigator or sub-investigator based on the preliminary examination specified in the research protocol.
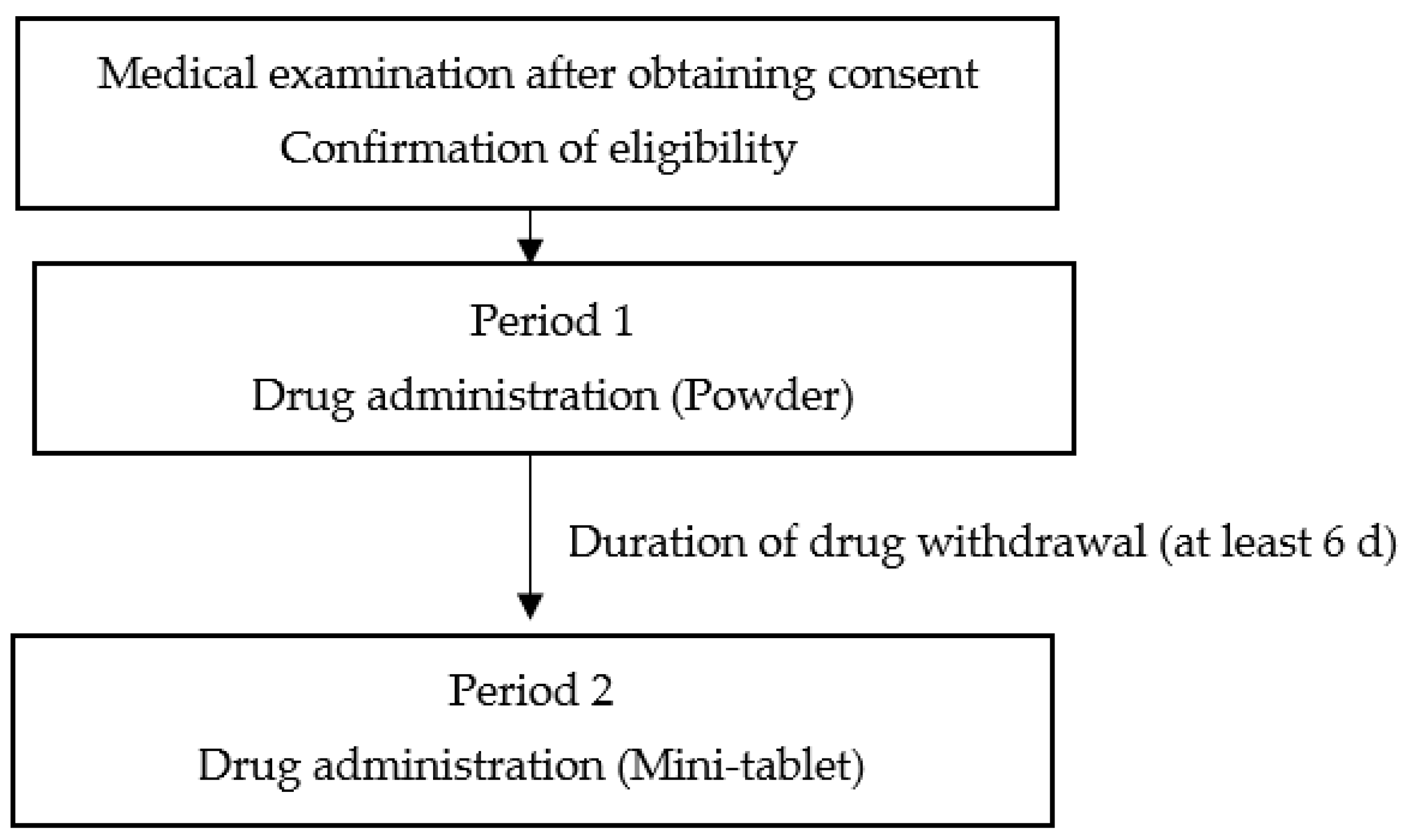
2.4. Study Design
2.5. Study Formulations
2.5.1. Drugs Administered
- Acetylsalicylic acid powder (manufactured and distributed by Yoshida Pharmaceutical Co., Ltd., Sayama, Japan): 1 g of this product contains 1 g of Japanese Pharmacopoeia acetylsalicylic acid.
- Acetylsalicylic acid mini-tablets (3 mm in diameter): Each tablet contained 10 mg of Japanese Pharmacopoeia acetylsalicylic acid. The test formulation was prepared in-house at the Pharmacy Department of Showa University Hospital.
2.5.2. Administration of Study Formulations
2.5.3. Observations and Blood Collection
2.6. Measurement of Blood Drug Concentration
2.7. Calculation of Pharmacokinetic Parameters
2.8. Statistical Analysis
2.8.1. Methods of Statistical Analysis
2.8.2. Primary Endpoint
2.8.3. Secondary Endpoints
2.8.4. Safety Evaluation
3. Results
3.1. Dissolution Test
3.2. Subjects
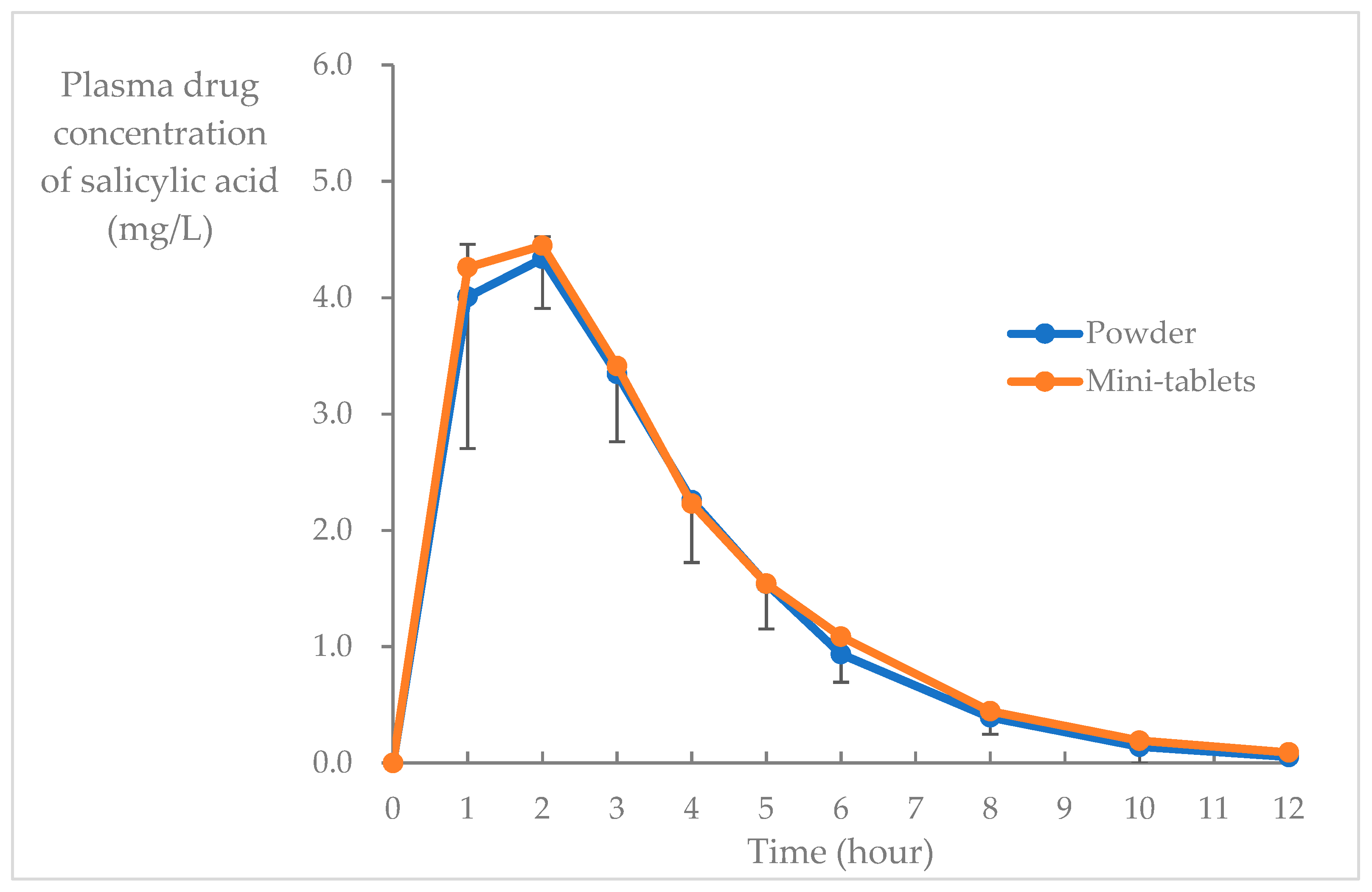
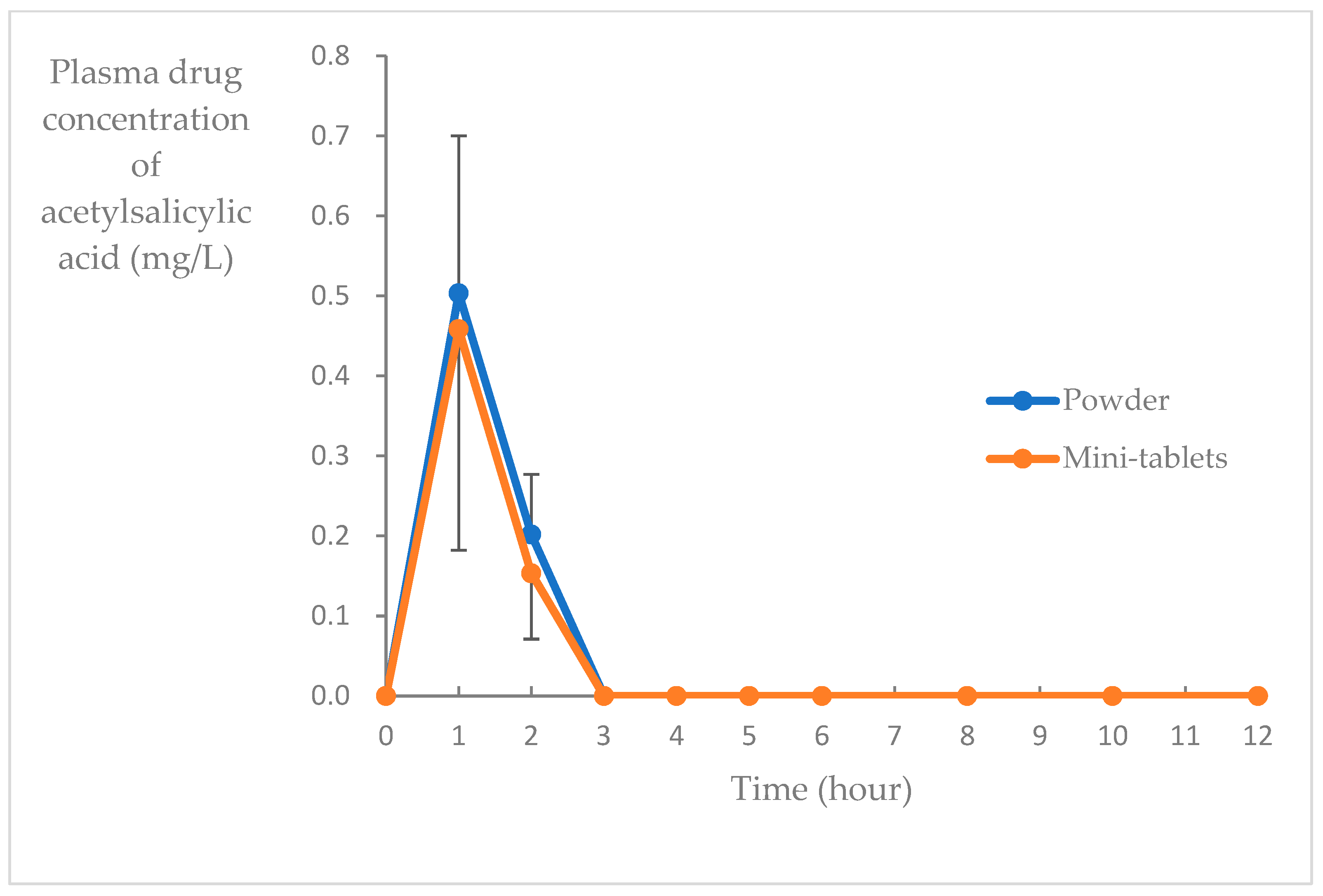
3.3. Blood Concentration
3.4. Safety Endpoints
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Development of Pediatric Medicines: Points to Consider in Formulation; WHO Technical Report Series No. 970; WHO Publications: Geneva, Switzerland, 2012.
- Kojima, J. Oral dosage forms for children: Acceptability and palatability. Yakugaku Zasshi 2015, 135, 245–247. [Google Scholar] [CrossRef]
- Nunn, T.; Williams, J. Formulation of medicines for children. Br. J. Clin. Pharmacol. 2005, 59, 674–676. [Google Scholar] [CrossRef]
- Alessandrini, E.; Brako, F.; Scarpa, M.; Lupo, M.; Bonifazi, D.; Pignataro, V.; Cavallo, M.; Cullufe, O.; Enache, C.; Nafria, B.; et al. Children’s preferences for oral dosage forms and their involvement in formulation research via EPTRI (European Paediatric Translational Research Infrastructure). Pharmaceutics 2021, 13, 730. [Google Scholar] [CrossRef]
- Thomson, S.A.; Tuleu, C.; Wong, I.C.K.; Keady, S.; Pitt, K.G.; Sutcliffe, A.G. Minitablets: New modality to deliver medicines to preschool-aged children. Pediatrics 2009, 123, e235–e238. [Google Scholar] [CrossRef]
- World Health Organization. Report of the Informal Expert Meeting on Dosage Forms of Medicines for Children; WHO Headquarters: Geneva, Switzerland, 2009; Available online: https://apps.who.int/iris/rest/bitstreams/52696/retrieve (accessed on 21 July 2023).
- Lajoinie, A.; Henin, E.; Kassai, B. Choisir la forme pharmaceutique orale la plus adaptée à l’enfant [Oral formulation of choice for children]. Arch. Pediatr. 2015, 22, 877–885. (In French) [Google Scholar] [CrossRef]
- Miyazaki, K.; Hida, N.; Kamiya, T.; Yamazaki, T.; Murayama, N.; Kuroiwa, M.; Kurata, N.; Ishikawa, Y.; Yamashita, S.; Nakamura, H.; et al. Comparative acceptability of mini-tablets, fine granules, and liquid formulations in young children: An exploratory randomized crossover study. J. Drug Deliv. Sci. Technol. 2022, 70, 103154. [Google Scholar] [CrossRef]
- Mitsui, N.; Hida, N.; Kamiya, T.; Yamazaki, T.; Miyazaki, K.; Saito, K.; Saito, J.; Yamatani, A.; Ishikawa, Y.; Nakamura, H.; et al. Swallowability of minitablets among children aged 6–23 months: An exploratory, randomized crossover study. Pharmaceutics 2022, 14, 198. [Google Scholar] [CrossRef]
- Shimomichi, Y.; Kawakami, Y.; Sugaya, K.; Takase, H. [Toward improving medication compliance in pediatric patients: A self-experimental case study] Syouni kanjya no hukuyaku konpuraiansu koujyou ni mukete Jikenrei ni okeru kufuu no teiji wo tsuujite (in Japanese). Jpn. J. Appl. Ther. 2018, 9, 15–20. [Google Scholar] [CrossRef]
- Japanese Society of Hospital Pharmacists. Guidelines for Preparation and Use of In-Hospital Products. 2014. Available online: https://www.jshp.or.jp/activity/guideline/20230206-2.pdf (accessed on 21 July 2023).
- Jenzer, H.; Fenton-May, V. Availability of medicines. In Practical Pharmaceutics; Bouwman-Boer, Y., Fenton-May, V., Le Brun, P., Eds.; Springer: Cham, Switzerland, 2015; pp. 25–49. [Google Scholar] [CrossRef]
- Kees, F.; Jehnich, D.; Grobecker, H. Simultaneous determination of acetylsalicylic acid and salicylic acid in human plasma by high-performance liquid chromatography. J. Chromatogr. B Biomed. Appl. 1996, 677, 172–177. [Google Scholar] [CrossRef]
- Jakka, S.; Rossbach, M. An economic perspective on personalized medicine. Hugo J. 2013, 7, 1. [Google Scholar] [CrossRef] [Green Version]
- Zuccari, G.; Alfei, S.; Marimpietri, D.; Iurilli, V.; Barabino, P.; Marchitto, L. Mini-tablets: A valid strategy to combine efficacy and safety in pediatrics. Pharmaceuticals 2022, 17, 108. [Google Scholar] [CrossRef] [PubMed]
- Klingmann, V.; Spomer, N.; Lerch, C.; Stoltenberg, I.; Frömke, C.; Bosse, H.M.; Breitkreutz, J.; Meissner, T. Favorable acceptance of mini-tablets compared with syrup: A randomized controlled trial in infants and preschool children. J. Pediatr. 2013, 163, 1728–1732.e1. [Google Scholar] [CrossRef] [PubMed]
- Spomer, N.; Klingmann, V.; Stoltenberg, I.; Lerch, C.; Meissner, T.; Breitkreutz, J. Acceptance of uncoated mini-tablets in young children: Results from a prospective exploratory cross-over study. Arch. Dis. Child 2012, 97, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Klingmann, V.; Seitz, A.; Meissner, T.; Breitkreutz, J.; Moeltner, A.; Bosse, H.M. Acceptability of uncoated mini-tablets in neonates—A randomized controlled trial. J. Pediatr. 2015, 167, 893–896.e2. [Google Scholar] [CrossRef] [PubMed]
- Klingmann, V.; Linderskamp, H.; Meissner, T.; Mayatepek, E.; Moeltner, A.; Breitkreutz, J.; Bosse, H.M. Acceptability of multiple uncoated minitablets in infants and toddlers: A Randomized Controlled Trial. J. Pediatr. 2018, 201, 202–207.e1. [Google Scholar] [CrossRef] [PubMed]
- Weiss, H.J.; Aledort, L.M. Impaired platelet-connective-tissue reaction in man after aspirin ingestion. Lancet 1967, 2, 495–497. [Google Scholar] [CrossRef]
- Antiplatelet Trialists’ Collaboration. Collaborative overview of randomised trials of antiplatelet therapy—1: Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients. BMJ 1994, 308, 81–106. [Google Scholar] [CrossRef]
- Lewis, H.D., Jr.; Davis, J.W.; Archibald, D.G.; Steinke, W.E.; Smitherman, T.C.; Doherty, J.E., 3rd; Schnaper, H.W.; LeWinter, M.M.; Linares, E.; Pouget, J.M.; et al. Protective effects of aspirin against acute myocardial infarction and death in men with unstable angina. Results of a veterans administration cooperative study. N. Engl. J. Med. 1983, 309, 396–403. [Google Scholar] [CrossRef]
- Cairns, J.A.; Gent, M.; Singer, J.; Finnie, K.J.; Froggatt, G.M.; Holder, D.A.; Jablonsky, G.; Kostuk, W.J.; Melendez, L.J.; Myers, M.G.; et al. Aspirin, sulfinpyrazone, or both in unstable angina—Results of a Canadian multicenter trial. N. Engl. J. Med. 1985, 313, 1369–1375. [Google Scholar] [CrossRef]
- Risk of myocardial infarction and death during treatment with low dose aspirin and intravenous heparin in men with unstable coronary artery disease. The RISC Group. Lancet 1990, 336, 827–830. [CrossRef]
- Ridker, P.M.; Manson, J.E.; Gaziano, J.M.; Buring, J.E.; Hennekens, C.H. Low-dose aspirin therapy for chronic stable angina. A randomized, placebo-controlled clinical trial. Ann. Intern. Med. 1991, 114, 835–839. [Google Scholar] [CrossRef]
- Nyman, I.; Larsson, H.; Wallentin, L. Prevention of serious cardiac events by low-dose aspirin in patients with silent myocardial ischaemia. The Research Group on Instability in Coronary Artery Disease in Southeast Sweden. Lancet 1992, 340, 497–501. [Google Scholar] [CrossRef]
- Juul-Möller, S.; Edvardsson, N.; Jahnmatz, B.; Rosén, A.; Sørensen, S.; Omblus, R. Double-blind trial of aspirin in primary prevention of myocardial infarction in patients with stable chronic angina pectoris. The Swedish Angina Pectoris Aspirin Trial (SAPAT) Group. Lancet 1992, 340, 1421–1425. [Google Scholar] [CrossRef]
- Elwood, P.C.; Cochrane, A.L.; Burr, M.L.; Sweetnam, P.M.; Williams, G.; Welsby, E.; Hughes, S.J.; Renton, R. A randomized controlled trial of acetyl salicylic acid in the secondary prevention of mortality from myocardial infarction. Br. Med. J. 1974, 1, 436–440. [Google Scholar] [CrossRef] [Green Version]
- Compound Summary Aspirin, PubChem. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Aspirin (accessed on 27 May 2023).
- Nagelschmitz, J.; Blunck, M.; Kraetzschmar, J.; Ludwig, M.; Wensing, G.; Hohlfeld, T. Pharmacokinetics and pharmacodynamics of acetylsalicylic acid after intravenous and oral administration to healthy volunteers. Clin. Pharmacol. Adv. Appl. 2014, 6, 51–59. [Google Scholar] [CrossRef] [Green Version]
- Marzo, A.; Dal Bo, L.; Verga, F.; Ceppi Monti, N.; Abbondati, G.; Tettamanti, R.A.; Crivelli, F.; Uhr, M.R.; Ismaili, S. Pharmacokinetics of diclofenac after oral administration of its potassium salt in sachet and tablet formulations. Arzneimittelforschung 2000, 50, 43–47. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time | Before Administration | 9:00 | 10:00 | 11:00 | 12:00 | 13:00 | 14:00 | 15:00 | 17:00 | 19:00 | 21:00 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Elapsed time (h) | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 8 | 10 | 12 | |
| Vital signs measurement | X | X | X | X | |||||||
| Medical examination | X | X | X | ||||||||
| Blood sampling | X | X | X | X | X | X | X | X | X | X | |
| Drug administration | X | ||||||||||
| Meal | X * | X * | |||||||||
| Subjective symptom survey | X | ||||||||||
| Adverse event observation | X |
| Salicylic Acid | Acetylsalicylic Acid | |||||
|---|---|---|---|---|---|---|
| 1st Period (Powder) | 2nd Period (Mini-Tablet) | Difference (2nd Period –1st Period) | 1st Period (Powder) | 2nd Period (Mini-Tablet) | Difference (2nd Period –1st Period) | |
| Cmax [mg/L] | 4.80 ± 0.79 [0.925–2.074] | 5.03 ± 0.97 [4.016–6.049] | 0.2313 [−0.898–1.361] p = 0.688 | 0.50 ± 0.20 [0.297–0.710] | 0.41 ± 0.24 [0.169–0.664] | −0.093 [−0.293–0.106] p = 0.063 |
| AUC0–12 [mg-h/L] | 18.0 ± 3.03 [14.82–21.19] | 18.9 ± 4.59 [14.82–21.19] | 0.880 [−1.640–3.400] p = 0.563 | 0.71 ± 0.27 [0.420–0.990] | 0.61 ± 0.36 [0.238–0.985] | −0.093 [−0.293–0.106] p = 0.313 |
| tmax [mg-h/L] | 1.67 ± 0.51 | 1.50 ± 0.54 | 1.000 | - | - | - |
| t1/2 [h] | 1.74 ± 0.24 | 1.86 ± 0.61 | 0.688 | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hida, N.; Yamazaki, T.; Fujita, Y.; Noda, H.; Sambe, T.; Ryu, K.; Mizukami, T.; Takenoshita, S.; Uchida, N.; Nakamura, A.; et al. A Study on Pharmacokinetics of Acetylsalicylic Acid Mini-Tablets in Healthy Adult Males—Comparison with the Powder Formulation. Pharmaceutics 2023, 15, 2079. https://doi.org/10.3390/pharmaceutics15082079
Hida N, Yamazaki T, Fujita Y, Noda H, Sambe T, Ryu K, Mizukami T, Takenoshita S, Uchida N, Nakamura A, et al. A Study on Pharmacokinetics of Acetylsalicylic Acid Mini-Tablets in Healthy Adult Males—Comparison with the Powder Formulation. Pharmaceutics. 2023; 15(8):2079. https://doi.org/10.3390/pharmaceutics15082079
Chicago/Turabian StyleHida, Noriko, Taigi Yamazaki, Yoshiaki Fujita, Hidehiro Noda, Takehiko Sambe, Kakei Ryu, Takuya Mizukami, Sachiko Takenoshita, Naoki Uchida, Akihiro Nakamura, and et al. 2023. "A Study on Pharmacokinetics of Acetylsalicylic Acid Mini-Tablets in Healthy Adult Males—Comparison with the Powder Formulation" Pharmaceutics 15, no. 8: 2079. https://doi.org/10.3390/pharmaceutics15082079