1. Introduction
Metastatic castration-resistant prostate cancer (mCRPC) is a fatal disease that follows an aggressive course with patients dying rapidly [
1]. In general, androgen receptor pathway inhibitor (ARPI) hormone therapy (e.g., abiraterone, enzalutamide, and apalutamide) and different taxanes-based chemotherapy regimens (cabazitaxel, docetaxel, and paclitaxel) achieve minimal improvement in these patients, resulting in progression of the disease [
2]. The prostate-specific membrane antigen (PSMA) is heavily expressed in 95% of cancer cells in patients with mCRPC. The expression degrees of PSMA directly associate with metastasis, progression, and androgen independence in prostate cancer [
3]. Lutetium-177 is a radionuclide that emits β radiation particles with a maximum tissue penetration of 2.2 mm (mean penetration 0.67 mm; maximum energy of 497 keV), sufficient to kill target tumor cells with a limited effect on neighboring normal cells. Thus, PSMA is used as a molecular target for radiotherapy of advanced mCRPC using specific
177Lu-radiopharmaceuticals as a third or fourth line of treatment, improving overall survival and analgesic control in the final phase of the disease [
4,
5].
Somatostatin receptors are commonly overexpressed in progressive and advanced neuroendocrine tumors (NET) [
6]. Twenty percent of the patients with NET present distant metastases, cases in which tumors are no longer resectable. Treatment options for unresectable metastatic disease include octreotide therapy (somatostatin analogs), first-line therapy, and targeted radiotherapy or interferon-alpha as second-line therapies [
7].
Pain is one of the most complicated symptoms in cancer patients, which negatively affects quality of life, especially in patients with prostate cancer bone metastases. Even with all the current scientific advances, the only option medical oncology can offer patients with advanced cancer is prolonged survival and improved quality of life (including pain relief), two aspects in which targeted radiotherapies with lutetium-177 have proven highly effective [
7,
8]. Unfortunately, only
177Lu-PSMA-617 (Pluvicto
TM, Novartis, Millburn, NJ, USA) and
177Lu-DOTATATE (Lutathera
TM, Novartis, Zaragoza, Spain) have been approved by the FDA (US Food and Drug Administration) as patented products for the treatment of advanced mCRPC and NET, respectively. Therefore, given the need for targeted radiotherapies to benefit a greater significant number of cancer patients whose cases are growing at an accelerated rate, we need to develop our own technology to enhance the benefits of lutetium-177 radiopharmaceuticals. Recently, we reported the design, synthesis, pharmaceutical formulation, preclinical evaluation, and assessment of biokinetics and dosimetry in patients of a novel
177Lu-labeled PSMA inhibitor (
177Lu-iPSMA) (Mexico-ININ) for prostate cancer therapy [
9,
10,
11], as well as the pharmaceutical grade preparation of
177Lu-DOTATOC as a patent-free radioligand molecularly recognized by somatostatin receptors (SSTR-2) for NET treatment [
11].
This translational research aimed to determine the efficacy and safety of 177Lu-iPSMA and 177Lu-DOTATOC developed as GMP pharmaceutical formulations for the treatment of progressive and advanced mCRPC and NET.
2. Materials and Methods
2.1. Preparation of Radiotracers
177LuCl
3 (40 GBq/mL, non-carrier-added in sterile 0.04 M HCl solution) was purchased from ITM, Garching bei München, Germany (EndolucinBeta). Analytical grade reagents were obtained from Merck Co., Boston, MA, USA and were used as received.
177Lu-iPSMA and
177Lu-DOTATOC were prepared according to the procedure reported by Luna-Gutierrez et al. [
11] using sterile and apyrogenic multidose lyophilized kits (ININ-Mexico) under GMP conditions. In brief, 1.5 mL of 1 M acetate buffer pH 5.0 was added to the
177LuCl
3 vial (40 GBq/mL). The total volume was used for the reconstitution of the iPSMA (DOTA-hydrazinylnicotinoyl-lysine(Nal)-urea-glutamate) or DOTATOC (DOTA-Tyr
3-octreotide) lyophilized kits followed by heating at 95 °C for 30 min (in a dry bath). Finally, the volume was adjusted to 20 mL with injectable-grade water (Pisa, Mexico). Dosing was performed in syringes using a GMP module (Musa, Comecer, Castel Bolognese, Italy) (7.4 GBq/4 mL). Under this procedure,
177Lu-iPSMA was prepared from lyophilized kits using sterile solutions of
177LuCl
3 for kit reconstitution without further purification or sterilization steps and radiochemical synthesizers. The quality control procedure evaluated parameters such as radiochemical purity (reversed-phase HPLC), sterility, bacterial endotoxins, pH, color, and appearance using the Mexican Pharmacopeia methods.
68Ga was obtained from a
68Ge/
68Ga generator (ITM, Baden-Württemberg, Germany).
68Ga-iPSMA and
68Ga-DOTATOC were synthesized on an iQS Ga-68 Fluidic Labeling Module (ITG, Baden-Württemberg, Germany). [
99mTc]TcO
4Na was obtained from a GETEC (
99Mo/
99mTc generator) (ININ, La Marquesa, Mexico). [
99mTc]Tc-iPSMA and [
99mTc]Tc-Tyr
3-octreotide radiotracers were prepared from lyophilized kits (ININ-Mexico), as previously reported [
12,
13].
2.2. Radiochemical Purity Assessment
Radiochemical purities over 95% were verified by radio-HPLC (Waters; Empower Software; Orlando, FL, USA) using a C18 column (µBondapak: 10 µm, 3.9 × 300 mm). A linear gradient in 20 min from 100% to 25% of solvent A (0.1% TFA/water) and from 0% to 75% of solvent B (0.1% TFA/acetonitrile) at a 1 mL/min flow rate was used. Retention times were as follows: 3–4 min (177LuCl3, [99mTc]TcO4Na, and 68GaCl3), 14–15 min (177Lu-iPSMA and 177Lu-DOTATOC), 13–14 min ([99mTc]Tc-iPSMA and [99mTc]Tc-Tyr3-octreotide), and 10–12 min (68Ga-iPSMA and 68Ga-DOTATOC).
2.3. Patients Characteristics and General Protocols
The
177Lu-iPSMA study enrolled 145 patients (median age: 69 years; range 57–86 years) with histologically-confirmed prostate cancer from four Mexican hospital institutions. Patients presented recurrent disease and confirmed biochemical progression (3 consecutive PSA elevations, separated by at least one week with PSA > 40 ng/mL) or radiological progression (2 or more bone lesions or in soft tissue or lymph node lesions). The Gleason score was 8 to 10 in 87% of the cases, and the rest of the patients had no score report. Most of the patients had previously been treated with Abiraterone or Enzalutamide (androgen receptor pathway inhibitor) with or without systemic chemotherapy (taxanes therapy) or radiation therapy (
Table 1). The primary diagnosis of prostate cancer was established in 2007–2019.
Patients received from 1 to 5 doses of
177Lu-iPSMA (7.4 GBq/dose, 120 µg of iPSMA peptide) every six weeks between January 2016 and May 2023. The number of
177Lu-iPSMA doses to be administered in each treatment was determined based on the tumor volume and the tumor standardized uptake value (SUVmax), estimated by
99mTc-iPSMA SPECT/CT or
68Ga-iPSMA PET/CT (radiological molecular imaging) [
10]. For example, tumor burden is related to the number of organic systems involved, including previous hematopoietic damage [
14]. Therefore, patients with higher bone tumor burden were selected to receive a maximum of 3 to 4 doses of
177Lu-iPSMA due to the increased likelihood of myelotoxicity. The biochemical and clinical condition of the patients was the second criterion for determining the number of doses to be administered. For the evaluation of survival, only patients who completed the administration of 3 to 5 doses of
177Lu-iPSMA between January 2016 and January 2020 were included (
n = 52). Time and cause of death were also recorded. Patients who died from causes other than prostate cancer were followed for cancer-specific survival until censoring. This group was compared with a historical control group of patients with mCRPC (
n = 31), which was retrospectively analyzed, given that they were diagnosed in the period 1989–2003, prior to the routine use of docetaxel, and were treated exclusively with antiandrogen withdrawal and palliative measures, which generally included analgesic management and oral prednisone (10 mg) in the terminal phase of the disease, as previously reported [
15]. Kaplan–Meier analysis, log-rank test, and proportional hazards analysis were performed. The response was evaluated using [
99mTc]Tc-iPSMA-SPECT/CT or
68Ga-iPSMA PET/CT images and serum PSA levels before and after
177Lu-iPSMA treatment. Patients initially selected with
99mTc-iPSMA/SPECT quantitative imaging were followed with the same imaging modality throughout the study, as were patients followed with
68Ga-iPSMA/PET. Radiologic progression-free survival was also determined from the start of targeted radiotherapy until disease progression.
The 177Lu-DOTATOC study enrolled 187 patients (83 men, median age: 64 years; range 51–81 years; and 104 women, median age: 63 years; range 48–74 years) diagnosed with metastatic and progressive NET from four Mexican hospital institutions. Eighty-three percent of the cases (n = 155) were patients with gastroenteropancreatic neuroendocrine tumors (GEP-NET: 67% gastroenteric and 33% pancreatic NET) and 17% (n = 32) other NETs (9 kidney, 17 lung, 5 ovary, and 1 thymus). Ninety-eight percent of the patients were previously treated with long-acting somatostatin analogs.
Patients received 2 to 8 doses of 177Lu-DOTATOC (7.4 GBq/dose, 200 µg of DOTATOC peptide) with co-infusion of an amino acid solution (hydrochloride L-lysine-25 g/hydrochloride L-arginine-25 g/0.9% NaCl) every 8 to 10 weeks between January 2016 and May 2023. For the evaluation of survival, only patients with NET who completed the administration of 4 to 8 doses of 177Lu-DOTATOC between January 2016 and January 2019 were included (n = 81). The time and cause of death were recorded. Patients who died from causes other than NET provided cancer-specific survival follow up until they were censored. Kaplan–Meier analysis was carried out. The response was evaluated using CT and [99mTc]Tc-Tyr3-octreotide-SPECT/CT or 68Ga-DOTATOC-PET/CT, and the clinical and biochemical (chromogranin A and serotonin levels) patient condition before and after therapy.
After 177Lu-iPSMA or 177Lu-DOTATOC administration, patients were hydrated with 0.5 L of water with urination before the radiological/nuclear image acquisition. All patients underwent [99mTc]Tc-MAG3 renal scintigraphy. Additional blood counts and laboratory parameters were performed to rule out clinically relevant bone marrow depression, hepatic function, and renal impairment. Each patient signed written informed consent.
The Hospital Institutional Review Boards approved the clinical trials for lutetium-177 therapies in compliance with the following approvals: (a) COFEPRIS (Federal Commission for Protection against Health Risks, the regulatory authority in Mexico) approval for 177Lu-iPSMA use in patients with progressive and advanced prostate cancer and 177Lu-DOTATOC use in patients with progressive and advanced NET (Registration numbers: 2763R2017 SSA, 2674R2016 SSA, and 1115R2019 SSA), under the ethical standards of the responsible committee on human studies (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008; (b) the GMP certificate issued by COFEPRIS to ININ facilities for the preparation of radiopharmaceuticals; and (c) the clinical background of PSMA inhibitors and Tyr3-octreotide for imaging approved by COFEPRIS (Registration numbers: 2764R2017 SSA and 0502R2017 SSA, respectively). The clinical protocol adhered to the ethical codes of objectivity, professional conduct, integrity, professional competence and due care, and confidentiality. Patients were informed that their identity and medical information would not be disclosed at any time. Therefore, in the collection of clinical data, patients would not face any risks related to the protection of confidentiality, which would be protected by coding his/her samples and information. The code is an identification number that does not contain personal information. Patients were also informed that their participation was voluntary. If the patient decided not to participate, it would not affect his/her relationship with his/her health care institution or his/her right to receive medical care or services to which he/she was entitled. If the patient decided to participate, he/she was free to withdraw consent and discontinue participation at any time without affecting his/her care by the health care institution.
3. Results
3.1. 177Lu-iPSMA
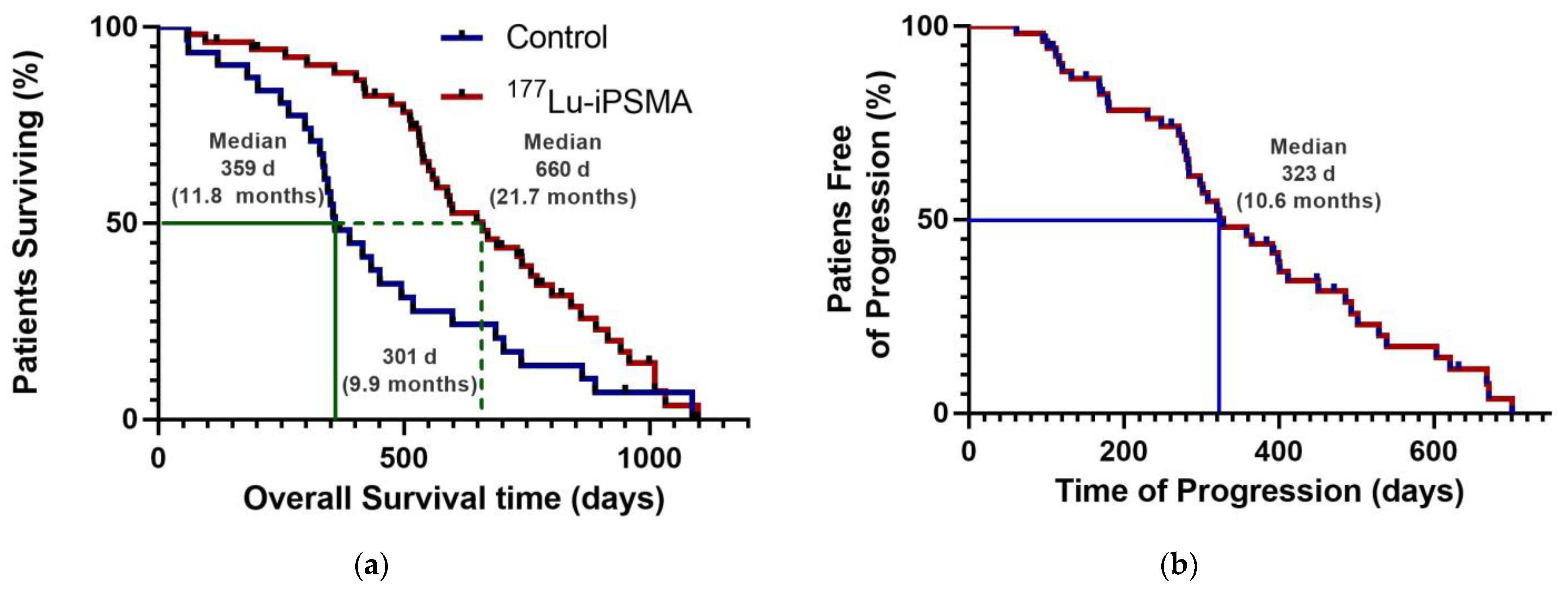
Patients with mPC who received three to five doses of
177Lu-iPSMA showed an overall survival of 660 days (21.7 months) (
Table 2;
Figure 1a) with decreased radiotracer tumor uptake (SUV) and PSA level in 80% (
n = 33) and 73% (
n = 30) of the subjects, respectively (
Table 2). Specifically, 52% of cases had a PSA decline of >50% after completing treatment.
The hazard ratio was 0.5650 (95% CI: 0.3391–0.9412), indicating a 43.5% reduction in the risk of death in favor of the
177Lu-iPSMA group (
Table 2). In addition, 50% of patients were free of progression at 323 d (10.6 months) after treatment (
Figure 1b).
177Lu-iPSMA showed an overall response rate of 36.6% (
Table 2).
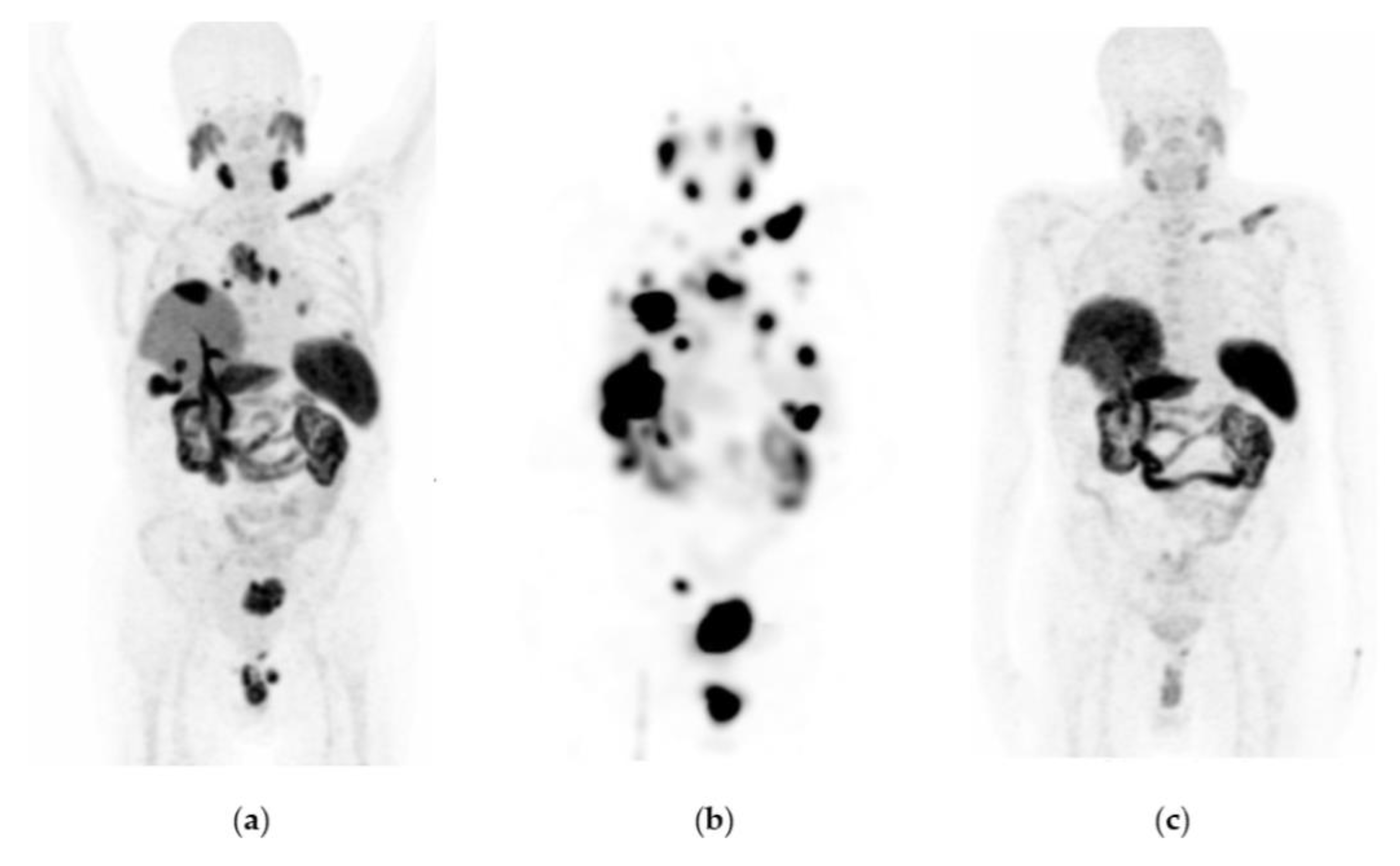
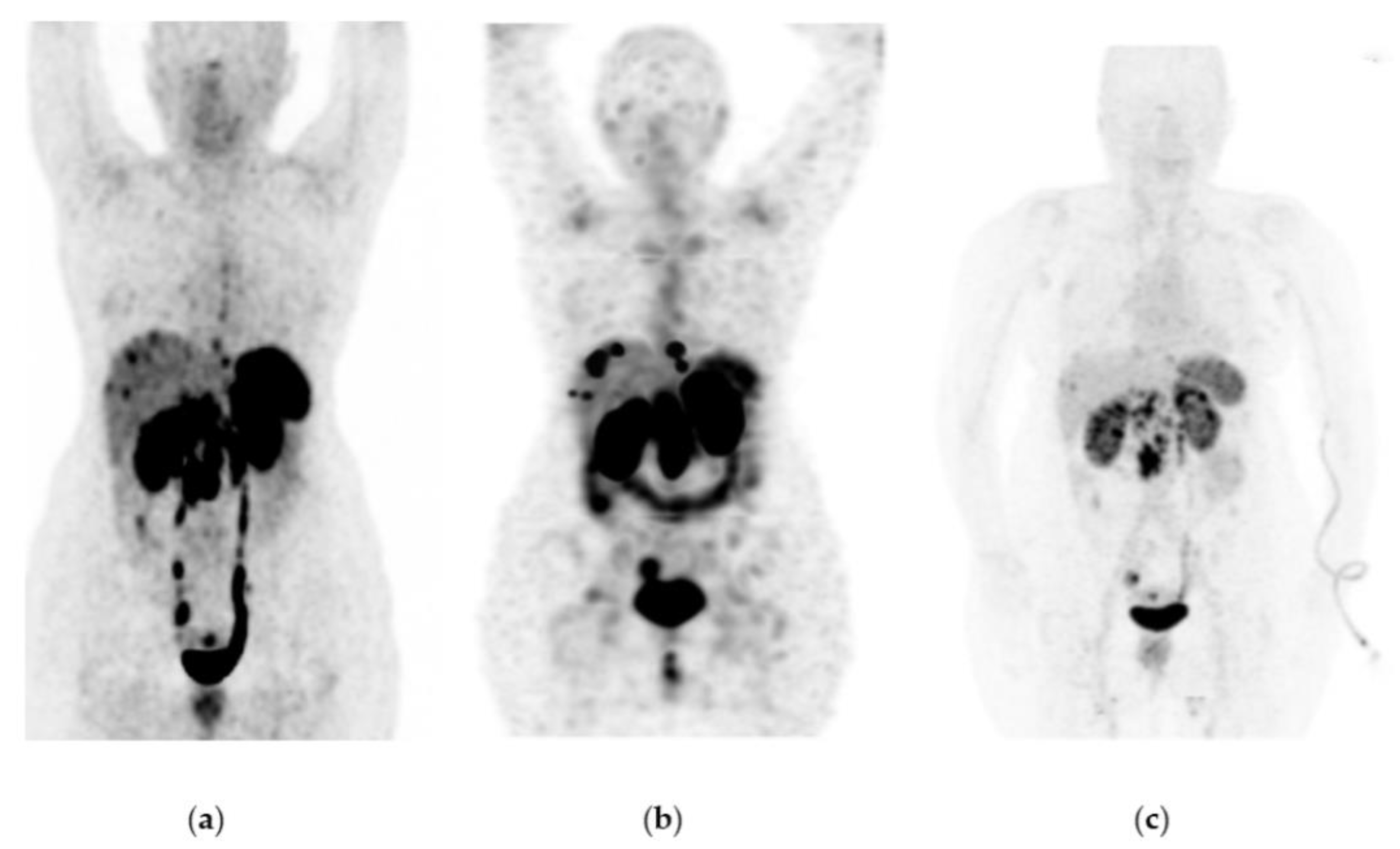
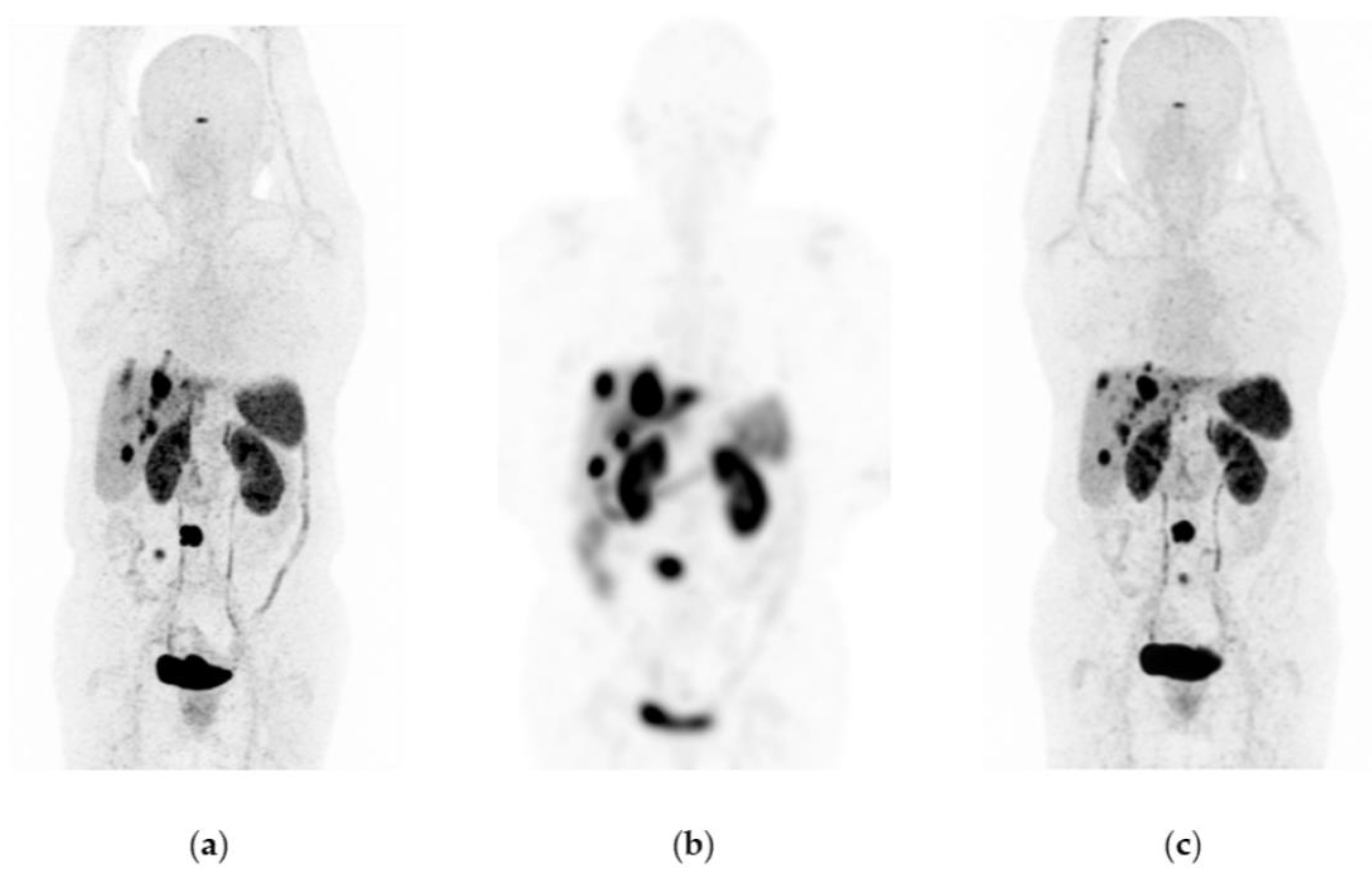
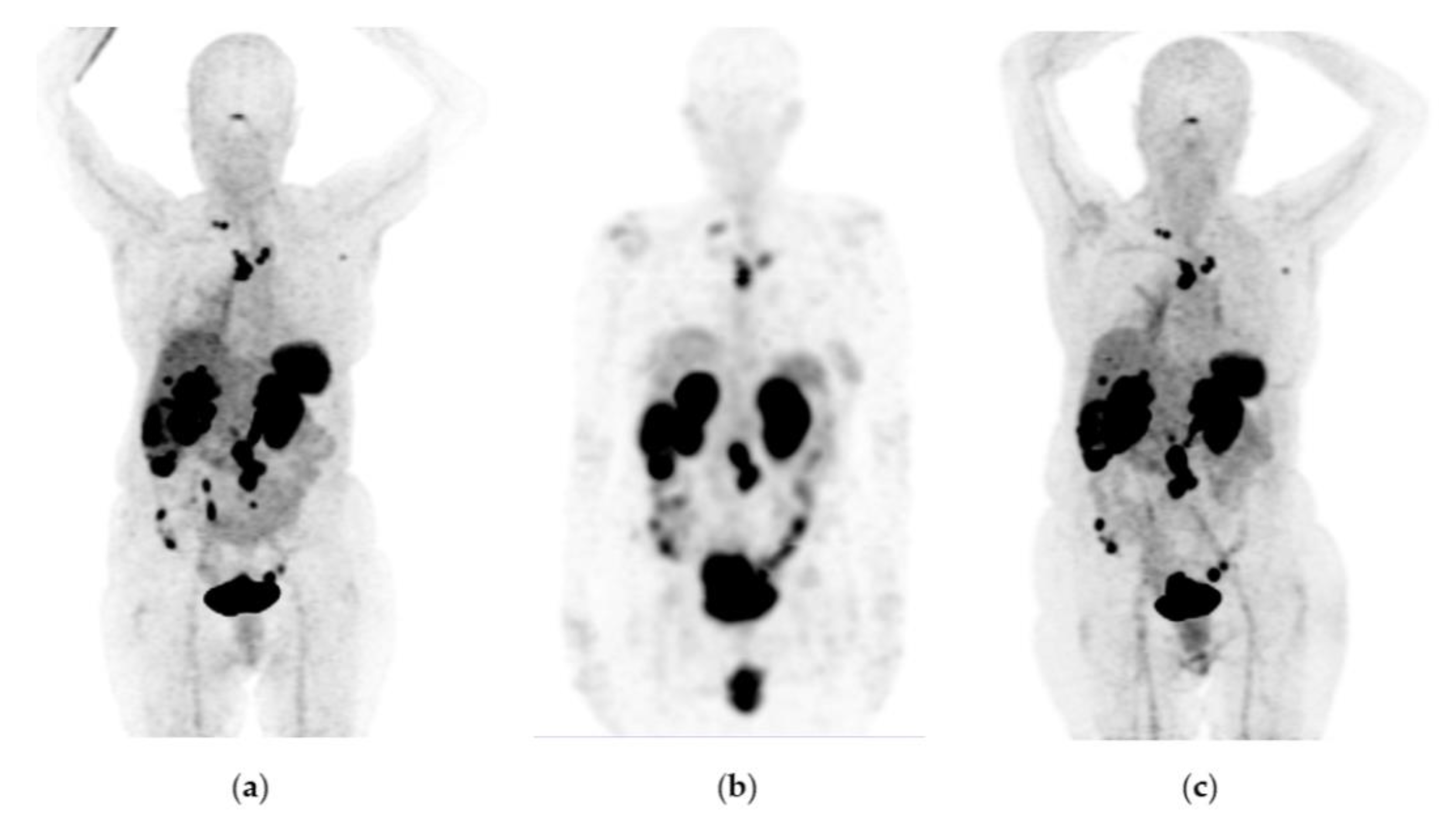
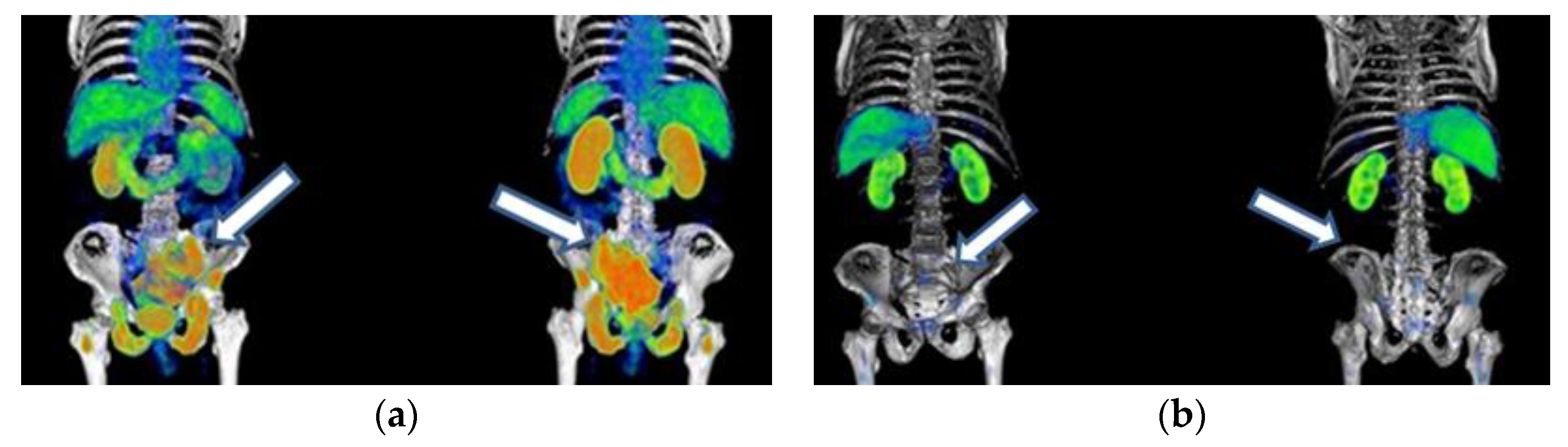
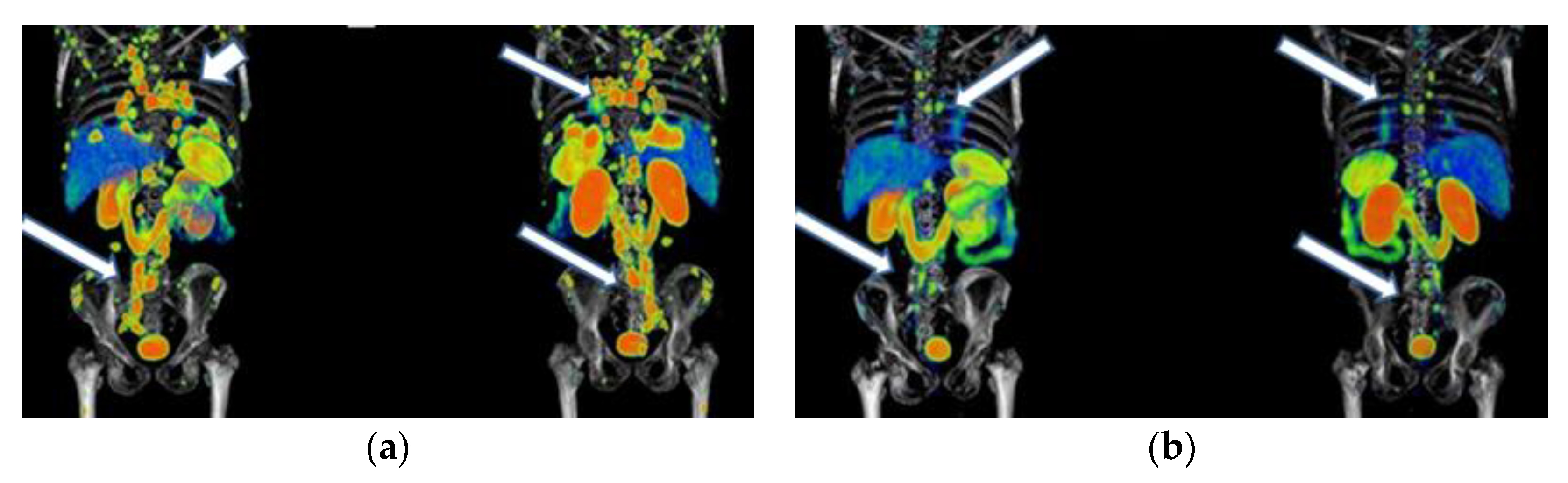
Figure 2 and
Figure 3 show typical clinical cases of complete response (disappearance of all lesions or adenopathies less than 10 mm short axis) and partial response (decrease of at least 30% in the sum of the largest diameters of lesions compared with the baseline study) after
177Lu-iPSMA therapy. In addition, the reduction of large tumors and multiple metastatic lesions are proof of the high specificity and molecular recognition of
177Lu iPSMA by PSMA at the tumor cell level (
Appendix A) (
Figure A1,
Figure A2 and
Figure A3).
In the group of patients who received one to two doses of 177Lu-iPSMA (7.4 GBq/dose) in the period from January 2016 to January 2020 (n = 26), a high percentage of censored cases was registered (69%; n = 18), and the rest of them (n = 8) died from progressive disease prior to further 177Lu-iPSMA radiotherapy (progressive disease: at least a 20% increase in the sum of tumor lesion diameters, using the smallest sum in the study as baseline).
Of the rest of the patients who have received from one to five doses between February 2020 and May 2023 (n = 67), 69 percent (n = 46) have not yet completed their treatment or remain alive with stable disease (free of progression); 13 percent (n = 9) were censored cases, and 18 percent (n = 12) died because of disease progression. However, 78% of this group of patients (n = 52) had a Karnofsky score between 90 and 70 after administering the second treatment dose. Furthermore, of patients with bone metastases (n = 109), 83% (n = 90) showed a significant decrease in pain (numerical scale from 10–7 to 3–1), which undoubtedly improved their quality of life.
In 40% of treated patients, adverse reactions were dry mouth, fatigue, and nausea, and less frequently (15% of patients), decreased appetite and constipation. These negative effects usually disappeared two months after administering the last dose of 177Lu-iPSMA. However, 19% of subjects treated with three to five doses developed permanent xerostomia. The decrease in hemoglobin, leukocytes, and platelets in 60% of the treated cases (myelosuppression grade 1 to 2) returned to baseline three months after concluding the treatment. Only three patients (6%) presented myelosuppression grade 3. There was no evidence of hepatotoxicity or nephrotoxicity.
3.2. 177Lu-DOTATOC
The results were classified according to the origin of the primary tumors [group 1: GEP-NT (n = 53), and group 2: other NTs (n = 28)] and the number of doses administered [group 3: GEP-NT three to four doses (n = 39); and group 4: GEP-NT five to six doses (n = 14)]. The other NET group received three to four doses (n = 28). The median follow up was 36 months (36 ± 16 months) for patients included at the January 2019 cut-off date (n = 81) in each study group.
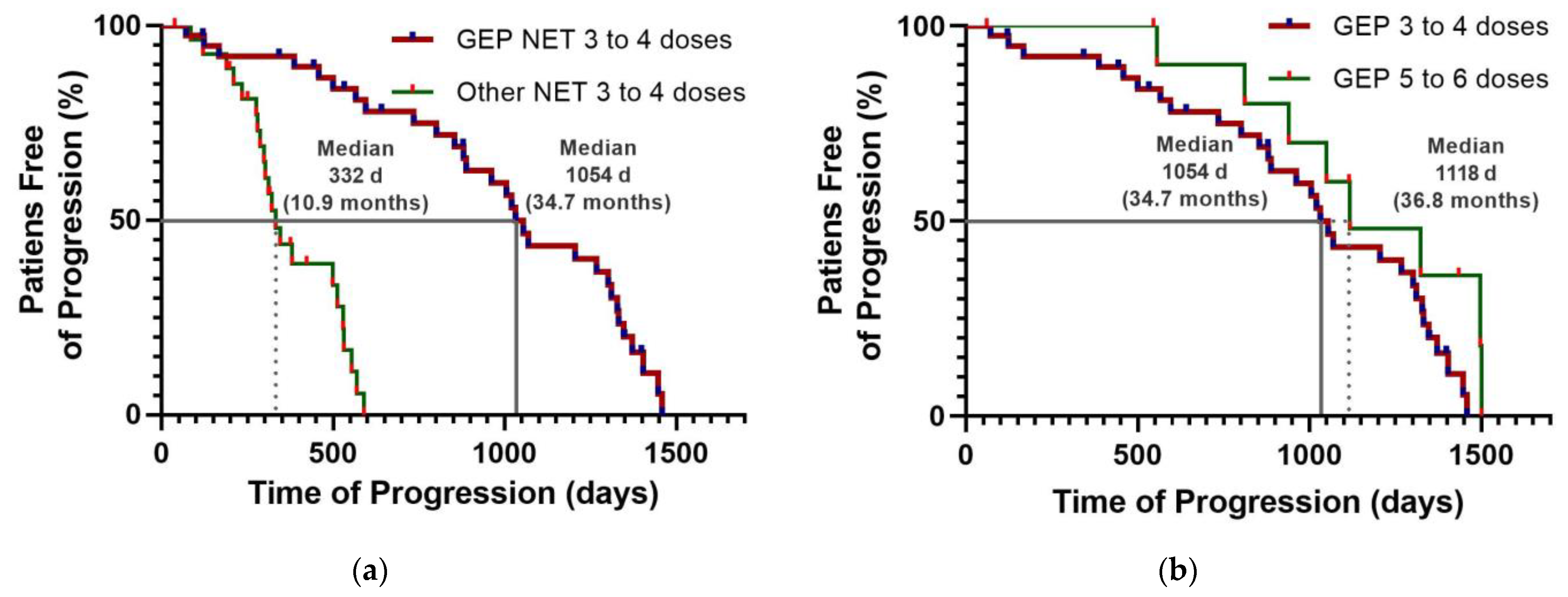
Fifty percent of patients with GEP-NET who received three to five doses of
177Lu-DOTATOC were free of progression at 1054 d (34.7 months) (
Table 3;
Figure 4a); while in the NET group (other NET different from GEP-NET), it was 332 days (10.9 months) (
Table 3;
Figure 4a). The hazard ratio was 0.1742 (95% CI: 0.05854–0.5182), indicating an 82.6% reduction in the risk of disease progression in favor of the GEP-NET group treated with
177Lu-DOTATOC (
Table 3). Fifty percent of patients in the GEP-NET group who received three to four doses of
177Lu-DOTATOC were free from progression at 34.7 months, compared to 36.8 months in the group who received five to six doses (
Figure 4b). However, the survival curves were not significantly different, with a hazard ratio of 0.5402 (95% CI: 0.275–1.062;
p = 0.2260, unstratified bilateral log-rank test) in favor of the GEP-NET group receiving five to six doses.
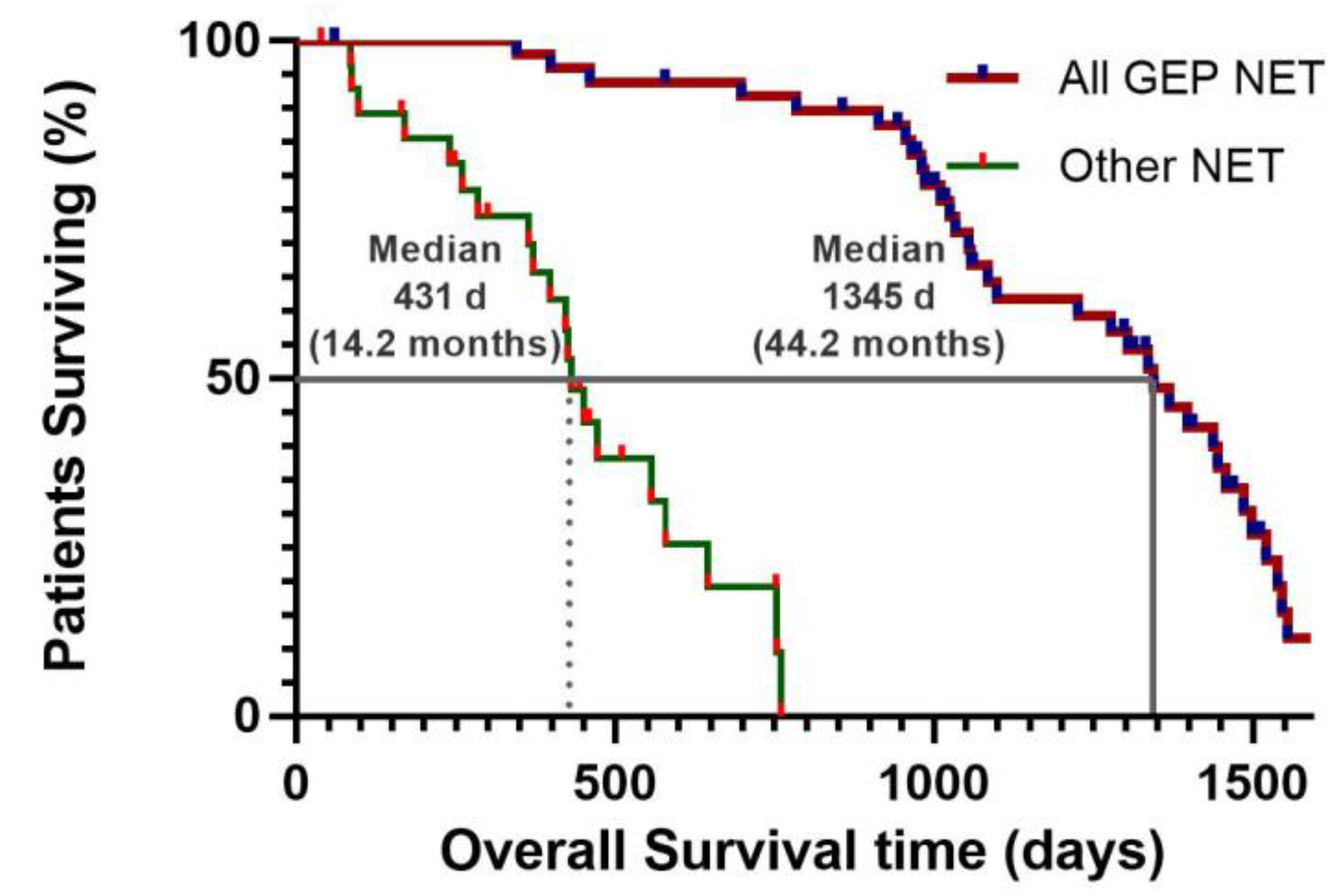
Follow up was 52 months at the time of the OS analysis, which was performed after the randomization of the last patient. Median OS was prolonged to a clinically relevant extent of 1345 day (44.2 months) in patients of the GEP-NET group compared with patients in the other-NET group with an OS of 431 days (14.2 months) (
Table 3) (
Figure 5). However, at the end of the study, the median overall survival of patients with GEP-NET treated with
177Lu-DOTATOC had not been reached, as three patients, two on the six-dose regimen and one on the four-dose regimen, were alive. Therefore, OS is >44.2 months (
Figure 5).
An overall response rate of 52% was observed in patients with GEP-NT treated with
177Lu-DOTATOC (
Table 3). As expected, most cases were partial responses (47%) and stable disease (45%), with a disease control rate of 97%. No patient had a complete or partial response in the group of patients with other NETs. However, they had a disease control rate of 71% (
Table 3).
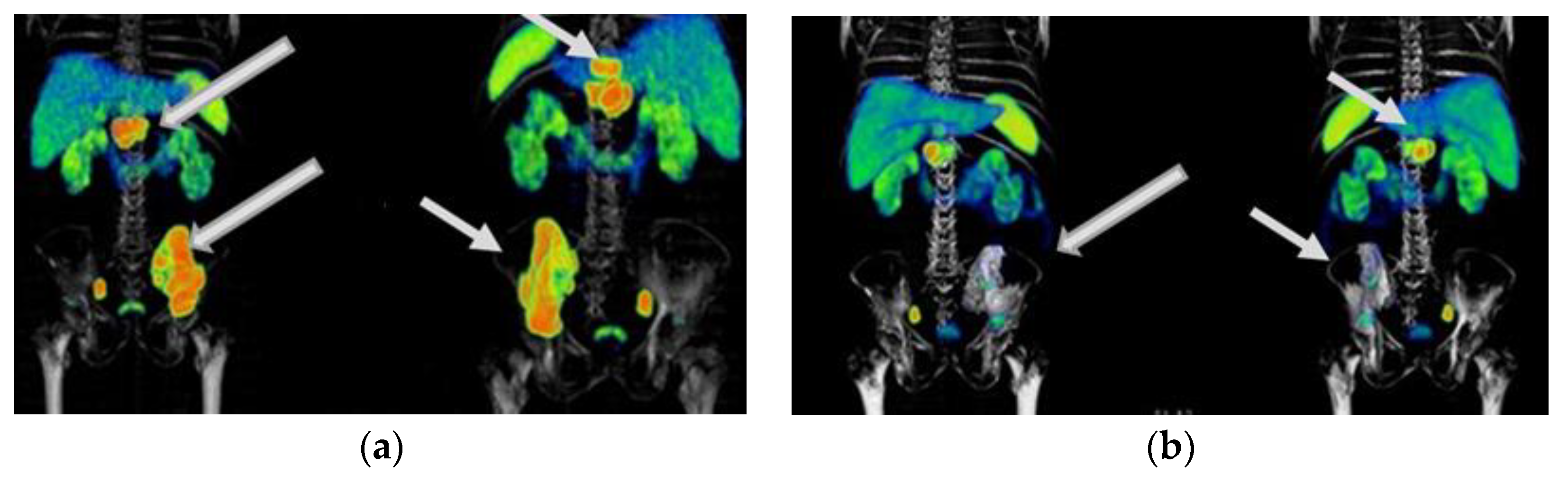
Figure 6,
Figure 7 and
Figure 8 show typical clinical cases of partial response and stable disease after
177Lu-DOTATOC therapy (the stable disease does not meet the criteria for partial response or progressive disease).
Of the rest of the patients who received from two to eight doses between February 2019 and May 2023 (n = 105), 58 percent (n = 61) have not yet completed their treatment or remain alive with stable disease; 22 percent (n = 23) were censored cases, and 20 percent (n = 21) died because of disease progression. However, 81% of patients had a Karnofsky score over 80 after administering the second treatment dose, significantly improving their quality of life.
In 48% of treated patients, adverse reactions were nausea and vomiting during perfusion of the radiopharmaceutical and co-administration of amino acids. Less frequently (19.5%), fatigue and decreased appetite were also presented. The decrease in hemoglobin, leukocytes, and platelets in 23.2% of the treated cases (myelosuppression grade 1 to 2) returned to baseline three months after concluding the treatment. Grade ≥ 3 of neutropenia, thrombocytopenia, or lymphopenia occurred in 4% (n = 7) of the total patients (n = 187) treated with 177Lu-DOTATOC. There was no evidence of hepatotoxicity or significant correlation between the assessment of renal function (biochemistry and dynamic nuclear imaging for renal function testing) and the use of therapeutic doses of 177Lu-DOTATOC that could indicate any moderate or severe nephrotoxicity.
4. Discussion
The clinical results of this translational study are consistent with the dozens of published clinical studies on the efficacy and toxicity of various
177Lu-labeled ligands for the treatment of advanced and progressive mCRPC and GEP-NET [
7,
8,
16,
17,
18].
It is important to note that, in line with the clinical results of these clinical trials, we have demonstrated that a maximum of three to five doses of 177Lu-iPSMA and three to four doses of 177Lu-DOTATOC are sufficient to achieve highly favorable response rates in terms of quality of life, with a low probability of serious side effects such as myelotoxicity (grade ≥ 3) or renal damage, which, far from being beneficial to patients, further compromise their critical health status.
177Lu-iPSMA therapy is a convenient option for the treatment of multiple metastases and large tumor lesions (
Appendix A) (
Figure A1,
Figure A2 and
Figure A3). For example, in the case shown in
Figure A1, the patient suffered from severe pain characteristic of the terminal stage of the disease. However, two weeks after administration of the first dose of
177Lu-iPSMA, the subject showed relevant pain relief. Furthermore, after administering four doses of
177Lu-iPSMA (four doses of 7.4 GBq), metastatic lesions in the hip and spine were significantly reduced, prolonging the patient’s life for 19 months after therapy. In this context and based on the results of this study,
177Lu-iPSMA therapy should be considered and evaluated in future clinical trials as a second-line rather than third- or fourth-line therapy in patients with mCRPC, with the potential to improve patient survival.
For more than a decade, peptide-targeted radionuclide therapies using lutetium-177 have experienced remarkable growth worldwide as they have demonstrated their ability to improve overall survival and quality of life in patients with advanced cancer. This fact has opened an important line of research for the development of new molecular sensors capable of delivering the radionuclide Lu-177 to tumor sites in a highly specific manner.
In prostate cancer and neuroendocrine tumors,
177Lu-PSMA-617 and
177Lu-DOTATATE are the radiopharmaceuticals with the most reported phase III clinical trials.
177Lu-iPSMA, whose clinical cases are reported in this research, is a new peptide ligand containing a pyridine ring and a hydrazine group that provides an additional anchoring site to target the PSMA enzyme and a molecular spatial configuration that favors its ability to remain in tumor lesions to produce ablative doses of radiation in a highly selective mode [
9,
10]. Therefore, this is the first report of a clinical trial of
177Lu-iPSMA in a significant number of patients with mCRPC. Our results showed an overall survival (OS) of 21.7 months. This finding is relevant and comparable to
177Lu-PSMA-617, for which an OS of 15.3 months is reported [
19,
20]. Of course, to determine whether there is a real difference between
177Lu-iPSMA and
177Lu-PSMA-617, a specific clinical trial would have to be performed under the same conditions and clinical parameters. Nevertheless, there is clearly a need for a greater number of new clinically proven ligands, such as iPSMA, which can be labeled with therapeutic radionuclides to treat these patients, given the 2020 data for prostate cancer, where 375,000 deaths and 1.4 million new cases were diagnosed in one year (the most diagnosed cancer in 112 countries) [
21].
On the other hand,
177Lu-DOTATOC is commonly prepared using commercially available radiochemical synthesizers connected to ISO Class 5 areas. However, the radiochemical yield using synthesizers ranges from 74 to 90% [
11]. Previously, we reported the use of multi-dose kit formulations to produce
177Lu-DOTATOC with radiochemical yields greater than 95% in a rapid process requiring only reconstitution of a lyophilized vial followed by incubation in a dry bath for 30 min [
11]. Therefore, this is the first time that clinical results in a significant number of patients have been reported for
177Lu-DOTATOC prepared from lyophilized formulations manufactured under GMP conditions. Considering that clinical reports for
177Lu-DOTATOC are scarce compared to
177Lu-DOTATATE (only one Phase II and no Phase III clinical trials have been reported for
177Lu-DOTATOC [
17]), the results reported in this research provide relevant clinical data for the consolidation of
177Lu-DOTATOC by demonstrating that it shows as high efficacy as
177Lu-DOTATATE in the treatment of patients with advanced neuroendocrine tumors. It is important to note that the clinical results of most clinical publications of
177Lu-DOTATOC and
177Lu-DOTATATE generally include patients with advanced and unresectable NET as inclusion and overall outcome characteristics. In this study, it was clearly demonstrated that in the GEP-NET population, the median progression-free survival was 34.7 months with an OS of >44.2 months, while the benefit in the other types of NET is only an OS of 14.2 months. This finding is consistent with the only reported phase II study of
177Lu-DOTATOC [
17] and provides a strong rationale for further phase III clinical trials specifically targeting GEP-NETs.
Finally, the retrospective nature of the control group study for 177Lu-iPSMA and the still limited sample size in both the 177Lu-iPSMA and 177Lu-DOTATOC trials are the main limitations of the present study. Nonetheless, the results obtained are promising and warrant further prospective phase III trials of PRRT in patients with mCRPC and NET to confirm or refute our findings.
Severe pain, which increases with disease progression, affects approximately 64% of patients with mCRPC or NET tumors. This condition has a direct impact on survival and quality of life in ways that are dependent on proper pain management. The challenge is to find a balance between pain control and analgesia so that the patient remains independent enough to perform daily activities [
22].
In current clinical practice, adequate pain control is achieved when the focus of palliative treatment is on targeted radiation therapy [
23]. It is important to note that cancer pain is thought to result from local inflammation due to mechanical compression of nerve terminals and tumor surrounding tissues [
24]. However, recent evidence suggests that the main mechanisms of cancer pain are the loss of homeostasis, anatomical remodeling, and neurochemical changes that occur between tumor, neuronal, immune, and stromal cells [
24]. These dynamic intercellular changes include the secretion of prostaglandins, interleukins, and growth factors that promote acidification of the environment, which remodels the relationship between osteoclasts and osteoblasts and alters the ion channel [
25]. In addition, the density of neuropathic and nociceptive receptors triggers neurochemical changes such as sensitization, with the consequent opening and closing of ion channels, altering the endogenous electrochemical potential of nerve fibers innervating bone [
25,
26]. Lutetium-177 radiopharmaceuticals are a fast and effective palliative treatment option. Unlike chemotherapy, they do not cause neuropathic pain as an adverse effect [
27]. As shown in this translational clinical trial,
177Lu-iPSMA and
177Lu-DOTATOC significantly reduce cancer pain. Thus, modern radiobiology suggests that the mechanism that drives pain relief is the reduction on ionic flux through the functional expression of voltage-gated ion channels, generating a radiation-induced nerve rearrangement [
28].


 ,
, 













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}