
Development of Atomoxetine-Loaded NLC In Situ Gel for Nose-to-Brain Delivery: Optimization, In Vitro, and Preclinical Evaluation
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Materials
2.2. Methods
2.2.1. Screening of Liquid Lipids
2.2.2. Screening of Solid Lipids
2.2.3. Screening of Surfactant
2.2.4. Miscibility Study
3. Experimental Design
3.1. Formulation of AXT-NLC
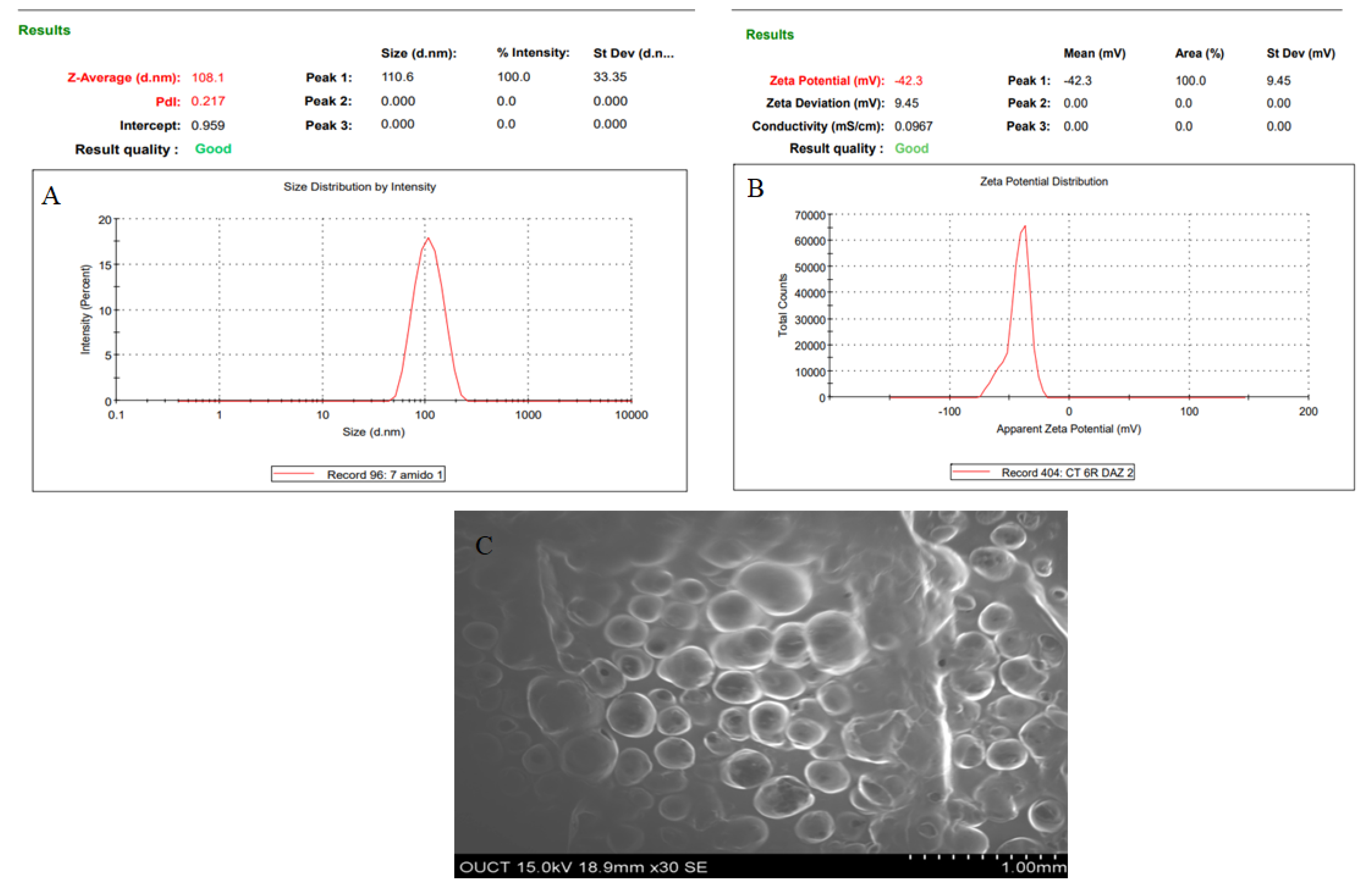
3.2. NLC Characterization
3.3. Entrapment Efficiency
3.4. Differential Scanning Calorimetry (DSC)
3.5. Fourier Transform Infrared Spectroscopy (FTIR) Analysis
3.6. Formulation of AXT-NLC In Situ Gel
3.7. Evaluation of AXT-NLC In Situ Gel
3.7.1. pH Analysis
3.7.2. Viscosity
3.7.3. Drug Content
3.7.4. Gelling Temperature
3.7.5. In Vitro Drug Release
3.7.6. Ex Vivo Permeation Study
3.8. In Vivo Studies
3.8.1. Animal
3.8.2. Pharmacokinetic Study
3.8.3. Collection of Blood Samples and AXT Extraction
3.8.4. Analysis of Extracted Plasma or Brain Samples by HPLC Technique
3.9. Pharmacokinetic and Neuropharmacokinetic Parameters Calculation
3.10. Pharmacodynamics Study
3.10.1. Study Design for Vascular Dementia
3.10.2. Morris Water Maze (MWM) Test
3.10.3. Statistical Analysis
4. Results and Discussion
4.1. Screening of Solid and Liquid Lipids
4.2. Miscibility Study
4.3. Optimization
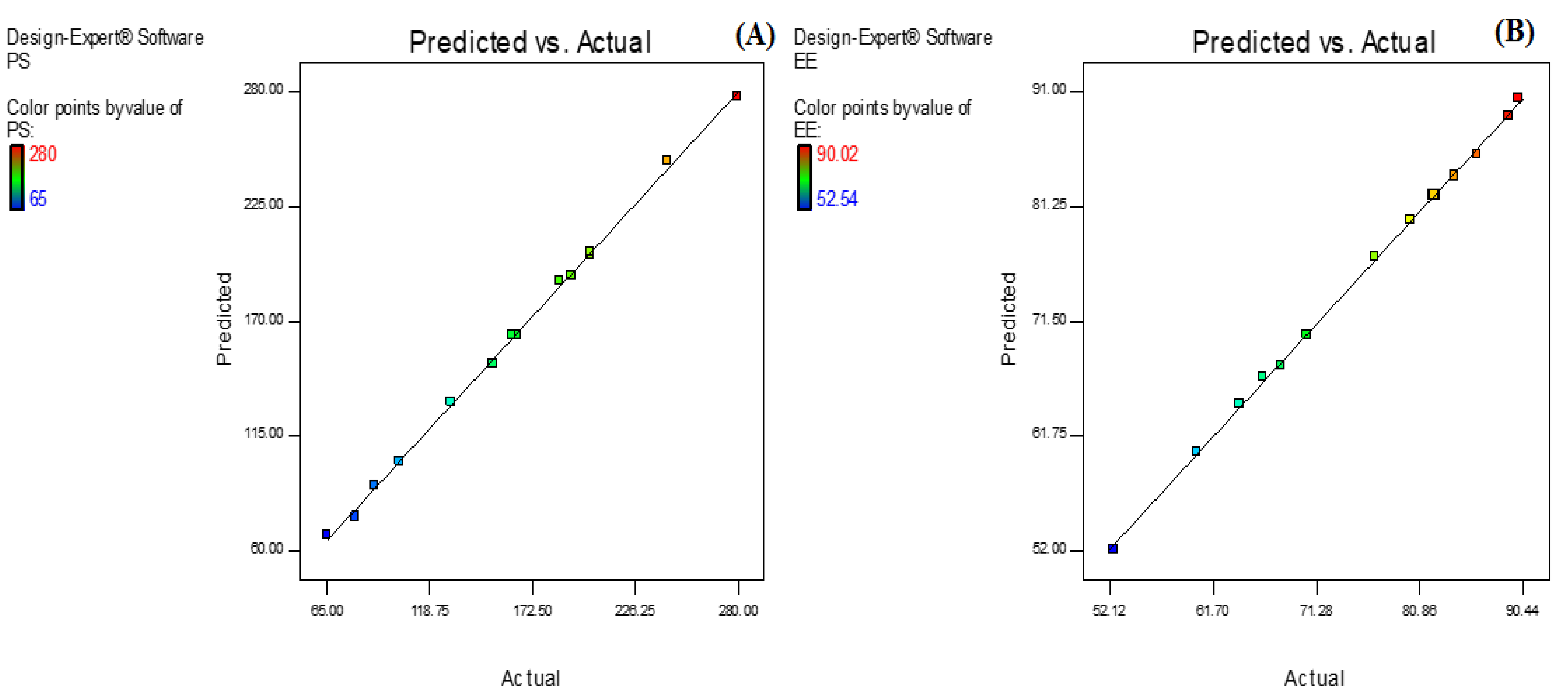
4.4. Effect of Olive Oil, Stearic Acid, and Sonication Time over the PS of NLC
4.5. Effect of Olive Oil, Stearic Acid, and Sonication Time over the EE of AXT in AXT-NLC
4.6. Selection of Optimized AXT-NLC
4.7. FTIR Analysis
4.8. DSC Analysis
4.9. Development of AXT-NLC In Situ Gel
4.10. Evaluation of AXT-NLC In Situ Gel
4.10.1. pH, Viscosity, and Drug Content
4.10.2. Gelling Temperature
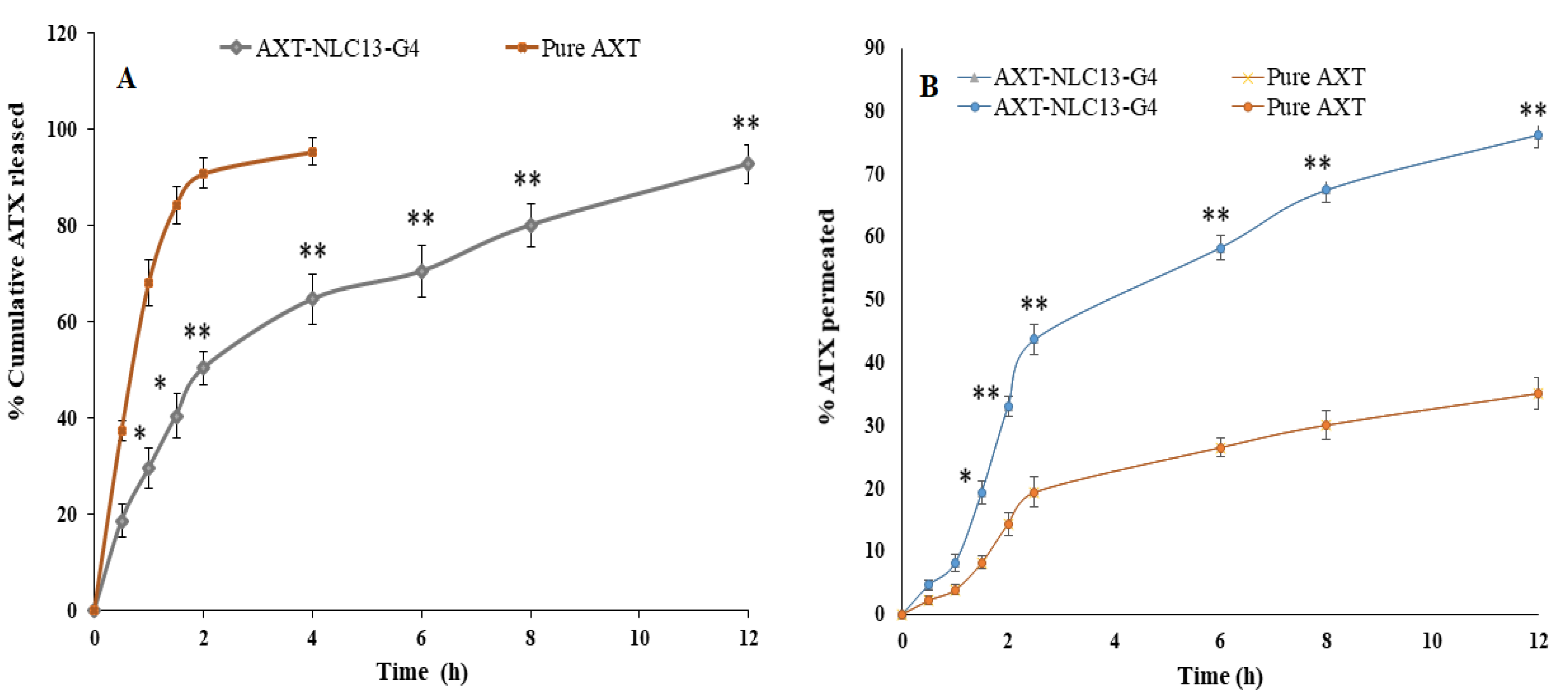
4.10.3. In Vitro Drug Release
4.10.4. Ex Vivo Permeation Study
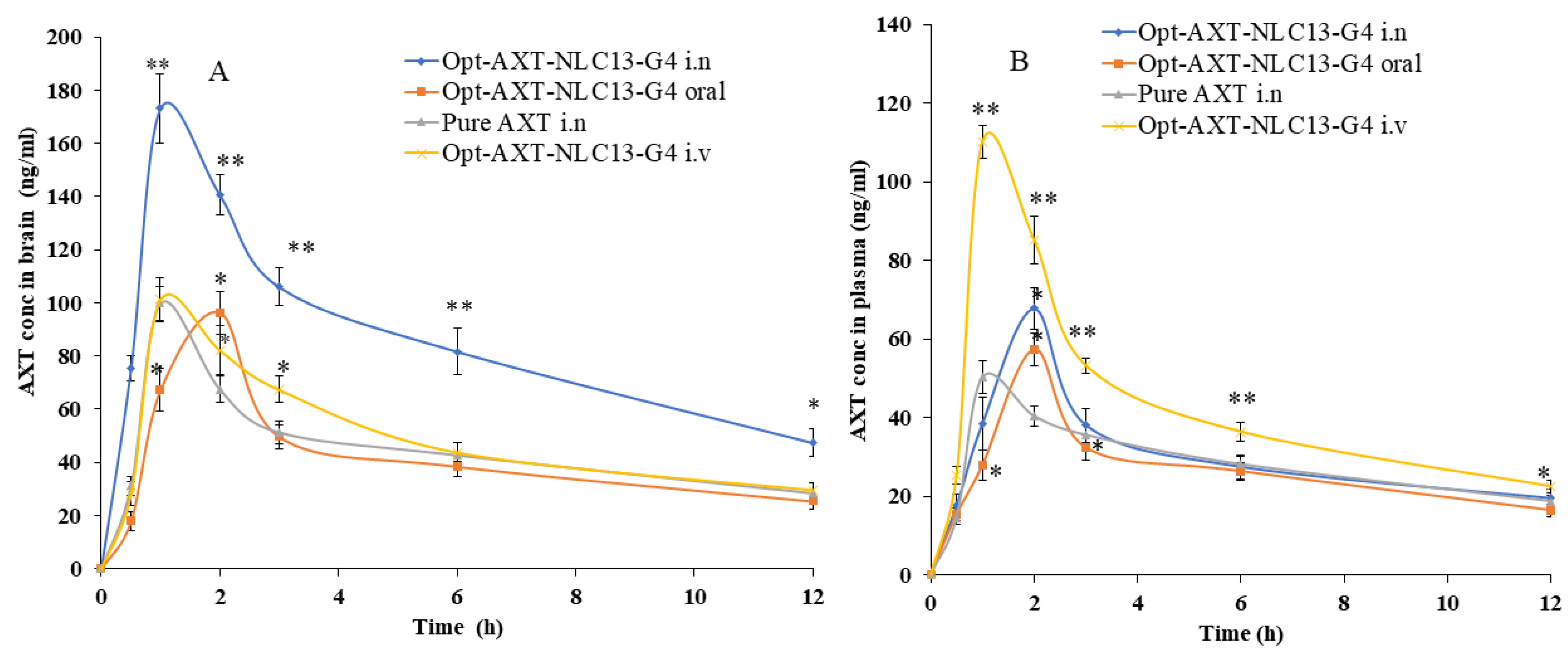
4.10.5. Pharmacokinetic and Neuro-Pharmacokinetic Study
4.10.6. Morris Water Maze Test
5. Conclusions
6. Limitation of the Study
- The main challenge is the retention of the formulation in the nasal cavity due to nasal clearance and ciliary movement. These are the first barriers to overcome when drugs are administered via the intranasal route since these issues can be overcome to a certain extent by using a nanogel drug delivery system [21].
- The anatomical location of the olfactory epithelium is another main limitation of this route since the dosage form must first be able to reach this site [21].
- Metabolic enzymes present in the olfactory mucosa must also be considered when designing a formulation for the nose-to-brain route. Consequently, intranasal formulations must be composed of biocompatible and odorless excipients to avoid rapid elimination due to mucociliary clearance and/or enzymatic degradation.
- Regarding nanogels, the slow responsiveness of stimuli-sensitive hydrogels, burst release during the initial swelling phase, and uncontrollable porosity are some limitations of hydrogel drug delivery [64].
- Many times, preclinical studies are not correlated with clinical studies due to differences in nasal anatomy between animal species and humans. To tackle these challenges, advanced mathematical models should be designed and used [21].
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Profyri, E.; Leung, P.; Huntley, J.; Orgeta, V. Effectiveness of treatments for people living with severe dementia: A systematic review and meta-analysis of randomised controlled clinical trials. Ageing Res. Rev. 2022, 82, 101758. [Google Scholar] [CrossRef]
- Marhánková, J.H. The role of dementia and Alzheimer’s disease in older adults’ representations of aging and anxieties regarding one’s own future. J. Aging Stud. 2023, 65, 101127. [Google Scholar] [CrossRef] [PubMed]
- Prajjwal, P.; Marsool, M.D.M.; Inban, P.; Sharma, B.; Asharaf, S.; Aleti, S.; Gadam, S.; Al Sakini, A.S.; Hadi, D.D. Vascular dementia subtypes, pathophysiology, genetics, neuroimaging, biomarkers, and treatment updates along with its association with Alzheimer’s dementia and diabetes mellitus. Dis. Mon. 2023, 69, 101557. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, Z.; Liu, J.; Guo, M.; Li, H. Panax Ginseng in the treatment of Alzheimer’s disease and vascular dementia. J. Ginseng Res. 2023, 47, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Khoodoruth, M.A.S.; Ouanes, S.; Khan, Y.S. A systematic review of the use of atomoxetine for management of comorbid anxiety disorders in children and adolescents with attention-deficit hyperactivity disorder. Res. Dev. Disabil. 2022, 128, 104275. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhang, Y.; Khan, A.R.; He, S.; Wang, Y.; Xu, J.; Zhai, G. Quantitative prediction of the bitterness of atomoxetine hydrochloride and taste-masked using hydroxypropyl-β-cyclodextrin: A biosensor evaluation and interaction study. Asian J. Pharm. Sci. 2020, 15, 492–505. [Google Scholar] [CrossRef] [PubMed]
- Teaima, M.H.; El-Nadi, M.T.; Hamed, R.R.; El-Nabarawi, M.A.; Abdelmonem, R. Lyophilized Nasal Inserts of Atomoxetine HCl Solid Lipid Nanoparticles for Brain Targeting as a Treatment of Attention-Deficit/Hyperactivity Disorder (ADHD): A Pharmacokinetics Study on Rats. Pharmaceuticals 2023, 16, 326. [Google Scholar] [CrossRef]
- Vaidya, A.V.; Shinde, U.A.; Shimpi, H.H. Preliminary studies on brain targeting of intranasal atomoxetine liposomes. Int. J. Pharm. Pharm. Sci. 2016, 8, 286–292. [Google Scholar]
- Lakshmi, P.; Harini, K. Design and Optimization of Thermo-reversible Nasal in situ Gel of Atomoxetine Hydrochloride Using Taguchi Orthogonal Array Design. Dhaka Univ. J. Pharm. Sci. 2019, 18, 183–193. [Google Scholar] [CrossRef] [Green Version]
- Selvaraj, K.; Gowthamarajan, K.; Karri, V.V.S.R. Nose to brain transport pathways an overview: Potential of nanostructured lipid carriers in nose to brain targeting. Artif. Cells Nanomed. Biotechnol. 2018, 46, 2088–2095. [Google Scholar] [CrossRef]
- Yasir, M.; Chauhan, I.; Zafar, A.; Verma, M.; Noorulla, K.M.; Tura, A.J.; Alruwaili, N.K.; Haji, M.J.; Puri, D.; Gobena, W.G.; et al. Buspirone loaded solid lipid nanoparticles for amplification of nose to brain efficacy: Formulation development, optimization by Box-Behnken design, in-vitro characterization and in-vivo biological evaluation. J. Drug Deliv. Sci. Technol. 2020, 61, 102164. [Google Scholar] [CrossRef]
- Chatzitaki, A.T.; Jesus, S.; Karavasili, C.; Andreadis, D.; Fatouros, D.G.; Borges, O. Chitosan-coated PLGA nanoparticles for the nasal delivery of ropinirole hydrochloride: In vitro and ex vivo evaluation of efficacy and safety. Int. J. Pharm. 2020, 589, 119776. [Google Scholar] [CrossRef]
- Costa, C.P.; Moreira, J.N.; Sousa Lobo, J.M.; Silva, A.C. Intranasal delivery of nanostructured lipid carriers, solid lipid nanoparticles and nanoemulsions: A current overview of in vivo studies. Acta Pharm. Sin. B 2021, 11, 925–940. [Google Scholar] [CrossRef]
- Kaur, I.P.; Bhandari, R.; Bhandari, S.; Kakkar, V. Potential of solid lipid nanoparticles in brain targeting. J. Control. Release 2008, 127, 97–109. [Google Scholar] [CrossRef]
- Patel, H.P.; Gandhi, P.A.; Chaudhari, P.S.; Desai, B.V.; Desai, D.T.; Dedhiya, P.P.; Maulvi, F.A.; Vyas, B.A. Clozapine loaded nanostructured lipid carriers engineered for brain targeting via nose-to-brain delivery: Optimization and in vivo pharmacokinetic studies. J. Drug Deliv. Sci. Technol. 2021, 64, 102533. [Google Scholar] [CrossRef]
- Correia, A.C.; Monteiro, A.R.; Silva, R.; Moreira, J.N.; Sousa Lobo, J.M.; Silva, A.C. Lipid nanoparticles strategies to modify pharmacokinetics of central nervous system targeting drugs: Crossing or circumventing the blood–brain barrier (BBB) to manage neurological disorders. Adv. Drug Deliv. Rev. 2022, 189, 114485. [Google Scholar] [CrossRef] [PubMed]
- Yasir, M.; Sara, U.V.S.; Chauhan, I.; Gaur, P.K.; Singh, A.P.; Puri, D.; Ameeduzzafar, A. Solid lipid nanoparticles for nose to brain delivery of donepezil: Formulation, optimization by Box–Behnken design, in vitro and in vivo evaluation. Artif. Cells Nanomed. Biotechnol. 2018, 46, 1838–1851. [Google Scholar] [CrossRef] [Green Version]
- Chauhan, I.; Yasir, M.; Verma, M.; Singh, A.P. Nanostructured lipid carriers: A groundbreaking approach for transdermal drug delivery. Adv. Pharm. Bull. 2020, 10, 150–165. [Google Scholar] [CrossRef]
- Masjedi, M.; Azadi, A.; Heidari, R.; Mohammadi-Samani, S. Nose-to-brain delivery of sumatriptan-loaded nanostructured lipid carriers: Preparation, optimization, characterization and pharmacokinetic evaluation. J. Pharm. Pharmacol. 2020, 72, 1341–1351. [Google Scholar] [CrossRef]
- Thakkar, H.; Vaghela, D.; Patel, B.P. Brain targeted intranasal in-situ gelling spray of paroxetine: Formulation, characterization and in-vivo evaluation. J. Drug Deliv. Sci. Technol. 2021, 62, 102317. [Google Scholar] [CrossRef]
- Formica, M.L.; Real, D.A.; Picchio, M.L.; Catlin, E.; Donnelly, R.F.; Paredes, A.J. On a highway to the brain: A review on nose-to-brain drug delivery using nanoparticles. Appl. Mater. Today 2022, 29, 101631. [Google Scholar] [CrossRef]
- Corazza, E.; di Cagno, M.P.; Bauer-Brandl, A.; Abruzzo, A.; Cerchiara, T.; Bigucci, F.; Luppi, B. Drug delivery to the brain: In situ gelling formulation enhances carbamazepine diffusion through nasal mucosa models with mucin. Eur. J. Pharm. Sci. 2022, 179, 106294. [Google Scholar] [CrossRef] [PubMed]
- Rajput, A.P.; Butani, S.B. Resveratrol anchored nanostructured lipid carrier loaded in situ gel via nasal route: Formulation, optimization and in vivo characterization. J. Drug Deliv. Sci. Technol. 2019, 51, 214–223. [Google Scholar] [CrossRef]
- Fahmy, U.A.; Ahmed, O.A.A.; Badr-Eldin, S.M.; Aldawsari, H.M.; Okbazghi, S.Z.; Awan, Z.A.; Bakhrebah, M.A.; Alomary, M.N.; Abdulaal, W.H.; Medina, C.; et al. Optimized nanostructured lipid carriers integrated into in situ nasal gel for enhancing brain delivery of flibanserin. Int. J. Nanomed. 2020, 15, 5253–5264. [Google Scholar] [CrossRef] [PubMed]
- Gabal, Y.M.; Kamel, A.O.; Sammour, O.A.; Elshafeey, A.H. Effect of surface charge on the brain delivery of nanostructured lipid carriers in situ gels via the nasal route. Int. J. Pharm. 2014, 473, 442–457. [Google Scholar] [CrossRef]
- Rajput, A.P.; Butani, S.B. Fabrication of an ion-sensitive in situ gel loaded with nanostructured lipid carrier for nose to brain delivery of Donepezil. Asian J. Pharm. 2018, 12, 293–302. [Google Scholar]
- Kapoor, H.; Aqil, M.; Imam, S.S.; Sultana, Y.; Ali, A. Formulation of amlodipine nano lipid carrier: Formulation design, physicochemical and transdermal absorption investigation. J. Drug Deliv. Sci. Technol. 2019, 49, 209–218. [Google Scholar] [CrossRef]
- Agrawal, M.; Saraf, S.; Pradhan, M.; Patel, R.J.; Singhvi, G.; Ajazuddin; Alexander, A. Design and optimization of curcumin loaded nano lipid carrier system using Box-Behnken design. Biomed. Pharmacother. 2021, 141, 111919. [Google Scholar] [CrossRef]
- Anand, A.; Arya, M.; Kaithwas, G.; Singh, G.; Saraf, S.A. Sucrose stearate as a biosurfactant for development of rivastigmine containing nanostructured lipid carriers and assessment of its activity against dementia in C. elegans model. J. Drug Deliv. Sci. Technol. 2019, 49, 219–226. [Google Scholar] [CrossRef]
- Shelke, S.; Shahi, S.; Jalalpure, S.; Dhamecha, D.; Shengule, S. Formulation and evaluation of thermoreversible mucoadhesive in-situ gel for intranasal delivery of naratriptan hydrochloride. J. Drug Deliv. Sci. Technol. 2015, 29, 238–244. [Google Scholar] [CrossRef]
- Altuntaş, E.; Yener, G. Formulation and Evaluation of Thermoreversible In Situ Nasal Gels Containing Mometasone Furoate for Allergic Rhinitis. AAPS PharmSciTech 2017, 18, 2673–2682. [Google Scholar] [CrossRef]
- Aderibigbe, B.A. In situ-based gels for nose to brain delivery for the treatment of neurological diseases. Pharmaceutics 2018, 10, 40. [Google Scholar] [CrossRef] [Green Version]
- Guo, W.; Li, W.; Guo, G.; Zhang, J.; Zhou, B.; Zhai, Y.; Wang, C. Determination of atomoxetine in human plasma by a high performance liquid chromatographic method with ultraviolet detection using liquid-liquid extraction. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2007, 854, 128–134. [Google Scholar] [CrossRef]
- Nair, A.; Jacob, S. A simple practice guide for dose conversion between animals and human. J. Basic Clin. Pharm. 2016, 7, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacob, S.; Nair, A.B.; Morsy, M.A. Dose Conversion Between Animals and Humans: A Practical Solution. Indian J. Pharm. Educ. Res. 2022, 56, 600–607. [Google Scholar] [CrossRef]
- Teichert, J.; Rowe, J.B.; Ersche, K.D.; Skandali, N.; Sacher, J.; Aigner, A.; Regenthal, R. Determination of atomoxetine or escitalopram in human plasma by HPLC: Applications in neuroscience research studies. Int. J. Clin. Pharmacol. Ther. 2020, 58, 426–438. [Google Scholar] [CrossRef]
- Zafar, A.; Awad Alsaidan, O.; Alruwaili, N.K.; Sarim Imam, S.; Yasir, M.; Saad Alharbi, K.; Singh, L.; Muqtader Ahmed, M. Formulation of intranasal surface engineered nanostructured lipid carriers of rotigotine: Full factorial design optimization, in vitro characterization, and pharmacokinetic evaluation. Int. J. Pharm. 2022, 627, 122232. [Google Scholar] [CrossRef] [PubMed]
- Abdelbary, G.A.; Tadros, M.I. Brain targeting of olanzapine via intranasal delivery of core-shell difunctional block copolymer mixed nanomicellar carriers: In vitro characterization, ex vivo estimation of nasal toxicity and in vivo biodistribution studies. Int. J. Pharm. 2013, 452, 300–310. [Google Scholar] [CrossRef]
- Alzoubi, K.H. Edaravone protects from memory impairment induced by chronic L-methionine administration. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2020, 393, 1221–1228. [Google Scholar] [CrossRef] [PubMed]
- Bromley-Brits, K.; Deng, Y.; Song, W. Morris Water Maze test for learning and memory deficits in Alzheimer’s disease model mice. J. Vis. Exp. 2011, 20, e2920. [Google Scholar] [CrossRef] [PubMed]
- Khodir, S.A.; Faried, M.A.; Abd-Elhafiz, H.I.; Sweed, E.M. Sitagliptin Attenuates the Cognitive Deficits in L-Methionine-Induced Vascular Dementia in Rats. Biomed Res. Int. 2022, 2022, 7222590. [Google Scholar] [CrossRef]
- Sachdeva, A.K.; Misra, S.; Pal Kaur, I.; Chopra, K. Neuroprotective potential of sesamol and its loaded solid lipid nanoparticles in ICV-STZ-induced cognitive deficits: Behavioral and biochemical evidence. Eur. J. Pharmacol. 2015, 747, 132–140. [Google Scholar] [CrossRef]
- Varshosaz, J.; Tabbakhian, M.; Mohammadi, M.Y. Formulation and optimization of solid lipid nanoparticles of buspirone HCl for enhancement of its oral bioavailability. J. Liposome Res. 2010, 20, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Jain, K.; Sood, S.; Gowthamarajan, K. Optimization of artemether-loaded NLC for intranasal delivery using central composite design. Drug Deliv. 2015, 22, 940–954. [Google Scholar] [CrossRef] [Green Version]
- Das, S.; Ng, W.K.; Tan, R.B.H. Are nanostructured lipid carriers (NLCs) better than solid lipid nanoparticles (SLNs): Development, characterizations and comparative evaluations of clotrimazole-loaded SLNs and NLCs? Eur. J. Pharm. Sci. 2012, 47, 139–151. [Google Scholar] [CrossRef]
- Gilani, S.J.; Bin-Jumah, M.; Rizwanullah, M.; Imam, S.S.; Imtiyaz, K.; Alshehri, S.; Rizvi, M.M.A. Chitosan coated luteolin nanostructured lipid carriers: Optimization, in vitro-ex vivo assessments and cytotoxicity study in breast cancer cells. Coatings 2021, 11, 158. [Google Scholar] [CrossRef]
- Brito Raj, S.; Chandrasekhar, K.B.; Reddy, K.B. Formulation, in-vitro and in-vivo pharmacokinetic evaluation of simvastatin nanostructured lipid carrier loaded transdermal drug delivery system. Futur. J. Pharm. Sci. 2019, 5, 9. [Google Scholar] [CrossRef] [Green Version]
- Pezeshki, A.; Ghanbarzadeh, B.; Mohammadi, M.; Fathollahi, I.; Hamishehkar, H. Encapsulation of vitamin A palmitate in nanostructured lipid carrier (NLC)-effect of surfactant concentration on the formulation properties. Adv. Pharm. Bull. 2014, 4, 563–568. [Google Scholar] [CrossRef]
- Pinheiro, M.; Ribeiro, R.; Vieira, A.; Andrade, F.; Reis, S. Design of a nanostructured lipid carrier intended to improve the treatment of tuberculosis. Drug Des. Devel. Ther. 2016, 10, 2467–2475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kesharwani, D.; Das, S.; Paliwal, R.; Satapathy, T. Journal of Radiation Research and Applied Sciences Development, QbD based optimization and in vitro characterization of Diacerein loaded nanostructured lipid carriers for topical applications. J. Radiat. Res. Appl. Sci. 2023, 16, 100565. [Google Scholar] [CrossRef]
- Pokharkar, V.; Patil-gadhe, A.; Palla, P. ScienceDirect Efavirenz loaded nanostructured lipid carrier engineered for brain targeting through intranasal route: In-vivo pharmacokinetic and toxicity study. Biomed. Pharmacother. 2017, 94, 150–164. [Google Scholar] [CrossRef]
- Wavikar, P.R.; Vavia, P.R. Rivastigmine-loaded in situ gelling nanostructured lipid carriers for nose to brain delivery. J. Liposome Res. 2014, 25, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Balakrishnan, P.; Park, E.K.; Song, C.K.; Ko, H.J.; Hahn, T.W.; Song, K.W.; Cho, H.J. Carbopol-Incorporated thermoreversible gel for intranasal drug delivery. Molecules 2015, 20, 4124–4135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravi, P.R.; Aditya, N.; Patil, S.; Cherian, L. Nasal in-situ gels for delivery of rasagiline mesylate: Improvement in bioavailability and brain localization. Drug Deliv. 2015, 22, 903–910. [Google Scholar] [CrossRef]
- Nair, A.B.; Chaudhary, S.; Shah, H.; Jacob, S.; Mewada, V.; Shinu, P.; Shah, J. Intranasal Delivery of Darunavir-Loaded Mucoadhesive In Situ Gel: Experimental Design, In Vitro Evaluation, and Pharmacokinetic Studies. Gels 2022, 8, 342. [Google Scholar] [CrossRef]
- Cunha, S.; Swedrowska, M.; Bellahnid, Y.; Xu, Z.; Sousa Lobo, J.M.; Forbes, B.; Silva, A.C. Thermosensitive in situ hydrogels of rivastigmine-loaded lipid-based nanosystems for nose-to-brain delivery: Characterisation, biocompatibility, and drug deposition studies. Int. J. Pharm. 2022, 620, 121720. [Google Scholar] [CrossRef] [PubMed]
- Youssef, A.; Dudhipala, N.; Majumdar, S. Ciprofloxacin Loaded Nanostructured Lipid Carriers Incorporated into In-Situ Gels to Improve Management of Bacterial Endophthalmitis. Pharmaceutics 2020, 12, 572. [Google Scholar] [CrossRef]
- Chin, L.Y.; Tan, J.Y.P.; Choudhury, H.; Pandey, M.; Sisinthy, S.P.; Gorain, B. Development and optimization of chitosan coated nanoemulgel of telmisartan for intranasal delivery: A comparative study. J. Drug Deliv. Sci. Technol. 2021, 62, 102341. [Google Scholar] [CrossRef]
- Yasir, M.; Vir Singh Sara, U.; Som, I.; Gaur, P.; Singh, M.; Ameeduzzafar. Nose to Brain Drug Delivery: A Novel Approach Through Solid Lipid Nanoparticles. Curr. Nanomed. 2016, 6, 105–132. [Google Scholar] [CrossRef]
- Wavikar, P.; Pai, R.; Vavia, P. Nose to Brain Delivery of Rivastigmine by In Situ Gelling Cationic Nanostructured Lipid Carriers: Enhanced Brain Distribution and Pharmacodynamics. J. Pharm. Sci. 2017, 106, 3613–3622. [Google Scholar] [CrossRef]
- Ahmadi, N.; Hosseini, M.J.; Rostamizadeh, K.; Anoush, M. Investigation of therapeutic effect of curcumin α and β glucoside anomers against Alzheimer’s disease by the nose to brain drug delivery. Brain Res. 2021, 1766, 147517. [Google Scholar] [CrossRef] [PubMed]
- Bourganis, V.; Kammona, O.; Alexopoulos, A.; Kiparissides, C. Recent Advances in Carrier Mediated Nose-to-Brain Delivery of Pharmaceutics. Eur. J. Pharm. Biopharm. 2018, 128, 337–362. [Google Scholar] [CrossRef]
- Cunha, S.; Amaral, M.H.; Sousa Lobo, J.M.; Silva, A.C. Lipid nanoparticles for nasal/intranasal drug delivery. Crit. Rev. Ther. Drug Carr. Syst. 2017, 34, 257–282. [Google Scholar] [CrossRef] [PubMed]
- Journal, A.I.; Sharma, A.; Garg, T.; Aman, A.; Panchal, K.; Sharma, R.; Kumar, S.; Markandeywar, T.; Sharma, A.; Garg, T.; et al. Nanogel—An advanced drug delivery tool: Current and future Nanogel—An advanced drug delivery tool: Current and future. Artif. Cells Nanomed. Biotechnol. 2016, 44, 165–177. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation Code | Total Lipid (%) | Surfactant (%) | Sonication Time (min) | Particle Size (nm) | Entrapment Efficiency (%) |
|---|---|---|---|---|---|
| AXT-NLC 1 | 5.5 | 3.5 | 9 | 187.0 | 76.71 |
| AXT-NLC 2 | 1.5 | 4.5 | 6 | 65.0 | 66.31 |
| AXT-NLC 3 | 3.5 | 2.5 | 3 | 243.0 | 80.01 |
| AXT-NLC 4 | 5.5 | 3.5 | 3 | 203.0 | 90.02 |
| AXT-NLC 5 | 3.5 | 4.5 | 9 | 80.0 | 70.43 |
| AXT-NLC 6 | 1.5 | 3.5 | 3 | 152.0 | 68.03 |
| AXT-NLC 7 | 1.5 | 2.5 | 6 | 193.0 | 60.21 |
| AXT-NLC 8 | 3.5 | 2.5 | 9 | 203.0 | 64.21 |
| AXT-NLC 9 | 5.5 | 4.5 | 6 | 130.0 | 89.12 |
| AXT-NLC 10 | 5.5 | 2.5 | 6 | 280.0 | 86.21 |
| AXT-NLC 11 | 3.5 | 3.5 | 6 | 165.0 | 82.02 |
| AXT-NLC 12 | 1.5 | 3.5 | 9 | 90.0 | 52.54 |
| AXT-NLC 13 | 3.5 | 4.5 | 3 | 108.1 | 84.12 |
| AXT-NLC 14 | 3.5 | 4.5 | 3 | 112.4 | 83.78 |
| AXT-NLC 15 | 3.5 | 4.5 | 3 | 109.9 | 84.62 |
| PS | ||||||
|---|---|---|---|---|---|---|
| Source | Std. Dev. | R2 | Adjusted R2 | Predicted R2 | PRESS | |
| Linear | 9.70 | 0.9798 | 0.9743 | 0.9571 | 2202.77 | |
| 2FI | 6.26 | 0.9938 | 0.9892 | 0.9688 | 1601.47 | |
| Quadratic | 3.54 | 0.9987 | 0.9965 | 0.9816 | 942.5 | Suggested |
| EE | ||||||
| Linear | 4.24 | 0.8897 | 0.8596 | 0.8358 | 294.99 | |
| 2FI | 4.91 | 0.8924 | 0.8117 | 0.7298 | 485.48 | |
| Quadratic | 0.49 | 0.9993 | 0.9980 | 0.9896 | 18.67 | Suggested |
| Particle Size (PS) | Entrapment Efficiency (EE) | |||||||
|---|---|---|---|---|---|---|---|---|
| Source | Sum of Squares | df | F Value | p-Value Prob > F | Sum of Squares | df | F-Value | p-Value |
| Model | 51,294.02 | 9 | 452.92 | <0.0001 | 1795.81 | 9 | 805.10 | <0.0001 |
| A: Total lipid | 11,250 | 1 | 894.03 | <0.0001 | 1127.41 | 1 | 4548.98 | <0.0001 |
| B: Surfactant | 36,585.13 | 1 | 2907.42 | <0.0001 | 46.75 | 1 | 188.64 | <0.0001 |
| C: Sonication time | 2485.13 | 1 | 197.49 | <0.0001 | 424.71 | 1 | 1713.68 | <0.0001 |
| AB | 121 | 1 | 9.62 | 0.026 | 2.54 | 1 | 10.26 | 0.0239 |
| AC | 529 | 1 | 42.04 | 0.001 | 1.18 | 1 | 4.79 | 0.0801 |
| BC | 72.25 | 1 | 5.74 | 0.062 * | 1.11 | 1 | 4.49 | 0.0876 |
| A2 | 18.00 | 1 | 1.43 | 0.285 * | 85.63 | 1 | 345.51 | <0.0001 |
| B2 | 7.85 | 1 | 0.62 | 0.465 | 14.01 | 1 | 56.55 | 0.0007 |
| C2 | 210.01 | 1 | 16.68 | 0.009 | 115.20 | 1 | 464.84 | <0.0001 |
| Residual | 62.91 | 5 | ---- | ---- | 1.23 | 5 | ---- | ---- |
| Lack of fit | 58.25 | 3 | 8.32 | 0.1092 * | 1.15 | 3 | 9.16 | 0.1000 * |
| Pure error | 4.66 | 2 | ----- | ------ | 0.08 | 2 | ----- | ----- |
| Cor total | 51,356.93 | 14 | ----- | ------ | 1797.05 | 14 | ----- | ----- |
| Batch Code | Conc of Poloxamer 407 (%) | Conc of Carbopol (%) | pH | Viscosity (cps, 37 °C) | Drug Content | Gelling Temp (°C) |
|---|---|---|---|---|---|---|
| AXT-NLC13G1 | 13 | 0.1 | 5.5 | 1054 ± 23 | 96.34 ± 0.84 | No gel formation up to 42 °C |
| AXT-NLC13G2 | 15 | 0.1 | 5.2 | 1432 ± 26 | 97.45 ± 0.43 | Viscosity increased but no gel formation up to 40 °C |
| AXT-NLC13G3 | 17 | 0.1 | 5.6 | 2109 ± 32 | 98.22 ± 0.24 | The gel form at 36–38 °C |
| AXT-NLC13G4 | 19 | 0.1 | 5.5 | 2532 ± 18 | 98.84 ± 0.76 | The gel formed at 28–34 °C |
| AXT-NLC13G5 | 21 | 0.1 | 5.3 | 3209 ± 26 | 96.85 ± 0.53 | The gel formed at 26–32 °C |
| PP | Type of Formulation with the Route of Administration | |||||||
|---|---|---|---|---|---|---|---|---|
| AXT-NLC13-G4 i.n | AXT-NLC13-G4 i.v | AXT-NLC13-G4 Oral | AXT-Sol i.n | |||||
| Brain | Plasma | Brain | Plasma | Brain | Plasma | Brain | Plasma | |
| Cmax (ng/mL) | 173.07 ± 13.02 b,c,d | 67.72 ± 6.08 | 101.18 ± 9.09 a,c | 110.21 ± 6.64 | 96.32 ± 8.00 a,b,d | 57.39 ± 4.11 | 99.70 ± 6.45 a,c | 50.27 ± 4.09 |
| Tmax (h) | 1.00 | 2.00 | 1.00 | 1.00 | 2.00 | 2.00 | 1.00 | 1 |
| AUC0–12 (ng∙h/mL) | 1409.58 ± 138.79 b,c,d | 547.86 ± 52.21 | 871.16 ± 82.95 a,c,d | 737.79 ± 72.19 | 720.67 ± 86.67 a,b,d | 469.58 ± 49.53 | 786.53 ± 93.86 a,b,c | 493.83 ± 43.18 |
| AUC0–∞ (ng∙h/mL) | 1520.47 ± 143.11 b,c,d | 627.23 ± 54.72 | 955.96 ± 85.58 a,c,d | 819.93 ± 75.03 | 781.04 ± 91.02 a,b | 514.31 ± 51.84 | 841.51 ± 97.21 a,b | 515.04 ± 45.44 |
| AUMC0–12 (ng∙h2/mL) | 11,126.77 ± 1347.33 b,c,d | 4979.71 ± 580.01 | 7617.40 ± 829.11 a,c,d | 6187.77 ± 779.83 | 5973.04 ± 924.00 a,b,d | 4176.95 ± 524.48 | 6811.74 ± 1035.80 a,b,c | 4227.58 ± 495.89 |
| AUMC0–∞ (ng∙h2/mL) | 14,432.88 ± 1456.36 b,c,d | 7403.29 ± 643.27 | 10,052.48 ± 894.95 a,c,d | 8598.35 ± 851.14 | 7739.61 ± 1034.50 a,b,d | 5461.53 ± 582.82 | 8341.93 ± 1119.87 a,b,c | 4794.36 ± 552.79 |
| Ke (h−1) | 0.17 ± 0.0015 b,c,b | 0.15 ± 0.0012 | 0.21 ± 0.0019 a,d | 0.19 ± 0.0027 | 0.73 ± 0.0025 a,,d | 0.21 ± 0.0034 | 0.26 ± 0.0021 a,b,c | 0.37 ± 0.0028 |
| T1/2 (h) | 4.03 ± 0.87 b,c,d | 4.53 ± 0.81 | 3.27 ± 0.70 a,d | 3.71 ± 0.73 | 3.65 ± 0.95 b,d | 3.27 ± 0.91 | 2.66 ± 0.75 a,b,c | 1.89 ± 0.83 |
| RB (%) * | 1.95 | |||||||
| RB ** | 1.81 | |||||||
| AB (%) # | 1.59 | |||||||
| FC and RA | Conc of AXT at 0.5 h (ng/mL) | Brain/Blood Ratio at 0.5 h | DTI | BTE (%) | BTP (%) |
|---|---|---|---|---|---|
| AXT-NLC13-G4 i.n | 75.29 ± 4.95 | 4.31 | 2.08 | 207.91 | 51.91 |
| Pure AXT i.n | 31.1 ± 3.61 | 2.14 | 1.40 | 140.14 | 28.64 |
| AXT-NLC13-G4 i.v | 28.09 ± 4.53 | 1.11 | - | - | - |
| AXT-NLC13-G4 oral | 17.80 ± 3.47 | 1.16 | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohanty, D.; Alsaidan, O.A.; Zafar, A.; Dodle, T.; Gupta, J.K.; Yasir, M.; Mohanty, A.; Khalid, M. Development of Atomoxetine-Loaded NLC In Situ Gel for Nose-to-Brain Delivery: Optimization, In Vitro, and Preclinical Evaluation. Pharmaceutics 2023, 15, 1985. https://doi.org/10.3390/pharmaceutics15071985
Mohanty D, Alsaidan OA, Zafar A, Dodle T, Gupta JK, Yasir M, Mohanty A, Khalid M. Development of Atomoxetine-Loaded NLC In Situ Gel for Nose-to-Brain Delivery: Optimization, In Vitro, and Preclinical Evaluation. Pharmaceutics. 2023; 15(7):1985. https://doi.org/10.3390/pharmaceutics15071985
Chicago/Turabian StyleMohanty, Dibyalochan, Omar Awad Alsaidan, Ameeduzzafar Zafar, Trishala Dodle, Jeetendra Kumar Gupta, Mohd Yasir, Anshuman Mohanty, and Mohammad Khalid. 2023. "Development of Atomoxetine-Loaded NLC In Situ Gel for Nose-to-Brain Delivery: Optimization, In Vitro, and Preclinical Evaluation" Pharmaceutics 15, no. 7: 1985. https://doi.org/10.3390/pharmaceutics15071985