
Therapeutic Drug Monitoring of Anti-TNFα Inhibitors: A Matter of Cut-Off Ranges

 , ,
, ,
Abstract
:1. Background
2. Materials and Methods
2.1. Laboratory Assays
2.2. Cut-Off Ranges
2.3. Sample Selection
2.4. Data Analysis
3. Results
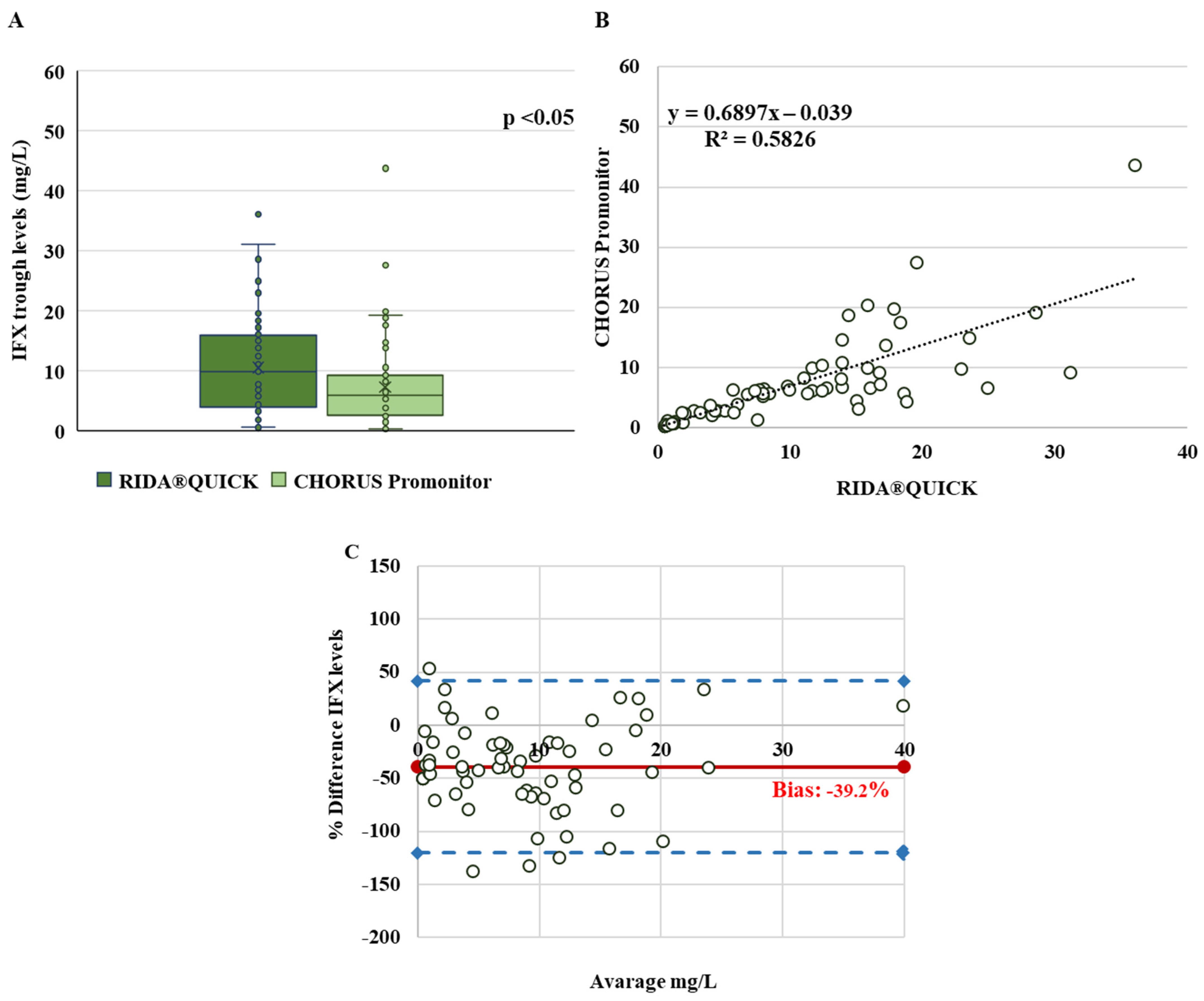
3.1. Infliximab Trough Levels
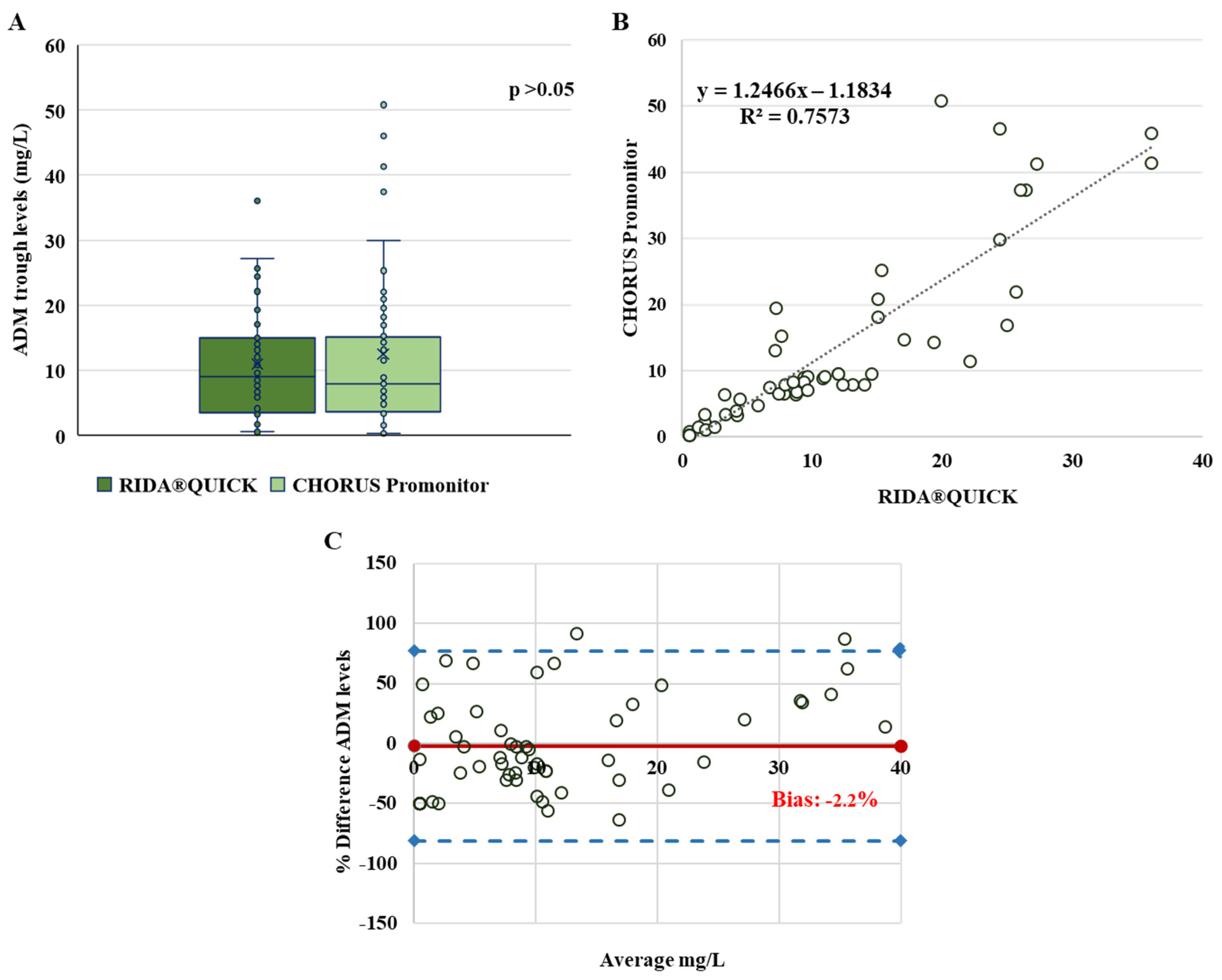
3.2. Adalimumab Trough Levels
3.3. Anti-Infliximab and Anti-Adalimumab Antibodies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Papamichael, K.; Cheifetz, A.S.; Melmed, G.Y.; Irving, P.M.; Casteele, N.V.; Kozuch, P.L.; Raffals, L.E.; Baidoo, L.; Bressler, B.; Devlin, S.M.; et al. Appropriate Therapeutic Drug Monitoring of Biologic Agents in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2019, 17, 1655–1668.e3. [Google Scholar] [CrossRef] [Green Version]
- Turner, D.; Ricciuto, A.; Lewis, A.; D’amico, F.; Dhaliwal, J.; Griffiths, A.M.; Bettenworth, D.; Sandborn, W.J.; Sands, B.E.; Reinisch, W.; et al. STRIDE-II: An update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining therapeutic goals for treat-to-target strategies in IBD. Gastroenterology 2021, 160, 1570–1583. [Google Scholar] [CrossRef]
- Aardoom, M.; Veereman, G.; de Ridder, L. A Review on the Use of Anti-TNF in Children and Adolescents with Inflammatory Bowel Disease. Int. J. Mol. Sci. 2019, 20, 2529. [Google Scholar] [CrossRef] [Green Version]
- van Rheenen, P.F.; Aloi, M.; Assa, A.; Bronsky, J.; Escher, J.C.; Fagerberg, U.L.; Gasparetto, M.; Gerasimidis, K.; Griffiths, A.; Henderson, P.; et al. The Medical Management of Paediatric Crohn’s Disease: An ECCO-ESPGHAN Guideline Update. J. Crohns Colitis 2020, 7, jjaa161. [Google Scholar] [CrossRef]
- Vermeire, S.; Gils, A.; Accossato, P.; Lula, S.; Marren, A. Immunogenicity of biologics in inflammatory bowel disease. Therap. Adv. Gastroenterol. 2018, 11, 1756283X17750355. [Google Scholar] [CrossRef] [Green Version]
- Qiu, Y.; Chen, B.L.; Mao, R.; Zhang, S.H.; He, Y.; Zeng, Z.R.; Ben-Horin, S.; Chen, M.H. Systematic review with meta-analysis: Loss of response and requirement of anti-TNFα dose intensification in Crohn’s disease. J. Gastroenterol. 2017, 52, 535–554. [Google Scholar] [CrossRef]
- Pecoraro, V.; De Santis, E.; Melegari, A.; Trenti, T. The impact of immunogenicity of TNFα inhibitors in autoimmune inflammatory disease. A systematic review and meta-analysis. Autoimmun. Rev. 2017, 16, 564–575. [Google Scholar] [CrossRef]
- Atzeni, F.; Talotta, R.; Salaffi, F.; Cassinotti, A.; Varisco, V.; Battellino, M.; Ardizzone, S.; Pace, F.; Sarzi-Puttini, P. Immunogenicity and autoimmunity during anti-TNF therapy. Autoimmun. Rev. 2013, 12, 703–708. [Google Scholar] [CrossRef]
- Mitrev, N.; Vande Casteele, N.; Seow, C.H.; Andrews, J.M.; Connor, S.J.; Moore, G.T.; Barclay, M.; Begun, J.; Bryant, R.; Chan, W.; et al. Review article: Consensus statements on therapeutic drug monitoring of anti-tumour necrosis factor therapy in inflammatory bowel diseases. Aliment. Pharmacol. Ther. 2017, 46, 1037–1053. [Google Scholar] [CrossRef] [Green Version]
- Papamichael, K.; Cheifetz, A.S. Use of anti-TNF drug levels to optimise patient management. Frontline Gastroenterol. 2016, 7, 289–300. [Google Scholar] [CrossRef] [Green Version]
- Vande Casteele, N.; Ferrante, M.; Van Assche, G.; Ballet, V.; Compernolle, G.; Van Steen, K.; Simoens, S.; Rutgeerts, P.; Gils, A.; Vermeire, S. Trough concentrations of infliximab guide dosing for patients with inflammatory bowel disease. Gastroenterology 2015, 148, 1320–1329.e3. [Google Scholar] [CrossRef]
- Cheifetz, A.S.; Abreu, M.T.; Afif, W.; Cross, R.K.; Dubinsky, M.C.; Loftus, E.V., Jr.; Osterman, M.T.; Saroufim, A.; Siegel, C.A.; Yarur, A.J.; et al. A Comprehensive Literature Review and Expert Consensus Statement on Therapeutic Drug Monitoring of Biologics in Inflammatory Bowel Disease. Am. J. Gastroenterol. 2021, 116, 2014–2025. [Google Scholar] [CrossRef]
- Carman, N.; Mack, D.R.; Benchimol, E.I. Therapeutic Drug Monitoring in Pediatric Inflammatory Bowel Disease. Curr. Gastroenterol. Rep. 2018, 20, 18. [Google Scholar] [CrossRef]
- Papamichael, K.; Chachu, K.A.; Vajravelu, R.K.; Vaughn, B.P.; Ni, J.; Osterman, M.T.; Cheifetz, A.S. Improved long-term outcomes of patients with inflammatory bowel disease receiving proactive compared with reactive monitoring of serum concentrations of infliximab. Clin. Gastroenterol. Hepatol. 2017, 15, 1580–1588.e3. [Google Scholar] [CrossRef]
- Vande Casteele, N. Assays for measurement of TNF antagonists in practice. Frontline Gastroenterol. 2017, 8, 236–242. [Google Scholar] [CrossRef] [Green Version]
- Steenholdt, C.; Ainsworth, M.A.; Tovey, M.; Klausen, T.W.; Thomsen, O.O.; Brynskov, J.; Bendtzen, K. Comparison of techniques for monitoring infliximab and antibodies against infliximab in Crohn’s disease. Ther. Drug Monit. 2013, 35, 530–538. [Google Scholar] [CrossRef]
- Vande Casteele, N.; Buurman, D.J.; Sturkenboom, M.G.; Kleibeuker, J.H.; Vermeire, S.; Rispens, T.; van der Kleij, D.; Gils, A.; Dijkstra, G. Detection of infliximab levels and anti-infliximab antibodies: A comparison of three different assays. Aliment. Pharmacol. Ther. 2012, 36, 765–771. [Google Scholar] [CrossRef] [Green Version]
- Sam, M.J.; Connor, S.J.; Ng, W.W.; Toong, C.M. Comparative Evaluation of 4 Commercially Available ELISA Kits for Measuring Adalimumab and Anti-adalimumab Antibodies. Ther. Drug Monit. 2020, 42, 821–828. [Google Scholar] [CrossRef]
- Curci, D.; Lucafò, M.; Cifù, A.; Bramuzzo, M.; Martelossi, S.; Favretto, D.; De Pellegrin, F.; Fabris, M.; Vascotto, F.; Naviglio, S.; et al. Determination of Serum Infliximab Concentration by Point-of-care Devices in Children With Inflammatory Bowel Disease. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 474–479. [Google Scholar] [CrossRef]
- Laserna-Mendieta, E.J.; Salvador-Martín, S.; Arias-González, L.; Ruiz-Ponce, M.; Menchén, L.A.; Sánchez, C.; López-Fernández, L.A.; Lucendo, A.J. Comparison of a new rapid method for the determination of adalimumab serum levels with two established ELISA kits. Clin. Chem. Lab. Med. 2019, 57, 1906–1914. [Google Scholar] [CrossRef]
- West, T.A.; Sam, M.; Toong, C. Comparison of three commercially available ELISA assays for anti-infliximab antibodies. Pathology 2021, 53, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Imbrechts, M.; Van Stappen, T.; Compernolle, G.; Tops, S.; Gils, A. Anti-infliximab antibodies: How to compare old and new data? J. Pharm. Biomed. Anal. 2020, 177, 112842. [Google Scholar] [CrossRef] [PubMed]
- Irving, P.M.; Gecse, K.B. Optimizing Therapies Using Therapeutic Drug Monitoring: Current Strategies and Future Perspectives. Gastroenterology 2022, 162, 1512–1524. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Bertin, D.; Serrero, M.; Grimaud, J.C.; Desjeux, A.; Desplat-Jégo, S. Monitoring of infliximab trough levels and anti-infliximab antibodies in inflammatory bowel diseases: A comparison of three commercially available ELISA kits. Cytokine 2020, 126, 154859. [Google Scholar] [CrossRef]
- Dutzer, D.; Nasser, Y.; Berger, A.E.; Roblin, X.; Paul, S. Letter: New thresholds need to be defined when using point of care assays to monitor infliximab trough levels in IBD patients. Aliment. Pharmacol. Ther. 2018, 47, 1571–1573. [Google Scholar] [CrossRef] [Green Version]
- Afonso, J.; Lopes, S.; Gonçalves, R.; Caldeira, P.; Lago, P.; de Sousa, H.T.; Ramos, J.; Gonçalves, A.R.; Ministro, P.; Rosa, I.; et al. Proactive therapeutic drug monitoring of infliximab: A comparative study of a new point-of-care quantitative test with two established ELISA assays. Aliment. Pharmacol. Ther. 2016, 44, 684–692. [Google Scholar] [CrossRef]
- Magro, F.; Afonso, J.; Lopes, S.; Coelho, R.; Gonçalves, R.; Caldeira, P.; Lago, P.; de Sousa, H.T.; Ramos, J.; Gonçalves, A.R.; et al. Clinical performance of an infliximab rapid quantification assay. Ther. Adv. Gastroenterol. 2017, 10, 651–660. [Google Scholar] [CrossRef] [Green Version]
- Nasser, Y.; Labetoulle, R.; Harzallah, I.; Berger, A.-E.; Roblin, X.; Paul, S. Comparison of point-of-care and classical immunoassays for the monitoring infliximab and antibodies against infliximab in IBD. Dig. Dis. Sci. 2018, 63, 2714–2721. [Google Scholar] [CrossRef]
- Papamichael, K.; Clarke, W.T.; Vande Casteele, N.; Germansky, K.A.; Feuerstein, J.D.; Melmed, G.Y.; Siegel, C.A.; Irving, P.M.; Cheifetz, A.S. Comparison of Assays for Therapeutic Monitoring of Infliximab and Adalimumab in Patients With Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2021, 19, 839–841.e2. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Groups | N° of Patients (%) | Kappa Statistics | |||
|---|---|---|---|---|---|
| IFX concentrations | RIDA®QUICK N = 65 | CHORUS Promonitor N = 65 | K | SE | CI 95% |
| <3 mg/L | 15 (23) | 22 (33.8) | 0.410 | 0.078 | 0.257–0.563 |
| ≥3 to ≤7 mg/L | 10 (15.5) | 23 (35.4) | |||
| >7 mg/L | 40 (61.5) | 20 (30.8) | |||
| Groups | N° of Patients (%) | Kappa Statistics | |||
|---|---|---|---|---|---|
| ADM concentrations | RIDA®QUICK N = 58 | CHORUS Promonitor N = 58 | K | SE | CI 95% |
| <5 mg/L | 18 (31) | 17 (29.3) | 0.66 | 0.082 | 0.503–0.824 |
| ≥5 to ≤10 mg/mL | 16 (27.6) | 22 (38) | |||
| >10 mg/L | 24 (41.4) | 19 (32.7) | |||
| Groups | N° of Samples (%) | Kappa Statistics | |||||
|---|---|---|---|---|---|---|---|
| Anti-IFX Antibodies | RIDASCREEN® (ng/mL) | K | SE | CI 95% | |||
| Positive | Negative | Total | |||||
| CHORUS Promonitor (AU/mL) | Positive | 25 (78.1) | 0 (0) | 25 (78.1) | 0.904 | 0.094 | 0.719–1.000 |
| Negative | 1 (3.1) | 6 (18.8) | 7 (21.9) | ||||
| Total | 26 (81.2) | 6 (18.8) | 32 (100) | ||||
| Anti-ADM Antibodies | RIDASCREEN® (ng/mL) | K | SE | CI 95% | |||
| Positive | Negative | Total | |||||
| CHORUS Promonitor (AU/mL) | Positive | 13 (56.5) | 0 (0) | 13 (56.5) | 0.819 | 0.120 | 0.583–1.000 |
| Negative | 2 (8.7) | 8 (34.8) | 10 (43.5) | ||||
| Total | 15 (65.2) | 8 (34.8) | 23 (100) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheli, S.; Savino, D.; Penagini, F.; Zuccotti, G.; Zuin, G.; Clementi, E.; Cattaneo, D. Therapeutic Drug Monitoring of Anti-TNFα Inhibitors: A Matter of Cut-Off Ranges. Pharmaceutics 2023, 15, 1834. https://doi.org/10.3390/pharmaceutics15071834
Cheli S, Savino D, Penagini F, Zuccotti G, Zuin G, Clementi E, Cattaneo D. Therapeutic Drug Monitoring of Anti-TNFα Inhibitors: A Matter of Cut-Off Ranges. Pharmaceutics. 2023; 15(7):1834. https://doi.org/10.3390/pharmaceutics15071834
Chicago/Turabian StyleCheli, Stefania, Diego Savino, Francesca Penagini, Gianvincenzo Zuccotti, Giovanna Zuin, Emilio Clementi, and Dario Cattaneo. 2023. "Therapeutic Drug Monitoring of Anti-TNFα Inhibitors: A Matter of Cut-Off Ranges" Pharmaceutics 15, no. 7: 1834. https://doi.org/10.3390/pharmaceutics15071834