
Development of a Minimalistic Physiologically Based Pharmacokinetic (mPBPK) Model for the Preclinical Development of Spectinamide Antibiotics

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
2.2. Animals
2.3. Plasma Protein Binding Assay
2.4. Blood to Plasma Partition Ratio Assay
2.5. Pharmacokinetic Studies in Healthy and Infected Mice
2.6. Pharmacokinetic Studies in Healthy Rats
2.7. Quantitative Analysis of Spectinamide Antibiotics
2.7.1. Sample Preparation
2.7.2. Chromatographic Conditions
2.7.3. Mass Spectrometric Conditions
2.8. Development of the PBPK Model
2.9. Model Qualification
- Visual inspection of overlays of predicted and observed concentration-time profile indicating a reasonable agreement
- The observed data are within the 95% prediction interval of the model predictions
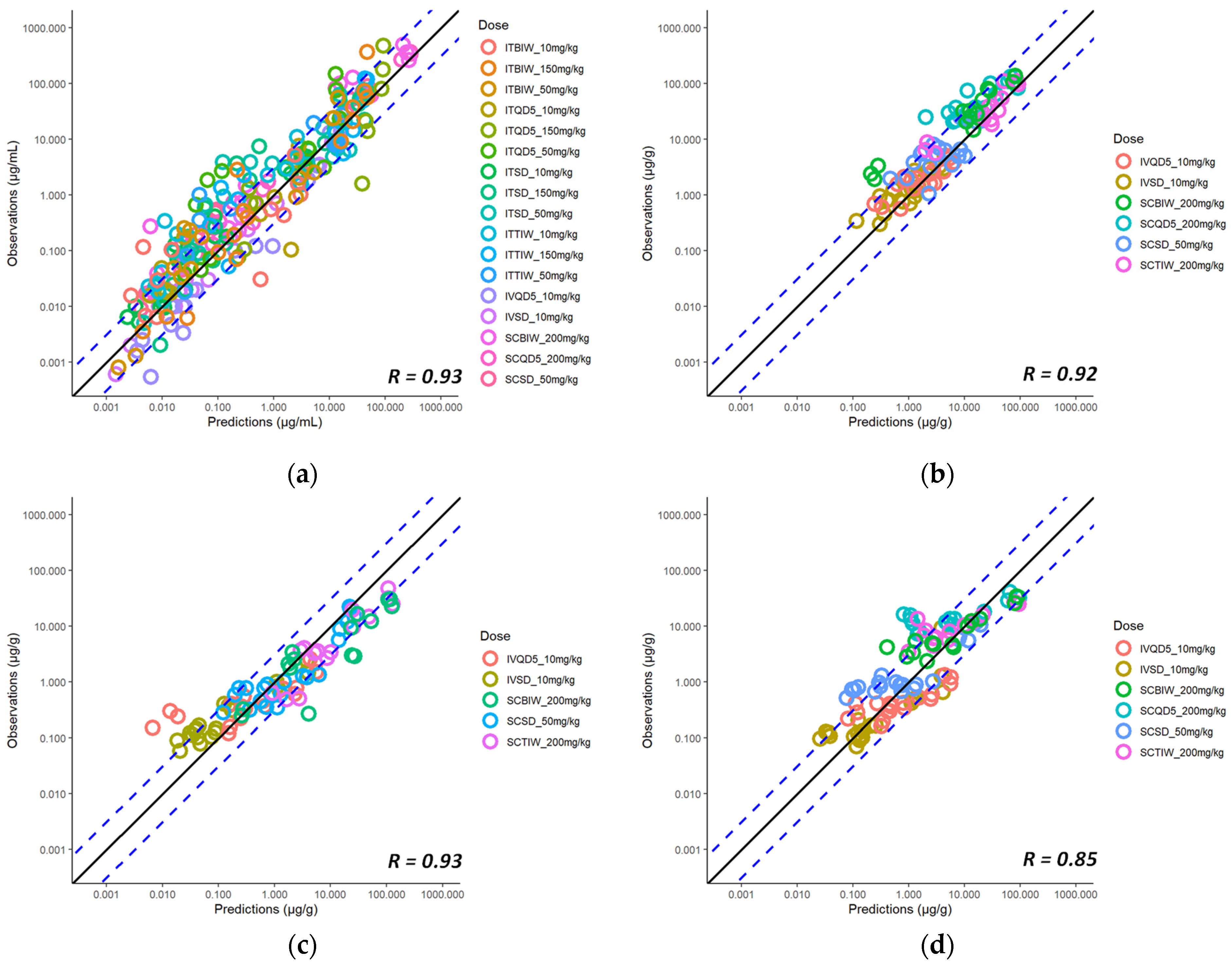
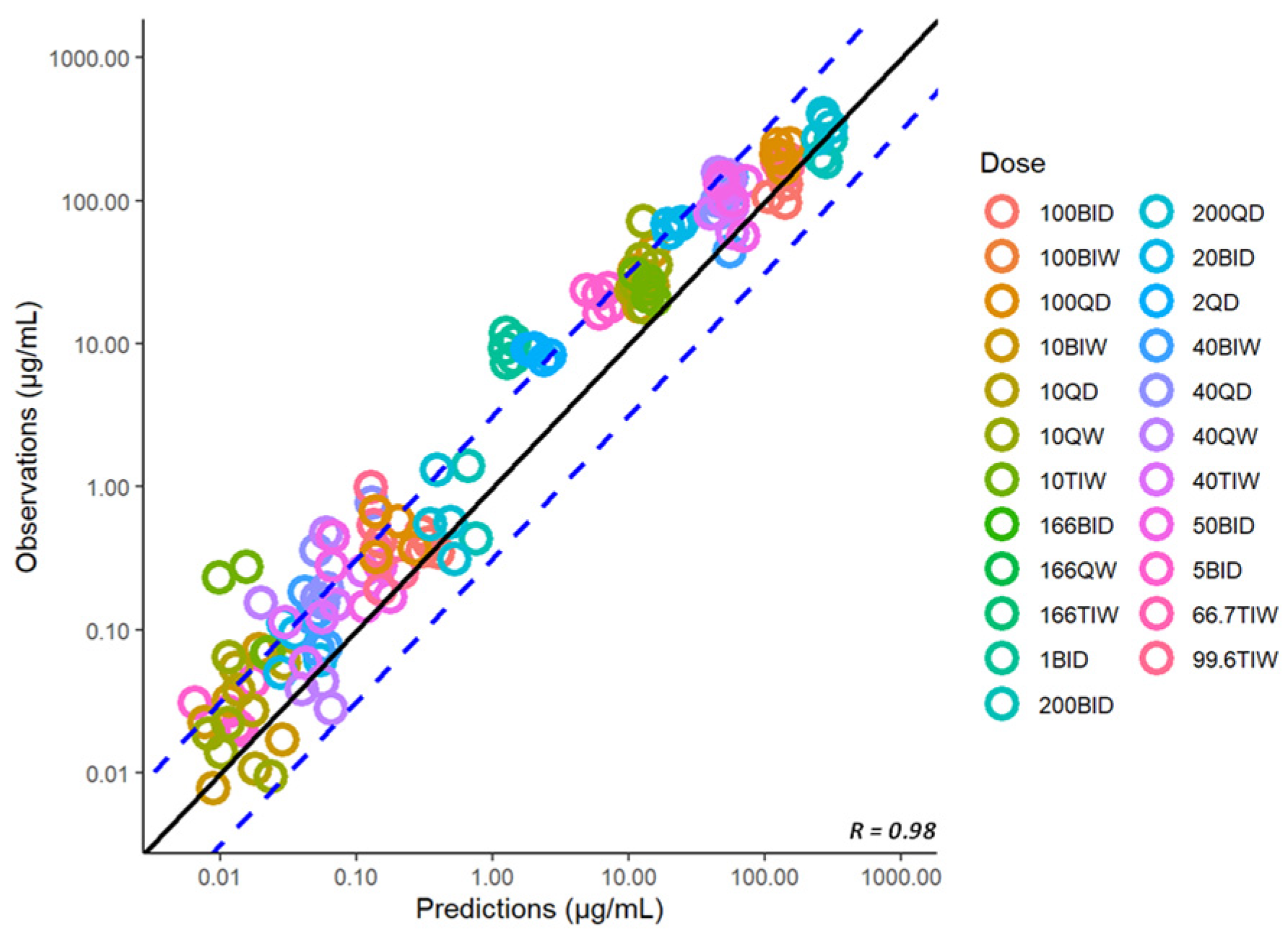
- The two-fold acceptance criteria between the observed and predicted exposures
2.10. Exploratory Simulation of Relative Drug Exposure in Granulomatous Lesion Substructures
3. Results
3.1. PK Data for PBPK Model Development
3.2. Model Parameterization for Spectinamide 1599
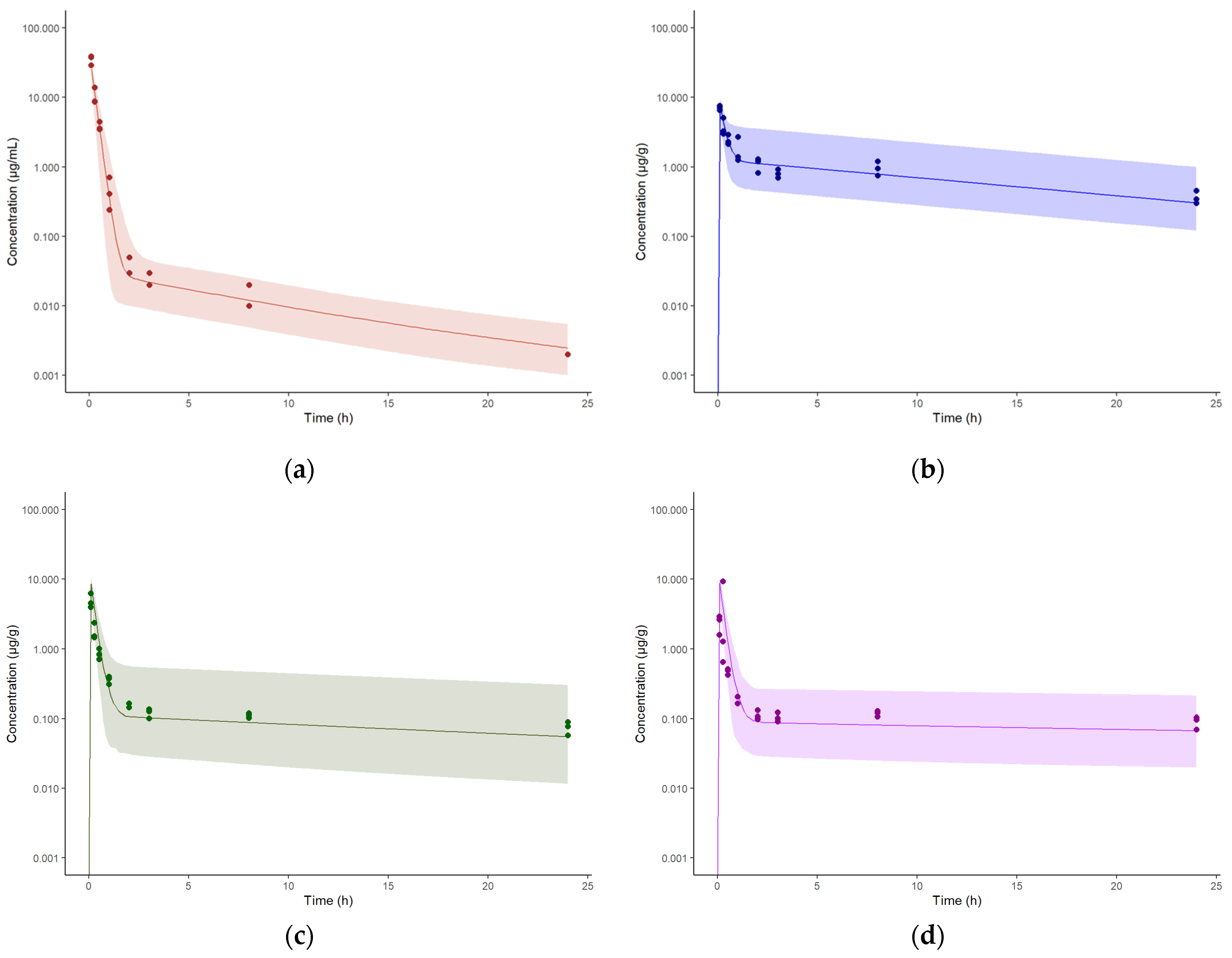
3.3. Model Establishment for Intravenous Administration in Healthy Mice
3.4. Model Expansion to Intrapulmonary Aerosol Administration in Healthy Mice
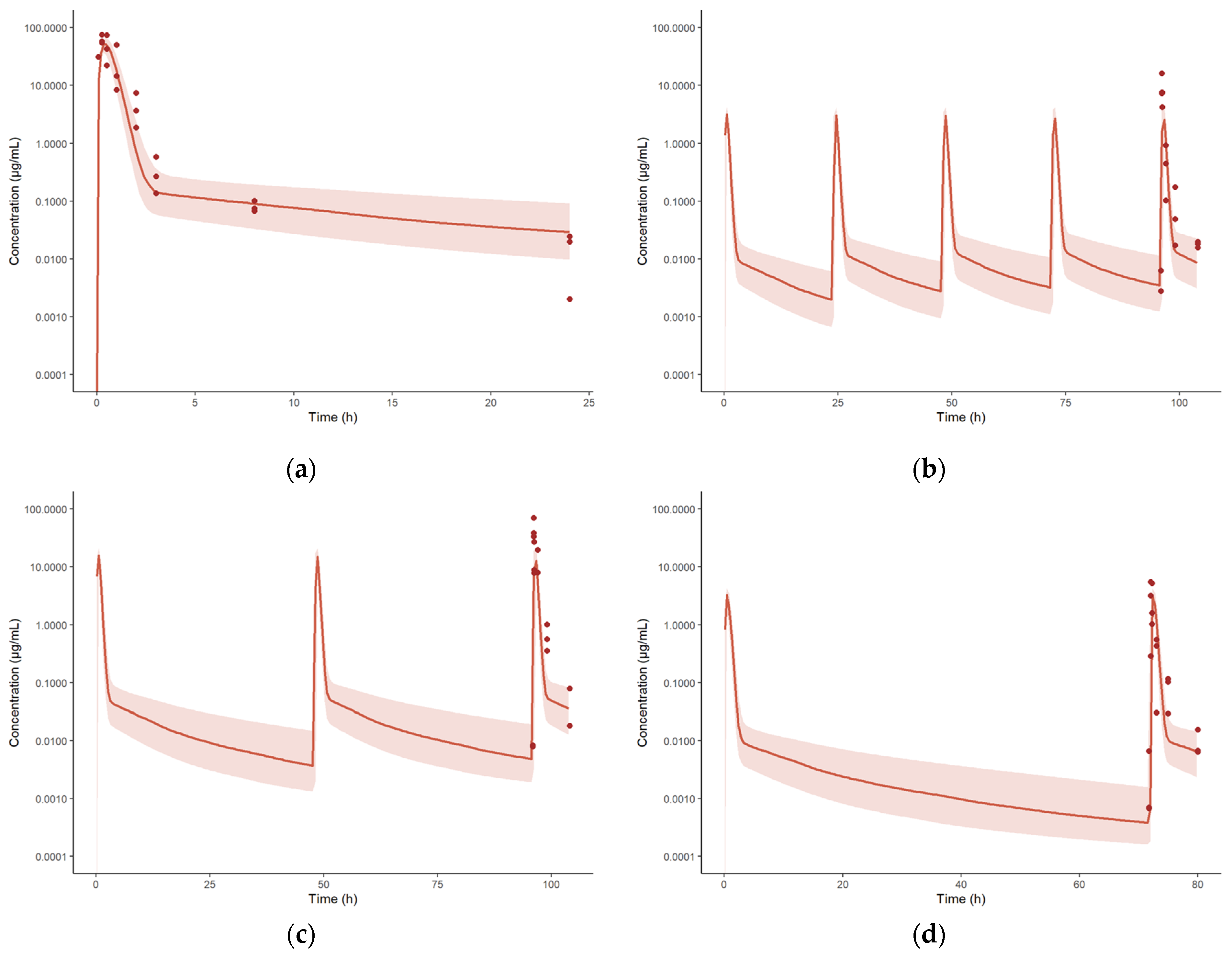
3.5. Model Expansion to Subcutaneous Administration in Healthy Mice
3.6. Model Expansion to Infected Mice
3.7. Model Expansion to Rat as a Different Species
3.8. Model Expansion to Another Structurally Similar Compound, Spectinamide 1810
3.9. Exploratory Assessment of Lesion Distribution of Spectinamide 1599 Based on the Simcyp Granuloma Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Tackling the Drug-Resistant TB Crisis. Available online: https://www.who.int/tb/areas-of-work/drug-resistant-tb/en/ (accessed on 11 March 2023).
- Robertson, G.T.; Scherman, M.S.; Bruhn, D.F.; Liu, J.; Hastings, C.; McNeil, M.R.; Butler, M.M.; Bowlin, T.L.; Lee, R.B.; Lee, R.E.; et al. Spectinamides are effective partner agents for the treatment of tuberculosis in multiple mouse infection models. J. Antimicrob. Chemother. 2017, 72, 770–777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoagland, D.T.; Liu, J.; Lee, R.B.; Lee, R.E. New agents for the treatment of drug-resistant Mycobacterium tuberculosis. Adv. Drug Deliv. Rev. 2016, 102, 55–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, R.E.; Hurdle, J.G.; Liu, J.; Bruhn, D.F.; Matt, T.; Scherman, M.S.; Vaddady, P.K.; Zheng, Z.; Qi, J.; Akbergenov, R.; et al. Spectinamides: A new class of semisynthetic antituberculosis agents that overcome native drug efflux. Nat. Med. 2014, 20, 152–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez-Juarrero, M.; Lukka, P.B.; Wagh, S.; Walz, A.; Arab, J.; Pearce, C.; Ali, Z.; Ryman, J.T.; Parmar, K.; Temrikar, Z.; et al. Preclinical Evaluation of Inhalational Spectinamide-1599 Therapy against Tuberculosis. ACS Infect. Dis. 2021, 7, 2850–2863. [Google Scholar] [CrossRef] [PubMed]
- Rathi, C.; Lukka, P.B.; Wagh, S.; Lee, R.E.; Lenaerts, A.J.; Braunstein, M.; Hickey, A.; Gonzalez-Juarrero, M.; Meibohm, B. Comparative pharmacokinetics of spectinamide 1599 after subcutaneous and intrapulmonary aerosol administration in mice. Tuberculosis 2019, 114, 119–122. [Google Scholar] [CrossRef]
- Wagh, S.; Rathi, C.; Lukka, P.B.; Parmar, K.; Temrikar, Z.; Liu, J.; Scherman, M.S.; Lee, R.E.; Robertson, G.T.; Lenaerts, A.J.; et al. Model-Based Exposure-Response Assessment for Spectinamide 1810 in a Mouse Model of Tuberculosis. Antimicrob. Agents Chemother. 2021, 65, e0174420. [Google Scholar] [CrossRef]
- Jones, H.M.; Chen, Y.; Gibson, C.; Heimbach, T.; Parrott, N.; Peters, S.A.; Snoeys, J.; Upreti, V.V.; Zheng, M.; Hall, S.D. Physiologically based pharmacokinetic modeling in drug discovery and development: A pharmaceutical industry perspective. Clin. Pharmacol. Ther. 2015, 97, 247–262. [Google Scholar] [CrossRef]
- Shebley, M.; Sandhu, P.; Riedmaier, A.E.; Jamei, M.; Narayanan, R.; Patel, A.; Peters, S.A.; Reddy, V.P.; Zheng, M.; de Zwart, L.; et al. Physiologically Based Pharmacokinetic Model Qualification and Reporting Procedures for Regulatory Submissions: A Consortium Perspective. Clin. Pharmacol. Ther. 2018, 104, 88–110. [Google Scholar] [CrossRef] [Green Version]
- Cao, Y.; Jusko, W.J. Applications of minimal physiologically-based pharmacokinetic models. J. Pharmacokinet. Pharmacodyn. 2012, 39, 711–723. [Google Scholar] [CrossRef]
- Liu, J.; Bruhn, D.F.; Lee, R.B.; Zheng, Z.; Janusic, T.; Scherbakov, D.; Scherman, M.S.; Boshoff, H.I.; Das, S.; Rakesh; et al. Structure-Activity Relationships of Spectinamide Antituberculosis Agents: A Dissection of Ribosomal Inhibition and Native Efflux Avoidance Contributions. ACS Infect. Dis. 2017, 3, 72–88. [Google Scholar] [CrossRef] [Green Version]
- Wen, Z.; Huang, Y.; Behler, N.; Bambal, R.; Bhoopathy, S.; Owen, A. Determination of red blood cell partitioning and whole blood to plasma ratio using human, rat, and mouse blood: Methods, model compounds and species differences. AAPS J. 2010, 12, 4305. [Google Scholar]
- Wagh, S.J. Model-Based Dose-Exposure-Response Assessment for Lead and Backup Spectinamide in a Mouse Model of Tuberculosis. Ph.D. Thesis, University of Tennessee Health Science Center, Memphis, TN, USA, 2020. [Google Scholar]
- Rathi, C. Translational Pharmacokinetic-Pharmacodynamic Modeling and Simulation in the Development of Spectinamides, a Novel Class of Anti-Tuberculosis Agents. Ph.D. Thesis, The University of Tennessee Health Science Center, Memphis, TN, USA, 2017. [Google Scholar]
- Nasu, R.; Kumagai, Y.; Kogetsu, H.; Tsujimoto, M.; Ohtani, H.; Sawada, Y. Physiologically based pharmacokinetic model for pralmorelin hydrochloride in rats. Drug Metab. Dispos. 2005, 33, 1488–1494. [Google Scholar] [CrossRef] [Green Version]
- Davies, B.; Morris, T. Physiological parameters in laboratory animals and humans. Pharm. Res. 1993, 10, 1093–1095. [Google Scholar] [CrossRef]
- Shah, D.K.; Betts, A.M. Towards a platform PBPK model to characterize the plasma and tissue disposition of monoclonal antibodies in preclinical species and human. J. Pharmacokinet. Pharmacodyn. 2012, 39, 67–86. [Google Scholar] [CrossRef]
- Frohlich, E.; Mercuri, A.; Wu, S.; Salar-Behzadi, S. Measurements of Deposition, Lung Surface Area and Lung Fluid for Simulation of Inhaled Compounds. Front. Pharmacol. 2016, 7, 181. [Google Scholar] [CrossRef]
- Poulin, P.; Theil, F.P. Prediction of pharmacokinetics prior to in vivo studies. II. Generic physiologically based pharmacokinetic models of drug disposition. J. Pharm. Sci. 2002, 91, 1358–1370. [Google Scholar] [CrossRef]
- Chan, P.L.; Jacqmin, P.; Lavielle, M.; McFadyen, L.; Weatherley, B. The use of the SAEM algorithm in MONOLIX software for estimation of population pharmacokinetic-pharmacodynamic-viral dynamics parameters of maraviroc in asymptomatic HIV subjects. J. Pharmacokinet. Pharmacodyn. 2011, 38, 41–61. [Google Scholar] [CrossRef] [Green Version]
- Wickham, H. Package ‘ggplot2′: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Sasindran, S.J.; Torrelles, J.B. Mycobacterium Tuberculosis Infection and Inflammation: What is Beneficial for the Host and for the Bacterium? Front. Microbiol. 2011, 2, 2. [Google Scholar] [CrossRef] [Green Version]
- Dartois, V. The path of anti-tuberculosis drugs: From blood to lesions to mycobacterial cells. Nat. Rev. Microbiol. 2014, 12, 159–167. [Google Scholar] [CrossRef] [Green Version]
- Gaohua, L.; Wedagedera, J.; Small, B.G.; Almond, L.; Romero, K.; Hermann, D.; Hanna, D.; Jamei, M.; Gardner, I. Development of a Multicompartment Permeability-Limited Lung PBPK Model and Its Application in Predicting Pulmonary Pharmacokinetics of Antituberculosis Drugs. CPT Pharmacomet. Syst. Pharmacol. 2015, 4, 605–613. [Google Scholar] [CrossRef]
- Rose, R.H.; Gaohua, L.; Wedagedera, J.; Small, B.G.; Barnett, A.; Romero, K.; Hermann, D.; Gardner, I.; Jamei, M. Development of a novel multi-compartment granuloma model to predict local drug distribution and its impact on pharmacodynamics and disease progression in tuberculosis. In Proceedings of the PAGE Conference, Lisboa, Portugal, 7–10 June 2016. [Google Scholar]
- Santos, K.; Lukka, P.B.; Grzegorzewicz, A.; Jackson, M.; Trivedi, A.; Pavan, F.; Chorilli, M.; Braunstein, M.; Hickey, A.; Meibohm, B.; et al. Primary Lung Dendritic Cell Cultures to Assess Efficacy of Spectinamide-1599 Against Intracellular Mycobacterium tuberculosis. Front. Microbiol. 2018, 9, 1895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edginton, A.N.; Ahr, G.; Willmann, S.; Stass, H. Defining the role of macrophages in local moxifloxacin tissue concentrations using biopsy data and whole-body physiologically based pharmacokinetic modelling. Clin. Pharmacokinet. 2009, 48, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Zumla, A.; Raviglione, M.; Hafner, R.; von Reyn, C.F. Tuberculosis. N. Engl. J. Med. 2013, 368, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Nestorov, I. Whole body pharmacokinetic models. Clin. Pharmacokinet. 2003, 42, 883–908. [Google Scholar] [CrossRef]
- Khor, S.P.; Bozigian, H.; Mayersohn, M. Potential error in the measurement of tissue to blood distribution coefficients in physiological pharmacokinetic modeling. Residual tissue blood. II. Distribution of phencyclidine in the rat. Drug Metab. Dispos. 1991, 19, 486–490. [Google Scholar]
- Robertson, G.T.; Ramey, M.E.; Massoudi, L.M.; Carter, C.L.; Zimmerman, M.; Kaya, F.; Graham, B.G.; Gruppo, V.; Hastings, C.; Woolhiser, L.K.; et al. Comparative Analysis of Pharmacodynamics in the C3HeB/FeJ Mouse Tuberculosis Model for DprE1 Inhibitors TBA-7371, PBTZ169, and OPC-167832. Antimicrob. Agents Chemother. 2021, 65, e0058321. [Google Scholar] [CrossRef]
- Walter, N.D.; Born, S.E.M.; Robertson, G.T.; Reichlen, M.; Dide-Agossou, C.; Ektnitphong, V.A.; Rossmassler, K.; Ramey, M.E.; Bauman, A.A.; Ozols, V.; et al. Mycobacterium tuberculosis precursor rRNA as a measure of treatment-shortening activity of drugs and regimens. Nat. Commun. 2021, 12, 2899. [Google Scholar] [CrossRef]
- Rostami-Hodjegan, A.; Toon, S. Physiologically Based Pharmacokinetics as a Component of Model-Informed Drug Development: Where We Were, Where We Are, and Where We Are Heading. J. Clin. Pharmacol. 2020, 60 (Suppl. S1), S12–S16. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug | Species | Disease Status | Route of Administration | Dosing Frequency | Dose Level (mg/kg) | No. of Animals | No. of Data Points/Animal (Tissues) | No. of Animals/Sampling Time Point | Reference |
|---|---|---|---|---|---|---|---|---|---|
| Spectinamide 1599 | BALB/c mice | Healthy | Intravenous | Single dose | 10 | 24 | 1 (plasma, lung, liver, spleen) | 3 | [5] |
| Spectinamide 1599 | BALB/c mice | Healthy | Intravenous | Daily dosing for 5 days (QD5) | 10 | 21 | 1 (plasma, lung, liver, spleen) | 3 | [5] |
| Spectinamide 1599 | BALB/c mice | Healthy | Subcutaneous | Single Dose | 50 | 24 | 1 (plasma, lung, liver, spleen) | 3 | [5,6] |
| Spectinamide 1599 | BALB/c mice | Healthy | Subcutaneous | Single Dose | 200 | 27 | 1 (plasma, lung, liver, spleen) | 3 | [5,6] |
| Spectinamide 1599 | BALB/c mice | Healthy | Subcutaneous | Daily dosing for 5 days (QD5) | 200 | 18 | 1 (plasma, lung, liver, spleen) | 3 | [5,6] |
| Spectinamide 1599 | BALB/c mice | Healthy | Subcutaneous | Twice a week (BIW) | 200 | 18 | 1 (plasma, lung, liver, spleen) | 3 | [5,6] |
| Spectinamide 1599 | BALB/c mice | Healthy | Subcutaneous | Three times a week (TIW) | 200 | 18 | 1 (plasma, lung, liver, spleen) | 3 | [5,6] |
| Spectinamide 1599 | BALB/c mice | Healthy | Subcutaneous | Three times a week (TIW) | 200 | 18 | 1 (plasma, lung, liver, spleen) | 3 | [5,6] |
| Spectinamide 1599 | BALB/c mice | Infected | Subcutaneous - Study 1A | Twice daily (QD5 for 4 weeks) | 1, 5, 20, 50, 100, 200 | 30 | 2 (plasma) | 5 | [13] |
| Spectinamide 1599 | BALB/c mice | Infected | Subcutaneous - Study 1A | Once daily (QD5 for 4 weeks) | 2, 10, 40, 100, 200 | 25 | 2 (plasma) | 5 | [13] |
| Spectinamide 1599 | BALB/c mice | Infected | Subcutaneous - Study 1A | TIW for 4 weeks | 10, 40, 99.6 | 15 | 2 (plasma) | 5 | [13] |
| Spectinamide 1599 | BALB/c mice | Infected | Subcutaneous - Study 1A | BIW for 4 weeks | 10, 40 | 10 | 2 (plasma) | 5 | [13] |
| Spectinamide 1599 | BALB/c mice | Infected | Subcutaneous - Study 1A | Once every week for 4 weeks | 10, 40 | 10 | 2 (plasma) | 5 | [13] |
| Spectinamide 1599 | BALB/c mice | Infected | Subcutaneous - Study 1B | Twice daily (QD5 for 4 weeks) | 100, 166 | 12 | 2 (plasma) | 6 | [13] |
| Spectinamide 1599 | BALB/c mice | Infected | Subcutaneous - Study 1B | TIW for 4 weeks | 66, 166 | 12 | 2 (plasma) | 6 | [13] |
| Spectinamide 1599 | BALB/c mice | Infected | Subcutaneous - Study 1B | BIW for 4 weeks | 100 | 6 | 2 (plasma) | 6 | [13] |
| Spectinamide 1599 | BALB/c mice | Infected | Subcutaneous - Study 1B | Once every week for 4 weeks | 166 | 6 | 2 (plasma) | 6 | [13] |
| Spectinamide 1599 | BALB/c mice | Infected | Subcutaneous - Study 1C | Twice daily (QD5 for 4 weeks) | 50 | 6 | 2 (plasma) | 6 | [13] |
| Spectinamide 1599 | BALB/c mice | Infected | Subcutaneous - Study 1C | Once daily (QD5 for 4 weeks) | 100 | 6 | 2 (plasma) | 6 | [13] |
| Spectinamide 1599 | BALB/c mice | Infected | Subcutaneous - Study 1C | TIW for 4 weeks | 166 | 6 | 2 (plasma) | 6 | [13] |
| Spectinamide 1599 | BALB/c mice | Infected | Subcutaneous - Study 1C | BIW for 4 weeks | 100 | 6 | 2 (plasma) | 6 | [13] |
| Spectinamide 1599 | BALB/c mice | Healthy | Intrapulmonary Aerosol | Single Dose | 10, 50, 150 | 72 | 1 (plasma, lung, liver, spleen, ELF) | 3 | [5,6] |
| Spectinamide 1599 | BALB/c mice | Healthy | Intrapulmonary Aerosol | QD5 | 10, 50, 150 | 54 | 1 (plasma, lung, liver, spleen, ELF) | 3 | [5,6] |
| Spectinamide 1599 | BALB/c mice | Healthy | Intrapulmonary Aerosol | BIW | 10, 50, 150 | 54 | 1 (plasma, lung, liver, spleen, ELF) | 3 | [5,6] |
| Spectinamide 1599 | BALB/c mice | Healthy | Intrapulmonary Aerosol | TIW | 10, 50, 150 | 54 | 1 (plasma, lung, liver, spleen, ELF) | 3 | [5,6] |
| Spectinamide 1599 | Sprague-Dawley rats | Healthy | Intravenous | Single Dose | 10 | 5 males/6 females | 13 (plasma) | 11 | [4] |
| Spectinamide 1599 | Sprague-Dawley rats | Healthy | Intravenous | Single Dose | 10 | 4 males/4 females | 1 (plasma, lung, liver, spleen) | 4 | Generated as described under Methods |
| Spectinamide 1810 | BALB/c mice | Healthy | Intravenous | Single Dose | 10 | 24 | 1 (plasma, lung, liver, spleen) | 3 | [7,13,14] |
| Spectinamide 1810 | BALB/c mice | Healthy | Intravenous | QD5 | 10 | 24 | 1 (plasma, lung, liver, spleen) | 3 | [7,13,14] |
| Spectinamide 1810 | BALB/c mice | Healthy | Subcutaneous | Single Dose | 46 | 21 | 1 (plasma) | 3 | [7,13,14] |
| Spectinamide 1810 | BALB/c mice | Healthy | Subcutaneous | Single Dose | 50, 200 | 48 | 1 (plasma) | 3 | [7,13,14] |
| Spectinamide 1810 | BALB/c mice | Healthy | Subcutaneous | QD5 | 50, 200 | 36 | 1 (plasma) | 3 | [7,13,14] |
| Spectinamide 1810 | BALB/c mice | Infected | Subcutaneous - Study 2A | Twice daily (QD5 for 4 weeks) | 10, 20, 50, 100, 200, 300, 500 | 35 | 2 (plasma) | 5 | [7,13,14] |
| Spectinamide 1810 | BALB/c mice | Infected | Subcutaneous - Study 2A | Once daily (QD5 for 4 weeks) | 20, 40, 100, 200, 400 | 25 | 2 (plasma) | 5 | [7,13,14] |
| Spectinamide 1810 | BALB/c mice | Infected | Subcutaneous - Study 2A | TIW for 4 weeks | 20, 40, 100, 200, 400 | 25 | 2 (plasma) | 5 | [7,13,14] |
| Spectinamide 1810 | BALB/c mice | Infected | Subcutaneous - Study 2A | BIW for 4 weeks | 20, 40, 100, 200 | 20 | 2 (plasma) | 5 | [7,13,14] |
| Spectinamide 1810 | BALB/c mice | Infected | Subcutaneous - Study 2A | Once every week for 4 weeks | 20, 40, 100 | 15 | 2 (plasma) | 5 | [7,13,14] |
| Spectinamide 1810 | BALB/c mice | Infected | Subcutaneous - Study 2B | Twice daily (QD5 for 4 weeks) | 50, 200 | 12 | 2 (plasma) | 6 | [7,13,14] |
| Spectinamide 1810 | BALB/c mice | Infected | Subcutaneous - Study 2B | Once daily (QD5 for 4 weeks) | 100 | 6 | 2 (plasma) | 6 | [7,13,14] |
| Spectinamide 1810 | BALB/c mice | Infected | Subcutaneous - Study 2B | TIW for 4 weeks | 166, 333 | 12 | 2 (plasma) | 6 | [7,13,14] |
| Spectinamide 1810 | Sprague-Dawley rats | Healthy | Intravenous | Single Dose | 10 | 18 males | 13 (plasma) | 18 | Generated in this study as described under Methods |
| Parameters | Values | Reference | |
|---|---|---|---|
| Mouse (20 g) | Rat (225 g) | ||
| QLung (L/h) | 0.618 | 4.83 | [16] |
| QSpleen (L/h) | 0.00695 | 0.0412 | [16] |
| QLiver (L/h) | 0.139 | 0.901 | [16] |
| QKidney (L/h) | 0.100 | 0.601 | [16] |
| QOther (L/h) | 0.371 | 3.29 | [16] |
| GFR (L/h) | 0.0168 | 0.088 | [16] |
| VVenous blood (L) | 0.00120 | 0.0115 | [17] |
| VArterial blood (L) | 0.000515 | 0.00494 | [17] |
| VLung (L) | 0.000194 | 0.00140 | [17] |
| VSpleen (L) | 0.000127 | 0.00277 | [17] |
| VLiver (L) | 0.00193 | 0.0157 | [17] |
| VKidney (L) | 0.000525 | 0.00241 | [17] |
| VOther (L) | 0.0235 | 0.245 | [17] |
| VELF (L) | 0.0000100 | 0.000100 | [18] |
| Spectinamide 1599 k(b/p) | 0.552 | 0.812 | Generated in this study as described under Methods |
| Spectinamide 1599 fuPlasma | 0.602 | 0.563 | |
| Spectinamide 1599 fuELF | 0.948 | 0.940 | |
| Spectinamide 1810 k(b/p) | 0.604 | 0.785 | |
| Spectinamide 1810 fuPlasma | 0.693 | 0.607 | |
| Spectinamide 1810 fuELF | 0.965 | 0.950 | |
| Tissues | Fraction Vascular | Fraction Interstitial | Fraction Cellular |
|---|---|---|---|
| Lung | 0.26 | 0.19 | 0.55 |
| Spleen | 0.22 | 0.20 | 0.58 |
| Liver | 0.15 | 0.20 | 0.64 |
| Kidney | 0.10 | 0.15 | 0.75 |
| Other | 0.040 | 0.19 | 0.77 |
| Parameters | Description | Units | Intravenous Estimate (%RSE) | Intratracheal Estimate (%RSE) | Subcutaneous Estimate (%RSE) |
|---|---|---|---|---|---|
| 1st order uptake from the rapid equilibrium sub compartment (V+I) to the cellular sub compartment of the lung | 1/h | 0.068 (15.3) | Fixed | Fixed | |
| 1st order back flux from the cellular sub compartment to the rapid equilibrium sub compartment of the lung | 1/h | 0.028 (41.5) | Fixed | Fixed | |
| 1st order uptake from the rapid equilibrium sub compartment (V+I) to the cellular sub compartment of the liver | 1/h | 0.87 (10.1) | Fixed | Fixed | |
| 1st order back flux from the cellular sub compartment to the rapid equilibrium sub compartment of the liver | 1/h | 0.061 (13.7) | Fixed | Fixed | |
| 1st order uptake from the rapid equilibrium sub compartment (V+I) to the cellular sub compartment of the spleen | 1/h | 0.048 (16.5) | Fixed | Fixed | |
| 1st order back flux from the cellular sub compartment to the rapid equilibrium sub compartment of the spleen | 1/h | 0.01 (106) | Fixed | Fixed | |
| 1st order uptake from the rapid equilibrium sub compartment (V+I) to the cellular sub compartment of the kidney | 1/h | 12.1 (19.7) | Fixed | Fixed | |
| 1st order back flux from the cellular sub compartment to the rapid equilibrium sub compartment of the kidney | 1/h | 0.15 (31.0) | Fixed | Fixed | |
| 1st order uptake from the rapid equilibrium sub compartment (V+I) to the cellular sub compartment of the other tissues | 1/h | 5.4 (4.92) | Fixed | Fixed | |
| 1st order back flux from the cellular sub compartment to the rapid equilibrium sub compartment of the other tissues | 1/h | 7.0 × 10−5 (142) | Fixed | Fixed | |
| Ka | 1st order absorption rate constant | - | - | 5.03 (4.53) | 4.36 (7.86) |
| F | Bioavailability component | - | - | 0.33 (2.03) | 0.86 (6.15) |
| ω | estimated by simultaneously fitting the mouse and rat plasma and tissue data obtained after intravenous administration | 0.87 (30.6) | Fixed | Fixed | |
| ω | estimated by simultaneously fitting the mouse and rat plasma and tissue data obtained after intravenous administration | 0.61 (29.8) | Fixed | Fixed | |
| ω | estimated by simultaneously fitting the mouse and rat plasma and tissue data obtained after intravenous administration | 0.66 (41.0) | Fixed | Fixed | |
| ω | estimated by simultaneously fitting the mouse and rat plasma and tissue data obtained after intravenous administration | 0.48 (21.6) | Fixed | Fixed | |
| Proportional error for plasma concentration-time profile | 0.32 (15.1) | 6.57 (8.62) | 0.54 (17.6) | ||
| Proportional error for lung concentration-time profile | 0.35 (14.4) | 0.95 (9.92) | 0.50 (15.3) | ||
| Proportional error for liver concentration-time profile | 0.28 (14.4) | 2.55 (10.3) | 0.29 (19.1) | ||
| Proportional error for spleen concentration-time profile | 0.53 (14.4) | 8.48 (9.86) | 0.97 (16.5) |
| Study | AUCinf (h × µg/mL) | ||
|---|---|---|---|
| Observed | Median Predicted | Fold Difference | |
| IV SD 10 mg/kg | 7.52 | 8.85 | 1.18 |
| IV QD5 10 mg/kg | 6.37 | 8.83 | 1.39 |
| SC SD 50 mg/kg | 40.4 | 39.8 | 1.02 |
| SC QD5 200 mg/kg | 227 | 159 | 1.43 |
| IPA SD 10 mg/kg | 5.51 | 4.87 | 1.13 |
| IPA QD5 10 mg/kg | 3.57 | 4.85 | 1.36 |
| IPA TIW 10 mg/kg | 5.36 | 4.83 | 1.11 |
| IPA SD 50 mg/kg | 23.2 | 24.4 | 1.05 |
| IPA QD5 50 mg/kg | 39.8 | 24.2 | 1.64 |
| IPA TIW 50 mg/kg | 24.3 | 24.2 | 1.00 |
| IPA BIW 50 mg/kg | 14.2 | 24.1 | 1.70 |
| IPA SD 150 mg/kg | 59.5 | 73.1 | 1.23 |
| IPA QD5 150 mg/kg | 96.9 | 72.7 | 1.33 |
| IPA TIW 150 mg/kg | 61.7 | 72.5 | 1.18 |
| IPA BIW 150 mg/kg | 108 | 72.4 | 1.49 |
| Rat IV SD 10 mg/kg | 19.8 | 12.5 | 1.58 |
| Study | AUCinf (h × µg/g) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Lung | Liver | Spleen | |||||||
| Observed | Predicted | Fold Difference | Observed | Predicted | Fold Difference | Observed | Predicted | Fold Difference | |
| IV SD 10 mg/kg | 3.79 | 6.24 | 1.65 | 19.9 | 16.6 | 1.2 | 3.42 | 5.02 | 1.47 |
| IV QD5 10 mg/kg | 4.05 | 5.62 | 1.39 | 19.6 | 12.4 | 1.58 | 3.91 | 5.62 | 1.44 |
| SC SD 50 mg/kg | 19.1 | 27 | 1.41 | 91.8 | 70.5 | 1.3 | 23.6 | 21.2 | 1.11 |
| SC QD5 200 mg/kg | 69.1 | 97.9 | 1.42 | 336 | 217 | 1.55 | 110 | 96.4 | 1.14 |
| Parameters | Description | Units | Intravenous Estimate (%RSE) | Subcutaneous Estimate (%RSE) |
|---|---|---|---|---|
| 1st order uptake from the rapid equilibrium sub compartment (V+I) to the cellular sub compartment of the lung | 1/h | 0.13 (16.0) | Fixed | |
| 1st order back flux from the cellular sub compartment to the rapid equilibrium sub compartment of the lung | 1/h | 0.076 (17.6) | Fixed | |
| 1st order uptake from the rapid equilibrium sub compartment (V+I) to the cellular sub compartment of the liver | 1/h | 1.19 (12.0) | Fixed | |
| 1st order back flux from the cellular sub compartment to the rapid equilibrium sub compartment of the liver | 1/h | 0.051 (17.2) | Fixed | |
| 1st order uptake from the rapid equilibrium sub compartment (V+I) to the cellular sub compartment of the spleen | 1/h | 0.059 (23.1) | Fixed | |
| 1st order back flux from the cellular sub compartment to the rapid equilibrium sub compartment of the spleen | 1/h | 0.013 (120) | Fixed | |
| 1st order uptake from the rapid equilibrium sub compartment (V+I) to the cellular sub compartment of the kidney | 1/h | 3.94 (43.9) | Fixed | |
| 1st order back flux from the cellular sub compartment to the rapid equilibrium sub compartment of the kidney | 1/h | 0.097 (45.1) | Fixed | |
| 1st order uptake from the rapid equilibrium sub compartment (V+I) to the cellular sub compartment of the other tissues | 1/h | 4.77 (7.88) | Fixed | |
| 1st order back flux from the cellular sub compartment to the rapid equilibrium sub compartment of the other tissues | 1/h | 7.0 × 10−5 (0.00278) | Fixed | |
| Ka | 1st order absorption rate constant | - | - | 8.26 (14.5) |
| F | Bioavailability component | - | - | 1.00 (0.463) |
| ω | Inter-animal variability on estimated by simultaneously fitting the mouse and rat plasma and tissue data obtained after intravenous administration | 0.31 (14.7) | Fixed | |
| Proportional error for plasma concentration-time profile | 0.43 (14.7) | 0.36 (15.6) | ||
| Proportional error for lung concentration-time profile | 0.13 (16.0) | 0.30 (14.7) | ||
| Proportional error for liver concentration-time profile | 0.076 (17.6) | 0.31 (14.7) | ||
| Proportional error for spleen concentration-time profile | 1.19 (12.0) | 0.43 (14.7) |
| Study | AUCinf (h × µg/mL) | ||
|---|---|---|---|
| Observed | Median Predicted | Fold Difference | |
| IV SD 10 mg/kg | 7.91 | 7.64 | 1.04 |
| IV QD5 10 mg/kg | 9.45 | 7.70 | 1.23 |
| SC SD 46 mg/kg | 38.6 | 36.8 | 1.05 |
| SC SD 50 mg/kg | 67.9 | 40.0 | 1.70 |
| SC SD 200 mg/kg | 267 | 160 | 1.67 |
| SC QD5 50 mg/kg | 65.5 | 40.3 | 1.63 |
| SC QD5 200 mg/kg | 265 | 161 | 1.65 |
| Rat IV SD 10 mg/kg | 20.8 | 12.9 | 1.61 |
| Study | AUCinf (h × µg/g) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Lung | Liver | Spleen | |||||||
| Observed | Predicted | Fold Difference | Observed | Predicted | Fold Difference | Observed | Predicted | Fold Difference | |
| IV SD 10 mg/kg | 5.75 | 8.53 | 1.48 | 31.6 | 25.2 | 1.25 | 4.29 | 4.43 | 1.03 |
| IV QD5 10 mg/kg | 11.2 | 9.79 | 1.14 | 51.2 | 37.4 | 1.37 | 9.45 | 7.91 | 1.19 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parmar, K.R.; Lukka, P.B.; Wagh, S.; Temrikar, Z.H.; Liu, J.; Lee, R.E.; Braunstein, M.; Hickey, A.J.; Robertson, G.T.; Gonzalez-Juarrero, M.; et al. Development of a Minimalistic Physiologically Based Pharmacokinetic (mPBPK) Model for the Preclinical Development of Spectinamide Antibiotics. Pharmaceutics 2023, 15, 1759. https://doi.org/10.3390/pharmaceutics15061759
Parmar KR, Lukka PB, Wagh S, Temrikar ZH, Liu J, Lee RE, Braunstein M, Hickey AJ, Robertson GT, Gonzalez-Juarrero M, et al. Development of a Minimalistic Physiologically Based Pharmacokinetic (mPBPK) Model for the Preclinical Development of Spectinamide Antibiotics. Pharmaceutics. 2023; 15(6):1759. https://doi.org/10.3390/pharmaceutics15061759
Chicago/Turabian StyleParmar, Keyur R., Pradeep B. Lukka, Santosh Wagh, Zaid H. Temrikar, Jiuyu Liu, Richard E. Lee, Miriam Braunstein, Anthony J. Hickey, Gregory T. Robertson, Mercedes Gonzalez-Juarrero, and et al. 2023. "Development of a Minimalistic Physiologically Based Pharmacokinetic (mPBPK) Model for the Preclinical Development of Spectinamide Antibiotics" Pharmaceutics 15, no. 6: 1759. https://doi.org/10.3390/pharmaceutics15061759