
Challenges in the Development and Application of Organ-on-Chips for Intranasal Drug Delivery Studies
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
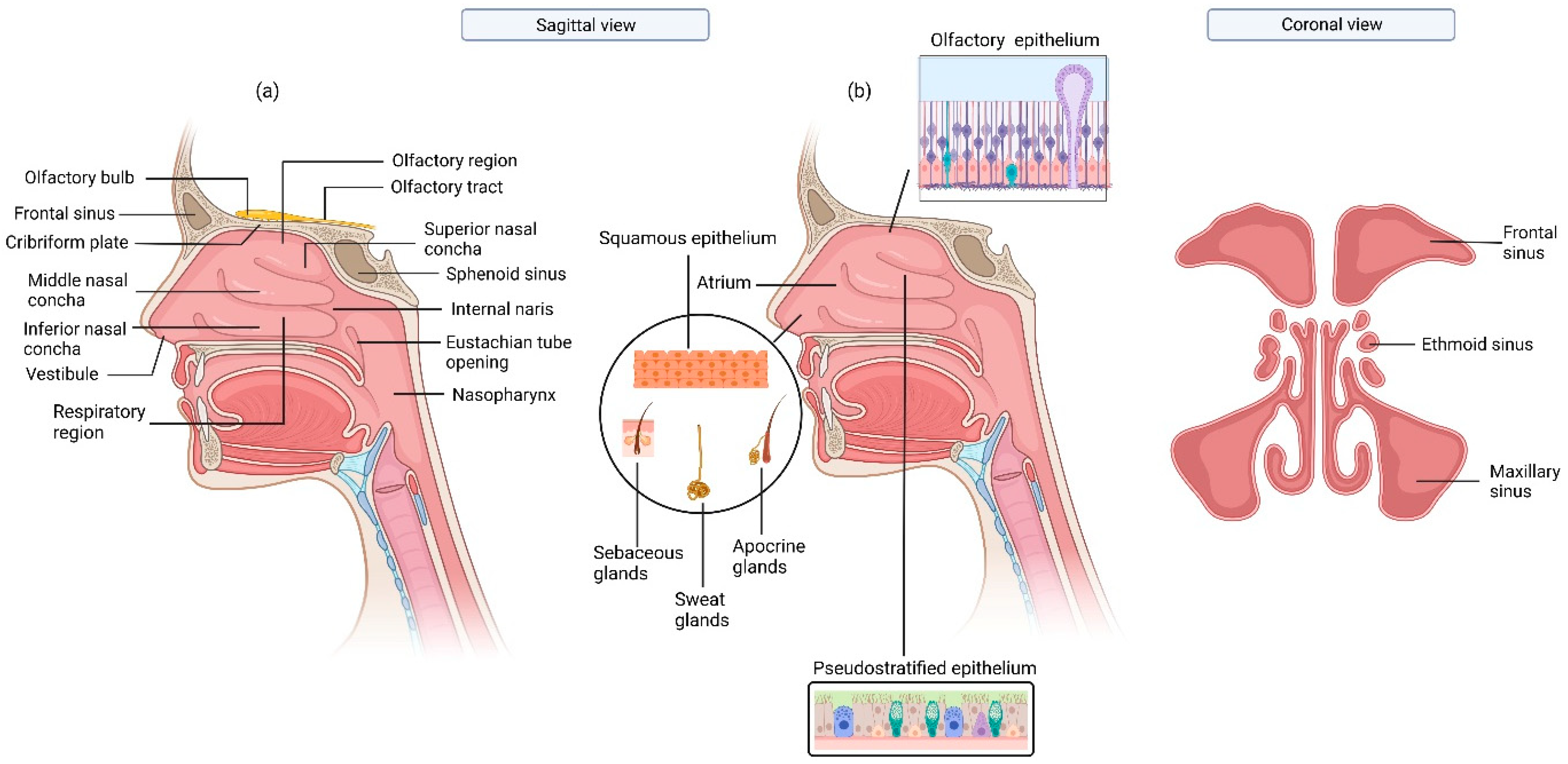
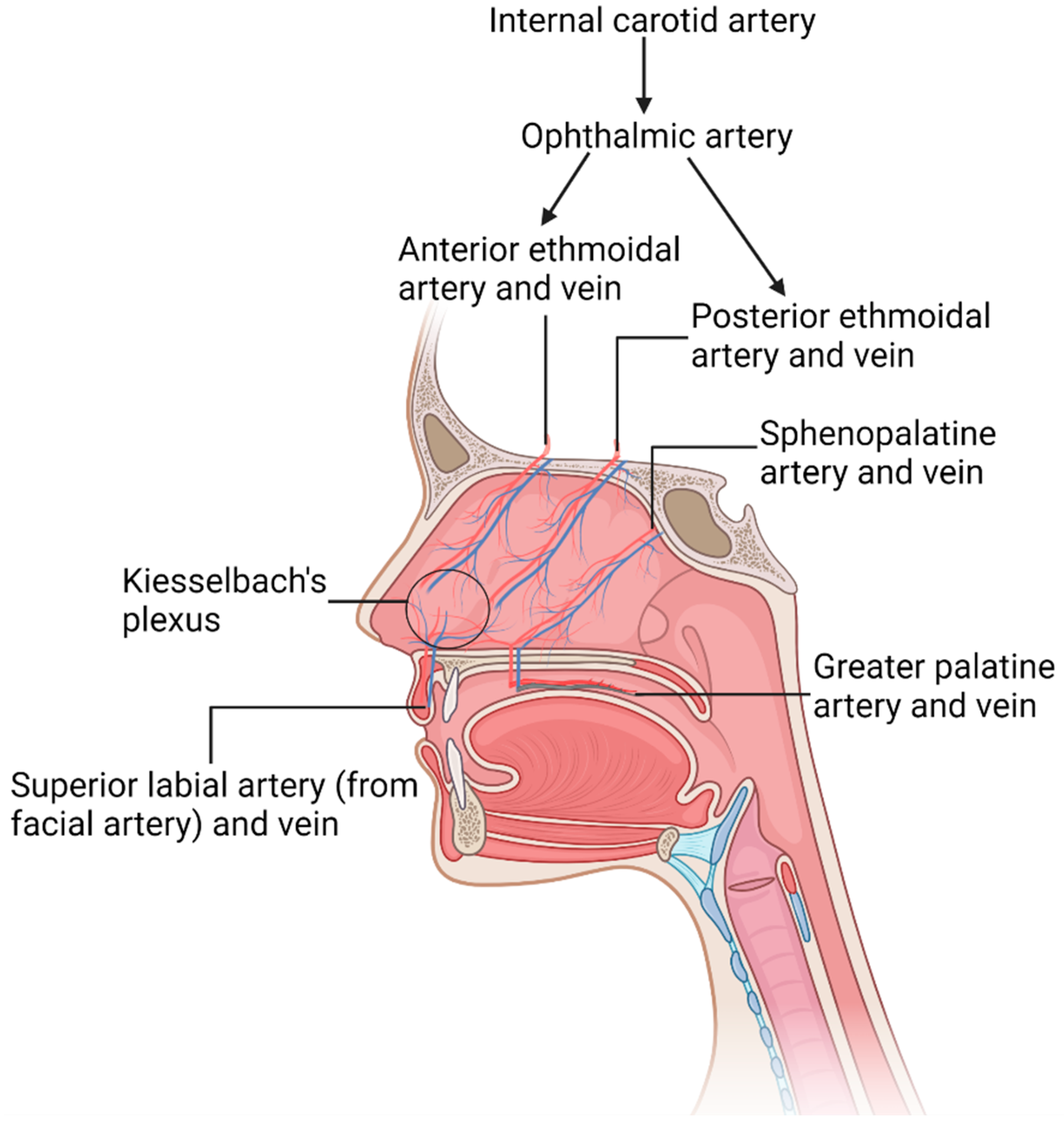
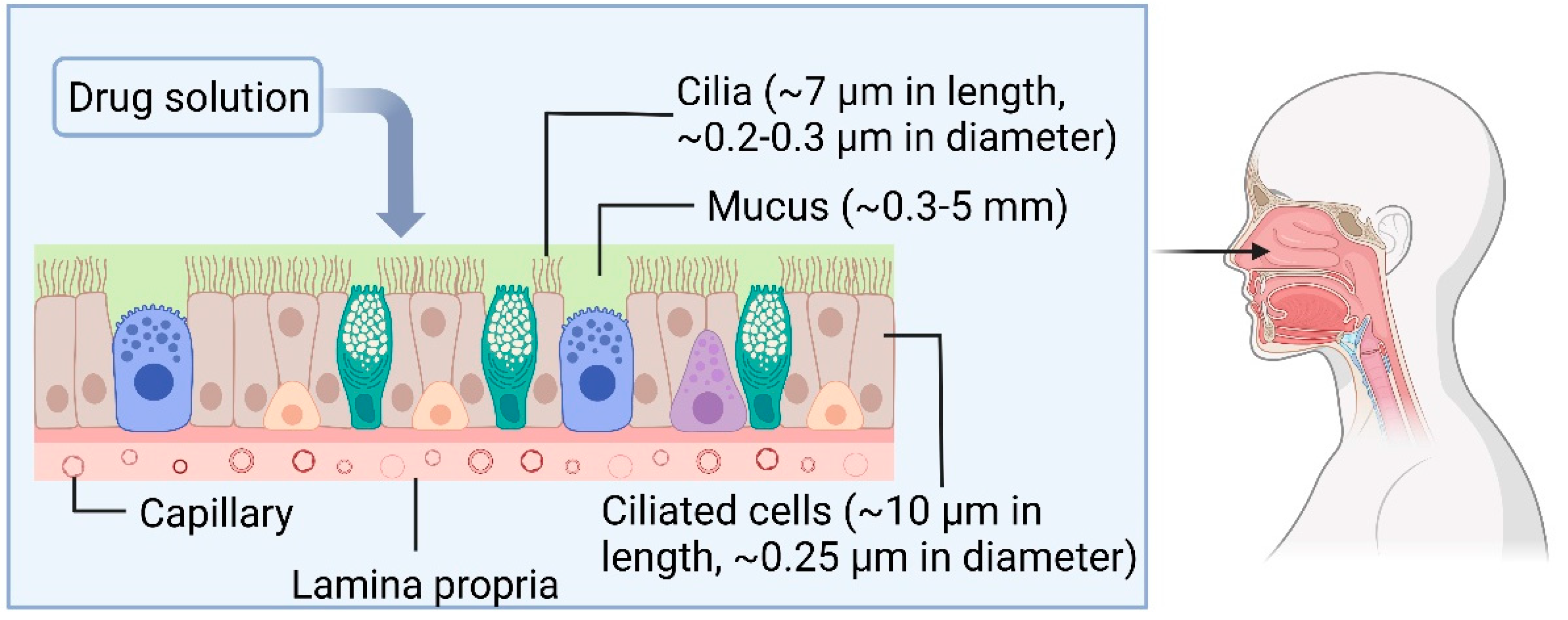
1.1. The Physiology of Nasal Cavity
1.2. IN Drug Delivery
1.3. The Potential Application of OoCs for Toxicological Studies on IN Drugs
1.3.1. The Systemic and CNS Side Effects of IN Drugs
1.3.2. The Pulmonary Toxic Effects of IN Drugs
1.3.3. The Local Side Effects of IN Drugs
2. Recent Technologies for In Vitro Studies on IN Drugs
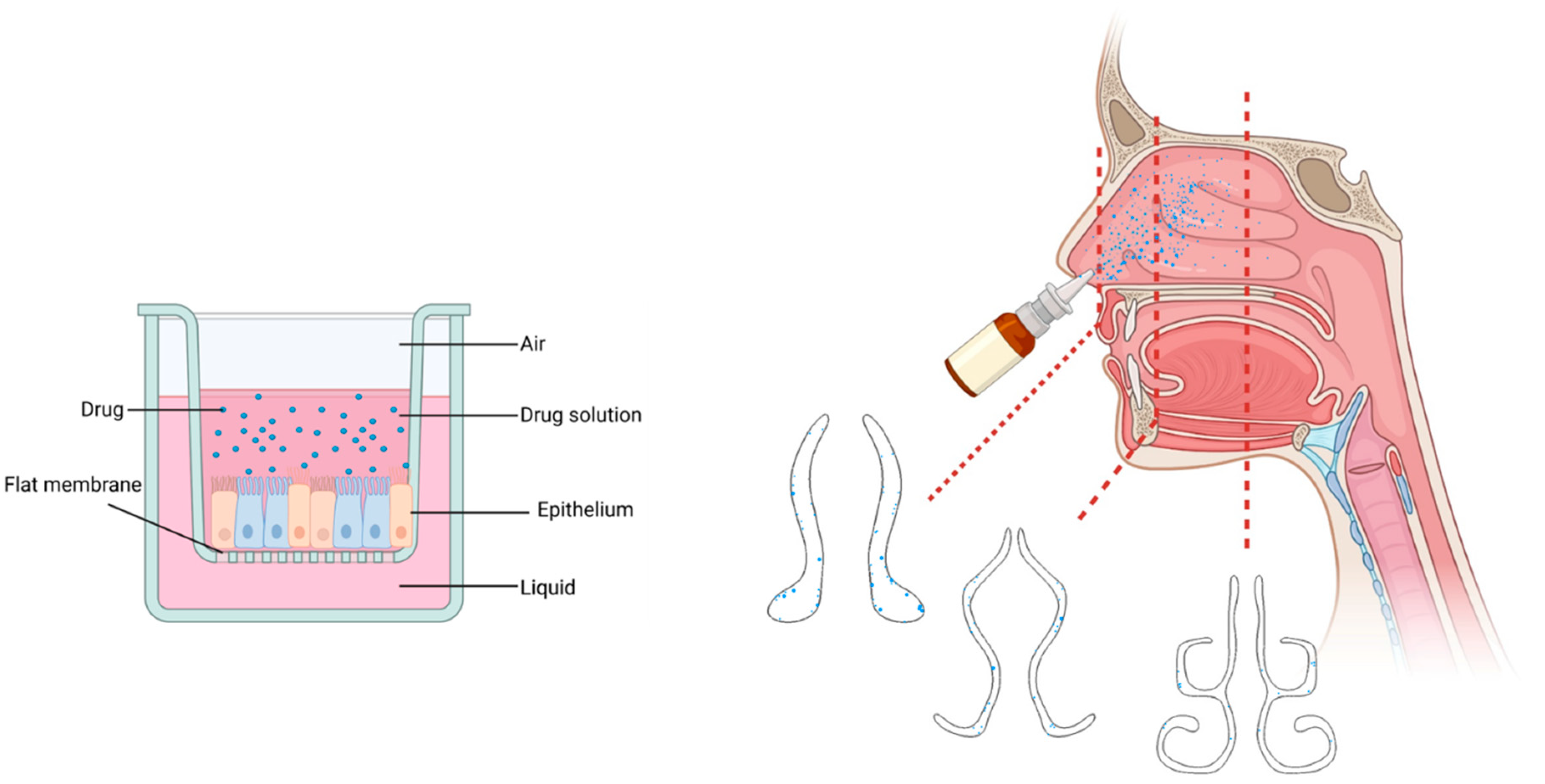
2.1. Physiologically Relevant 3D Models of Human Nasal Cavity
2.2. Microfluidic OoC Models of the Nasal Mucosa
2.3. Challenges with Studying in Drugs Toxicity by OoC Models
2.3.1. Mimicking the Cellular Architecture and Tissue–Tissue Crosstalk
2.3.2. Mimicking Complex Geometry of Nasal Cavity
2.3.3. Evaluation of IN Drugs’ Side Effects by OoCs
Hepatotoxicity Assessments
Nephrotoxicity Assessments
2.3.4. Fabrication and Operation of OoCs
3. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fortuna, A.; Alves, G.; Serralheiro, A.; Sousa, J.; Falcão, A. Intranasal delivery of systemic-acting drugs: Small-molecules and biomacromolecules. Eur. J. Pharm. Biopharm. 2014, 88, 8–27. [Google Scholar] [CrossRef] [PubMed]
- Bors, L.A.; Erdő, F. Overcoming the blood–brain barrier. challenges and tricks for CNS drug delivery. Sci. Pharm. 2019, 87, 6. [Google Scholar] [CrossRef]
- Grassin-Delyle, S.; Buenestado, A.; Naline, E.; Faisy, C.; Blouquit-Laye, S.; Couderc, L.-J.; Le Guen, M.; Fischler, M.; Devillier, P. Intranasal drug delivery: An efficient and non-invasive route for systemic administration: Focus on opioids. Pharmacol. Ther. 2012, 134, 366–379. [Google Scholar] [CrossRef] [PubMed]
- Keller, L.-A.; Merkel, O.; Popp, A. Intranasal drug delivery: Opportunities and toxicologic challenges during drug development. Drug Deliv. Transl. Res. 2021, 12, 735–757. [Google Scholar] [CrossRef]
- Ingber, D.E. Human organs-on-chips for disease modelling, drug development and personalized medicine. Nat. Rev. Genet. 2022, 23, 467–491. [Google Scholar] [CrossRef]
- Gholizadeh, H.; Cheng, S.; Kourmatzis, A.; Xing, H.; Traini, D.; Young, P.M.; Ong, H.X. Application of Micro-Engineered Kidney, Liver, and Respiratory System Models to Accelerate Preclinical Drug Testing and Development. Bioengineering 2022, 9, 150. [Google Scholar] [CrossRef]
- Sung, J.H.; Wang, Y.I.; Narasimhan Sriram, N.; Jackson, M.; Long, C.; Hickman, J.J.; Shuler, M.L. Recent advances in body-on-a-chip systems. Anal. Chem. 2018, 91, 330–351. [Google Scholar] [CrossRef]
- Ma, C.-J. Experimental Verification of the Particle Blocking Feature of Nasal Hair. Asian J. Atmos. Environ. 2019, 13, 99–105. [Google Scholar] [CrossRef]
- Sobiesk, J.L.; Munakomi, S. Anatomy, Head and Neck, Nasal Cavity; StatPearls: Treasure Island, FL, USA, 2019. [Google Scholar]
- Mygind, N.; Dahl, R. Anatomy, physiology and function of the nasal cavities in health and disease. Adv. Drug Deliv. Rev. 1998, 29, 3–12. [Google Scholar] [CrossRef]
- Widdicombe, J. Microvascular anatomy of the nose. Allergy 1997, 52, 7–11. [Google Scholar] [CrossRef]
- Batson, O.V. XLV The Venous Networks of the Nasal Mucosa. Ann. Otol. Rhinol. Laryngol. 1954, 63, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-G. Surgical Anatomy of the Nose: Update. Nihon Bika Gakkai Kaishi (Jpn. J. Rhinol.) 2005, 44, 29–30. [Google Scholar] [CrossRef]
- Hagan, W.E.; Walker, L.B. The nasolabial musculocutaneous flap: Clinical and anatomical correlations. Laryngoscope 1988, 98, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Mangalgiri, A.; Namdev, L.N.; Mahore, D.; Kapre, M. The study of higher origin of facial artery and its surgical significance. Indian J. Otolaryngol. Head Neck Surg. 2015, 67, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Cauna, N.; Hinderer, K.H. LXXVI Fine Structure of Blood Vessels of the Human Nasal Respiratory Mucosa. Ann. Otol. Rhinol. Laryngol. 1969, 78, 865–879. [Google Scholar] [CrossRef]
- Saunders, M.; Jones, N.; Kabala, J.; Lowe, J. An anatomical, histological and magnetic resonance imaging study of the nasal septum. Clin. Otolaryngol. Allied Sci. 1995, 20, 434–438. [Google Scholar] [CrossRef]
- Boegh, M.; Nielsen, H.M. Mucus as a barrier to drug delivery–understanding and mimicking the barrier properties. Basic Clin. Pharmacol. Toxicol. 2015, 116, 179–186. [Google Scholar] [CrossRef]
- Helwany, M.; Bordoni, B. Neuroanatomy, Cranial Nerve 1 (Olfactory); StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Battaglia, L.; Panciani, P.P.; Muntoni, E.; Capucchio, M.T.; Biasibetti, E.; De Bonis, P.; Mioletti, S.; Fontanella, M.; Swaminathan, S. Lipid nanoparticles for intranasal administration: Application to nose-to-brain delivery. Expert Opin. Drug Deliv. 2018, 15, 369–378. [Google Scholar] [CrossRef]
- Sleigh, M.A.; Blake, J.R.; Liron, N. The propulsion of mucus by cilia. Am. Rev. Respir. Dis. 1988, 137, 726–741. [Google Scholar] [CrossRef]
- Lorenzi, G.; Böhm, G.; Guimarães, E.; Vaz, C.; King, M.; Saldiva, P.H.N. Correlation between rheologic properties and in vitro ciliary transport of rat nasal mucus. Biorheology 1992, 29, 433–440. [Google Scholar] [CrossRef]
- England, R.; Homer, J.; Knight, L.; Ell, S. Nasal pH measurement: A reliable and repeatable parameter. Clin. Otolaryngol. Allied Sci. 1999, 24, 67–68. [Google Scholar] [CrossRef] [PubMed]
- Sigurdsson, H.H.; Kirch, J.; Lehr, C.-M. Mucus as a barrier to lipophilic drugs. Int. J. Pharm. 2013, 453, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Ballenger, J.J. Some effects of the respired environment on the nose. Laryngoscope 1981, 91, 1622–1628. [Google Scholar] [CrossRef] [PubMed]
- Proctor, D.F.; Andersen, I.; Lundqvist, G. Human nasal mucosal function at controlled temperatures. Respir. Physiol. 1977, 30, 109–124. [Google Scholar] [CrossRef] [PubMed]
- Soyka, M.B.; Wawrzyniak, P.; Eiwegger, T.; Holzmann, D.; Treis, A.; Wanke, K.; Kast, J.I.; Akdis, C.A. Defective epithelial barrier in chronic rhinosinusitis: The regulation of tight junctions by IFN-γ and IL-4. J. Allergy Clin. Immunol. 2012, 130, 1087–1096.e10. [Google Scholar] [CrossRef] [PubMed]
- Macchi, A.; Terranova, P.; Castelnuovo, P. Recurrent acute rhinosinusitis: A single blind clinical study of N-acetylcysteine vs ambroxol associated to corticosteroid therapy. Int. J. Immunopathol. Pharmacol. 2012, 25, 207–217. [Google Scholar] [CrossRef]
- Rhee, C.-S.; Majima, Y.; Cho, J.-S.; Arima, S.; Min, Y.-G.; Sakakura, Y. Effects of mucokinetic drugs on rheological properties of reconstituted human nasal mucus. Arch. Otolaryngol. Head Neck Surg. 1999, 125, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, H.; Murti Vemuri, N. Chapter 32—Chemical and Physicochemical Approaches to Solve Formulation Problems. In The Practice of Medicinal Chemistry, 4th ed.; Wermuth, C.G., Aldous, D., Raboisson, P., Rognan, D., Eds.; Academic Press: San Diego, CA, USA, 2015; pp. 767–791. [Google Scholar] [CrossRef]
- Bhise, S.B.; Yadav, A.V.; Avachat, A.M.; Malayandi, R. Bioavailability of intranasal drug delivery system. Asian J. Pharm. 2008, 2. [Google Scholar] [CrossRef]
- Snape, T.J.; Astles, A.M.; Davies, J. Understanding the chemical basis of drug stability and degradation. Pharm. J. 2010, 285, 416–417. [Google Scholar]
- Hickey, A.J.; Garmise, R.J. Dry powder nasal vaccines as an alternative to needle-based delivery. Crit. Rev. Ther. Drug Carrier Syst. 2009, 26, 1–27. [Google Scholar] [CrossRef]
- Trows, S.; Scherließ, R. Carrier-based dry powder formulation for nasal delivery of vaccines utilizing BSA as model drug. Powder Technol. 2016, 292, 223–231. [Google Scholar] [CrossRef]
- Alobid, I.; Benitez, P.; Cardelús, S.; de Borja Callejas, F.; Lehrer-Coriat, E.; Pujols, L.; Picado, C.; Mullol, J. Oral plus nasal corticosteroids improve smell, nasal congestion, and inflammation in sino-nasal polyposis. Laryngoscope 2014, 124, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Pires, A.; Fortuna, A.; Alves, G.; Falcão, A. Intranasal drug delivery: How, why and what for? J. Pharm. Pharm. Sci. 2009, 12, 288–311. [Google Scholar] [CrossRef] [PubMed]
- Salib, R.J.; Howarth, P.H. Safety and tolerability profiles of intranasal antihistamines and intranasal corticosteroids in the treatment of allergic rhinitis. Drug Saf. 2003, 26, 863–893. [Google Scholar] [CrossRef]
- Costantino, H.R.; Illum, L.; Brandt, G.; Johnson, P.H.; Quay, S.C. Intranasal delivery: Physicochemical and therapeutic aspects. Int. J. Pharm. 2007, 337, 1–24. [Google Scholar] [CrossRef]
- Sachan, N.; Bahadur, S.; Sharma, P.K. Recent advances and novel approaches for nose to brain drug delivery for treatment of migraine. Drug Deliv. Lett. 2019, 9, 182–198. [Google Scholar] [CrossRef]
- Graustella, A.J.; MacLeod, C. A critical review of the influence of oxytocin nasal spray on social cognition in humans: Evidence and future directions. Horm. Behav. 2012, 61, 410–418. [Google Scholar] [CrossRef]
- Kapoor, M.; Cloyd, J.C.; Siegel, R.A. A review of intranasal formulations for the treatment of seizure emergencies. J. Control. Release 2016, 237, 147–159. [Google Scholar] [CrossRef]
- Illum, L.; Watts, P.; Fisher, A.; Hinchcliffe, M.; Norbury, H.; Jabbal-Gill, I.; Nankervis, R.; Davis, S. Intranasal delivery of morphine. J. Pharmacol. Exp. Ther. 2002, 301, 391–400. [Google Scholar] [CrossRef]
- Fitzgibbon, D.; Morgan, D.; Dockter, D.; Barry, C.; Kharasch, E.D. Initial pharmacokinetic, safety and efficacy evaluation of nasal morphine gluconate for breakthrough pain in cancer patients. Pain 2003, 106, 309–315. [Google Scholar] [CrossRef]
- Behl, C.; Pimplaskar, H.; Sileno, A.; Demeireles, J.; Romeo, V. Effects of physicochemical properties and other factors on systemic nasal drug delivery. Adv. Drug Deliv. Rev. 1998, 29, 89–116. [Google Scholar] [CrossRef] [PubMed]
- Zihni, C.; Mills, C.; Matter, K.; Balda, M.S. Tight junctions: From simple barriers to multifunctional molecular gates. Nat. Rev. Mol. Cell Biol. 2016, 17, 564–580. [Google Scholar] [CrossRef] [PubMed]
- Rogers, G.A.; Beste, K.D.; Parkos, C.A.; Nusrat, A.; DelGaudio, J.M.; Wise, S.K. (Eds.) Epithelial tight junction alterations in nasal polyposis. In International Forum of Allergy & Rhinology; Wiley Online Library: Hoboken, NJ, USA, 2011. [Google Scholar]
- Yasuda, M.; Niisato, N.; Miyazaki, H.; Hama, T.; Dejima, K.; Hisa, Y.; Marunaka, Y. Epithelial ion transport of human nasal polyp and paranasal sinus mucosa. Am. J. Respir. Cell Mol. Biol. 2007, 36, 466–472. [Google Scholar] [CrossRef]
- Yasuda, M.; Niisato, N.; Miyazaki, H.; Iwasaki, Y.; Hama, T.; Dejima, K.; Hisa, Y.; Marunaka, Y. Epithelial Na+ channel and ion transport in human nasal polyp and paranasal sinus mucosa. Biochem. Biophys. Res. Commun. 2007, 362, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Steelant, B.; Farré, R.; Wawrzyniak, P.; Belmans, J.; Dekimpe, E.; Vanheel, H.; Van Gerven, L.; Krohn, I.K.; Bullens, D.M.; Ceuppens, J.L. Impaired barrier function in patients with house dust mite–induced allergic rhinitis is accompanied by decreased occludin and zonula occludens-1 expression. J. Allergy Clin. Immunol. 2016, 137, 1043–1053.e5. [Google Scholar] [CrossRef]
- Zhou, S.; Huang, H.; Chen, Q.; Tan, K.S.; Zhu, Z.; Peng, Y.; Ong, H.H.; Liu, J.; Xu, M.; Gao, J. Long-term defects of nasal epithelium barrier functions in patients with nasopharyngeal carcinoma post chemo-radiotherapy. Radiother. Oncol. 2020, 148, 116–125. [Google Scholar] [CrossRef]
- Tatsuta, M.; Kan-o, K.; Ishii, Y.; Yamamoto, N.; Ogawa, T.; Fukuyama, S.; Ogawa, A.; Fujita, A.; Nakanishi, Y.; Matsumoto, K. Effects of cigarette smoke on barrier function and tight junction proteins in the bronchial epithelium: Protective role of cathelicidin LL-37. Respir. Res. 2019, 20, 251. [Google Scholar] [CrossRef]
- Illum, L. Transport of drugs from the nasal cavity to the central nervous system. Eur. J. Pharm. Sci. 2000, 11, 1–18. [Google Scholar] [CrossRef]
- Fouad, S.A.; Shamma, R.N.; Basalious, E.B.; El-Nabarawi, M.A.; Tayel, S.A. Novel instantly-soluble transmucosal matrix (ISTM) using dual mechanism solubilizer for sublingual and nasal delivery of dapoxetine hydrochloride: In-vitro/in-vivo evaluation. Int. J. Pharm. 2016, 505, 212–222. [Google Scholar] [CrossRef]
- Wen, Z.; Yan, Z.; Hu, K.; Pang, Z.; Cheng, X.; Guo, L.; Zhang, Q.; Jiang, X.; Fang, L.; Lai, R. Odorranalectin-conjugated nanoparticles: Preparation, brain delivery and pharmacodynamic study on Parkinson’s disease following intranasal administration. J. Control. Release 2011, 151, 131–138. [Google Scholar] [CrossRef]
- Mischley, L.K.; Lau, R.C.; Shankland, E.G.; Wilbur, T.K.; Padowski, J.M. Phase IIb Study of Intranasal Glutathione in Parkinson’s Disease. J. Park. Dis. 2017, 7, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Gartziandia, O.; Herrán, E.; Ruiz-Ortega, J.; Miguelez, C.; Igartua, M.; Lafuente, J.; Pedraz, J.; Ugedo, L.; Hernández, R. Intranasal administration of chitosan-coated nanostructured lipid carriers loaded with GDNF improves behavioral and histological recovery in a partial lesion model of Parkinson’s disease. J. Biomed. Nanotechnol. 2016, 12, 2220–2280. [Google Scholar] [CrossRef] [PubMed]
- Novak, P.; Pimentel Maldonado, D.A.; Novak, V. Safety and preliminary efficacy of intranasal insulin for cognitive impairment in Parkinson disease and multiple system atrophy: A double-blinded placebo-controlled pilot study. PLoS ONE 2019, 14, e0214364. [Google Scholar] [CrossRef]
- Claxton, A.; Baker, L.D.; Hanson, A.; Trittschuh, E.H.; Cholerton, B.; Morgan, A.; Callaghan, M.; Arbuckle, M.; Behl, C.; Craft, S. Long-Acting Intranasal Insulin Detemir Improves Cognition for Adults with Mild Cognitive Impairment or Early-Stage Alzheimer’s Disease Dementia. J. Alzheimer’s Dis. 2015, 44, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Craft, S.; Baker, L.D.; Montine, T.J.; Minoshima, S.; Watson, G.S.; Claxton, A.; Arbuckle, M.; Callaghan, M.; Tsai, E.; Plymate, S.R. Intranasal insulin therapy for Alzheimer disease and amnestic mild cognitive impairment: A pilot clinical trial. Arch. Neurol. 2012, 69, 29–38. [Google Scholar] [CrossRef]
- Shehata, M.K.; Ismail, A.A.; Kamel, M.A. Nose to Brain Delivery of Astaxanthin–Loaded Nanostructured Lipid Carriers in Rat Model of Alzheimer’s Disease: Preparation, in vitro and in vivo Evaluation. Int. J. Nanomed. 2023, 18, 1631–1658. [Google Scholar] [CrossRef]
- Pedersen, C.A.; Gibson, C.M.; Rau, S.W.; Salimi, K.; Smedley, K.L.; Casey, R.L.; Leserman, J.; Jarskog, L.F.; Penn, D.L. Intranasal oxytocin reduces psychotic symptoms and improves Theory of Mind and social perception in schizophrenia. Schizophr. Res. 2011, 132, 50–53. [Google Scholar] [CrossRef]
- Cacciotti-Saija, C.; Langdon, R.; Ward, P.B.; Hickie, I.B.; Scott, E.M.; Naismith, S.L.; Moore, L.; Alvares, G.A.; Redoblado Hodge, M.A.; Guastella, A.J. A Double-Blind Randomized Controlled Trial of Oxytocin Nasal Spray and Social Cognition Training for Young People With Early Psychosis. Schizophr. Bull. 2014, 41, 483–493. [Google Scholar] [CrossRef]
- Van Woensel, M.; Wauthoz, N.; Rosière, R.; Amighi, K.; Mathieu, V.; Lefranc, F.; Van Gool, S.W.; De Vleeschouwer, S. Formulations for intranasal delivery of pharmacological agents to combat brain disease: A new opportunity to tackle GBM? Cancers 2013, 5, 1020–1048. [Google Scholar] [CrossRef]
- Balyasnikova, I.V.; Prasol, M.S.; Ferguson, S.D.; Han, Y.; Ahmed, A.U.; Gutova, M.; Tobias, A.L.; Mustafi, D.; Rincón, E.; Zhang, L. Intranasal delivery of mesenchymal stem cells significantly extends survival of irradiated mice with experimental brain tumors. Mol. Ther. 2014, 22, 140–148. [Google Scholar] [CrossRef]
- Khan, A.R.; Liu, M.; Khan, M.W.; Zhai, G. Progress in brain targeting drug delivery system by nasal route. J. Control. Release 2017, 268, 364–389. [Google Scholar] [CrossRef]
- Hashizume, R.; Ozawa, T.; Gryaznov, S.M.; Bollen, A.W.; Lamborn, K.R.; Frey, W.H.; Deen, D.F. New therapeutic approach for brain tumors: Intranasal delivery of telomerase inhibitor GRN163. Neuro-Oncol. 2008, 10, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Shingaki, T.; Inoue, D.; Furubayashi, T.; Sakane, T.; Katsumi, H.; Yamamoto, A.; Yamashita, S. Transnasal delivery of methotrexate to brain tumors in rats: A new strategy for brain tumor chemotherapy. Mol. Pharm. 2010, 7, 1561–1568. [Google Scholar] [CrossRef]
- Da Fonseca, C.O.; Teixeira, R.M.; Ramina, R.; Kovaleski, G.; Silva, J.T.; Nagel, J.; Quirico-Santos, T. Case of advanced recurrent glioblastoma successfully treated with monoterpene perillyl alcohol by intranasal administration. J. Cancer Ther. 2011, 2, 16–21. [Google Scholar] [CrossRef]
- Chen, T.C.; Da Fonseca, C.O.; Schönthal, A.H. Intranasal perillyl alcohol for glioma therapy: Molecular mechanisms and clinical development. Int. J. Mol. Sci. 2018, 19, 3905. [Google Scholar] [CrossRef]
- Danielyan, L.; Schäfer, R.; von Ameln-Mayerhofer, A.; Buadze, M.; Geisler, J.; Klopfer, T.; Burkhardt, U.; Proksch, B.; Verleysdonk, S.; Ayturan, M. Intranasal delivery of cells to the brain. Eur. J. Cell Biol. 2009, 88, 315–324. [Google Scholar] [CrossRef]
- Li, G.; Bonamici, N.; Dey, M.; Lesniak, M.S.; Balyasnikova, I.V. Intranasal delivery of stem cell-based therapies for the treatment of brain malignancies. Expert Opin. Drug Deliv. 2018, 15, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Yu-Taeger, L.; Stricker-Shaver, J.; Arnold, K.; Bambynek-Dziuk, P.; Novati, A.; Singer, E.; Lourhmati, A.; Fabian, C.; Magg, J.; Riess, O. Intranasal administration of mesenchymal stem cells ameliorates the abnormal dopamine transmission system and inflammatory reaction in the R6/2 mouse model of Huntington disease. Cells 2019, 8, 595. [Google Scholar] [CrossRef] [PubMed]
- Ayala, Y.M.; Nguyen, A.D. RNA-Based Therapies for Neurodegenerative Diseases. Mo Med. 2021, 118, 340–345. [Google Scholar]
- Sugaya, K.; Vaidya, M. Stem cell therapies for neurodegenerative diseases. Exosomes Stem Cells MicroRNA Aging Cancer Age Relat. Disord. 2018, 7, 61–84. [Google Scholar]
- Ballios, B.G.; Cooke, M.J.; Donaldson, L.; Coles, B.L.; Morshead, C.M.; van der Kooy, D.; Shoichet, M.S. A hyaluronan-based injectable hydrogel improves the survival and integration of stem cell progeny following transplantation. Stem Cell Rep. 2015, 4, 1031–1045. [Google Scholar] [CrossRef]
- Abdollahzadeh Jamalabadi, M.Y.; Xi, J. Olfactory Drug Aerosol Delivery with Acoustic Radiation. Biomedicines 2022, 10, 1347. [Google Scholar] [CrossRef] [PubMed]
- Yarragudi, S.B.; Kumar, H.; Jain, R.; Tawhai, M.; Rizwan, S. Olfactory targeting of microparticles through inhalation and bi-directional airflow: Effect of particle size and nasal anatomy. J. Aerosol Med. Pulm. Drug Deliv. 2020, 33, 258–270. [Google Scholar] [CrossRef]
- Bourganis, V.; Kammona, O.; Alexopoulos, A.; Kiparissides, C. Recent advances in carrier mediated nose-to-brain delivery of pharmaceutics. Eur. J. Pharm. Biopharm. 2018, 128, 337–362. [Google Scholar] [CrossRef]
- Quadir, M.; Zia, H.; Needham, T.E. Toxicological implications of nasal formulations. Drug Deliv. 1999, 6, 227–242. [Google Scholar] [CrossRef]
- Ugwoke, M.I.; Agu, R.U.; Verbeke, N.; Kinget, R. Nasal mucoadhesive drug delivery: Background, applications, trends and future perspectives. Adv. Drug Deliv. Rev. 2005, 57, 1640–1665. [Google Scholar] [CrossRef]
- Jiao, J.; Zhang, L. Influence of intranasal drugs on human nasal mucociliary clearance and ciliary beat frequency. Allergy Asthma Immunol. Res. 2019, 11, 306–319. [Google Scholar] [CrossRef]
- Inactive Ingredient Search for Approved Drug Products: The US Food and Drug Administration. Available online: http://www.accessdata.fda.gov/scripts/cder/iig/index.cfm (accessed on 26 March 2023).
- Loewen, A.H.; Hudon, M.E.; Hill, M.D. Thunderclap headache and reversible segmental cerebral vasoconstriction associated with use of oxymetazoline nasal spray. CMAJ 2004, 171, 593–594. [Google Scholar] [CrossRef]
- Dokuyucu, R.; Gokce, H.; Sahan, M.; Sefil, F.; Tas, Z.A.; Tutuk, O.; Ozturk, A.; Tumer, C.; Cevik, C. Systemic side effects of locally used oxymetazoline. Int. J. Clin. Exp. Med. 2015, 8, 2674. [Google Scholar]
- Kumar, M.; Kakkar, V.; Mishra, A.K.; Chuttani, K.; Kaur, I.P. Intranasal delivery of streptomycin sulfate (STRS) loaded solid lipid nanoparticles to brain and blood. Int. J. Pharm. 2014, 461, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Kammoun, A.K.; Khedr, A.; Hegazy, M.A.; Almalki, A.J.; Hosny, K.M.; Abualsunun, W.A.; Murshid, S.S.; Bakhaidar, R.B. Formulation, optimization, and nephrotoxicity evaluation of an antifungal in situ nasal gel loaded with voriconazole-clove oil transferosomal nanoparticles. Drug Deliv. 2021, 28, 2229–2240. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Xiong, G.; Tsang, W.C.; Schätzlein, A.G.; Uchegbu, I.F. Nose-to-brain delivery. J. Pharmacol. Exp. Ther. 2019, 370, 593–601. [Google Scholar] [CrossRef]
- Mula, M. The safety and tolerability of intranasal midazolam in epilepsy. Expert Rev. Neurother. 2014, 14, 735–740. [Google Scholar] [CrossRef]
- Shringarpure, M.; Gharat, S.; Momin, M.; Omri, A. Management of epileptic disorders using nanotechnology-based strategies for nose-to-brain drug delivery. Expert Opin. Drug Deliv. 2021, 18, 169–185. [Google Scholar] [CrossRef]
- Tan, M.S.; Parekh, H.S.; Pandey, P.; Siskind, D.J.; Falconer, J.R. Nose-to-brain delivery of antipsychotics using nanotechnology: A review. Expert Opin. Drug Deliv. 2020, 17, 839–853. [Google Scholar] [CrossRef] [PubMed]
- Ansari, M.A.; Chung, I.-M.; Rajakumar, G.; Alzohairy, M.A.; Alomary, M.N.; Thiruvengadam, M.; Pottoo, F.H.; Ahmad, N. Current nanoparticle approaches in nose to brain drug delivery and anticancer therapy-a review. Curr. Pharm. Des. 2020, 26, 1128–1137. [Google Scholar] [CrossRef]
- Lee, D.; Minko, T. Nanotherapeutics for Nose-to-Brain Drug Delivery: An Approach to Bypass the Blood Brain Barrier. Pharmaceutics 2021, 13, 2049. [Google Scholar] [CrossRef] [PubMed]
- Borrajo, M.L.; Alonso, M.J. Using nanotechnology to deliver biomolecules from nose to brain—Peptides, proteins, monoclonal antibodies and RNA. Drug Deliv. Transl. Res. 2022, 12, 862–880. [Google Scholar] [CrossRef]
- Bioavailability and Bioequivalence Studies for Nasal Aerosols and Nasal Sprays for Local Action; The US Food and Drug Aministration: Silver Spring, MD, USA, 2003.
- Choi, H.-Y.; Lee, Y.-H.; Lim, C.-H.; Kim, Y.-S.; Lee, I.-S.; Jo, J.-M.; Lee, H.-Y.; Cha, H.-G.; Woo, H.J.; Seo, D.-S. Assessment of respiratory and systemic toxicity of Benzalkonium chloride following a 14-day inhalation study in rats. Part. Fibre Toxicol. 2020, 17, 5. [Google Scholar] [CrossRef]
- Swiercz, R.; Hałatek, T.; Wasowicz, W.; Kur, B.; Grzelińska, Z.; Majcherek, W. Pulmonary irritation after inhalation exposure to benzalkonium chloride in rats. Int. J. Occup. Med. Environ. Health 2008, 21, 157–163. [Google Scholar] [CrossRef]
- Schleimer, R.P.; Kato, A.; Kern, R.; Kuperman, D.; Avila, P.C. Epithelium: At the interface of innate and adaptive immune responses. J. Allergy Clin. Immunol. 2007, 120, 1279–1284. [Google Scholar] [CrossRef] [PubMed]
- Jiao, J.; Meng, N.; Zhang, L. The effect of topical corticosteroids, topical antihistamines, and preservatives on human ciliary beat frequency. ORL 2014, 76, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, M.A. Drug metabolism in the nasal mucosa. Pharm. Res. 1992, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Genter, M.B.; Apparaju, S.; Desai, P.B. Induction of olfactory mucosal and liver metabolism of lidocaine by 2, 3, 7, 8-tetrachlorodibenzo-p-dioxin. J. Biochem. Mol. Toxicol. 2002, 16, 128–134. [Google Scholar] [CrossRef]
- Longo, V.; Ingelman-Sundberg, M.; Amato, G.; Salvetti, A.; Gervasi, P.G. Effect of starvation and chlormethiazole on cytochrome P450s of rat nasal mucosa. Biochem. Pharmacol. 2000, 59, 1425–1432. [Google Scholar] [CrossRef] [PubMed]
- Åkerlund, A.; Arfors, K.-E.; Bende, M.; Intaglietta, M. Effect of oxymetazoline on nasal and sinus mucosal blood flow in the rabbit as measured with laser-Doppler flowmetry. Ann. Otol. Rhinol. Laryngol. 1993, 102, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Gholizadeh, H.; Cheng, S.; Pozzoli, M.; Messerotti, E.; Traini, D.; Young, P.; Kourmatzis, A.; Ong, H.X. Smart thermosensitive chitosan hydrogel for nasal delivery of ibuprofen to treat neurological disorders. Expert Opin. Drug Deliv. 2019, 16, 453–466. [Google Scholar] [CrossRef]
- Gholizadeh, H.; Messerotti, E.; Pozzoli, M.; Cheng, S.; Traini, D.; Young, P.; Kourmatzis, A.; Caramella, C.; Ong, H.X. Application of a thermosensitive in situ gel of chitosan-based nasal spray loaded with tranexamic acid for localised treatment of nasal wounds. AAPS PharmSciTech 2019, 20, 299. [Google Scholar] [CrossRef]
- Chen, J.Z.; Finlay, W.H.; Martin, A. In Vitro Regional Deposition of Nasal Sprays in an Idealized Nasal Inlet: Comparison with In Vivo Gamma Scintigraphy. Pharm. Res. 2022, 39, 3021–3028. [Google Scholar] [CrossRef]
- Gholizadeh, H.; Ong, H.X.; Bradbury, P.; Kourmatzis, A.; Traini, D.; Young, P.; Li, M.; Cheng, S. Real-time quantitative monitoring of in vitro nasal drug delivery by a nasal epithelial mucosa-on-a-chip model. Expert Opin. Drug Deliv. 2021, 18, 803–818. [Google Scholar] [CrossRef]
- Na, K.; Lee, M.; Shin, H.-W.; Chung, S. In vitro nasal mucosa gland-like structure formation on a chip. Lab Chip 2017, 17, 1578–1584. [Google Scholar] [CrossRef]
- Wang, W.; Yan, Y.; Li, C.W.; Xia, H.M.; Chao, S.S.; Wang, Z.P. Live human nasal epithelial cells (hNECs) on chip for in vitro testing of gaseous formaldehyde toxicity via airway delivery. Lab Chip 2014, 14, 677–680. [Google Scholar] [CrossRef]
- Gholizadeh, H.; Cheng, S.; Kourmatzis, A.; Traini, D.; Young, P.; Sheikh, Z.; Ong, H.X. In vitro interactions of aerosol formulations with human nasal epithelium using real-time monitoring of drug transport in a nasal mucosa-on-a-chip. Biosens. Bioelectron. 2023, 223, 115010. [Google Scholar] [CrossRef]
- Huh, D.; Leslie, D.C.; Matthews, B.D.; Fraser, J.P.; Jurek, S.; Hamilton, G.A.; Thorneloe, K.S.; McAlexander, M.A.; Ingber, D.E. A Human Disease Model of Drug Toxicity–Induced Pulmonary Edema in a Lung-on-a-Chip Microdevice. Sci. Transl. Med. 2012, 4, 159ra147. [Google Scholar] [CrossRef]
- Bovard, D.; Sandoz, A.; Luettich, K.; Frentzel, S.; Iskandar, A.; Marescotti, D.; Trivedi, K.; Guedj, E.; Dutertre, Q.; Peitsch, M.C. A lung/liver-on-a-chip platform for acute and chronic toxicity studies. Lab Chip 2018, 18, 3814–3829. [Google Scholar] [CrossRef] [PubMed]
- Nof, E.; Zidan, H.; Artzy-Schnirman, A.; Mouhadeb, O.; Beckerman, M.; Bhardwaj, S.; Elias-Kirma, S.; Gur, D.; Beth-Din, A.; Levenberg, S.; et al. Human Multi-Compartment Airways-on-Chip Platform for Emulating Respiratory Airborne Transmission: From Nose to Pulmonary Acini. Front. Physiol. 2022, 13, 853317. [Google Scholar] [CrossRef] [PubMed]
- Costa, A.; Andrade, F. 4.4—Tissue-based in vitro and ex vivo models for pulmonary permeability studies. In Concepts and Models for Drug Permeability Studies; Sarmento, B., Ed.; Woodhead Publishing: Cambridge, UK, 2016; pp. 255–272. [Google Scholar] [CrossRef]
- Krinke, G.J.; Weber, K. Chapter 2.3—Histology. In The Laboratory Mouse, 2nd ed.; Hedrich, H.J., Ed.; Academic Press: Boston, MA, USA, 2012; pp. 161–192. [Google Scholar] [CrossRef]
- Mahler, G.J.; Esch, M.B.; Glahn, R.P.; Shuler, M.L. Characterization of a gastrointestinal tract microscale cell culture analog used to predict drug toxicity. Biotechnol. Bioeng. 2009, 104, 193–205. [Google Scholar] [CrossRef]
- Abaci, H.E.; Shuler, M.L. Human-on-a-chip design strategies and principles for physiologically based pharmacokinetics/pharmacodynamics modeling. Integr. Biol. 2015, 7, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.H.; Shuler, M.L. A micro cell culture analog (µCCA) with 3-D hydrogel culture of multiple cell lines to assess metabolism-dependent cytotoxicity of anti-cancer drugs. Lab Chip 2009, 9, 1385–1394. [Google Scholar] [CrossRef]
- Oleaga, C.; Bernabini, C.; Smith, A.S.; Srinivasan, B.; Jackson, M.; McLamb, W.; Platt, V.; Bridges, R.; Cai, Y.; Santhanam, N. Multi-Organ toxicity demonstration in a functional human in vitro system composed of four organs. Sci. Rep. 2016, 6, 20030. [Google Scholar] [CrossRef]
- Edington, C.D.; Chen, W.L.K.; Geishecker, E.; Kassis, T.; Soenksen, L.R.; Bhushan, B.M.; Freake, D.; Kirschner, J.; Maass, C.; Tsamandouras, N. Interconnected microphysiological systems for quantitative biology and pharmacology studies. Sci. Rep. 2018, 8, 4530. [Google Scholar] [CrossRef]
- Chen, Y.; Gao, D.; Liu, H.; Lin, S.; Jiang, Y. Drug cytotoxicity and signaling pathway analysis with three-dimensional tumor spheroids in a microwell-based microfluidic chip for drug screening. Anal. Chim. Acta 2015, 898, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.-P.; Ma, Y.; Lou, Q.; Zhu, H.; Yang, B.; Fang, Q. Three-dimensional cell culture and drug testing in a microfluidic sidewall-attached droplet array. Anal. Chem. 2017, 89, 10153–10157. [Google Scholar] [CrossRef]
- Jang, K.-J.; Otieno, M.A.; Ronxhi, J.; Lim, H.-K.; Ewart, L.; Kodella, K.R.; Petropolis, D.B.; Kulkarni, G.; Rubins, J.E.; Conegliano, D.; et al. Reproducing human and cross-species drug toxicities using a Liver-Chip. Science Transl. Med. 2019, 11, eaax5516. [Google Scholar] [CrossRef]
- Vachhani, S.; Kleinstreuer, C. Comparison of micron- and nano-particle transport in the human nasal cavity with a focus on the olfactory region. Comput. Biol. Med. 2021, 128, 104103. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.; Deng, R.; Hao Tong, W.; Huan, L.; Chan Way, N.; IslamBadhan, A.; Iliescu, C.; Yu, H. A perfusion incubator liver chip for 3D cell culture with application on chronic hepatotoxicity testing. Sci. Rep. 2017, 7, 14528. [Google Scholar] [CrossRef]
- Ma, C.; Zhao, L.; Zhou, E.-M.; Xu, J.; Shen, S.; Wang, J. On-chip construction of liver lobule-like microtissue and its application for adverse drug reaction assay. Anal. Chem. 2016, 88, 1719–1727. [Google Scholar] [CrossRef]
- Theobald, J.; Ghanem, A.; Wallisch, P.; Banaeiyan, A.A.; Andrade-Navarro, M.A.; Taškova, K.; Haltmeier, M.; Kurtz, A.; Becker, H.; Reuter, S.; et al. Liver-Kidney-on-Chip To Study Toxicity of Drug Metabolites. ACS Biomater. Sci. Eng. 2018, 4, 78–89. [Google Scholar] [CrossRef]
- Delalat, B.; Cozzi, C.; Rasi Ghaemi, S.; Polito, G.; Kriel, F.H.; Michl, T.D.; Harding, F.J.; Priest, C.; Barillaro, G.; Voelcker, N.H. Microengineered bioartificial liver chip for drug toxicity screening. Adv. Funct. Mater. 2018, 28, 1801825. [Google Scholar] [CrossRef]
- Shankar, K.; Mehendale, H.M. Cytochrome P450. In Encyclopedia of Toxicology, 3rd ed.; Wexler, P., Ed.; Academic Press: Oxford, UK, 2014; pp. 1125–1127. [Google Scholar] [CrossRef]
- Bernhardt, R. Cytochromes P450 as versatile biocatalysts. J. Biotechnol. 2006, 124, 128–145. [Google Scholar] [CrossRef] [PubMed]
- Foster, A.J.; Chouhan, B.; Regan, S.L.; Rollison, H.; Amberntsson, S.; Andersson, L.C.; Srivastava, A.; Darnell, M.; Cairns, J.; Lazic, S.E.; et al. Integrated in vitro models for hepatic safety and metabolism: Evaluation of a human Liver-Chip and liver spheroid. Arch. Toxicol. 2019, 93, 1021–1037. [Google Scholar] [CrossRef]
- Jang, K.-J.; Mehr, A.P.; Hamilton, G.A.; McPartlin, L.A.; Chung, S.; Suh, K.-Y.; Ingber, D.E. Human kidney proximal tubule-on-a-chip for drug transport and nephrotoxicity assessment. Integr. Biol. 2013, 5, 1119–1129. [Google Scholar] [CrossRef]
- Li, Z.; Jiang, L.; Zhu, Y.; Su, W.; Xu, C.; Tao, T.; Shi, Y.; Qin, J. Assessment of hepatic metabolism-dependent nephrotoxicity on an organs-on-a-chip microdevice. Toxicol. In Vitro 2018, 46, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zager, R.A.; Johnson, A.C.; Becker, K. Renal Cortical Lactate Dehydrogenase: A Useful, Accurate, Quantitative Marker of In Vivo Tubular Injury and Acute Renal Failure. PLoS ONE 2013, 8, e66776. [Google Scholar] [CrossRef]
- Li, Z.; Su, W.; Zhu, Y.; Tao, T.; Li, D.; Peng, X.; Qin, J. Drug absorption related nephrotoxicity assessment on an intestine-kidney chip. Biomicrofluidics 2017, 11, 034114. [Google Scholar] [CrossRef]
- Song, N.; Yang, M.; Zhang, H.; Yang, S.K. Intracellular Calcium Homeostasis and Kidney Disease. Curr. Med. Chem. 2021, 28, 3647–3665. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Yang, D. Role of intracellular Ca2+ and Na+/Ca2+ exchanger in the pathogenesis of contrast-induced acute kidney injury. BioMed Res. Int. 2013, 2013, 678456. [Google Scholar] [CrossRef]
- Choucha-Snouber, L.; Aninat, C.; Grsicom, L.; Madalinski, G.; Brochot, C.; Poleni, P.E.; Razan, F.; Guillouzo, C.G.; Legallais, C.; Corlu, A. Investigation of ifosfamide nephrotoxicity induced in a liver–kidney co-culture biochip. Biotechnol. Bioeng. 2013, 110, 597–608. [Google Scholar] [CrossRef]
- Weber, E.J.; Lidberg, K.A.; Wang, L.; Bammler, T.K.; MacDonald, J.W.; Li, M.J.; Redhair, M.; Atkins, W.M.; Tran, C.; Hines, K.M.; et al. Human kidney on a chip assessment of polymyxin antibiotic nephrotoxicity. JCI Insight 2018, 3, e123673. [Google Scholar] [CrossRef] [PubMed]
- Mathur, A.; Loskill, P.; Shao, K.; Huebsch, N.; Hong, S.; Marcus, S.G.; Marks, N.; Mandegar, M.; Conklin, B.R.; Lee, L.P. Human iPSC-based cardiac microphysiological system for drug screening applications. Sci. Rep. 2015, 5, 8883. [Google Scholar] [CrossRef]
- Kanamori, T.; Sugiura, S.; Sakai, Y. Technical aspects of microphysiological systems (MPS) as a promising wet human-in-vivo simulator. Drug Metab. Pharmacokinet. 2018, 33, 40–42. [Google Scholar] [CrossRef] [PubMed]
- Maschmeyer, I.; Lorenz, A.K.; Schimek, K.; Hasenberg, T.; Ramme, A.P.; Hübner, J.; Lindner, M.; Drewell, C.; Bauer, S.; Thomas, A. A four-organ-chip for interconnected long-term co-culture of human intestine, liver, skin and kidney equivalents. Lab Chip 2015, 15, 2688–2699. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Usman Khan, M.; Cai, X.; Shen, Z.; Mekonnen, T.; Kourmatzis, A.; Cheng, S.; Gholizadeh, H. Challenges in the Development and Application of Organ-on-Chips for Intranasal Drug Delivery Studies. Pharmaceutics 2023, 15, 1557. https://doi.org/10.3390/pharmaceutics15051557
Usman Khan M, Cai X, Shen Z, Mekonnen T, Kourmatzis A, Cheng S, Gholizadeh H. Challenges in the Development and Application of Organ-on-Chips for Intranasal Drug Delivery Studies. Pharmaceutics. 2023; 15(5):1557. https://doi.org/10.3390/pharmaceutics15051557
Chicago/Turabian StyleUsman Khan, Muhammad, Xinyu Cai, Zhiwei Shen, Taye Mekonnen, Agisilaos Kourmatzis, Shaokoon Cheng, and Hanieh Gholizadeh. 2023. "Challenges in the Development and Application of Organ-on-Chips for Intranasal Drug Delivery Studies" Pharmaceutics 15, no. 5: 1557. https://doi.org/10.3390/pharmaceutics15051557