
The Effect of Intracellular Tacrolimus Exposure on Calcineurin Inhibition in Immediate- and Extended-Release Tacrolimus Formulations
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Measurement of Intracellular and Whole Blood Tacrolimus
2.3. Calcineurin Activity Measurement
2.4. Pharmacokinetic and Pharmacodynamic Analysis
2.4.1. Model-Independent Approach
2.4.2. Pharmacodynamic Modelling
2.5. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Intracellular Pharmacokinetics
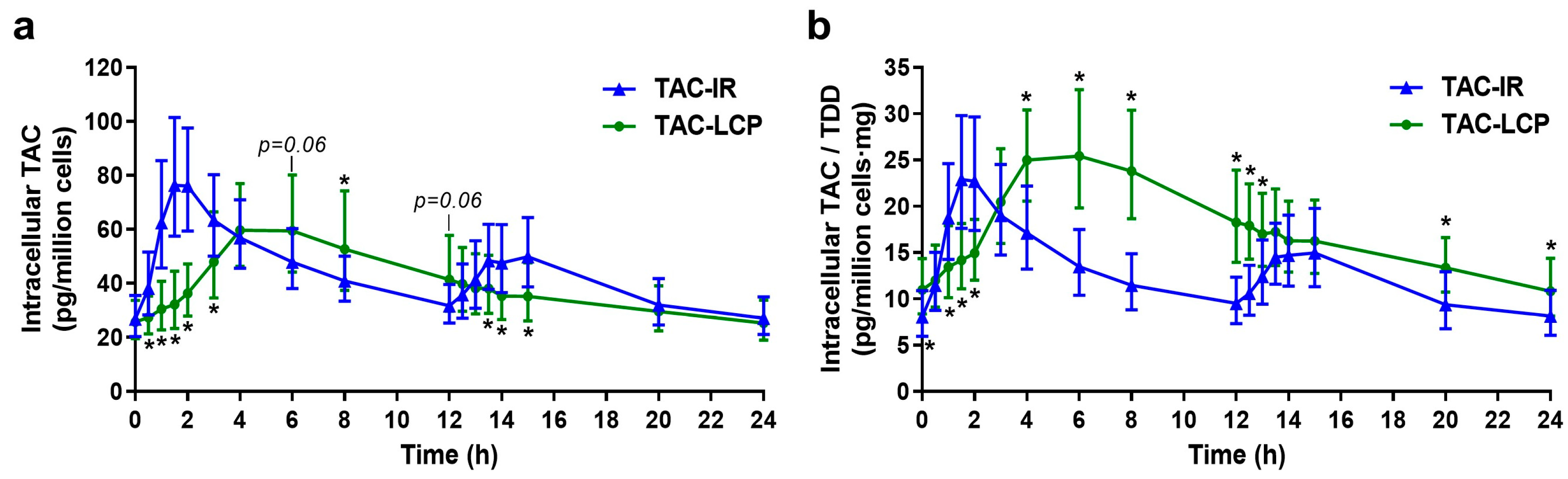
3.2.1. Differences between Intracellular TAC-IR and TAC-LCP Pharmacokinetics
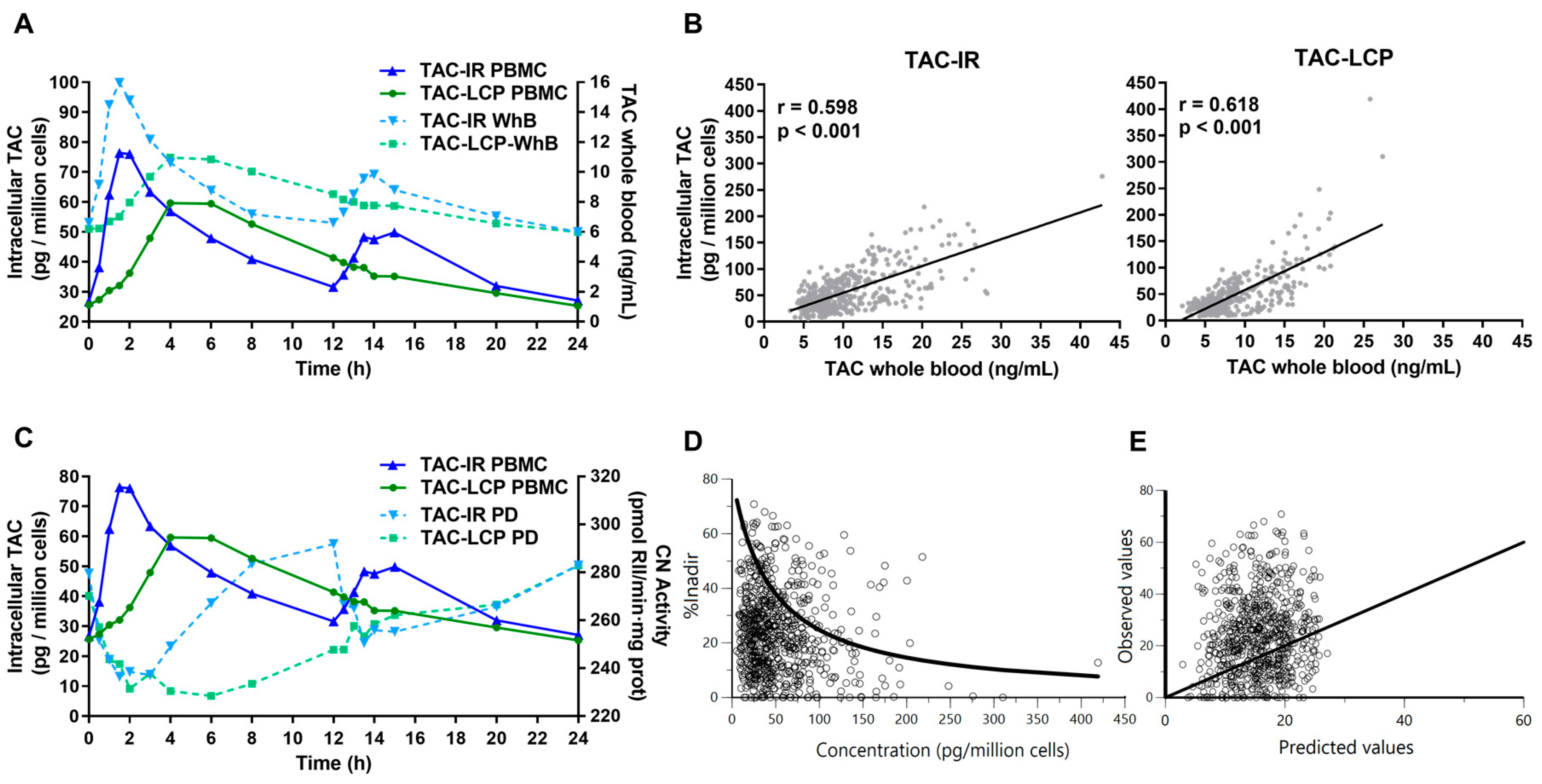
3.2.2. Relationship between Intracellular and Whole Blood Tacrolimus
3.3. Relationship between Intracellular Tacrolimus and Calcineurin Activity
3.4. Pharmacodynamic Modelling
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Venkataramanan, R.; Shaw, L.M.; Sarkozi, L.; Mullins, R.; Pirsch, J.; MacFarlane, G.; Scheller, D.; Ersfeld, D.; Frick, M.; Fitzsimmons, W.E.; et al. Clinical Utility of Monitoring Tacrolimus Blood Concentrations in Liver Transplant Patients. J. Clin. Pharmacol. 2001, 41, 542–551. [Google Scholar] [CrossRef]
- Andrews, L.M.; Li, Y.; De Winter, B.C.M.; Shi, Y.Y.; Baan, C.C.; Van Gelder, T.; Hesselink, D.A. Pharmacokinetic Considerations Related to Therapeutic Drug Monitoring of Tacrolimus in Kidney Transplant Patients. Expert Opin. Drug Metab. Toxicol. 2017, 13, 1225–1236. [Google Scholar] [CrossRef]
- Tron, C.; Woillard, J.B.; Houssel-Debry, P.; David, V.; Jezequel, C.; Rayar, M.; Balakirouchenane, D.; Blanchet, B.; Debord, J.; Petitcollin, A.; et al. Pharmacogenetic—Whole Blood and Intracellular Pharmacokinetic—Pharmacodynamic (PG-PK2-PD) Relationship of Tacrolimus in Liver Transplant Recipients. PLoS ONE 2020, 15, e0230195. [Google Scholar] [CrossRef]
- Tron, C.; Lemaitre, F.; Verstuyft, C.; Petitcollin, A.; Verdier, M.C.; Bellissant, E. Pharmacogenetics of Membrane Transporters of Tacrolimus in Solid Organ Transplantation. Clin. Pharmacokinet. 2019, 58, 593–613. [Google Scholar] [CrossRef] [PubMed]
- Vafadari, R.; Bouamar, R.; Hesselink, D.A.; Kraaijeveld, R.; Van Schaik, R.H.N.; Weimar, W.; Baan, C.C.; Van Gelder, T. Genetic Polymorphisms in ABCB1 Influence the Pharmacodynamics of Tacrolimus. Ther. Drug Monit. 2013, 35, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Capron, A.; Mourad, M.; De Meyer, M.; De Pauw, L.; Eddour, D.C.; Latinne, D.; Elens, L.; Haufroid, V.; Wallemacq, P. CYP3A5 and ABCB1 Polymorphisms Influence Tacrolimus Concentrations in Peripheral Blood Mononuclear Cells after Renal Transplantation. Pharmacogenomics 2010, 11, 703–714. [Google Scholar] [CrossRef] [PubMed]
- Capron, A.; Lerut, J.; Latinne, D.; Rahier, J.; Haufroid, V.; Wallemacq, P. Correlation of Tacrolimus Levels in Peripheral Blood Mononuclear Cells with Histological Staging of Rejection after Liver Transplantation: Preliminary Results of a Prospective Study. Transpl. Int. 2012, 25, 41–47. [Google Scholar] [CrossRef]
- Lemaitre, F.; Antignac, M.; Fernandez, C. Monitoring of Tacrolimus Concentrations in Peripheral Blood Mononuclear Cells: Application to Cardiac Transplant Recipients. Clin. Biochem. 2013, 46, 1538–1541. [Google Scholar] [CrossRef]
- Capron, A.; Musuamba, F.; Latinne, D.; Mourad, M.; Lerut, J.; Haufroid, V.; Wallemacq, P.E. Validation of a Liquid Chromatography-Mass Spectrometric Assay for Tacrolimus in Peripheral Blood Mononuclear Cells. Ther. Drug Monit. 2009, 31, 178–186. [Google Scholar] [CrossRef]
- Capron, A.; Haufroid, V.; Wallemacq, P. Intra-Cellular Immunosuppressive Drugs Monitoring: A Step Forward towards Better Therapeutic Efficacy after Organ Transplantation? Pharmacol. Res. 2016, 111, 610–618. [Google Scholar] [CrossRef]
- Lemaitre, F.; Antignac, M.; Verdier, M.C.; Bellissant, E.; Fernandez, C. Opportunity to Monitor Immunosuppressive Drugs in Peripheral Blood Mononuclear Cells: Where Are We and Where Are We Going? Pharmacol. Res. 2013, 74, 109–112. [Google Scholar] [CrossRef]
- Brunet, M.; van Gelder, T.; Asberg, A.; Haufroid, V.; Hesselink, D.A.; Langman, L.; Lemaitre, F.; Marquet, P.; Seger, C.; Shipkova, M.; et al. Therapeutic Drug Monitoring of Tacrolimus-Personalized Therapy: Second Consensus Report. Ther. Drug Monit. 2019, 41, 261–307. [Google Scholar] [CrossRef] [PubMed]
- Bouamar, R.; Shuker, N.; Hesselink, D.A.; Weimar, W.; Ekberg, H.; Kaplan, B.; Bernasconi, C.; Van Gelder, T. Tacrolimus Predose Concentrations Do Not Predict the Risk of Acute Rejection after Renal Transplantation: A Pooled Analysis from Three Randomized-Controlled Clinical Trials. Am. J. Transplant. 2013, 13, 1253–1261. [Google Scholar] [CrossRef]
- Kuypers, D.R.J.; Claes, K.; Evenepoel, P.; Maes, B.; Vanrenterghem, Y. Clinical Efficacy and Toxicity Profile of Tacrolimus and Mycophenolic Acid in Relation to Combined Long-Term Pharmacokinetics in de Novo Renal Allograft Recipients. Clin. Pharmacol. Ther. 2004, 75, 434–447. [Google Scholar] [CrossRef]
- Fontova, P.; Colom, H.; Rigo-Bonnin, R.; Bestard, O.; Vidal-Alabró, A.; van Merendonk, L.N.; Cerezo, G.; Polo, C.; Montero, N.; Melilli, E.; et al. Sustained Inhibition of Calcineurin Activity With a Melt-Dose Once-Daily Tacrolimus Formulation in Renal Transplant Recipients. Clin. Pharmacol. Ther. 2021, 110, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Fontova, P.; Colom, H.; Rigo-Bonnin, R.; van Merendonk, L.N.; Vidal-Alabró, A.; Montero, N.; Melilli, E.; Meneghini, M.; Manonelles, A.; Cruzado, J.M.; et al. Influence of the Circadian Timing System on Tacrolimus Pharmacokinetics and Pharmacodynamics After Kidney Transplantation. Front. Pharmacol. 2021, 12, 636048. [Google Scholar] [CrossRef] [PubMed]
- Han, S.S.; Yang, S.H.; Kim, M.C.; Cho, J.Y.; Min, S.I.; Lee, J.P.; Kim, D.K.; Ha, J.; Kim, Y.S. Monitoring the Intracellular Tacrolimus Concentration in Kidney Transplant Recipients with Stable Graft Function. PLoS ONE 2016, 11, e0153491. [Google Scholar] [CrossRef] [PubMed]
- Fruman, D.A.; Klee, C.B.; Bierer, B.E.; Burakoff, S.J. Calcineurin Phosphatase Activity in T Lymphocytes Is Inhibited by FK 506 and Cyclosporin A. Proc. Natl. Acad. Sci. USA 1992, 89, 3686–3690. [Google Scholar] [CrossRef]
- Halloran, P.F. Immunosuppressive Drugs for Kidney Transplantation. N. Engl. J. Med. 2004, 351, 2715–2729. [Google Scholar] [CrossRef] [PubMed]
- Francke, M.I.; Andrews, L.M.; Lan Le, H.; van de Velde, D.; Dieterich, M.; Udomkarnjananun, S.; Clahsen-van Groningen, M.C.; Baan, C.C.; van Gelder, T.; de Winter, B.C.M.; et al. Monitoring Intracellular Tacrolimus Concentrations and Its Relationship with Rejection in the Early Phase after Renal Transplantation. Clin. Biochem. 2022, 101, 9–15. [Google Scholar] [CrossRef]
- Lemaitre, F.; Blanchet, B.; Latournerie, M.; Antignac, M.; Houssel-Debry, P.; Verdier, M.C.; Dermu, M.; Camus, C.; Le Priol, J.; Roussel, M.; et al. Pharmacokinetics and Pharmacodynamics of Tacrolimus in Liver Transplant Recipients: Inside the White Blood Cells. Clin. Biochem. 2015, 48, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Johnston, A. Equivalence and Interchangeability of Narrow Therapeutic Index Drugs in Organ Transplantation. Eur. J. Hosp. Pharm. 2013, 20, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Kung, L.; Halloran, P.F. Immunophilins May Limit Calcineurin Inhibition by Cyclosporine and Tacrolimus at High Drug Concentrations. Transplantation 2000, 70, 327–335. [Google Scholar] [CrossRef] [PubMed]
- van Merendonk, L.N.; Fontova, P.; Rigo-Bonnin, R.; Colom, H.; Vidal-Alabró, A.; Bestard, O.; Torras, J.; Cruzado, J.M.; Grinyó, J.M.; Lloberas, N. Validation and Evaluation of Four Sample Preparation Methods for the Quantification of Intracellular Tacrolimus in Peripheral Blood Mononuclear Cells by UHPLC-MS/MS. Clin. Chim. Acta 2020, 503, 210–217. [Google Scholar] [CrossRef]
- Rigo-Bonnin, R.; Arbiol-Roca, A.; de Aledo-Castillo, J.M.G.; Alía, P. Simultaneous Measurement of Cyclosporine A, Everolimus, Sirolimus and Tacrolimus Concentrations in Human Blood by UPLC–MS/MS. Chromatographia 2015, 78, 1459–1474. [Google Scholar] [CrossRef]
- Fontova, P.; Rigo-Bonnin, R.; Vidal-Alabró, A.; Cerezo, G.; Bestard, O.; Cruzado, J.M.; Torras, J.; Grinyó, J.M.; Lloberas, N. Measurement of Calcineurin Activity in Peripheral Blood Mononuclear Cells by Ultra-High Performance Liquid Chromatography-Tandem Mass Spectrometry. Renal Transplant Recipients Application (Pharmacodynamic Monitoring). Clin. Chim. Acta 2019, 495, 287–293. [Google Scholar] [CrossRef]
- Yamaoka, T.; Nakagawa, T.; Uno, T. Application of Akaike’s Information Criterion (AIC) in the Evaluation of Linear Pharmacokinetics Equations. J. Pharmacokinet. Biopharm. 1978, 6, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Francke, M.I.; Hesselink, D.A.; Li, Y.; Koch, B.C.P.; de Wit, L.E.A.; van Schaik, R.H.N.; Yang, L.; Baan, C.C.; van Gelder, T.; de Winter, B.C.M. Monitoring the Tacrolimus Concentration in Peripheral Blood Mononuclear Cells of Kidney Transplant Recipients. Br. J. Clin. Pharmacol. 2021, 87, 1918–1929. [Google Scholar] [CrossRef]
- Tremblay, S.; Nigro, V.; Weinberg, J.; Woodle, E.S.; Alloway, R.R. A Steady-State Head-to-Head Pharmacokinetic Comparison of All FK-506 (Tacrolimus) Formulations (ASTCOFF): An Open-Label, Prospective, Randomized, Two-Arm, Three-Period Crossover Study. Am. J. Transplant. 2017, 17, 432–442. [Google Scholar] [CrossRef]
- Budde, K.; Bunnapradist, S.; Grinyo, J.M.; Ciechanowski, K.; Denny, J.E.; Silva, H.T.; Rostaing, L. Novel Once-Daily Extended-Release Tacrolimus (LCPT) versus Twice-Daily Tacrolimus in de Novo Kidney Transplants: One-Year Results of Phase III, Double-Blind, Randomized Trial. Am. J. Transplant. 2014, 14, 2796–2806. [Google Scholar] [CrossRef]
- Pensi, D.; De Nicolò, A.; Pinon, M.; Calvo, P.L.; Nonnato, A.; Brunati, A.; Di Perri, G.; D’Avolio, A. An UPLC-MS/MS Method Coupled with Automated on-Line SPE for Quantification of Tacrolimus in Peripheral Blood Mononuclear Cells. J. Pharm. Biomed. Anal. 2015, 107, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Tron, C.; Allard, M.; Petitcollin, A.; Ferrand-Sorre, M.-J.; Verdier, M.-C.; Querzerho-Raguideau, J.; Blanchet, B.; Le Priol, J.; Roussel, M.; Deugnier, Y.; et al. Tacrolimus Diffusion across the Peripheral Mononuclear Blood Cell Membrane: Impact of Drug Transporters. Fundam. Clin. Pharmacol. 2018, 2, 113–121. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | N = 25 |
|---|---|
| Gender: Male/Female (%) | 18/7 (72/28) |
| Age (years) | 58.80 [48.44–71.12] |
| Body weight (kg) | 73.00 [62.75–79.90] |
| BMI (kg/m2) | 26.27 [22.53–29.82] |
| BSA (m2) | 1.83 [1.68–1.92] |
| Time post-transplantation (years) | 1.84 [0.97–3.88] |
| Prior kidney transplantation: Yes/No (%) | 1/24 (4/96) |
| Total daily dose (mg) | |
| - TAC-IR | 3.0 [2.25–5.00] |
| - TAC-LCP | 2.0 [1.63–3.50] |
| Dosing conversion rate [TAC-IR:TAC-LCP] | 0.70 [0.67–0.80] |
| Genotype CYP3A5 polymorphism n (%) | |
| - *1/*3 | 5 (20) |
| - *3/*3 | 20 (80) |
| Genotype CYP3A4 polymorphism n (%) | |
| - *1/*1 | 24 (96) |
| - *1/*22 | 1 (4) |
| Genotype ABCB1 polymorphism n (%) | |
| - *T/*T | 6 (24) |
| - *C-carriers | 19 (76) |
| Parameters | TAC-IR | TAC-LCP | p | |
| C0 (pg/million cells) | 26.78 (9.19–73.45) | 25.63 (8.92–79.38) | 0.789 a | |
| C0/TDD (pg/million cells/mg) | 8.03 (1.93–26.71) | 10.95 (3.01–38.39) | 0.001 a | |
| C24 (pg/million cells) | 27.09 (6.02–62.23) | 25.28 (9.27–95.26) | 0.633 a | |
| C24/TDD (pg/million cells/mg) | 8.13 (1.97–24.34) | 10.81 (3.01–40.90) | 0.008 a | |
| Cmax (pg/million cells) | 93.06 (31.51–239.41) | 70.65 (16.82–256.30) | 0.016 a | |
| Cmax/TDD (pg/million cells/mg) | 27.37 (11.13–61.54) | 30.20 (9.46–92.95) | 0.162 a | |
| AUC0–24h (pg/million cells·h) | 1052.69 (363.38–2349.86) | 969.45 (308.81–3087.34) | 0.387 a | |
| AUC0–24h/TDD (pg/million cells·h/mg) | 315.70 (119.92–878.81) | 414.38 (160.13–1141.91) | 0.001 a | |
| Tmax (h) | 1.53 [0.83–3.92] | 6.00 [3.08–13.92] | <0.001 b | |
| λz | 0.0787 (0.0280–0.160) * | 0.0461 (0.015–0.110) | <0.001 a | |
| t1/2z (h) | 8.80 (4.33–24.81) * | 15.19 (6.34–46.74) | 0.001 | |
| Correlations | TAC-IR | TAC-LCP | ||
| r | p | r | p | |
| C0 vs. AUC0–24h | 0.927 | <0.001 | 0.879 | <0.001 |
| C0/TDD vs. AUC0–24h/TDD | 0.938 | <0.001 | 0.871 | <0.001 |
| C24 vs. AUC0–24h | 0.921 | <0.001 | 0.916 | <0.001 |
| C24/TDD vs. AUC0–24h/TDD | 0.945 | <0.001 | 0.921 | <0.001 |
| Cmax vs. AUC0–24h | 0.898 | <0.001 | 0.961 | <0.001 |
| Cmax/TDD vs. AUC0–24h/TDD | 0.873 | <0.001 | 0.933 | <0.001 |
| C0 vs. Cmax | 0.772 | <0.001 | 0.792 | <0.001 |
| C0/TDD vs. Cmax/TDD | 0.779 | <0.001 | 0.732 | <0.001 |
| C24 vs. Cmax | 0.751 | <0.001 | 0.825 | <0.001 |
| C24/TDD vs. Cmax/TDD | 0.795 | <0.001 | 0.781 | <0.001 |
| Parameters | TAC-IR | TAC-LCP | p | |
| C0 intracellular/C0 WhB | 4.05 (1.46–9.70) | 4.23 (1.70–8.95) | 0.595 | |
| C24 intracellular/C24 WhB | 4.52 (1.15–11.70) | 4.39 (1.20–12.33) | 0.942 | |
| Cmax intracellular/Cmax WhB | 5.12 (2.07–9.88) | 5.89 (1.32–14.92) | 0.041 | |
| AUC0–24h intracellular/AUC0–24h WhB | 5.03 (1.79–10.02) | 4.96 (1.45–10.28) | 0.931 | |
| Correlations | TAC-IR | TAC-LCP | ||
| r | p | r | p | |
| C0 | 0.444 | 0.027 | 0.583 | 0.004 |
| C0/TDD | 0.589 | 0.002 | 0.631 | 0.001 |
| C24 | 0.231 | 0.265 | 0.420 | 0.046 |
| C24/TDD | 0.585 | 0.002 | 0.538 | 0.008 |
| Cmax | 0.686 | <0.001 | 0.567 | 0.005 |
| Cmax/TDD | 0.603 | 0.001 | 0.288 | 0.183 |
| AUC0–24h | 0.339 | 0.098 | 0.572 | 0.004 |
| AUC0–24h/TDD | 0.602 | 0.001 | 0.423 | 0.044 |
| Correlations | TAC-IR | TAC-LCP | ||
|---|---|---|---|---|
| r | p | r | p | |
| C0 vs. I0 | −0.388 | 0.055 | −0.301 | 0.153 |
| Cmax vs. Inadir | −0.326 | 0.112 | −0.493 | 0.014 |
| C0 vs. AUE0–24h Imin | −0.247 | 0.233 | 0.212 | 0.319 |
| AUC0–24h vs. AUE0–24h Imin | −0.327 | 0.110 | 0.236 | 0.267 |
| C0 vs. AUE0–24h Inadir | 0.325 | 0.113 | 0.053 | 0.806 |
| AUC0–24h vs. AUE0–24h Inadir | 0.454 | 0.023 | −0.032 | 0.882 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fontova, P.; van Merendonk, L.N.; Vidal-Alabró, A.; Rigo-Bonnin, R.; Cerezo, G.; van Oevelen, S.; Bestard, O.; Melilli, E.; Montero, N.; Coloma, A.; et al. The Effect of Intracellular Tacrolimus Exposure on Calcineurin Inhibition in Immediate- and Extended-Release Tacrolimus Formulations. Pharmaceutics 2023, 15, 1481. https://doi.org/10.3390/pharmaceutics15051481
Fontova P, van Merendonk LN, Vidal-Alabró A, Rigo-Bonnin R, Cerezo G, van Oevelen S, Bestard O, Melilli E, Montero N, Coloma A, et al. The Effect of Intracellular Tacrolimus Exposure on Calcineurin Inhibition in Immediate- and Extended-Release Tacrolimus Formulations. Pharmaceutics. 2023; 15(5):1481. https://doi.org/10.3390/pharmaceutics15051481
Chicago/Turabian StyleFontova, Pere, Lisanne N. van Merendonk, Anna Vidal-Alabró, Raül Rigo-Bonnin, Gema Cerezo, Stefaan van Oevelen, Oriol Bestard, Edoardo Melilli, Nuria Montero, Ana Coloma, and et al. 2023. "The Effect of Intracellular Tacrolimus Exposure on Calcineurin Inhibition in Immediate- and Extended-Release Tacrolimus Formulations" Pharmaceutics 15, no. 5: 1481. https://doi.org/10.3390/pharmaceutics15051481