
An Update on Recent Advances of Photodynamic Therapy for Primary Cutaneous Lymphomas

Abstract
:1. Introduction
2. Primary Cutaneous Lymphomas
2.1. Classification of Different Subtypes of Cutaneous Lymphoma
2.1.1. Cutaneous T-Cell Lymphoma
2.1.2. Cutaneous B-Cell Lymphoma
2.2. Management of Cutaneous T-Cell Lymphomas
2.3. Management of Cutaneous B-Cell Lymphomas
3. The Role of Photodynamic Therapy in Treating Primary Cutaneous Lymphomas
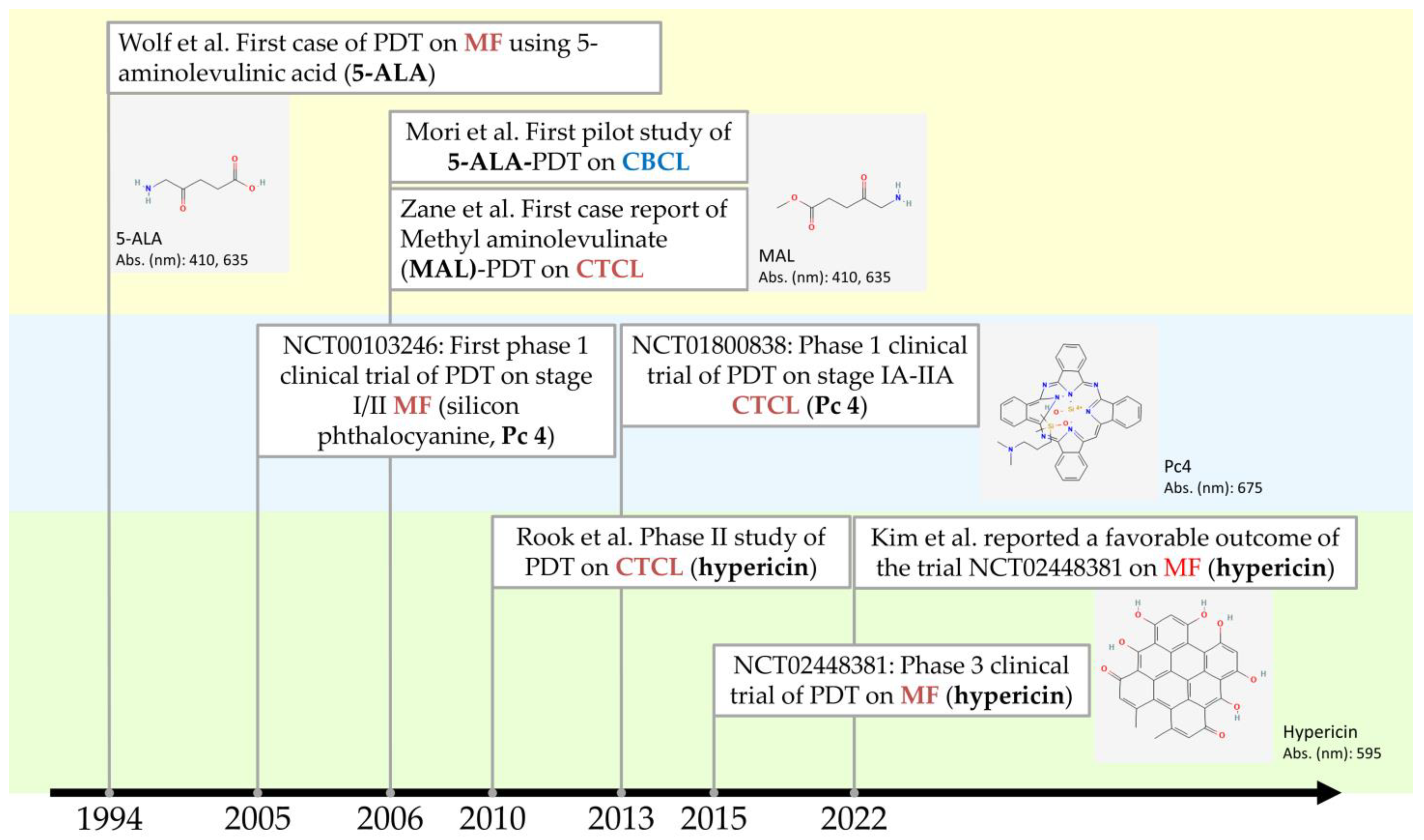
3.1. History of PDT for Primary Cutaneous Lymphomas
3.2. In Vitro Studies of PDT for PCLs
3.3. Clinical Evidence and Clinical Trials of PDT for PCLs

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Photosensitizer | Classification | Absorption Wavelength | ε (Molar Extinction Coefficient) | Depth of Penetration | Localization | Other FDA-Proved Indications |
|---|---|---|---|---|---|---|
| Silicon phthalocyanine 4 (Pc 4) | Porphyrin-based PS | 670–770 nm (675 nm) | 2 × 105 M−1 cm−1 | Can absorb more photons at greater tissue depth than PpIX (higher molar extinction coefficient) [65] | Mitochondria, Golgi apparatus, endoplasmic reticulum | NA |
| Methyl aminolevulinic acid (MAL) | Porphyrin-based PS | 410 nm > 510 nm, 540 nm, 580 nm and 635 nm | 5 × 103 M−1 cm−1 (PpIX) | Metvix: 2 mm in BCC | Endoplasmic reticulum, mitochondria | Actinic keratosis (AK) |
| 5-aminolevulinic acid (ALA) | Porphyrin-based PS | 410 nm > 510 nm, 540 nm, 580 nm and 635 nm | 5 × 103 M−1 cm−1 (PpIX) | Levulan (20% solution): 1 mm in BCC Ameluz (10% gel): may be deeper | Endoplasmic reticulum, mitochondria | AK |
| Hypericin | Non-porphyrin-based PS | 590 nm | ~4.5 × 104 M−1 cm−1 | Up to 10 mm in animal model for colon carcinoma [68] | Mitochondria and lysosomes [69] | NA |
| NCT Number Year Start | Title | Intervention | Phases | Status | Results |
|---|---|---|---|---|---|
| NCT00023790 2003 | Photodynamic Therapy in Treating Patients with Skin Cancer or Solid Tumors Metastatic to the Skin | Silicon phthalocyanine 4 (Pc 4) over 2 h on Day 1, followed by light therapy over 30–60 min on Day 2. Treatments repeated 6 weeks for a total of 2 courses. | Phase 1 | Terminated due to slow accrual | N/A |
| NCT00103246 8 February 2005 | Photodynamic Therapy Using Silicon Phthalocyanine 4 in Treating Patients with Actinic Keratosis, Bowen’s Disease, Skin Cancer, or Stage I or Stage II Mycosis Fungoides | Participants receive topical silicon phthalocyanine 4 (Pc 4). One hour later, participants undergo photodynamic therapy. Treatment repeats weekly for up to 3 weeks (up to 3 total treatments for the same lesion OR up to 3 lesions treated if multiple lesions are present). Cohorts of 3 participants receive escalating doses of Pc 4 and visible light until the maximum tolerated dose (MTD) is determined. | Phase 1 44 cases were enrolled: MF 35 cases, actinic keratosis 4 cases, squamous cell carcinoma 2 cased, basal cell carcinoma, 2 cases | Completed August 2010 | MF, 14/35 (40% with 95% CI: 0.26–0.56) responded [65] |
| NCT01800838 April 2013 | Silicon Phthalocyanine 4 and Photodynamic Therapy in Stage IA-IIA Cutaneous T-Cell Non-Hodgkin Lymphoma | A dose-escalation study. Silicon Phthalocyanine 4 (Pc 4) PDT at 0.1–0.5 mg/mL with visible light at a wavelength of 675 nm at a fluence of 50–150 J/cm2. | Phase 1 | Completed May 2015 | All 11 patients completed the trial with no serious adverse events. The maximum tolerated dose (MTD) of PDT was 150 J/cm2, and the MTD of Pc 4 was 0.1 mg/mL. |
| NCT02448381 December 2015 | FLASH [Fluorescent Light Activated Synthetic Hypericin] Clinical Study: Topical SGX301 (Synthetic Hypericin) for the Treatment of Cutaneous T-Cell Lymphoma (Mycosis Fungoides) | SGX301 (synthetic hypericin)-PDT for early-stage (IA-IIA) MF/CLCT, twice weekly for 6 weeks. | Phase 3 Randomized, double-blind, placebo-controlled study | Completed November 2020 | Hypericin PDT was more effective than placebo, index lesion response rate (ILRR), defined as 50% or greater improvement, after Cycle 1 of treatment (16% vs. 4%; p = 0.04) [67] |
| NCT03281811 13 November 2017 | Photodynamic Therapy in Treating Patients with Refractory Mycosis Fungoides | Patients receive aminolevulinic acid hydrochloride topically and undergo photodynamic therapy on Day 1. Treatment repeats every 4 weeks for up to 6 cycles in the absence of disease progression or unacceptable toxicity. Beginning at Week 24, patients undergo radiation therapy daily for 4 weeks. | Early phase 1 11 cases with 30 lesions, single group assignment | Completed 12 August 2020 | Response rates of 36.4% by Physician Global Assessment [64] |
| NCT05380635 9 May 2022 | Pharmacokinetic (PK) and electrocardiogram (ECG) Determinations Following 8 Weeks of HyBryte Treatment for Cutaneous T-Cell Lymphoma | HyBryte (0.25% hypericin, SGX301) ointment was applied to CTCL lesions and treated with visible light 18–24 h later starting at 5 J/cm2. Treatment performed twice a week for 8 weeks | Phase 2 Single group assignment | Completed 16 August 2022 | N/A |
4. Pros and Cons of PDT for Primary Cutaneous Lymphomas
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Comprehensive Cancer Network. Primary Cutaneous Lymphomas (Version 2. 2022). Available online: https://www.nccn.org/professionals/physician_gls/pdf/primary_cutaneous.pdf (accessed on 20 December 2022).
- Dobos, G.; Pohrt, A.; Ram-Wolff, C.; Lebbé, C.; Bouaziz, J.D.; Battistella, M.; Bagot, M.; de Masson, A. Epidemiology of Cutaneous T-Cell Lymphomas: A Systematic Review and Meta-Analysis of 16,953 Patients. Cancers 2020, 12, 2921. [Google Scholar] [CrossRef] [PubMed]
- Willemze, R.; Jaffe, E.S.; Burg, G.; Cerroni, L.; Berti, E.; Swerdlow, S.H.; Ralfkiaer, E.; Chimenti, S.; Diaz-Perez, J.L.; Duncan, L.M.; et al. WHO-EORTC classification for cutaneous lymphomas. Blood 2005, 105, 3768–3785. [Google Scholar] [CrossRef] [PubMed]
- Willemze, R.; Cerroni, L.; Kempf, W.; Berti, E.; Facchetti, F.; Swerdlow, S.H.; Jaffe, E.S. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood 2019, 133, 1703–1714. [Google Scholar] [CrossRef]
- Kempf, W.; Zimmermann, A.K.; Mitteldorf, C. Cutaneous lymphomas-An update 2019. Hematol. Oncol. 2019, 37 (Suppl. S1), 43–47. [Google Scholar] [CrossRef]
- Willemze, R.; Hodak, E.; Zinzani, P.L.; Specht, L.; Ladetto, M. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv30–iv40. [Google Scholar] [CrossRef]
- Kessel, D. Photodynamic Therapy: A Brief History. J. Clin. Med. 2019, 8, 1581. [Google Scholar] [CrossRef]
- Lee, C.N.; Hsu, R.; Chen, H.; Wong, T.W. Daylight Photodynamic Therapy: An Update. Molecules 2020, 25, 5195. [Google Scholar] [CrossRef]
- Correia, J.H.; Rodrigues, J.A.; Pimenta, S.; Dong, T.; Yang, Z. Photodynamic Therapy Review: Principles, Photosensitizers, Applications, and Future Directions. Pharmaceutics 2021, 13, 1332. [Google Scholar] [CrossRef] [PubMed]
- Ozog, D.M.; Rkein, A.M.; Fabi, S.G.; Gold, M.H.; Goldman, M.P.; Lowe, N.J.; Martin, G.M.; Munavalli, G.S. Photodynamic Therapy: A Clinical Consensus Guide. Dermatol. Surg. 2016, 42, 804–827. [Google Scholar] [CrossRef]
- Lin, M.H.; Lee, J.Y.; Pan, S.C.; Wong, T.W. Enhancing wound healing in recalcitrant leg ulcers with aminolevulinic acid-mediated antimicrobial photodynamic therapy. Photodiagn. Photodyn. Ther. 2021, 33, 102149. [Google Scholar] [CrossRef]
- Nordmann, N.J.; Michael, A.P. 5-Aminolevulinic acid radiodynamic therapy for treatment of high-grade gliomas: A systematic review. Clin. Neurol. Neurosurg. 2021, 201, 106430. [Google Scholar] [CrossRef]
- Dolmans, D.E.; Fukumura, D.; Jain, R.K. Photodynamic therapy for cancer. Nat. Rev. Cancer 2003, 3, 380–387. [Google Scholar] [CrossRef]
- Wu, J.-J.; Zhang, J.; Xia, C.-Y.; Ding, K.; Li, X.-X.; Pan, X.-G.; Xu, J.-K.; He, J.; Zhang, W.-K. Hypericin: A natural anthraquinone as promising therapeutic agent. Phytomedicine 2023, 111, 154654. [Google Scholar] [CrossRef]
- Wong, T.W.; Liao, S.Z.; Ko, W.C.; Wu, C.J.; Wu, S.B.; Chuang, Y.C.; Huang, I.H. Indocyanine Green-Mediated Photodynamic Therapy Reduces Methicillin-Resistant Staphylococcus aureus Drug Resistance. J. Clin. Med. 2019, 8, 411. [Google Scholar] [CrossRef]
- Hung, J.H.; Wang, Z.X.; Lo, Y.H.; Lee, C.N.; Chang, Y.; Chang, R.Y.; Huang, C.C.; Wong, T.W. Rose Bengal-Mediated Photodynamic Therapy to Inhibit Candida albicans. J. Vis. Exp. 2022. [Google Scholar] [CrossRef]
- Youf, R.; Müller, M.; Balasini, A.; Thétiot, F.; Müller, M.; Hascoët, A.; Jonas, U.; Schönherr, H.; Lemercier, G.; Montier, T.; et al. Antimicrobial Photodynamic Therapy: Latest Developments with a Focus on Combinatory Strategies. Pharmaceutics 2021, 13, 1995. [Google Scholar] [CrossRef] [PubMed]
- Hamada, T.; Iwatsuki, K. Cutaneous lymphoma in Japan: A nationwide study of 1733 patients. J. Dermatol. 2014, 41, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Campo, E.; Jaffe, E.S.; Cook, J.R.; Quintanilla-Martinez, L.; Swerdlow, S.H.; Anderson, K.C.; Brousset, P.; Cerroni, L.; de Leval, L.; Dirnhofer, S.; et al. The International Consensus Classification of Mature Lymphoid Neoplasms: A report from the Clinical Advisory Committee. Blood 2022, 140, 1229–1253. [Google Scholar] [CrossRef]
- Ohtsuka, M.; Hamada, T.; Miyagaki, T.; Shimauchi, T.; Yonekura, K.; Kiyohara, E.; Fujita, H.; Izutsu, K.; Okuma, K.; Kawai, K.; et al. Outlines of the Japanese guidelines for the management of primary cutaneous lymphomas 2020. J. Dermatol. 2021, 48, e49–e71. [Google Scholar] [CrossRef]
- Keto, J.; Hahtola, S.; Linna, M.; Väkevä, L. Mycosis fungoides and Sézary syndrome: A population-wide study on prevalence and health care use in Finland in 1998–2016. BMC Health Serv. Res. 2021, 21, 166. [Google Scholar] [CrossRef]
- Olsen, E.A.; Whittaker, S.; Willemze, R.; Pinter-Brown, L.; Foss, F.; Geskin, L.; Schwartz, L.; Horwitz, S.; Guitart, J.; Zic, J.; et al. Primary cutaneous lymphoma: Recommendations for clinical trial design and staging update from the ISCL, USCLC, and EORTC. Blood 2022, 140, 419–437. [Google Scholar] [CrossRef] [PubMed]
- Mehta-Shah, N.; Ratner, L.; Horwitz, S.M. Adult T-Cell Leukemia/Lymphoma. J. Oncol. Pract. 2017, 13, 487–492. [Google Scholar] [CrossRef]
- Sarfraz, H.; Gentille, C.; Ensor, J.; Wang, L.; Wong, S.; Ketcham, M.S.; Joshi, J.; Pingali, S.R.K. Primary cutaneous anaplastic large-cell lymphoma: A review of the SEER database from 2005 to 2016. Clin. Exp. Dermatol. 2021, 46, 1420–1426. [Google Scholar] [CrossRef]
- Martinez-Cabriales, S.A.; Walsh, S.; Sade, S.; Shear, N.H. Lymphomatoid papulosis: An update and review. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 59–73. [Google Scholar] [CrossRef]
- Takahara, M.; Kumai, T.; Kishibe, K.; Nagato, T.; Harabuchi, Y. Extranodal NK/T-Cell Lymphoma, Nasal Type: Genetic, Biologic, and Clinical Aspects with a Central Focus on Epstein–Barr Virus Relation. Microorganisms 2021, 9, 1381. [Google Scholar] [CrossRef]
- David, K.A.; Pulitzer, M.; Guitart, J.; Martinez-Escala, M.E.; Geller, S.; Wang, Y.; Bennani, N.N.; Ristow, K.M.; Landsburg, D.J.; Winchell, N.; et al. Characteristics, Treatment Patterns, and Outcomes in Primary Cutaneous Gamma Delta T Cell Lymphoma (PCGDTCL): A Real World Multi-Institutional Analysis of a Rare Malignancy. Blood 2019, 134, 4028. [Google Scholar] [CrossRef]
- Vutukuri, S.; Powell, F.; Haddad, P.A. Primary Cutaneous CD8+ Aggressive Epidermotropic Cytotoxic T-Cell Lymphoma (PCAECTCL) Descriptors and Clinicopathologic Determinants of Survival: Analysis of a Pooled Database. Blood 2022, 140, 6591. [Google Scholar] [CrossRef]
- Kempf, W.; Petrella, T.; Willemze, R.; Jansen, P.; Berti, E.; Santucci, M.; Geissinger, E.; Cerroni, L.; Maubec, E.; Battistella, M.; et al. Clinical, histopathological and prognostic features of primary cutaneous acral CD8+ T-cell lymphoma and other dermal CD8+ cutaneous lymphoproliferations: Results of an EORTC Cutaneous Lymphoma Group workshop*. Br. J. Dermatol. 2022, 186, 887–897. [Google Scholar] [CrossRef]
- Surmanowicz, P.; Doherty, S.; Sivanand, A.; Parvinnejad, N.; Deschenes, J.; Schneider, M.; Hardin, J.; Gniadecki, R. The Clinical Spectrum of Primary Cutaneous CD4+ Small/Medium-Sized Pleomorphic T-Cell Lymphoproliferative Disorder: An Updated Systematic Literature Review and Case Series. Dermatology 2021, 237, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Fava, P.; Roccuzzo, G.; Alberti-Violetti, S.; Grandi, V.; Pileri, A.; Pimpinelli, N.; Berti, E.; Quaglino, P. Cutaneous B-cell lymphomas: Update on diagnosis, risk-stratification, and management. La Presse Méd. 2022, 51, 104109. [Google Scholar] [CrossRef]
- Lucioni, M.; Fraticelli, S.; Neri, G.; Feltri, M.; Ferrario, G.; Riboni, R.; Paulli, M. Primary Cutaneous B-Cell Lymphoma: An Update on Pathologic and Molecular Features. Hemato 2022, 3, 23. [Google Scholar] [CrossRef]
- Travaglino, A.; Varricchio, S.; Pace, M.; Russo, D.; Picardi, M.; Baldo, A.; Staibano, S.; Mascolo, M. Borrelia burgdorferi in primary cutaneous lymphomas: A systematic review and meta-analysis. J. Dtsch. Dermatol. Ges. 2020, 18, 1379–1384. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Inagaki, H.; Kuo, T.T.; Hu, S.; Okabe, M.; Eimoto, T. Primary cutaneous marginal zone B-cell lymphoma: A molecular and clinicopathologic study of 24 asian cases. Am. J. Surg. Pathol. 2003, 27, 1061–1069. [Google Scholar] [CrossRef]
- Vitiello, P.; Sica, A.; Ronchi, A.; Caccavale, S.; Franco, R.; Argenziano, G. Primary Cutaneous B-Cell Lymphomas: An Update. Front. Oncol. 2020, 10, 651. [Google Scholar] [CrossRef]
- Hamilton, S.N.; Wai, E.S.; Tan, K.; Alexander, C.; Gascoyne, R.D.; Connors, J.M. Treatment and outcomes in patients with primary cutaneous B-cell lymphoma: The BC Cancer Agency experience. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 719–725. [Google Scholar] [CrossRef]
- Grange, F.; Beylot-Barry, M.; Courville, P.; Maubec, E.; Bagot, M.; Vergier, B.; Souteyrand, P.; Machet, L.; Dalac, S.; Esteve, E.; et al. Primary Cutaneous Diffuse Large B-Cell Lymphoma, Leg Type: Clinicopathologic Features and Prognostic Analysis in 60 Cases. Arch. Dermatol. 2007, 143, 1144–1150. [Google Scholar] [CrossRef]
- Kaye, F.J.; Bunn, P.A., Jr.; Steinberg, S.M.; Stocker, J.L.; Ihde, D.C.; Fischmann, A.B.; Glatstein, E.J.; Schechter, G.P.; Phelps, R.M.; Foss, F.M.; et al. A randomized trial comparing combination electron-beam radiation and chemotherapy with topical therapy in the initial treatment of mycosis fungoides. N. Engl. J. Med. 1989, 321, 1784–1790. [Google Scholar] [CrossRef] [PubMed]
- Brunner, P.M.; Jonak, C.; Knobler, R. Recent advances in understanding and managing cutaneous T-cell lymphomas. F1000Research 2020, 9, 331. [Google Scholar] [CrossRef]
- Gilson, D.; Whittaker, S.J.; Child, F.J.; Scarisbrick, J.J.; Illidge, T.M.; Parry, E.J.; Mohd Mustapa, M.F.; Exton, L.S.; Kanfer, E.; Rezvani, K.; et al. British Association of Dermatologists and U.K. Cutaneous Lymphoma Group guidelines for the management of primary cutaneous lymphomas 2018. Br. J. Dermatol. 2019, 180, 496–526. [Google Scholar] [CrossRef]
- Tarabadkar, E.S.; Shinohara, M.M. Skin Directed Therapy in Cutaneous T-Cell Lymphoma. Front. Oncol. 2019, 9, 260. [Google Scholar] [CrossRef] [PubMed]
- Krenitsky, A.; Klager, S.; Hatch, L.; Sarriera-Lazaro, C.; Chen, P.L.; Seminario-Vidal, L. Update in Diagnosis and Management of Primary Cutaneous B-Cell Lymphomas. Am. J. Clin. Dermatol. 2022, 23, 689–706. [Google Scholar] [CrossRef] [PubMed]
- Dumont, M.; Battistella, M.; Ram-Wolff, C.; Bagot, M.; de Masson, A. Diagnosis and Treatment of Primary Cutaneous B-Cell Lymphomas: State of the Art and Perspectives. Cancers 2020, 12, 1497. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.V.; Bohjanen, K.A. Skin-Directed Therapies in Cutaneous T-Cell Lymphoma. Dermatol. Clin. 2015, 33, 683–696. [Google Scholar] [CrossRef]
- Olsen, E.A.; Whittaker, S.; Kim, Y.H.; Duvic, M.; Prince, H.M.; Lessin, S.R.; Wood, G.S.; Willemze, R.; Demierre, M.F.; Pimpinelli, N.; et al. Clinical end points and response criteria in mycosis fungoides and Sézary syndrome: A consensus statement of the International Society for Cutaneous Lymphomas, the United States Cutaneous Lymphoma Consortium, and the Cutaneous Lymphoma Task Force of the European Organisation for Research and Treatment of Cancer. J. Clin. Oncol. 2011, 29, 2598–2607. [Google Scholar] [CrossRef]
- Caccavale, S.; Tancredi, V.; Vitiello, P.; Sica, A.; Ronchi, A.; Franco, R.; Pastore, F.; Argenziano, G. Photodynamic Therapy as an Effective Treatment for Cutaneous Lymphomas. Pharmaceutics 2022, 15, 47. [Google Scholar] [CrossRef]
- Hasson, A.; Navarrete-Dechent, C.; Nicklas, C.; Sazunic, I. Topical photodynamic therapy with 5-aminolevulinate for the treatment of tumor-stage mycosis fungoides: A case report. Int. J. Dermatol. 2013, 52, 1535–1537. [Google Scholar] [CrossRef] [PubMed]
- Hooper, M.; Hatch, L.; Seminario-Vidal, L. Photodynamic therapy of mycosis fungoides: A systematic review of case studies. Photodermatol. Photoimmunol. Photomed. 2021, 37, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Mori, M.; Campolmi, P.; Mavilia, L.; Rossi, R.; Cappugi, P.; Pimpinelli, N. Topical photodynamic therapy for primary cutaneous B-cell lymphoma: A pilot study. J. Am. Acad. Dermatol. 2006, 54, 524–526. [Google Scholar] [CrossRef]
- Toulemonde, E.; Faiz, S.; Dubois, R.; Verhasselt-Crinquette, M.; Carpentier, O.; Abi Rached, H.; Mortier, L. Photodynamic therapy for the treatment of primary cutaneous B-cell marginal zone lymphoma: A series of 4 patients. JAAD Case Rep. 2023, 33, 62–66. [Google Scholar] [CrossRef]
- Edström, D.W.; Porwit, A.; Ros, A.M. Photodynamic therapy with topical 5-aminolevulinic acid for mycosis fungoides: Clinical and histological response. Acta Derm. Venereol. 2001, 81, 184–188. [Google Scholar] [CrossRef]
- Wolf, P.; Fink-Puches, R.; Cerroni, L.; Kerl, H. Photodynamic therapy for mycosis fungoides after topical photosensitization with 5-aminolevulinic acid. J. Am. Acad. Dermatol. 1994, 31, 678–680. [Google Scholar] [CrossRef]
- Vallecorsa, P.; Di Venosa, G.; Gola, G.; Sáenz, D.; Mamone, L.; MacRobert, A.J.; Ramírez, J.; Casas, A. Photodynamic therapy of cutaneous T-cell lymphoma cell lines mediated by 5-aminolevulinic acid and derivatives. J. Photochem. Photobiol. B 2021, 221, 112244. [Google Scholar] [CrossRef]
- Trivedi, N.S.; Wang, H.W.; Nieminen, A.L.; Oleinick, N.L.; Izatt, J.A. Quantitative analysis of Pc 4 localization in mouse lymphoma (LY-R) cells via double-label confocal fluorescence microscopy. Photochem. Photobiol. 2000, 71, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Ke, M.S.; Xue, L.Y.; Feyes, D.K.; Azizuddin, K.; Baron, E.D.; McCormick, T.S.; Mukhtar, H.; Panneerselvam, A.; Schluchter, M.D.; Cooper, K.D.; et al. Apoptosis mechanisms related to the increased sensitivity of Jurkat T-cells vs A431 epidermoid cells to photodynamic therapy with the phthalocyanine Pc 4. Photochem. Photobiol. 2008, 84, 407–414. [Google Scholar] [CrossRef]
- Chen, R.; Huang, Z.; Chen, G.; Li, Y.; Chen, X.; Chen, J.; Zeng, H. Kinetics and subcellular localization of 5-ALA-induced PpIX in DHL cells via two-photon excitation fluorescence microscopy. Int. J. Oncol. 2008, 32, 861–867. [Google Scholar]
- Shahzidi, S.; Cunderlíková, B.; Więdłocha, A.; Zhen, Y.; Vasovič, V.; Nesland, J.M.; Peng, Q. Simultaneously targeting mitochondria and endoplasmic reticulum by photodynamic therapy induces apoptosis in human lymphoma cells. Photochem. Photobiol. Sci. 2011, 10, 1773–1782. [Google Scholar] [CrossRef]
- Furre, I.E.; Møller, M.T.; Shahzidi, S.; Nesland, J.M.; Peng, Q. Involvement of both caspase-dependent and -independent pathways in apoptotic induction by hexaminolevulinate-mediated photodynamic therapy in human lymphoma cells. Apoptosis 2006, 11, 2031–2042. [Google Scholar] [CrossRef]
- Amo, T.; Kawanishi, N.; Uchida, M.; Fujita, H.; Oyanagi, E.; Utsumi, T.; Ogino, T.; Inoue, K.; Shuin, T.; Utsumi, K.; et al. Mechanism of cell death by 5-aminolevulinic acid-based photodynamic action and its enhancement by ferrochelatase inhibitors in human histiocytic lymphoma cell line U937. Cell Biochem. Funct. 2009, 27, 503–515. [Google Scholar] [CrossRef]
- Oka, T.; Mizuno, H.; Sakata, M.; Fujita, H.; Yoshino, T.; Yamano, Y.; Utsumi, K.; Masujima, T.; Utsunomiya, A. Metabolic abnormalities in adult T-cell leukemia/lymphoma and induction of specific leukemic cell death using photodynamic therapy. Sci. Rep. 2018, 8, 14979. [Google Scholar] [CrossRef]
- Sando, Y.; Matsuoka, K.I.; Sumii, Y.; Kondo, T.; Ikegawa, S.; Sugiura, H.; Nakamura, M.; Iwamoto, M.; Meguri, Y.; Asada, N.; et al. 5-aminolevulinic acid-mediated photodynamic therapy can target aggressive adult T cell leukemia/lymphoma resistant to conventional chemotherapy. Sci. Rep. 2020, 10, 17237. [Google Scholar] [CrossRef]
- Lam, M.; Lee, Y.; Deng, M.; Hsia, A.H.; Morrissey, K.A.; Yan, C.; Azzizudin, K.; Oleinick, N.L.; McCormick, T.S.; Cooper, K.D.; et al. Photodynamic therapy with the silicon phthalocyanine pc 4 induces apoptosis in mycosis fungoides and sezary syndrome. Adv. Hematol. 2010, 2010, 896161. [Google Scholar] [CrossRef]
- O’Connor, A.E.; Gallagher, W.M.; Byrne, A.T. Porphyrin and nonporphyrin photosensitizers in oncology: Preclinical and clinical advances in photodynamic therapy. Photochem. Photobiol. 2009, 85, 1053–1074. [Google Scholar] [CrossRef]
- Brumfiel, C.M.; Severson, K.J.; Patel, M.H.; Cumsky, H.J.L.; Ginos, B.F.; Kosiorek, H.E.; Janeczek, M.C.; Besch-Stokes, J.; Rule, W.; DiCaudo, D.; et al. Photodynamic Therapy in Refractory Mycosis Fungoides: A Prospective, Open-Label Study. Blood 2020, 136, 32. [Google Scholar] [CrossRef]
- Baron, E.D.; Malbasa, C.L.; Santo-Domingo, D.; Fu, P.; Miller, J.D.; Hanneman, K.K.; Hsia, A.H.; Oleinick, N.L.; Colussi, V.C.; Cooper, K.D. Silicon phthalocyanine (Pc 4) photodynamic therapy is a safe modality for cutaneous neoplasms: Results of a phase 1 clinical trial. Lasers Surg. Med. 2010, 42, 728–735. [Google Scholar] [CrossRef]
- Rook, A.H.; Wood, G.S.; Duvic, M.; Vonderheid, E.C.; Tobia, A.; Cabana, B. A phase II placebo-controlled study of photodynamic therapy with topical hypericin and visible light irradiation in the treatment of cutaneous T-cell lymphoma and psoriasis. J. Am. Acad. Dermatol. 2010, 63, 984–990. [Google Scholar] [CrossRef]
- Kim, E.J.; Mangold, A.R.; DeSimone, J.A.; Wong, H.K.; Seminario-Vidal, L.; Guitart, J.; Appel, J.; Geskin, L.; Lain, E.; Korman, N.J.; et al. Efficacy and Safety of Topical Hypericin Photodynamic Therapy for Early-Stage Cutaneous T-Cell Lymphoma (Mycosis Fungoides): The FLASH Phase 3 Randomized Clinical Trial. JAMA Dermatol. 2022, 158, 1031–1039. [Google Scholar] [CrossRef]
- Blank, M.; Kostenich, G.; Lavie, G.; Kimel, S.; Keisari, Y.; Orenstein, A. Wavelength-dependent properties of photodynamic therapy using hypericin in vitro and in an animal model. Photochem. Photobiol. 2002, 76, 335–340. [Google Scholar] [CrossRef]
- Ali, S.M.; Olivo, M. Bio-distribution and subcellular localization of Hypericin and its role in PDT induced apoptosis in cancer cells. Int. J. Oncol. 2002, 21, 531–540. [Google Scholar] [CrossRef]
- Paba, V.; Quarto, M.; Varriale, L.; Crescenzi, E.; Palumbo, G. Photo-activation of hypericin with low doses of light promotes apparent photo-resistance in human histiocytic lymphoma U937 cells. J. Photochem. Photobiol. B 2001, 60, 87–96. [Google Scholar] [CrossRef]
- Salva, K.A.; Wood, G.S. Epigenetically Enhanced Photodynamic Therapy (ePDT) is Superior to Conventional Photodynamic Therapy for Inducing Apoptosis in Cutaneous T-Cell Lymphoma. Photochem. Photobiol. 2015, 91, 1444–1451. [Google Scholar] [CrossRef]
- Shi, L.; Hu, F.; Duan, Y.; Wu, W.; Dong, J.; Meng, X.; Zhu, X.; Liu, B. Hybrid Nanospheres to Overcome Hypoxia and Intrinsic Oxidative Resistance for Enhanced Photodynamic Therapy. ACS Nano 2020, 14, 2183–2190. [Google Scholar] [CrossRef]
- Wen, L.Y.; Bae, S.M.; Chun, H.J.; Park, K.S.; Ahn, W.S. Therapeutic effects of systemic photodynamic therapy in a leukemia animal model using A20 cells. Lasers Med. Sci. 2012, 27, 445–452. [Google Scholar] [CrossRef]
- Li, Z.; Yin, Y.; Jin, W.; Zhang, B.; Yan, H.; Mei, H.; Wang, H.; Guo, T.; Shi, W.; Hu, Y. Tissue Factor-Targeted “O(2)-Evolving” Nanoparticles for Photodynamic Therapy in Malignant Lymphoma. Front. Oncol. 2020, 10, 524712. [Google Scholar] [CrossRef]
- Li, W.P.; Yen, C.J.; Wu, B.S.; Wong, T.W. Recent Advances in Photodynamic Therapy for Deep-Seated Tumors with the Aid of Nanomedicine. Biomedicines 2021, 9, 69. [Google Scholar] [CrossRef]





| Entity | Disease | Changes in ICC, 2021 |
|---|---|---|
| CTCL | MF MF variants Folliculotropic MF Pagetoid reticulosis Granulomatous slack skin SS Adult T-cell leukemia/lymphoma Primary cutaneous CD30+ LPDs C-ALCL LyP Subcutaneous panniculitis-like T-cell lymphoma Extranodal NK/T-cell lymphoma, nasal type Chronic active EBV infection Primary cutaneous peripheral T-cell lymphoma, rare subtypes Primary cutaneous γ/δ T-cell lymphoma CD8+ AECTCL (provisional) Primary cutaneous CD4+ small/medium T-cell lymphoproliferative disorder (provisional) Primary cutaneous acral CD8+ T-cell lymphoma (provisional) Primary cutaneous peripheral T-cell lymphoma, NOS | Primary cutaneous acral CD8+ T-cell LPD |
| CBCL | PCMZL PCFCL PCDLBLC, LT EBV+ mucocutaneous ulcer (provisional) Intravascular large B-cell lymphoma | Primary cutaneous marginal zone LPD |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, W.-T.; Wang, H.-T.; Yeh, Y.-H.; Wong, T.-W. An Update on Recent Advances of Photodynamic Therapy for Primary Cutaneous Lymphomas. Pharmaceutics 2023, 15, 1328. https://doi.org/10.3390/pharmaceutics15051328
Liu W-T, Wang H-T, Yeh Y-H, Wong T-W. An Update on Recent Advances of Photodynamic Therapy for Primary Cutaneous Lymphomas. Pharmaceutics. 2023; 15(5):1328. https://doi.org/10.3390/pharmaceutics15051328
Chicago/Turabian StyleLiu, Wei-Ting, Han-Tang Wang, Yi-Hsuan Yeh, and Tak-Wah Wong. 2023. "An Update on Recent Advances of Photodynamic Therapy for Primary Cutaneous Lymphomas" Pharmaceutics 15, no. 5: 1328. https://doi.org/10.3390/pharmaceutics15051328