
Design, Development, and Evaluation of Treprostinil Embedded Adhesive Transdermal Patch

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Estimation of Treprostinil by High-Performance Liquid Chromatography (HPLC)
2.3. Preparation of Drug in Adhesive Transdermal Patch
2.4. Screening of Transdermal Patch Components
2.5. Preliminary Trial Batches of Transdermal Patch
2.6. Factorial Design
2.7. Drug Release
2.8. Characterization of Transdermal Patch
2.8.1. Drug Content
2.8.2. Microscopic Observations
2.8.3. Fourier Transform Infrared Spectroscopy (FTIR) Study
2.8.4. Differential Scanning Calorimetry (DSC)
2.8.5. Coat Weight
2.8.6. Adhesion Testing
2.9. Skin Irritation
2.10. Ex Vivo and In Vivo Studies
2.11. Statistical Analysis
3. Results and Discussion
3.1. Screening of Transdermal Patch Components
3.2. Preliminary Trial Batches of Transdermal Patch
3.3. 32 Full Factorial Design
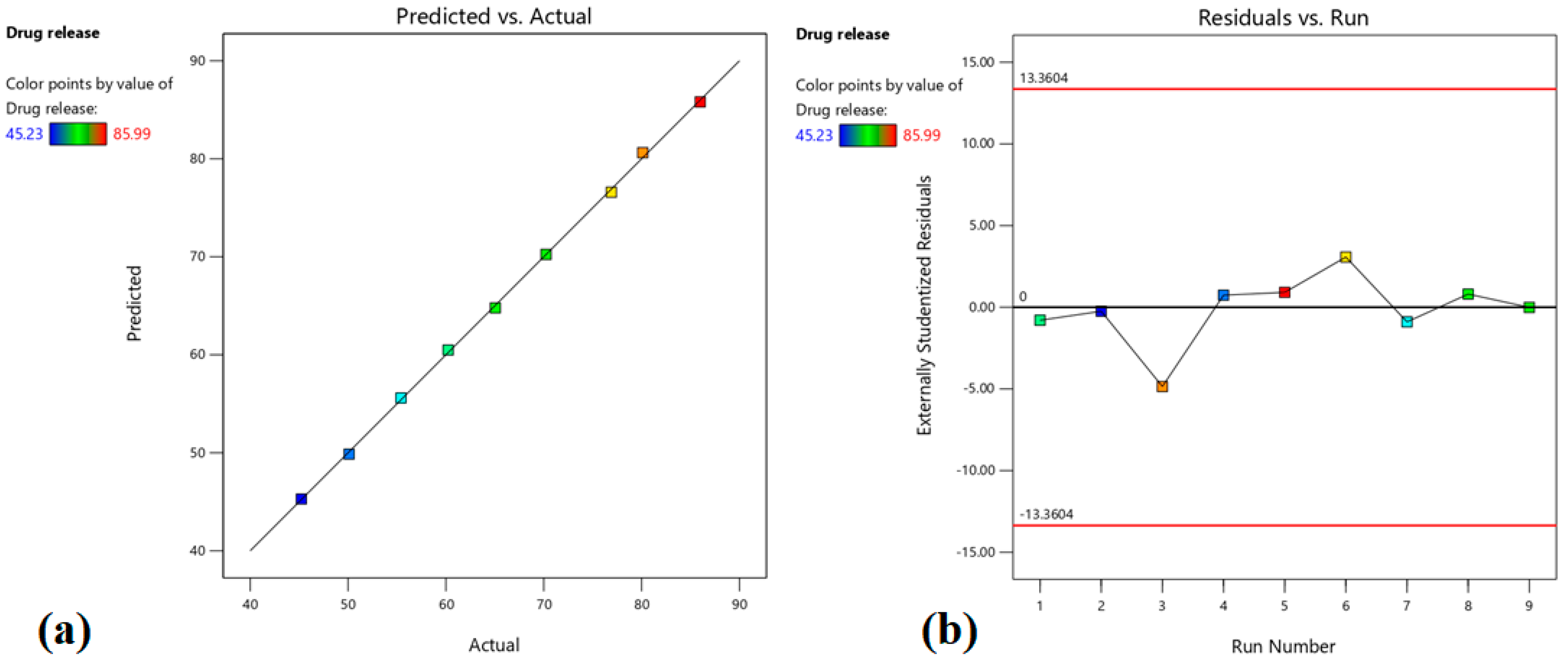
3.3.1. Effect on Drug Release
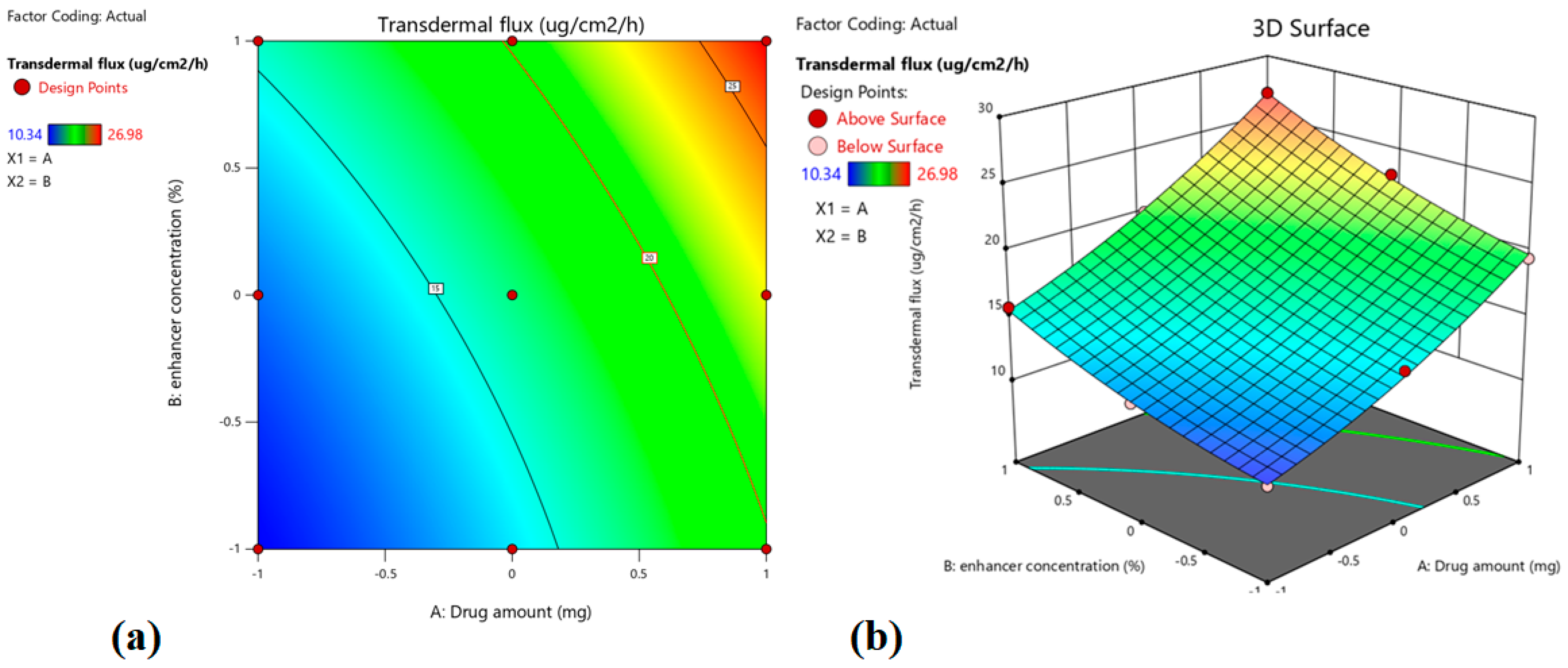
3.3.2. Effect on Transdermal Flux
3.3.3. Optimized Batch Selected by Point Prediction
3.4. Characterization of Transdermal Patch
3.4.1. Drug Content
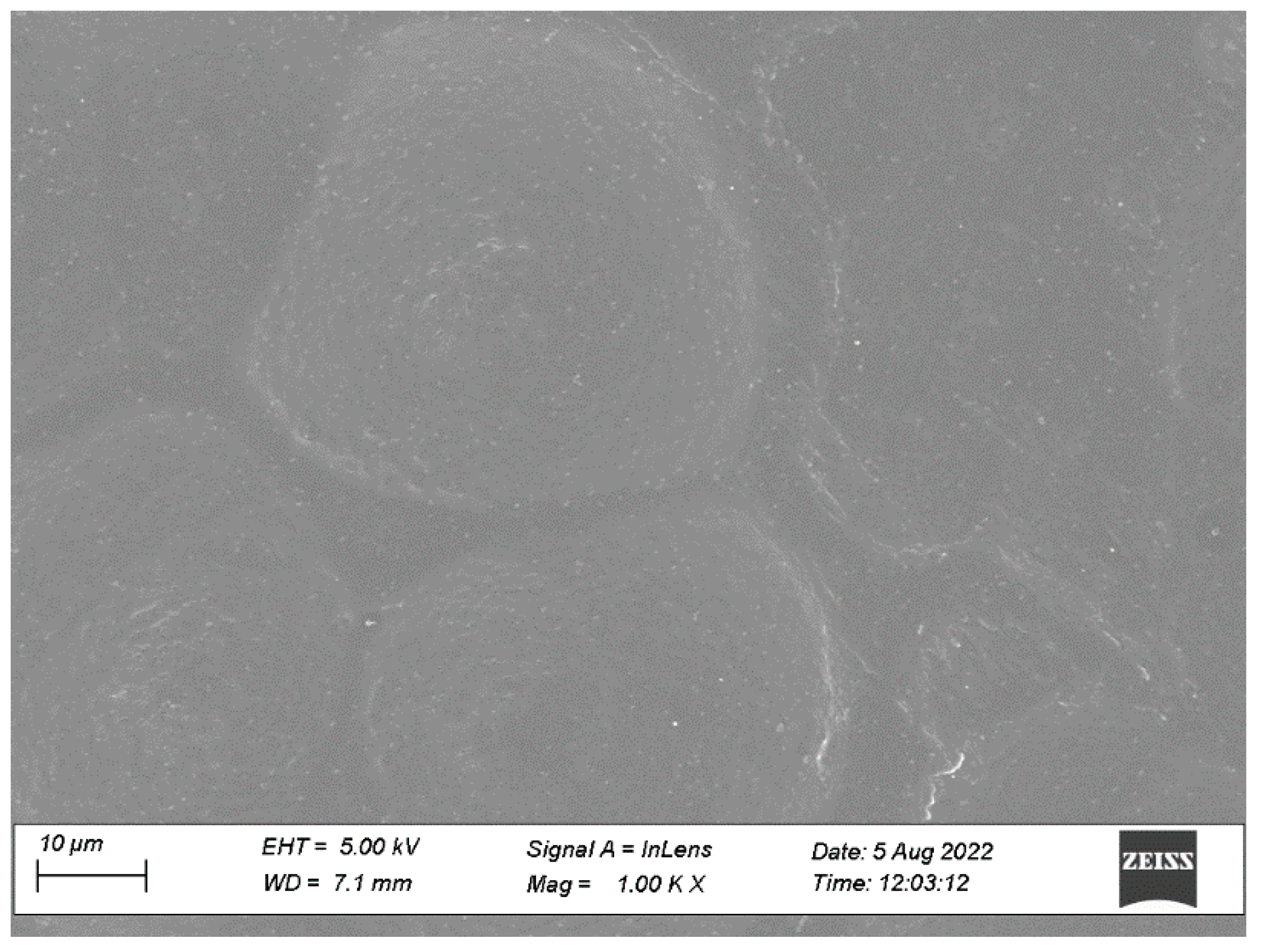
3.4.2. Microscopic Observations
3.4.3. FTIR Study
3.4.4. DSC
3.4.5. Coat Weight
3.4.6. Adhesion Testing
3.5. Skin Irritation
3.6. In Vivo Study
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Levine, D.J. Pulmonary arterial hypertension: Updates in epidemiology and evaluation of patients. Am. J. Manag. Care 2021, 27, S35–S41. [Google Scholar] [CrossRef] [PubMed]
- Luna-López, R.; Ruiz Martín, A.; Escribano Subías, P. Pulmonary arterial hypertension. Med. Clin. 2022, 158, 622–629. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, V.V.; Shah, S.J.; Souza, R.; Humbert, M. Management of pulmonary arterial hypertension. J. Am. Coll. Cardiol. 2015, 65, 1976–1997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruopp, N.F.; Cockrill, B.A. Diagnosis and Treatment of Pulmonary Arterial Hypertension: A Review. JAMA 2022, 327, 1379–1391. [Google Scholar] [CrossRef]
- Lindegaard Pedersen, M.; Krüger, M.; Grimm, D.; Infanger, M.; Wehland, M. The prostacyclin analogue treprostinil in the treatment of pulmonary arterial hypertension. Basic Clin. Pharmacol. Toxicol. 2020, 126, 32–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapman, R.W.; Corboz, M.R.; Malinin, V.S.; Plaunt, A.J.; Konicek, D.M.; Li, Z.; Perkins, W.R. An overview of the biology of a long-acting inhaled treprostinil prodrug. Pulm. Pharmacol. Ther. 2020, 65, 102002. [Google Scholar] [CrossRef]
- Kumar, P.; Thudium, E.; Laliberte, K.; Zaccardelli, D.; Nelsen, A. A Comprehensive Review of Treprostinil Pharmacokinetics via Four Routes of Administration. Clin. Pharmacokinet. 2016, 55, 1495–1505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leifer, F.G.; Konicek, D.M.; Chen, K.J.; Plaunt, A.J.; Salvail, D.; Laurent, C.E.; Corboz, M.R.; Li, Z.; Chapman, R.W.; Perkins, W.R.; et al. Inhaled Treprostinil-Prodrug Lipid Nanoparticle Formulations Provide Long-Acting Pulmonary Vasodilation. Drug Res. 2018, 68, 605–614. [Google Scholar] [CrossRef] [Green Version]
- Otani, N.; Tomoe, T.; Kawabe, A.; Sugiyama, T.; Horie, Y.; Sugimura, H.; Yasu, T.; Nakamoto, T. Recent Advances in the Treatment of Pulmonary Arterial Hypertension. Pharmaceuticals 2022, 15, 1277. [Google Scholar] [CrossRef]
- Torres, F.; Rubin, L.J. Treprostinil for the treatment of pulmonary arterial hypertension. Expert Rev. Cardiovasc. Ther. 2013, 11, 13–25. [Google Scholar] [CrossRef]
- Skoro-Sajer, N.; Lang, I. Extended-release oral treprostinil for the treatment of pulmonary arterial hypertension. Expert Rev. Cardiovasc. Ther. 2014, 12, 1391–1399. [Google Scholar] [CrossRef] [PubMed]
- Leong, E.W.X.; Ge, R. Lipid Nanoparticles as Delivery Vehicles for Inhaled Therapeutics. Biomedicines 2022, 10, 2179. [Google Scholar] [CrossRef] [PubMed]
- Anselmo, A.C.; Gokarn, Y.; Mitragotri, S. Non-invasive delivery strategies for biologics. Nat. Rev. Drug Discov. 2019, 18, 19–40. [Google Scholar] [CrossRef] [PubMed]
- Alkilani, A.Z.; McCrudden, M.T.; Donnelly, R.F. Transdermal Drug Delivery: Innovative Pharmaceutical Developments Based on Disruption of the Barrier Properties of the stratum corneum. Pharmaceutics 2015, 7, 438–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akhtar, N.; Singh, V.; Yusuf, M.; Khan, R.A. Non-invasive drug delivery technology: Development and current status of transdermal drug delivery devices, techniques and biomedical applications. Biomed. Tech. Biomed. Eng. 2020, 65, 243–272. [Google Scholar] [CrossRef] [Green Version]
- Bird, D.; Ravindra, N.M. Transdermal drug delivery and patches—An overview. Med. Devices Sens. 2020, 3, e10069. [Google Scholar] [CrossRef]
- Liu, C.; Quan, P.; Fang, L. Effect of drug physicochemical properties on drug release and their relationship with drug skin permeation behaviors in hydroxyl pressure sensitive adhesive. Eur. J. Pharm. Sci. Off. J. Eur. Fed. Pharm. Sci. 2016, 93, 437–446. [Google Scholar] [CrossRef]
- Luo, Z.; Liu, C.; Quan, P.; Zhang, Y.; Fang, L. Effect of Chemical Penetration Enhancer-Adhesive Interaction on Drug Release from Transdermal Patch: Mechanism Study Based on FT-IR Spectroscopy, (13)C NMR Spectroscopy, and Molecular Simulation. AAPS PharmSciTech 2021, 22, 198. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.B.; Jacob, S.; Al-Dhubiab, B.E.; Alhumam, R.N. Influence of skin permeation enhancers on the transdermal delivery of palonosetron: An in vitro evaluation. J. Appl. Biomed. 2018, 16, 192–197. [Google Scholar] [CrossRef]
- Weng, W.; Quan, P.; Liu, C.; Zhao, H.; Fang, L. Design of a Drug-in-Adhesive Transdermal Patch for Risperidone: Effect of Drug-Additive Interactions on the Crystallization Inhibition and In Vitro/In Vivo Correlation Study. J. Pharm. Sci. 2016, 105, 3153–3161. [Google Scholar] [CrossRef]
- Ganti, S.S.; Bhattaccharjee, S.A.; Murnane, K.S.; Blough, B.E.; Banga, A.K. Formulation and evaluation of 4-benzylpiperidine drug-in-adhesive matrix type transdermal patch. Int. J. Pharm. 2018, 550, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Hui, M.; Quan, P.; Fang, L. Drug in adhesive patch of palonosetron: Effect of pressure sensitive adhesive on drug skin permeation and in vitro-in vivo correlation. Int. J. Pharm. 2016, 511, 1088–1097. [Google Scholar] [CrossRef] [PubMed]
- Al Hanbali, O.A.; Khan, H.M.S.; Sarfraz, M.; Arafat, M.; Ijaz, S.; Hameed, A. Transdermal patches: Design and current approaches to painless drug delivery. Acta Pharm. 2019, 69, 197–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nair, A.B.; Gupta, S.; Al-Dhubiab, B.E.; Jacob, S.; Shinu, P.; Shah, J.; Morsy, M.A.; SreeHarsha, N.; Attimarad, M.; Venugopala, K.N.; et al. Effective therapeutic delivery and bioavailability enhancement of pioglitazone using drug in adhesive transdermal patch. Pharmaceutics 2019, 11, 359. [Google Scholar] [CrossRef]
- Agyralides, G.G.; Dallas, P.P.; Rekkas, D.M. Development and in vitro evaluation of furosemide transdermal formulations using experimental design techniques. Int. J. Pharm. 2004, 281, 35–43. [Google Scholar] [CrossRef]
- Nair, A.B.; Shah, J.; Aljaeid, B.M.; Al-Dhubiab, B.E.; Jacob, S. Gellan gum-based hydrogel for the transdermal delivery of nebivolol: Optimization and evaluation. Polymers 2019, 11, 1699. [Google Scholar] [CrossRef] [Green Version]
- Nair, A.; Gupta, R.; Vasanti, S. In vitro controlled release of alfuzosin hydrochloride using HPMC-based matrix tablets and its comparison with marketed product. Pharm. Dev. Technol. 2007, 12, 621–625. [Google Scholar] [CrossRef]
- Shah, H.; Nair, A.B.; Shah, J.; Bharadia, P.; Al-Dhubiab, B.E. Proniosomal gel for transdermal delivery of lornoxicam: Optimization using factorial design and in vivo evaluation in rats. DARU J. Pharm. Sci. 2019, 27, 59–70. [Google Scholar] [CrossRef]
- Shah, J.; Nair, A.B.; Shah, H.; Jacob, S.; Shehata, T.M.; Morsy, M.A. Enhancement in antinociceptive and anti-inflammatory effects of tramadol by transdermal proniosome gel. Asian J. Pharm. Sci. 2020, 15, 786–796. [Google Scholar] [CrossRef]
- Arunprasert, K.; Pornpitchanarong, C.; Rojanarata, T.; Ngawhirunpat, T.; Opanasopit, P.; Aumklad, P.; Patrojanasophon, P. Development and Evaluation of Novel Water-Based Drug-in-Adhesive Patches for the Transdermal Delivery of Ketoprofen. Pharmaceutics 2021, 13, 789. [Google Scholar] [CrossRef]
- Cilurzo, F.; Minghetti, P.; Gennari, C.G.; Casiraghi, A.; Selmin, F.; Montanari, L. Formulation study of a patch containing propranolol by design of experiments. Drug Dev. Ind. Pharm. 2014, 40, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.B.; Kumria, R.; Al-Dhubiab, B.E.; Attimarad, M.; Harsha, S. Development of transdermal delivery system of vildagliptin and its comparison with oral therapy. Indian J. Pharm. Educ. Res. 2016, 50, 130–137. [Google Scholar] [CrossRef] [Green Version]
- Su, Y.; Lu, W.; Fu, X.; Xu, Y.; Ye, L.; Yang, J.; Huang, H.; Yu, C. Formulation and Pharmacokinetic Evaluation of a Drug-in-Adhesive Patch for Transdermal Delivery of Koumine. AAPS PharmSciTech 2020, 21, 297. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.; Vyas, H.; Shah, J.; Kumar, A. Effect of permeation enhancers on the iontophoretic transport of metoprolol tartrate and the drug retention in skin. Drug Deliv. 2011, 18, 19–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nair, A.B.; Sammeta, S.M.; Vaka, S.R.; Narasimha Murthy, S. A study on the effect of inorganic salts in transungual drug delivery of terbinafine. J. Pharm. Pharmacol. 2009, 61, 431–437. [Google Scholar] [CrossRef]
- Barry, B.W. Mode of action of penetration enhancers in human skin. J. Control. Release 1987, 6, 85–97. [Google Scholar] [CrossRef]
- Chen, X.; Wang, Y.; Cheng, Z.; Wei, J.; Shi, Y.; Qian, J. Diffusion Behavior of Drug Molecules in Acrylic Pressure-Sensitive Adhesive. ACS Omega 2020, 5, 9408–9419. [Google Scholar] [CrossRef]
- Vora, N.; Lin, S.; Madan, P. Development and in-vitro evaluation of an optimized carvedilol transdermal therapeutic system using experimental design approach. Asian J. Pharm. Sci. 2013, 8, 28–38. [Google Scholar] [CrossRef] [Green Version]
- Jafri, I.; Shoaib, M.H.; Yousuf, R.I.; Ali, F.R. Effect of permeation enhancers on in vitro release and transdermal delivery of lamotrigine from Eudragit(®)RS100 polymer matrix-type drug in adhesive patches. Prog. Biomater. 2019, 8, 91–100. [Google Scholar] [CrossRef] [Green Version]
- Corsaro, C.; Neri, G.; Mezzasalma, A.M.; Fazio, E. Weibull Modeling of Controlled Drug Release from Ag-PMA Nanosystems. Polymers 2021, 13, 2897. [Google Scholar] [CrossRef]
- Souto, E.B.; Fangueiro, J.F.; Fernandes, A.R.; Cano, A.; Sanchez-Lopez, E.; Garcia, M.L.; Severino, P.; Paganelli, M.O.; Chaud, M.V.; Silva, A.M. Physicochemical and biopharmaceutical aspects influencing skin permeation and role of SLN and NLC for skin drug delivery. Heliyon 2022, 8, e08938. [Google Scholar] [CrossRef] [PubMed]
- Jeong, W.Y.; Kwon, M.; Choi, H.E.; Kim, K.S. Recent advances in transdermal drug delivery systems: A review. Biomater. Res. 2021, 25, 24. [Google Scholar] [CrossRef] [PubMed]
- Kováčik, A.; Kopečná, M.; Vávrová, K. Permeation enhancers in transdermal drug delivery: Benefits and limitations. Expert Opin. Drug Deliv. 2020, 17, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Kriplani, P.; Guarve, K.; Singh Baghel, U. Formulation optimization and characterization of transdermal film of curcumin by response surface methodology. Chin. Herb. Med. 2021, 13, 274–285. [Google Scholar] [CrossRef]
- Agrawal, M.B.; Patel, M.M. Optimization and in vivo evaluation of quetiapine-loaded transdermal drug delivery system for the treatment of schizophrenia. Drug Dev. Ind. Pharm. 2020, 46, 1819–1831. [Google Scholar] [CrossRef]
- Cai, Y.; Tian, Q.; Liu, C.; Fang, L. Development of long-acting rivastigmine drug-in-adhesive patch utilizing ion-pair strategy and characterization of controlled release mechanism. Eur. J. Pharm. Sci. Off. J. Eur. Fed. Pharm. Sci. 2021, 161, 105774. [Google Scholar] [CrossRef]
- Mikolaszek, B.; Jamrógiewicz, M.; Mojsiewicz-Pieńkowska, K.; Sznitowska, M. Microscopic and Spectroscopic Imaging and Thermal Analysis of Acrylates, Silicones and Active Pharmaceutical Ingredients in Adhesive Transdermal Patches. Polymers 2022, 14, 2888. [Google Scholar] [CrossRef]
- Wei, S.-Y.; Jheng, J.-B.; Hsu, M.-K.; Hsu, M.-K.; Wei, T.-M. Efficient crystallization process for preparing ultrapure Treprostinil and crystal prepared therefrom. U.S. Patent 11,339,110, 24 May 2022. [Google Scholar]
- Terao, K. Poly(acrylic acid) (PAA). In Encyclopedia of Polymeric Nanomaterials; Kobayashi, S., Müllen, K., Eds.; Springer: Berlin/Heidelberg, Germany, 2021; pp. 1–6. [Google Scholar]
- Parhi, R.; Padilam, S. In vitro permeation and stability studies on developed drug-in-adhesive transdermal patch of simvastatin. Bull. Fac. Pharm. Cairo Univ. 2018, 56, 26–33. [Google Scholar] [CrossRef]
- Bozorg, B.D.; Banga, A.K. Effect of Different Pressure-Sensitive Adhesives on Performance Parameters of Matrix-Type Transdermal Delivery Systems. Pharmaceutics 2020, 12, 209. [Google Scholar] [CrossRef] [Green Version]
- Cilurzo, F.; Gennari, C.G.; Minghetti, P. Adhesive properties: A critical issue in transdermal patch development. Expert Opin. Drug Deliv. 2012, 9, 33–45. [Google Scholar] [CrossRef]
- Musazzi, U.M.; Ortenzi, M.A.; Gennari, C.G.M.; Casiraghi, A.; Minghetti, P.; Cilurzo, F. Design of pressure-sensitive adhesive suitable for the preparation of transdermal patches by hot-melt printing. Int. J. Pharm. 2020, 586, 119607. [Google Scholar] [CrossRef] [PubMed]
- Hai, N.T.; Kim, J.; Park, E.-S.; Chi, S.-C. Formulation and biopharmaceutical evaluation of transdermal patch containing benztropine. Int. J. Pharm. 2008, 357, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Tuntiyasawasdikul, S.; Limpongsa, E.; Jaipakdee, N.; Sripanidkulchai, B. A monolithic drug-in-adhesive patch of methoxyflavones from Kaempferia parviflora: In vitro and in vivo evaluation. Int. J. Pharm. 2015, 478, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Quaroni, G.M.G.; Gennari, C.G.M.; Cilurzo, F.; Ducouret, G.; Creton, C.; Minghetti, P. Tuning the rheological properties of an ammonium methacrylate copolymer for the design of adhesives suitable for transdermal patches. Eur. J. Pharm. Sci. Off. J. Eur. Fed. Pharm. Sci. 2018, 111, 238–246. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors, Response | Level Used, Actual Coded | ||
|---|---|---|---|
| Low (−1) | Medium (0) | High (+1) | |
| Independent variables | |||
| X1 = Drug amount (%, w/w) | 0.3 | 0.5 | 0.7 |
| X2 = Enhancer concentration (%, w/w) | 3 | 5 | 7 |
| Dependent variables | Targets | ||
| Y1 = Drug release (%) | Maximum | ||
| Y2 = Transdermal flux (µg/cm2/h) | Maximum | ||
| Batch | Factor 1 | Factor 2 |
|---|---|---|
| X1: Drug Amount (%) | X2: Enhancer Concentration (%) | |
| F1 | 0 | −1 |
| F2 | −1 | −1 |
| F3 | 1 | 0 |
| F4 | −1 | 0 |
| F5 | 1 | 1 |
| F6 | 1 | −1 |
| F7 | −1 | 1 |
| F8 | 0 | 0 |
| F9 | 0 | 1 |
| Batch Number | Factor 1 | Factor 2 | Response 1 | Response 2 |
|---|---|---|---|---|
| X1: Drug Amount (%, w/w) | X2: Enhancer Concentration (%, w/w) | Y1: Drug Release (%) | Y2: Transdermal Flux (µg/cm2/h) | |
| F1 | 0.5 | 3 | 60.23 | 14.54 |
| F2 | 0.3 | 3 | 45.23 | 10.34 |
| F3 | 0.7 | 5 | 80.12 | 22.96 |
| F4 | 0.3 | 5 | 50.11 | 12.12 |
| F5 | 0.7 | 7 | 85.99 | 26.98 |
| F6 | 0.7 | 3 | 76.91 | 19.45 |
| F7 | 0.3 | 7 | 55.41 | 15.67 |
| F8 | 0.5 | 5 | 65.05 | 16.28 |
| F9 | 0.5 | 7 | 70.24 | 19.98 |
| Y1 (Drug Release) % | Y2 (Transdermal Flux) µg/cm2/h | ||
|---|---|---|---|
| Estimated | Observed | Estimated | Observed |
| 80.621 | 81.341 ± 4.93 | 23.279 | 23.259 ± 3.54 |
| Wave Numbers (cm−1) | Functional Groups |
|---|---|
| 3517 | O-H stretching-alcohol |
| 3278 | O-H stretching-carboxylic acid |
| 2923 | C-H stretching |
| 1707 | C=O stretching |
| 1585 | C=C stretching |
| 1469 | C-H bending |
| 1346 | O-H bending |
| 1261 | C-O stretching |
| 1114 | C-O stretching—secondary alcohol |
| 1025, 898, 732 | C=C bending |
| Parameters | Treprostinil Suspension (Mean ± SD) | Treprostinil Transdermal Patch (Mean ± SD) |
|---|---|---|
| Cmax (ng/mL) | 284.87 ± 19.44 | 259.75 ± 21.28 |
| Tmax (h) | 1 | 4 |
| AUC0-α (ng.h/mL) | 1351.49 ± 106.43 | 3977.11 ± 287.65 * |
| Relative bioavailability (%) | 100 | 237 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alissa, I.; Nair, A.B.; Aldhubiab, B.; Shah, H.; Shah, J.; Mewada, V.; Almuqbil, R.M.; Jacob, S. Design, Development, and Evaluation of Treprostinil Embedded Adhesive Transdermal Patch. Pharmaceutics 2023, 15, 1226. https://doi.org/10.3390/pharmaceutics15041226
Alissa I, Nair AB, Aldhubiab B, Shah H, Shah J, Mewada V, Almuqbil RM, Jacob S. Design, Development, and Evaluation of Treprostinil Embedded Adhesive Transdermal Patch. Pharmaceutics. 2023; 15(4):1226. https://doi.org/10.3390/pharmaceutics15041226
Chicago/Turabian StyleAlissa, Ibrahim, Anroop B. Nair, Bandar Aldhubiab, Hiral Shah, Jigar Shah, Vivek Mewada, Rashed M. Almuqbil, and Shery Jacob. 2023. "Design, Development, and Evaluation of Treprostinil Embedded Adhesive Transdermal Patch" Pharmaceutics 15, no. 4: 1226. https://doi.org/10.3390/pharmaceutics15041226