
From Personalized to Precision Medicine in Oncology: A Model-Based Dosing Approach to Optimize Achievement of Imatinib Target Exposure

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Pharmacokinetic Model
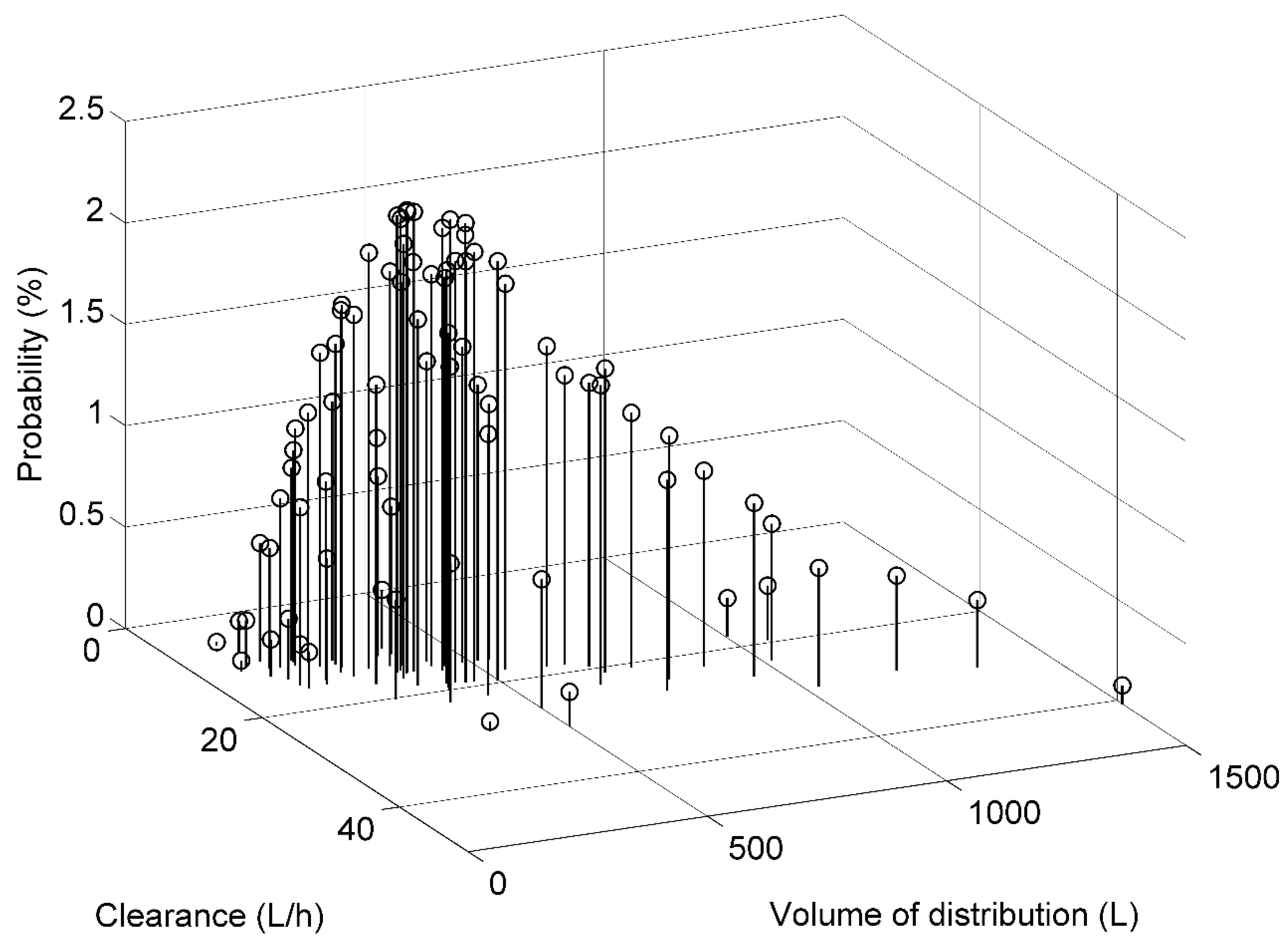
2.2. Model Discretization
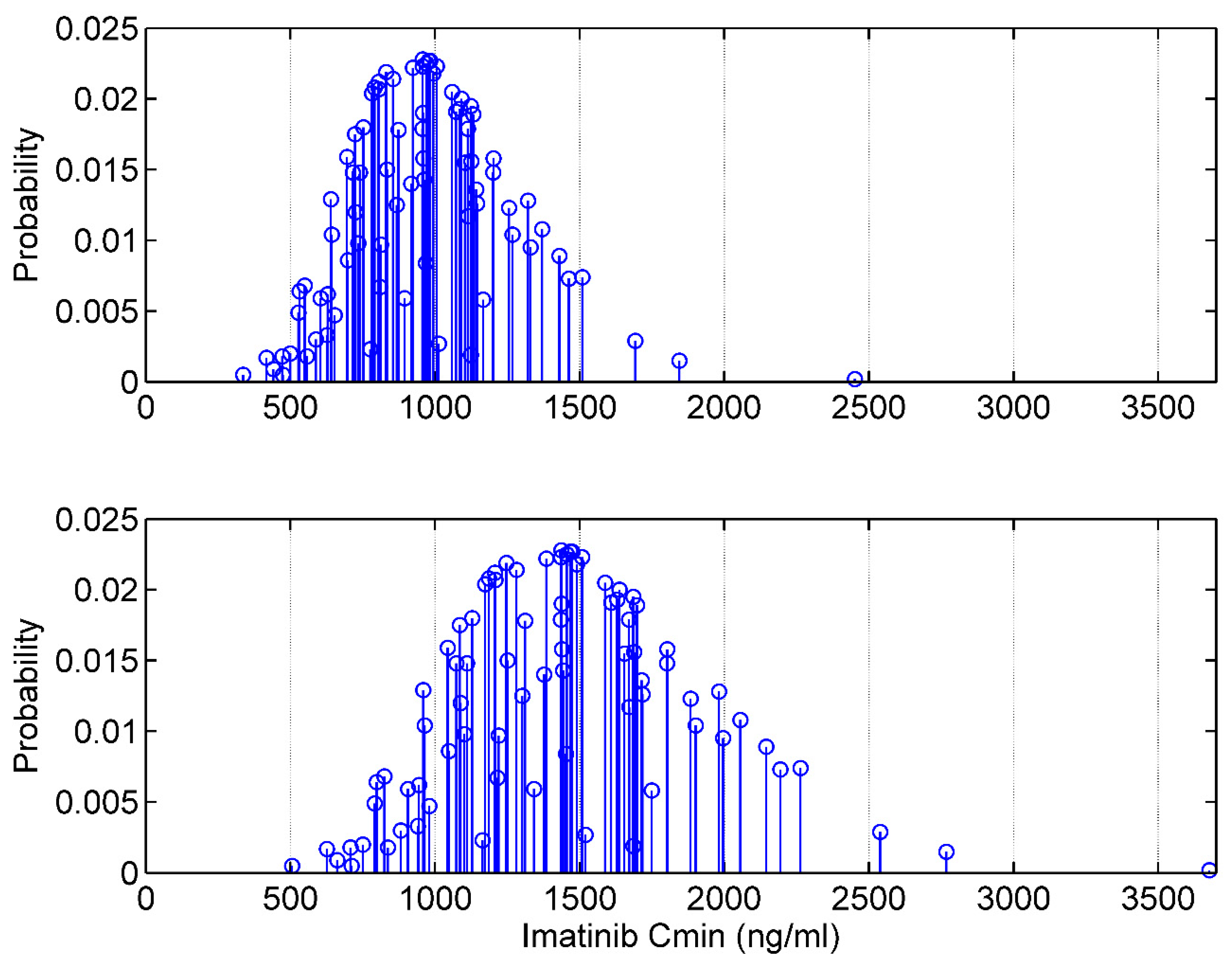
2.3. The Target Interval Dosing (TID) Approach
2.4. Dosing Based on the Traditional Model-Based Approach
2.5. Evaluation of TID and Other Dosing Methods in Simulated Patients
- -
- ODint, the dosage maximizing the attainment of the target interval as defined in Equation (8);
- -
- ODLmin, the dosage minimizing underexposure (Cmin < L, see Equation (10));
- -
- ODL5%, the dosage associated with a priori probability of underexposure less than 5% (Equation (11)).
2.6. Evaluation of TID and Other Dosing Methods Based on Data from Real Patients
2.7. Model-Based Dosing Recommendations
2.8. Software Tools
3. Results
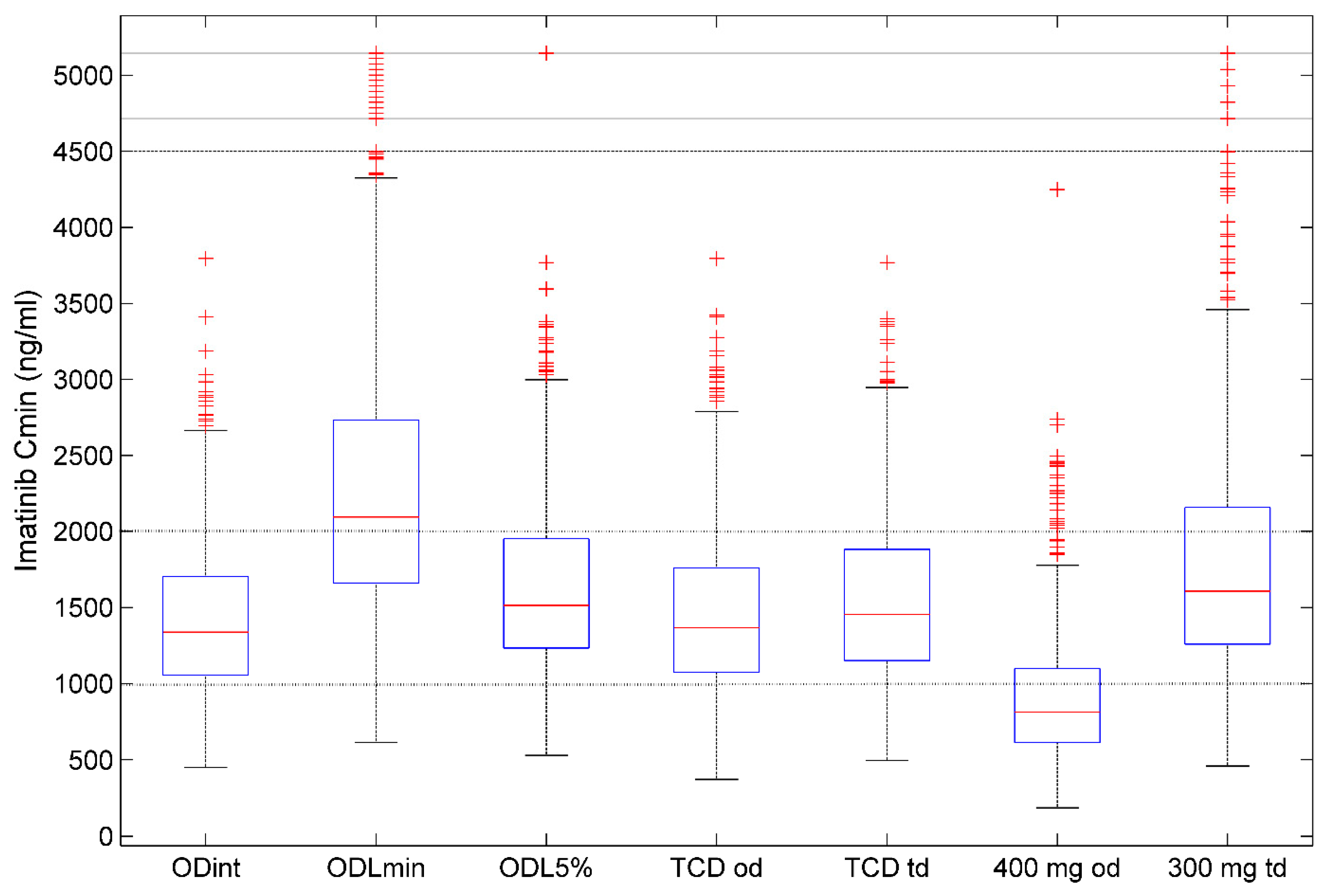
3.1. Imatinib Dosing and Target Attainment in Simulated Patients
3.2. Performance of Imatinib Dosing Methods Based on Real Patients’ Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Capdeville, R.; Buchdunger, E.; Zimmermann, J.; Matter, A. Glivec (STI571, imatinib), a rationally developed, targeted anticancer drug. Nat. Rev. Drug Discov. 2002, 1, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Demetri, G.D.; von Mehren, M.; Blanke, C.D.; Van den Abbeele, A.D.; Eisenberg, B.; Roberts, P.J.; Heinrich, M.C.; Tuveson, D.A.; Singer, S.; Janicek, M.; et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N. Engl. J. Med. 2002, 347, 472–480. [Google Scholar] [CrossRef] [Green Version]
- Druker, B.J.; Guilhot, F.; O’Brien, S.G.; Gathmann, I.; Kantarjian, H.; Gattermann, N.; Deininger, M.W.; Silver, R.T.; Goldman, J.M.; Stone, R.M.; et al. Five-year follow-up of patients receiving imatinib for chronic myeloid leukemia. N. Engl. J. Med. 2006, 355, 2408–2417. [Google Scholar] [CrossRef] [PubMed]
- Maggiora, G. Is imatinib a prototypical example of targeted drug therapy? Future Med. Chem. 2016, 8, 1907–1911. [Google Scholar] [CrossRef] [PubMed]
- Schilsky, R.L. Personalized medicine in oncology: The future is now. Nat. Rev. Drug Discov. 2010, 9, 363–366. [Google Scholar] [CrossRef]
- Kalia, M. Personalized oncology: Recent advances and future challenges. Metab. Clin. Exp. 2013, 62 (Suppl. 1), S11–S14. [Google Scholar] [CrossRef]
- Joyner, M.J.; Paneth, N. Seven Questions for Personalized Medicine. JAMA 2015, 314, 999–1000. [Google Scholar] [CrossRef]
- Collins, F.S.; Varmus, H. A new initiative on precision medicine. N. Engl. J. Med. 2015, 372, 793–795. [Google Scholar] [CrossRef] [Green Version]
- Darwich, A.S.; Ogungbenro, K.; Vinks, A.A.; Powell, J.R.; Reny, J.L.; Marsousi, N.; Daali, Y.; Fairman, D.; Cook, J.; Lesko, L.J.; et al. Why has model-informed precision dosing not yet become common clinical reality? lessons from the past and a roadmap for the future. Clin. Pharmacol. Ther. 2017, 101, 646–656. [Google Scholar] [CrossRef]
- Neely, M. Scalpels not hammers: The way forward for precision drug prescription. Clin. Pharmacol. Ther. 2017, 101, 368–372. [Google Scholar] [CrossRef]
- Peng, B.; Lloyd, P.; Schran, H. Clinical pharmacokinetics of imatinib. Clin. Pharmacokinet. 2005, 44, 879–894. [Google Scholar] [CrossRef] [PubMed]
- Stegmeier, F.; Warmuth, M.; Sellers, W.R.; Dorsch, M. Targeted cancer therapies in the twenty-first century: Lessons from imatinib. Clin. Pharmacol. Ther. 2010, 87, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Kantarjian, H.; Talpaz, M.; O’Brien, S.; Garcia-Manero, G.; Verstovsek, S.; Giles, F.; Rios, M.B.; Shan, J.; Letvak, L.; Thomas, D.; et al. High-dose imatinib mesylate therapy in newly diagnosed Philadelphia chromosome-positive chronic phase chronic myeloid leukemia. Blood 2004, 103, 2873–2878. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.E.; Baccarani, M.; Guilhot, F.; Druker, B.J.; Branford, S.; Kim, D.W.; Pane, F.; Pasquini, R.; Goldberg, S.L.; Kalaycio, M.; et al. Phase III, randomized, open-label study of daily imatinib mesylate 400 mg versus 800 mg in patients with newly diagnosed, previously untreated chronic myeloid leukemia in chronic phase using molecular end points: Tyrosine kinase inhibitor optimization and selectivity study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 424–430. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, V.S.; Hasford, J.; Deininger, M.; Cortes, J.; Baccarani, M.; Hehlmann, R. Systematic review and meta-analysis of standard-dose imatinib vs. high-dose imatinib and second generation tyrosine kinase inhibitors for chronic myeloid leukemia. J. Cancer Res. Clin. Oncol. 2017, 143, 1311–1318. [Google Scholar] [CrossRef]
- Larson, R.A.; Druker, B.J.; Guilhot, F.; O’Brien, S.G.; Riviere, G.J.; Krahnke, T.; Gathmann, I.; Wang, Y. Imatinib pharmacokinetics and its correlation with response and safety in chronic-phase chronic myeloid leukemia: A subanalysis of the IRIS study. Blood 2008, 111, 4022–4028. [Google Scholar] [CrossRef] [Green Version]
- Picard, S.; Titier, K.; Etienne, G.; Teilhet, E.; Ducint, D.; Bernard, M.A.; Lassalle, R.; Marit, G.; Reiffers, J.; Begaud, B.; et al. Trough imatinib plasma levels are associated with both cytogenetic and molecular responses to standard-dose imatinib in chronic myeloid leukemia. Blood 2007, 109, 3496–3499. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, N.; Wakita, H.; Miura, M.; Scott, S.A.; Nishii, K.; Masuko, M.; Sakai, M.; Maeda, Y.; Ishige, K.; Kashimura, M.; et al. Correlation between imatinib pharmacokinetics and clinical response in Japanese patients with chronic-phase chronic myeloid leukemia. Clin. Pharmacol. Ther. 2010, 88, 809–813. [Google Scholar] [CrossRef]
- Demetri, G.D.; Wang, Y.; Wehrle, E.; Racine, A.; Nikolova, Z.; Blanke, C.D.; Joensuu, H.; von Mehren, M. Imatinib plasma levels are correlated with clinical benefit in patients with unresectable/metastatic gastrointestinal stromal tumors. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 3141–3147. [Google Scholar] [CrossRef]
- Garcia-Ferrer, M.; Wojnicz, A.; Mejia, G.; Koller, D.; Zubiaur, P.; Abad-Santos, F. Utility of Therapeutic Drug Monitoring of Imatinib, Nilotinib, and Dasatinib in Chronic Myeloid Leukemia: A Systematic Review and Meta-analysis. Clin. Ther. 2019, 41, 2558–2570.e2557. [Google Scholar] [CrossRef]
- Bouchet, S.; Titier, K.; Moore, N.; Lassalle, R.; Ambrosino, B.; Poulette, S.; Schuld, P.; Belanger, C.; Mahon, F.X.; Molimard, M. Therapeutic drug monitoring of imatinib in chronic myeloid leukemia: Experience from 1216 patients at a centralized laboratory. Fundam. Clin. Pharmacol. 2013, 27, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Bouchet, S.; Poulette, S.; Titier, K.; Moore, N.; Lassalle, R.; Abouelfath, A.; Italiano, A.; Chevreau, C.; Bompas, E.; Collard, O.; et al. Relationship between imatinib trough concentration and outcomes in the treatment of advanced gastrointestinal stromal tumours in a real-life setting. Eur. J. Cancer 2016, 57, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Gotta, V.; Bouchet, S.; Widmer, N.; Schuld, P.; Decosterd, L.A.; Buclin, T.; Mahon, F.X.; Csajka, C.; Molimard, M. Large-scale imatinib dose-concentration-effect study in CML patients under routine care conditions. Leuk. Res. 2014, 38, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Clarke, W.A.; Chatelut, E.; Fotoohi, A.K.; Larson, R.A.; Martin, J.H.; Mathijssen, R.H.J.; Salamone, S.J. Therapeutic Drug Monitoring in Oncology: International Association of Therapeutic Drug Monitoring and Clinical Toxicology Consensus Guidelines for Imatinib Therapy. Eur. J. Cancer 2021, 157, 428–440. [Google Scholar] [CrossRef] [PubMed]
- Zuidema, S.; Desar, I.M.E.; van Erp, N.P.; Kievit, W. Optimizing the dose in patients treated with imatinib as first line treatment for gastrointestinal stromal tumours: A cost-effectiveness study. Br. J. Clin. Pharmacol. 2019, 85, 1994–2001. [Google Scholar] [CrossRef] [PubMed]
- Widmer, N.; Decosterd, L.A.; Csajka, C.; Leyvraz, S.; Duchosal, M.A.; Rosselet, A.; Rochat, B.; Eap, C.B.; Henry, H.; Biollaz, J.; et al. Population pharmacokinetics of imatinib and the role of alpha-acid glycoprotein. Br. J. Clin. Pharmacol. 2006, 62, 97–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gotta, V.; Widmer, N.; Montemurro, M.; Leyvraz, S.; Haouala, A.; Decosterd, L.A.; Csajka, C.; Buclin, T. Therapeutic drug monitoring of imatinib: Bayesian and alternative methods to predict trough levels. Clin. Pharmacokinet. 2012, 51, 187–201. [Google Scholar] [CrossRef]
- Philippe, M.; Neely, M.; Bertrand, Y.; Bleyzac, N.; Goutelle, S. A Nonparametric Method to Optimize Initial Drug Dosing and Attainment of a Target Exposure Interval: Concepts and Application to Busulfan in Pediatrics. Clin. Pharmacokinet. 2017, 56, 435–447. [Google Scholar] [CrossRef]
- Katz, D.; D’Argenio, D.Z. Implementation and evaluation of control strategies for individualizing dosage regimens, with application to the aminoglycoside antibiotics. J. Pharmacokinet. Biopharm. 1986, 14, 523–537. [Google Scholar] [CrossRef]
- D’Argenio, D.Z.; Rodman, J.H. Targeting the systemic exposure of teniposide in the population and the individual using a stochastic therapeutic objective. J. Pharmacokinet. Biopharm. 1993, 21, 223–251. [Google Scholar] [CrossRef]
- Katz, D.; D’Argenio, D.Z. Discrete approximation of multivariate densities with application to Bayesian estimation. Comput. Stat. Data Anal. 1984, 2, 27–36. [Google Scholar] [CrossRef]
- Macdonald, I.; Staatz, C.E.; Jelliffe, R.W.; Thomson, A.H. Evaluation and comparison of simple multiple model, richer data multiple model, and sequential interacting multiple model (IMM) Bayesian analyses of gentamicin and vancomycin data collected from patients undergoing cardiothoracic surgery. Ther. Drug Monit. 2008, 30, 67–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holford, N.H. Target concentration intervention: Beyond Y2K. Br. J. Clin. Pharmacol. 1999, 48, 9–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claxton, A.J.; Cramer, J.; Pierce, C. A systematic review of the associations between dose regimens and medication compliance. Clin. Ther. 2001, 23, 1296–1310. [Google Scholar] [CrossRef]
- Overbeek, J.K.; Heine, R.T.; Verheul, H.M.W.; Chatelut, E.; Rudek, M.A.; Gurney, H.; Plummer, R.; Gilbert, D.C.; Buclin, T.; Burger, D.M.; et al. Off-label, but on target: The evidence needed to implement alternative dosing regimens of anticancer drugs. ESMO Open 2023, 8, 100749. [Google Scholar] [CrossRef]
- Yu, H.; Steeghs, N.; Nijenhuis, C.M.; Schellens, J.H.; Beijnen, J.H.; Huitema, A.D. Practical guidelines for therapeutic drug monitoring of anticancer tyrosine kinase inhibitors: Focus on the pharmacokinetic targets. Clin. Pharmacokinet. 2014, 53, 305–325. [Google Scholar] [CrossRef]
- Verheijen, R.B.; Yu, H.; Schellens, J.H.M.; Beijnen, J.H.; Steeghs, N.; Huitema, A.D.R. Practical Recommendations for Therapeutic Drug Monitoring of Kinase Inhibitors in Oncology. Clin. Pharmacol. Ther. 2017, 102, 765–776. [Google Scholar] [CrossRef]
- Farag, S.; Verheijen, R.B.; Martijn Kerst, J.; Cats, A.; Huitema, A.D.; Steeghs, N. Imatinib Pharmacokinetics in a Large Observational Cohort of Gastrointestinal Stromal Tumour Patients. Clin. Pharmacokinet. 2017, 56, 287–292. [Google Scholar] [CrossRef]
- Jelliffe, R.W.; Schumitzky, A.; Bayard, D.; Milman, M.; Van Guilder, M.; Wang, X.; Jiang, F.; Barbaut, X.; Maire, P. Model-based, goal-oriented, individualised drug therapy. Linkage of population modelling, new ‘multiple model’ dosage design, bayesian feedback and individualised target goals. Clin. Pharmacokinet. 1998, 34, 57–77. [Google Scholar] [CrossRef]
- Patel, J.N.; Papachristos, A. Personalizing chemotherapy dosing using pharmacological methods. Cancer Chemother. Pharmacol. 2015, 76, 879–896. [Google Scholar] [CrossRef]
- Buclin, T.; Thoma, Y.; Widmer, N.; Andre, P.; Guidi, M.; Csajka, C.; Decosterd, L.A. The Steps to Therapeutic Drug Monitoring: A Structured Approach Illustrated with Imatinib. Front. Pharmacol. 2020, 11, 177. [Google Scholar] [CrossRef] [PubMed]
- Gotta, V.; Buclin, T.; Csajka, C.; Widmer, N. Systematic review of population pharmacokinetic analyses of imatinib and relationships with treatment outcomes. Ther. Drug Monit. 2013, 35, 150–167. [Google Scholar] [CrossRef] [PubMed]
- Haouala, A.; Widmer, N.; Duchosal, M.A.; Montemurro, M.; Buclin, T.; Decosterd, L.A. Drug interactions with the tyrosine kinase inhibitors imatinib, dasatinib, and nilotinib. Blood 2011, 117, e75–e87. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TID-ODint | TID-ODLmin | TID-ODL5% | TCD q24h | TCD q12h | 400 mg/24 h | 600 mg/24 h | 200 mg/12 h | 300 mg/12 g | |
|---|---|---|---|---|---|---|---|---|---|
| Number of predictions | 800 | 800 | 791 a | 800 | 800 | 800 | 800 | 800 | 800 |
| Mean imatinib dose per dosing interval (mg) | NA | NA | NA | 683 (131) | 278 (68) | 400 | 600 | 200 | 300 |
| Mean Cmin (ng/mL) | 1420 | 2252 | 1624 | 1458 | 1553 | 902 | 1353 | 1182 | 1773 |
| Coefficient of variation of Cmin (%) | 35% | 39% | 35% | 37% | 36% | 48% | 48% | 44% | 44% |
| Median Cmin (ng/mL) | 1340 | 2087 | 1515 | 1365 | 1454 | 804 | 1205 | 1069 | 1603 |
| 5th and 95th percentiles of Cmin (ng/mL) | 755–2325 | 1118–3959 | 850–2727 | 739–2433 | 807–2626 | 398–1694 | 597–2541 | 559–2164 | 839–3245 |
| Cmin within target interval (%) | 66.0% | 43.1% | 66.2% | 64.5% | 64.6% | 29% | 54.7% | 49.3% | 56.6% |
| Cmin < 1000 ng/mL (%) | 20.2% | 2.8% | 10.9% | 18.9% | 15.6% | 68.2% | 32% | 43.2% | 13.4% |
| Cmin > 2000 ng/mL (%) | 13.8% | 54.1% | 22.9% | 16.6% | 19.8% | 2.8% | 13.3% | 7.3% | 30% |
| ODint | ODLmin | ODL5% | ||
|---|---|---|---|---|
| Dosing schedule a | q8h | 12% | 2.5% | 16.2% |
| q12h | 21% | 95.3% | 67.5% | |
| q24h | 67% | 2.2% | 16.3% | |
| Mean dose per dosing interval | q8h | 180 mg | 200 mg | 188 mg |
| q12h | 266 mg | 394 mg | 299 mg | |
| q24h | 639 mg | 611 mg | 581 mg | |
| Variable | Value |
|---|---|
| Number of females/males | 44/41 |
| Age (years) | 62 ± 13 (23–85) |
| Body weight (kg) | 71.2 ± 13.2 (48–100) |
| Imatinib clearance (L/h) | 12.9 ± 3.7 (2.6–24.4) |
| Imatinib volume of distribution (L) | 376 ± 146 (51–717) |
| TID-ODint | TID-ODLmin | TID-ODL5% | TCD q24h | TCD q12h | 400 mg/24 h | 600 mg/24 h | 200 mg/12 h | 300 mg/12 h | |
|---|---|---|---|---|---|---|---|---|---|
| Mean Cmin (ng/mL) | 1462 | 2369 | 1754 | 1514 | 1543 | 945 | 1417 | 1216 | 1824 |
| Coefficient of variation of Cmin (%) | 39% | 44% | 49% | 37% | 39% | 40% | 40% | 44% | 44% |
| Median Cmin (ng/mL) | 1303 | 2208 | 1547 | 1413 | 1344 | 886 | 1329 | 1130 | 1695 |
| 5th and 95th percentiles of Cmin (ng/mL) | 980–2144 | 1475–3744 | 1040–2944 | 1001–2109 | 966–2390 | 567–1488 | 851–2233 | 753–1896 | 1130–2845 |
| Cmin within target interval (%) | 75.3% | 36.5% | 64.7% | 80.0% | 72.9% | 16.5% | 65.9% | 51.8% | 72.9% |
| Cmin < 1100 ng/mL (%) | 16.5% | 0% | 9.4% | 11.8% | 14.1% | 82.3% | 24.7% | 45.9% | 3.5% |
| Cmin > 2000 ng/mL (%) | 8.2% | 63.5% | 25.9% | 8.2% | 13.0% | 1.2% | 9.4% | 2.3% | 23.6% |
| Age (Years) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Body Weight (kg) | 20 | 30 | 40 | 50 | 60 | 70 | 80 | 90 | ||||||||
| 40 | 400/12 | 300/12 | 300/12 | 800/24 | 300/12 | 700/24 | 700/24 | 600/24 | 600/24 | 200/12 | 600/24 | 400/24 | 200/12 | 400/24 | 400/24 | 300/24 |
| 300/12 | 700/24 | 800/24 | 600/24 | 700/24 | 200/12 | 600/24 | 500/24 | 500/24 | 400/24 | 500/24 | 300/24 | 400/24 | 100/12 | 300/24 | 200/24 | |
| 50 | 400/12 | 300/12 | 400/12 | 300/12 | 300/12 | 700/24 | 800/24 | 600/24 | 700/24 | 600/24 | 600/24 | 500/24 | 500/24 | 400/24 | 200/12 | 300/24 |
| 300/12 | 800/24 | 800/24 | 700/24 | 800/24 | 600/24 | 700/24 | 500/24 | 600/24 | 400/24 | 500/24 | 400/24 | 400/24 | 300/24 | 400/24 | 100/12 | |
| 60 | 400/12 | 400/12 | 400/12 | 300/12 | 300/12 | 800/24 | 800/24 | 700/24 | 800/24 | 600/24 | 700/24 | 500/24 | 600/24 | 400/24 | 500/24 | 400/24 |
| 400/12 | 300/12 | 300/12 | 800/24 | 300/12 | 700/24 | 700/24 | 200/12 | 600/24 | 500/24 | 600/24 | 400/24 | 200/12 | 300/24 | 400/24 | 300/24 | |
| 70 | 400/12 | 400/12 | 400/12 | 300/12 | 400/12 | 300/12 | 300/12 | 800/24 | 300/12 | 700/24 | 700/24 | 600/24 | 600/24 | 200/12 | 600/24 | 400/24 |
| 400/12 | 300/12 | 400/12 | 300/12 | 300/12 | 700/24 | 800/24 | 600/24 | 700/24 | 200/12 | 600/24 | 500/24 | 500/24 | 400/24 | 500/24 | 300/24 | |
| 80 | 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 300/12 | 400/12 | 300/12 | 300/12 | 700/24 | 800/24 | 600/24 | 700/24 | 600/24 | 600/24 | 500/24 |
| 400/12 | 400/12 | 400/12 | 300/12 | 300/12 | 800/24 | 800/24 | 700/24 | 800/24 | 600/24 | 700/24 | 500/24 | 600/24 | 400/24 | 500/24 | 400/24 | |
| 90 | 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 300/12 | 300/12 | 800/24 | 800/24 | 700/24 | 800/24 | 600/24 | 700/24 | 500/24 |
| 400/12 | 400/12 | 400/12 | 300/12 | 400/12 | 300/12 | 300/12 | 800/24 | 300/12 | 700/24 | 700/24 | 200/12 | 600/24 | 500/24 | 600/24 | 400/24 | |
| 100 | 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 300/12 | 400/12 | 300/12 | 300/12 | 800/24 | 300/12 | 700/24 | 700/24 | 600/24 |
| 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 300/12 | 400/12 | 300/12 | 300/12 | 700/24 | 800/24 | 600/24 | 700/24 | 200/12 | 600/24 | 500/24 | |
| 110 | 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 300/12 | 400/12 | 300/12 | 300/12 | 700/24 | 800/24 | 600/24 |
| 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 400/12 | 300/12 | 300/12 | 800/24 | 800/24 | 700/24 | 700/24 | 600/24 | 700/24 | 500/24 | |
| Man with CML | Woman with CML | |||||||||||||||
| Man with GIST | Woman with GIST | |||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goutelle, S.; Guidi, M.; Gotta, V.; Csajka, C.; Buclin, T.; Widmer, N. From Personalized to Precision Medicine in Oncology: A Model-Based Dosing Approach to Optimize Achievement of Imatinib Target Exposure. Pharmaceutics 2023, 15, 1081. https://doi.org/10.3390/pharmaceutics15041081
Goutelle S, Guidi M, Gotta V, Csajka C, Buclin T, Widmer N. From Personalized to Precision Medicine in Oncology: A Model-Based Dosing Approach to Optimize Achievement of Imatinib Target Exposure. Pharmaceutics. 2023; 15(4):1081. https://doi.org/10.3390/pharmaceutics15041081
Chicago/Turabian StyleGoutelle, Sylvain, Monia Guidi, Verena Gotta, Chantal Csajka, Thierry Buclin, and Nicolas Widmer. 2023. "From Personalized to Precision Medicine in Oncology: A Model-Based Dosing Approach to Optimize Achievement of Imatinib Target Exposure" Pharmaceutics 15, no. 4: 1081. https://doi.org/10.3390/pharmaceutics15041081