

Half a Century of Fragmented Research on Deviations from Advised Therapies: Is This a Good Time to Call for Multidisciplinary Medication Adherence Research Centres of Excellence?
 ,
,  , ,
, , (This article belongs to the Section Clinical Pharmaceutics)
Abstract
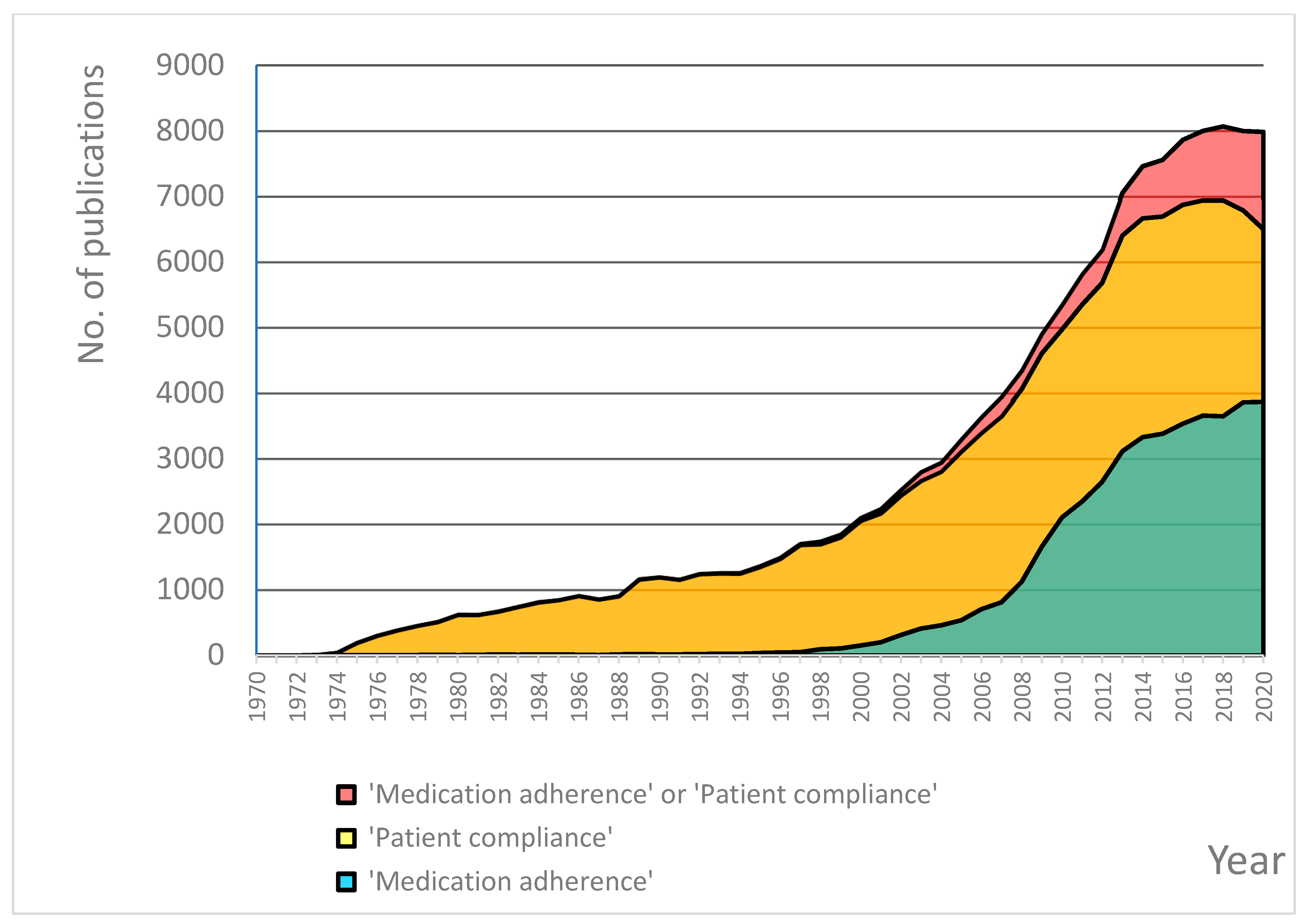
:1. Introduction
2. Scope of the Centre
- Educational centres;
- Clinical or health care centres;
- Research centres, which usually provide some educational and/or clinical services; however, research remains their dominant activity [16].
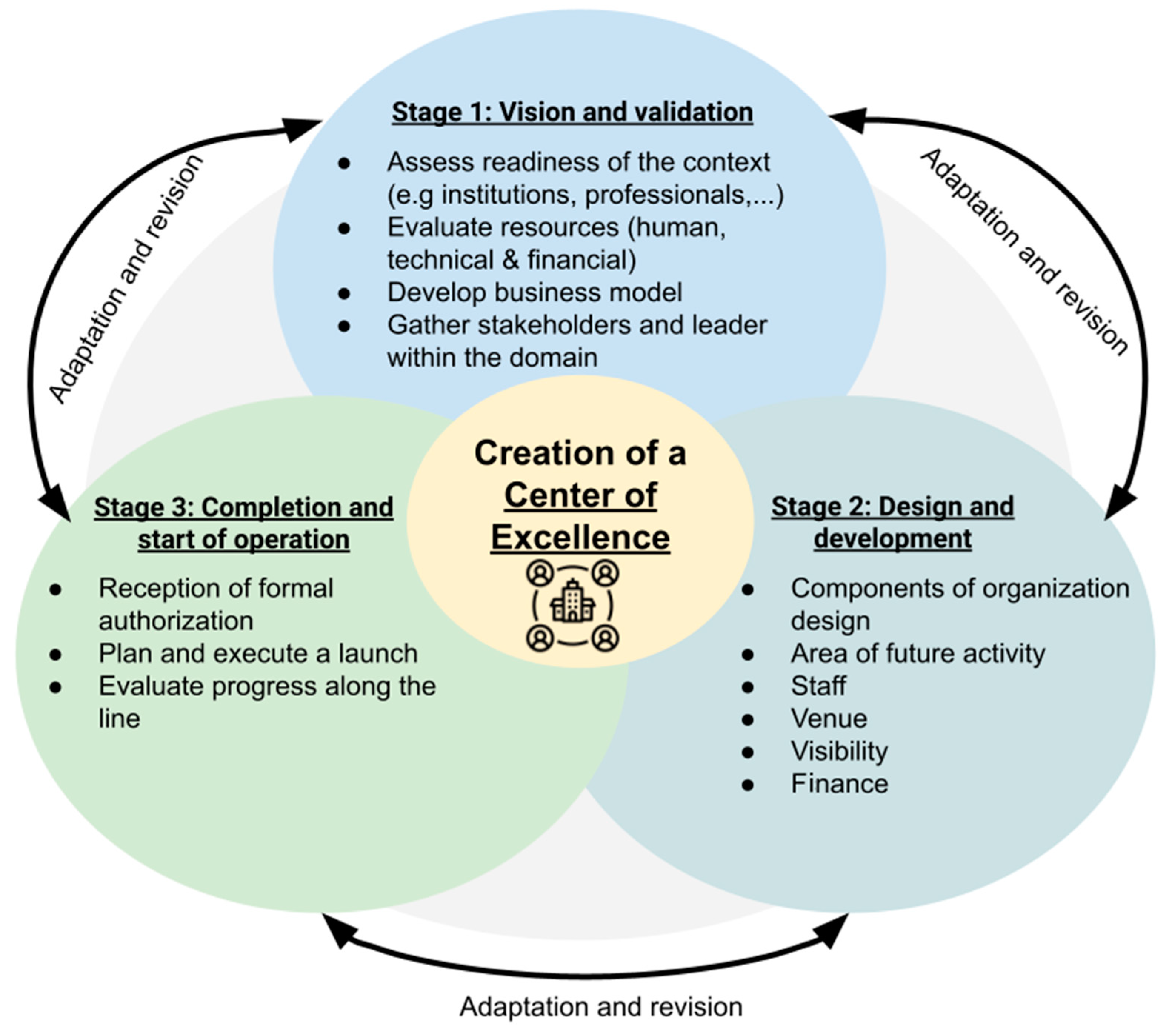
3. How to Create a Centre of Excellence?
3.1. Stage 1: Vision and Validation
| Mission | To design, execute and disseminate high-quality research in the area of medication adherence. |
| Vision | Medication Adherence Research CoE will be the leading regional/national source of high-quality evidence-based recommendations to guide scientific research, clinical practice, healthcare system organisation, and education in the area of medication adherence. |
| Values | Good research practice; Innovation. |
3.2. Stage 2: Design and Development
3.3. Stage 3: Completion and Start of Operation
- Affiliation—although a non-academic affiliation is potentially possible, it seems that a direct link to academia is a natural scenario for a research-oriented CoE. This, however, may create another challenge, as universities usually do not have established policies for developing centres of research excellence. Moreover, they may insist on refocusing the major area of CoE activity from research to education.
- Infrastructure—is it possible for CoE to obtain its own venue, equipment etc., or will it rather be a ‘virtual’ institution or platform within the umbrella organisation that shares or reuses its infrastructure?
- Budget—is it possible to guarantee a certain budget for the centre, or is it rather going to be funded by its activities, e.g., research grants, expert opinions, training, etc.?
4. Success Stories
5. Dutch Experience
6. Polish Experience
7. Lessons Learned
- (1)
- Is it necessary to meet specific predefined criteria for the creation of CoE? Both above-described CoEs benefit from the long-term commitment of their founding members to the area of medication adherence research, and they have been shaped according to an ‘organic’ evolutionary process. Therefore, their design is rather the consequence of locally available resources and historical reasons and is not necessarily informed by a set of predefined criteria. Of note, for medication adherence research CoEs, such criteria are not agreed upon yet. However, setting these criteria might be useful for potential new CoEs to come. Outside the medication adherence area, there are a few good practices that can serve as inspiration. For example, in software engineering, an assessment approach has been developed, which uses established scoring criteria and standards to certify an organisation [41].
- (2)
- How to secure a sufficient budget for the CoE? Adopted solutions included making as much as possible use of facilities existing in hospitals/academia, searching for external grants, and attracting both public and private funding.
- (3)
- How to assure good cohesion among CoE members if the CoE works across departments, within and outside the hospital? The way of addressing this challenge was to set up an efficient management structure, assure transparent communication, and complement each other’s expertise without rivalry.
- (4)
- Last but not least, how to increase the visibility of the CoE across the country and beyond? Actions taken to address this aim included press releases, organising a National Day of Medication adherence, creating an attractive website, scientific publications in high-impacted journals (using the affiliation of the CoE), and other methods of active targeting of different stakeholders, such as pharmaceutical and MedTech industry, healthcare professionals, patients, etc.
8. Looking Ahead
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sabate, E. (Ed.) Adherence to Long-Term Therapies Evidence for Action; World Health Organization: Geneva, Switzerland, 2003; pp. 1–196. [Google Scholar]
- van Boven, J.F.; Tsiligianni, I.; Potočnjak, I.; Mihajlović, J.; Dima, A.L.; Nabergoj Makovec, U.; Ágh, T.; Kardas, P.; Ghiciuc, C.M.; Petrova, G.; et al. European Network to Advance Best Practices and Technology on Medication Adherence: Mission Statement. Front. Pharmacol. 2021, 12, 748702. [Google Scholar] [CrossRef] [PubMed]
- Cutler, R.L.; Fernandez-Llimos, F.; Frommer, M.; Benrimoj, C.; Garcia-Cardenas, V. Economic impact of medication non-adherence by disease groups: A systematic review. BMJ Open 2018, 8, e016982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, C.A.; Cahir, C.; Tecklenborg, S.; Byrne, C.; Culbertson, M.A.; Bennett, K.E. The association between medication non-adherence and adverse health outcomes in ageing populations: A systematic review and meta-analysis. Br. J. Clin. Pharmacol. 2019, 85, 2464–2478. [Google Scholar] [CrossRef] [PubMed]
- Kurczewska-Michalak, M.; Lewek, P.; Jankowska-Polańska, B.; Giardini, A.; Granata, N.; Maffoni, M.; Costa, E.; Midão, L.; Kardas, P. Polypharmacy Management in the Older Adults: A Scoping Review of Available Interventions. Front. Pharmacol. 2021, 12, 734045. [Google Scholar] [CrossRef] [PubMed]
- Ágh, T.; van Boven, J.F.; Wettermark, B.; Menditto, E.; Pinnock, H.; Tsiligianni, I.; Petrova, G.; Potočnjak, I.; Kamberi, F.; Kardas, P. A Cross-Sectional Survey on Medication Management Practices for Noncommunicable Diseases in Europe During the Second Wave of the COVID-19 Pandemic. Front. Pharmacol. 2021, 12, 685696. [Google Scholar] [CrossRef]
- Kardas, P.; van Boven, J.F.M.; Pinnock, H.; Menditto, E.; Wettermark, B.; Tsiligianni, I.; Ágh, T.; ENABLE collaborators. Disparities in European healthcare system approaches to maintaining continuity of medication for non-communicable diseases during the COVID-19 outbreak. Lancet Reg. Health Eur. 2021, 4, 100099. [Google Scholar] [CrossRef]
- Kardas, P.; Dabrowa, M.; Witkowski, K. Adherence to treatment in paediatric patients—Results of the nationwide survey in Poland. BMC Pediatr. 2021, 21, 16. [Google Scholar] [CrossRef]
- Vrijens, B.; De Geest, S.; Hughes, D.A.; Przemyslaw, K.; Demonceau, J.; Ruppar, T.; Dobbels, F.; Fargher, E.; Morrison, V.; Lewek, P.; et al. A new taxonomy for describing and defining adherence to medications. Br. J. Clin. Pharmacol. 2012, 73, 691–705. [Google Scholar] [CrossRef]
- De Geest, S.; Zullig, L.L.; Dunbar-Jacob, J.; Helmy, R.; Hughes, D.A.; Wilson, I.B.; Vrijens, B. ESPACOMP Medication Adherence Reporting Guideline (EMERGE). Ann. Intern. Med. 2018, 169, 30–35. [Google Scholar] [CrossRef] [Green Version]
- Kardas, P.; Aguilar-Palacio, I.; Almada, M.; Cahir, C.; Costa, E.; Giardini, A.; Malo, S.; Massot Mesquida, M.; Menditto, E.; Midão, L.; et al. The Need to Develop Standard Measures of Patient Adherence for Big Data: Viewpoint. J. Med. Internet Res. 2020, 22, e18150. [Google Scholar] [CrossRef]
- Khan, R.; Socha-Dietrich, K. Investing in Medication Adherence Improves Health Outcomes and Health System Efficiency: Adherence to Medicines for Diabetes, Hypertension, and Hyperlipidaemia; OECD Health Working Papers, No. 105; OECD Publishing: Paris, France, 2018; pp. 1–39. [Google Scholar]
- Ágh, T.; Hadžiabdić, M.O.; Garuoliene, K.; Granas, A.G.; Aarnio, E.; Menditto, E.; Gregório, J.; Barnestein-Fonseca, P.; Mevsim, V.; Kardas, P. Reimbursed Medication Adherence Enhancing Interventions in European Countries: Results of the EUREcA Study. Front. Pharmacol. 2022, 13, 892240. [Google Scholar] [CrossRef] [PubMed]
- Kardas, P.; Bago, M.; Barnestein-Fonseca, P.; Garuolienė, K.; Granas, A.G.; Gregório, J.; Hadžiabdić, M.O.; Kostalova, B.; Leiva-Fernández, F.; Lewek, P.; et al. Reimbursed medication adherence enhancing interventions in 12 European countries: Current state of the art and future challenges. Front. Pharmacol. 2022, 13, 944829. [Google Scholar] [CrossRef] [PubMed]
- Elrod, J.K.; Fortenberry, J.L., Jr. Centers of excellence in healthcare institutions: What they are and how to assemble them. BMC Health Serv. Res. 2017, 17 (Suppl. 1), 425. [Google Scholar] [CrossRef] [PubMed]
- Damari, B.; Kamrava, S.K.; Kazemi-Asl, S.; Rostamigooran, N. Iranian centers of excellence in medical sciences: A qualitative study to analyze the current state and design of a future roadmap. Med. J. Islam. Repub. Iran. 2020, 34, 143. [Google Scholar] [CrossRef] [PubMed]
- Alkhenizan, A.; Khoja, T. Toward excellence in health care: A call for the Saudi Center for Health Excellence. J. Family Community Med. 2011, 18, 99–100. [Google Scholar] [CrossRef] [Green Version]
- Bandiera, C.; Ribaut, J.; Dima, A.L.; Allemann, S.S.; Molesworth, K.; Kalumiya, K.; Käser, F.; Olson, M.S.; Burnier, M.; van Boven, J.F.M.; et al. Swiss Priority Setting on Implementing Medication Adherence Interventions as Part of the European ENABLE COST Action. Int. J. Public. Health 2022, 67, 1605204. [Google Scholar] [CrossRef]
- Skills4Adherence. Available online: https://skills4adherence.eu/ (accessed on 2 June 2022).
- Dierick, B.H.J.; Achterbosch, M.; Been-Buck, S.; Klemmeier, T.; van de Hei, S.J.; Hagedoorn, P.; Kerstjens, H.A.M.; Kocks, J.W.H.; van Boven, J.F.M. Can electronic monitoring with a digital smart spacer support personalised medication adherence and inhaler technique education in patients with asthma?: Protocol of the randomised controlled OUTERSPACE trial. BMJ Open 2022, 12, e059929. [Google Scholar] [CrossRef]
- Zijp, T.R.; Touw, D.J.; van Boven, J.F.M. User Acceptability and Technical Robustness Evaluation of a Novel Smart Pill Bottle Prototype Designed to Support Medication Adherence. Patient Prefer. Adherence 2020, 14, 625–634. [Google Scholar] [CrossRef] [Green Version]
- Zijp, T.R.; Izzah, Z.; Åberg, C.; Gan, C.T.; Bakker, S.J.L.; Touw, D.J.; van Boven, J.F.M. Clinical Value of Emerging Bioanalytical Methods for Drug Measurements: A Scoping Review of Their Applicability for Medication Adherence and Therapeutic Drug Monitoring. Drugs 2021, 81, 1983–2002. [Google Scholar] [CrossRef]
- van de Hei, S.J.; Dierick, B.J.H.; Aarts, J.E.P.; Kocks, J.W.H.; van Boven, J.F.M. Personalized Medication Adherence Management in Asthma and Chronic Obstructive Pulmonary Disease: A Review of Effective Interventions and Development of a Practical Adherence Toolkit. J. Allergy Clin. Immunol. Pract. 2021, 9, 3979–3994. [Google Scholar] [CrossRef]
- Ridho, A.; Alfian, S.D.; van Boven, J.F.M.; Levita, J.; Yalcin, E.A.; Le, L.; Alffenaar, J.W.; Hak, E.; Abdulah, R.; Pradipta, I.S. Digital Health Technologies to Improve Medication Adherence and Treatment Outcomes in Patients With Tuberculosis: Systematic Review of Randomized Controlled Trials. J. Med. Internet Res. 2022, 24, e33062. [Google Scholar] [CrossRef] [PubMed]
- van Boven, J.F.M.; Alffenaar, J.C. An Inca trail to the Holy Grail: Digital medication adherence support for TB care. Int. J. Tuberc. Lung Dis. 2022, 26, 1–3. [Google Scholar] [CrossRef] [PubMed]
- van Boven, J.F.M.; Dierick, B.J.H.; Usmani, O.S. When biology meets behaviour: Can medication adherence mask the contribution of pharmacogenetic effects in asthma? Eur. Respir. J. 2021, 58, 2100304. [Google Scholar] [CrossRef] [PubMed]
- van Boven, J.F.M.; Fonseca, J.A. Editorial: Digital Tools to Measure and Promote Medication Adherence. Front. Med. Technol. 2021, 3, 751976. [Google Scholar] [CrossRef]
- Kardas, P.; Ratajczyk-Pakalska, E. Patient adherence in respiratory tract infections: Ceftibuten versus other antibiotics (PARTICULAR study). Pol. Merkur. Lekarski. 2001, 10, 445–449. [Google Scholar]
- Kardas, P. Comparison of patient compliance with once-daily and twice-daily antibiotic regimens in respiratory tract infections: Results of a randomized trial. J. Antimicrob. Chemother. 2007, 59, 531–536. [Google Scholar] [CrossRef] [Green Version]
- Kardas, P. Compliance, clinical outcome, and quality of life of patients with stable angina pectoris receiving once-daily betaxolol versus twice daily metoprolol: A randomized controlled trial. Vasc. Health Risk Manag. 2007, 3, 235–242. [Google Scholar] [CrossRef]
- Kardas, P. The DIACOM study (effect of DosIng frequency of oral Antidiabetic agents on the COMpliance and biochemical control of type 2 diabetes). Diabetes Obes. Metab. 2005, 7, 722–728. [Google Scholar] [CrossRef]
- Kardas, P.; COMPASS Investigators. Comparison of once daily versus twice daily oral nitrates in stable angina pectoris. Am. J. Cardiol. 2004, 94, 213–216. [Google Scholar] [CrossRef]
- Kardas, P. Drug compliance in patients treated with antibiotics in an ambulatory setting for respiratory tract infections. Pneumonol. Alergol. Pol. 1999, 67, 398–408. [Google Scholar]
- Ascertaining Barriers for Compliance: Policies for Safe, Effective and Cost-Effective Use of Medicines in Europe. Available online: http://www.abcproject.eu/ (accessed on 2 June 2022).
- Demonceau, J.; Ruppar, T.; Kristanto, P.; Hughes, D.A.; Fargher, E.; Kardas, P.; De Geest, S.; Dobbels, F.; Lewek, P.; Urquhart, J.; et al. Identification and assessment of adherence-enhancing interventions in studies assessing medication adherence through electronically compiled drug dosing histories: A systematic literature review and meta-analysis. Drugs 2013, 73, 545–562. [Google Scholar] [CrossRef] [Green Version]
- Maffoni, M.; Traversoni, S.; Granata, N.; Weinman, J.; Lewek, P.; Kurczewska-Michalak, M.; Kardas, P.; Almada, M.; Midão, L.; Costa, E.; et al. Lesson learned from an international training program on patients medication adherence for healthcare professionals. Giornale Italiano di Medicina del Lavoro ed Ergonomia 2021, 43, 137–143. [Google Scholar]
- Menditto, E.; Orlando, V.; De Rosa, G.; Minghetti, P.; Musazzi, U.M.; Cahir, C.; Kurczewska-Michalak, M.; Kardas, P.; Costa, E.; Sousa Lobo, J.M.; et al. Patient Centric Pharmaceutical Drug Product Design-The Impact on Medication Adherence. Pharmaceutics 2020, 12, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurczewska-Michalak, M.; Kardas, P.; Czajkowski, M. Patients’ Preferences and Willingness to Pay for Solid Forms of Oral Medications-Results of the Discrete Choice Experiment in Polish Outpatients. Pharmaceutics 2020, 12, 236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kardas, P.; Cieszyński, J.; Czech, M.; Banaś, I.; Lewek, P. Primary nonadherence to medication and its drivers in Poland: Findings from the electronic prescription pilot analysis. Pol. Arch. Intern. Med. 2020, 130, 8–16. [Google Scholar] [PubMed] [Green Version]
- Kardas, P.; Urbański, F.; Lichwierowicz, A.; Chudzyńska, E.; Kardas, G.; Czech, M. Prevalence and Age Structure of Polypharmacy in Poland: Results of the Analysis of the National Real-World Database of 38 Million Citizens. Front. Pharmacol. 2021, 12, 655364. [Google Scholar] [CrossRef]
- Craig, W.; Fisher, M.; Garcia, S.; Kaylor, C.; Porter, J.; Reed, L.S. Generalized Criteria and Evaluation Method for Center of Excellence: A Preliminary Report. Available online: https://resources.sei.cmu.edu/library/asset-view.cfm?assetid=8971 (accessed on 1 February 2023).
- Pronovost, P.J.; Ata, G.J.; Carson, B.; Gordon, Z.; Smith, G.A.; Khaitan, L.; Kraay, M.J. What Is a Center of Excellence? Popul. Health Manag. 2022, 25, 561–567. [Google Scholar] [CrossRef]
- Li, J.; Burson, R.C.; Clapp, J.T.; Fleisher, L.A. Centers of excellence: Are there standards? Healthcare 2020, 8, 100388. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Area of Activity | Objectives |
|---|---|
| Research |
|
| Clinical practice |
|
| Education |
|
| Advocacy & Policy |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kardas, P.; Ágh, T.; Dima, A.; Goetzinger, C.; Potočnjak, I.; Wettermark, B.; van Boven, J.F.M. Half a Century of Fragmented Research on Deviations from Advised Therapies: Is This a Good Time to Call for Multidisciplinary Medication Adherence Research Centres of Excellence? Pharmaceutics 2023, 15, 933. https://doi.org/10.3390/pharmaceutics15030933
Kardas P, Ágh T, Dima A, Goetzinger C, Potočnjak I, Wettermark B, van Boven JFM. Half a Century of Fragmented Research on Deviations from Advised Therapies: Is This a Good Time to Call for Multidisciplinary Medication Adherence Research Centres of Excellence? Pharmaceutics. 2023; 15(3):933. https://doi.org/10.3390/pharmaceutics15030933
Chicago/Turabian StyleKardas, Przemysław, Tamás Ágh, Alexandra Dima, Catherine Goetzinger, Ines Potočnjak, Björn Wettermark, and Job F. M. van Boven. 2023. "Half a Century of Fragmented Research on Deviations from Advised Therapies: Is This a Good Time to Call for Multidisciplinary Medication Adherence Research Centres of Excellence?" Pharmaceutics 15, no. 3: 933. https://doi.org/10.3390/pharmaceutics15030933