
A Validated Chiral LC–MS/MS Method for the Enantioselective Determination of (S)-(+)- and (R)-(-)-Ibuprofen in Dog Plasma: Its Application to a Pharmacokinetic Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
2.2. LC–MS/MS System
2.3. Preparation of Calibration Standards and Quality Control (QC) Samples
2.4. Plasma Sample Preparation
2.5. Method Validation
2.5.1. Selectivity and Sensitivity
2.5.2. Linearity and Carryover
2.5.3. Precision and Accuracy
2.5.4. Recovery and Matrix Effect
2.5.5. Stability
2.5.6. Dilution Integrity
2.6. Application to a Pharmacokinetic Study
2.7. Incurred Sample Reanalysis (ISR)
3. Results and Discussion
3.1. Method Development
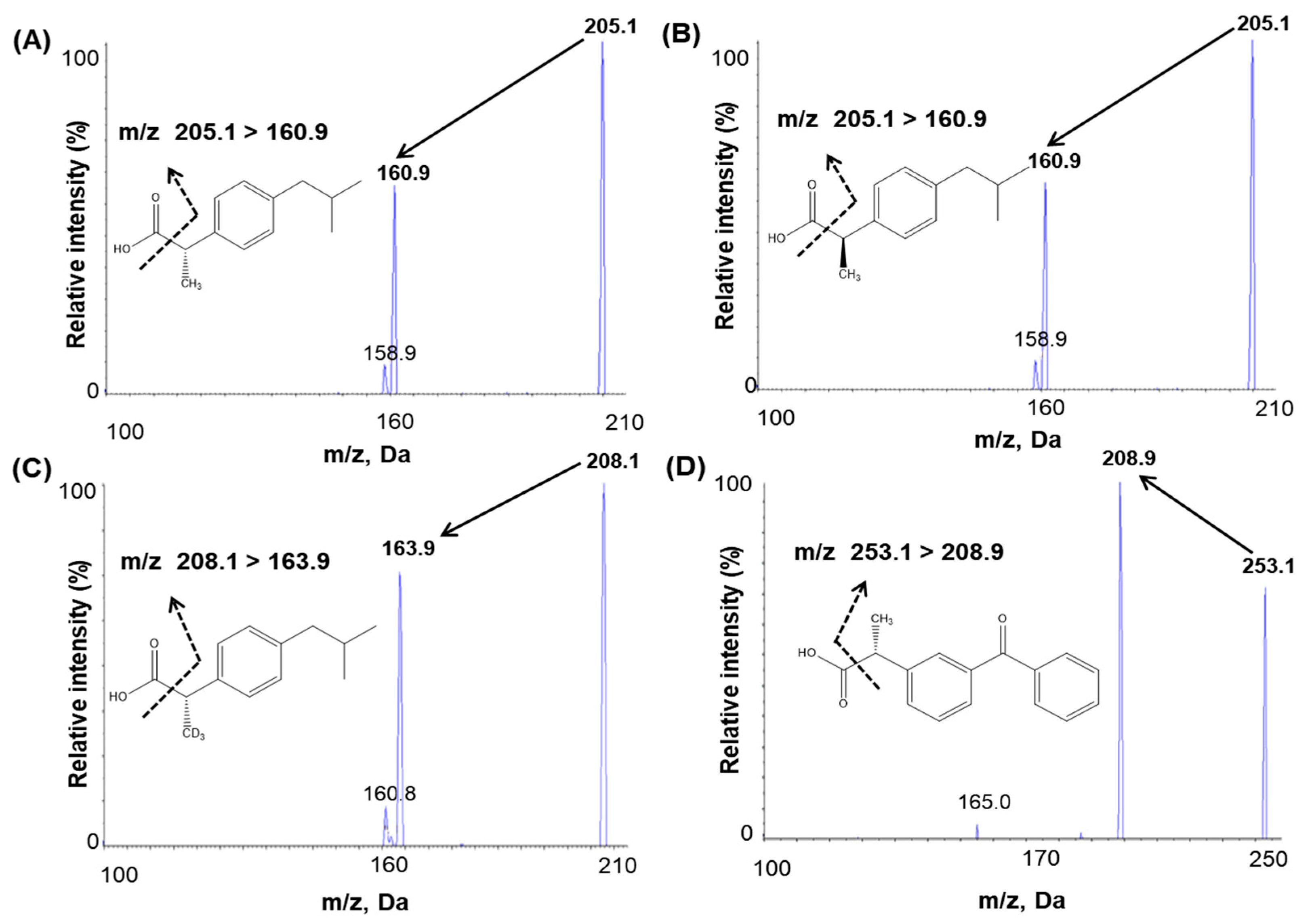
3.1.1. Mass Spectrometry
3.1.2. Chromatographic Conditions
3.1.3. Sample Preparation
3.2. Method Validation
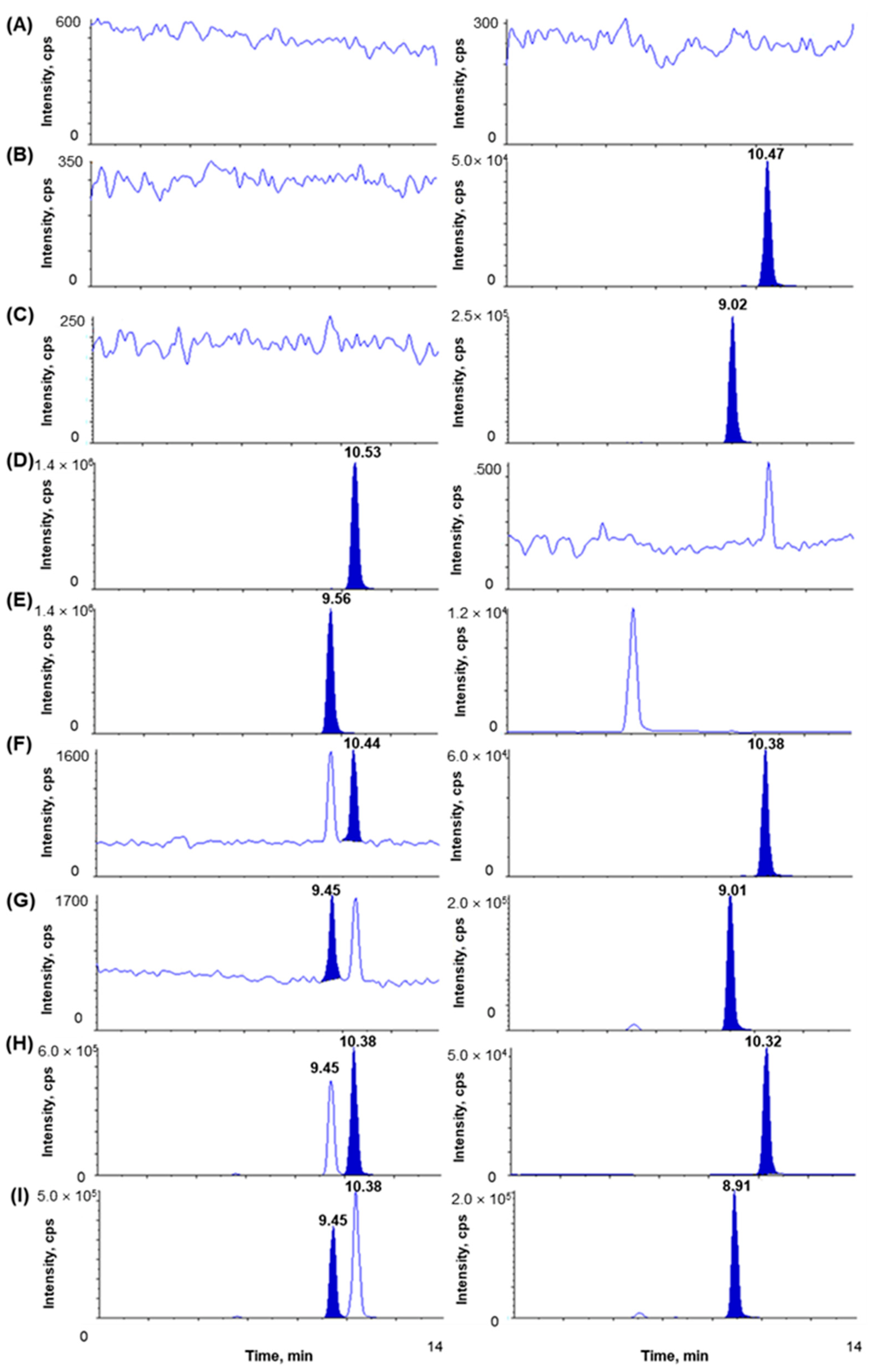
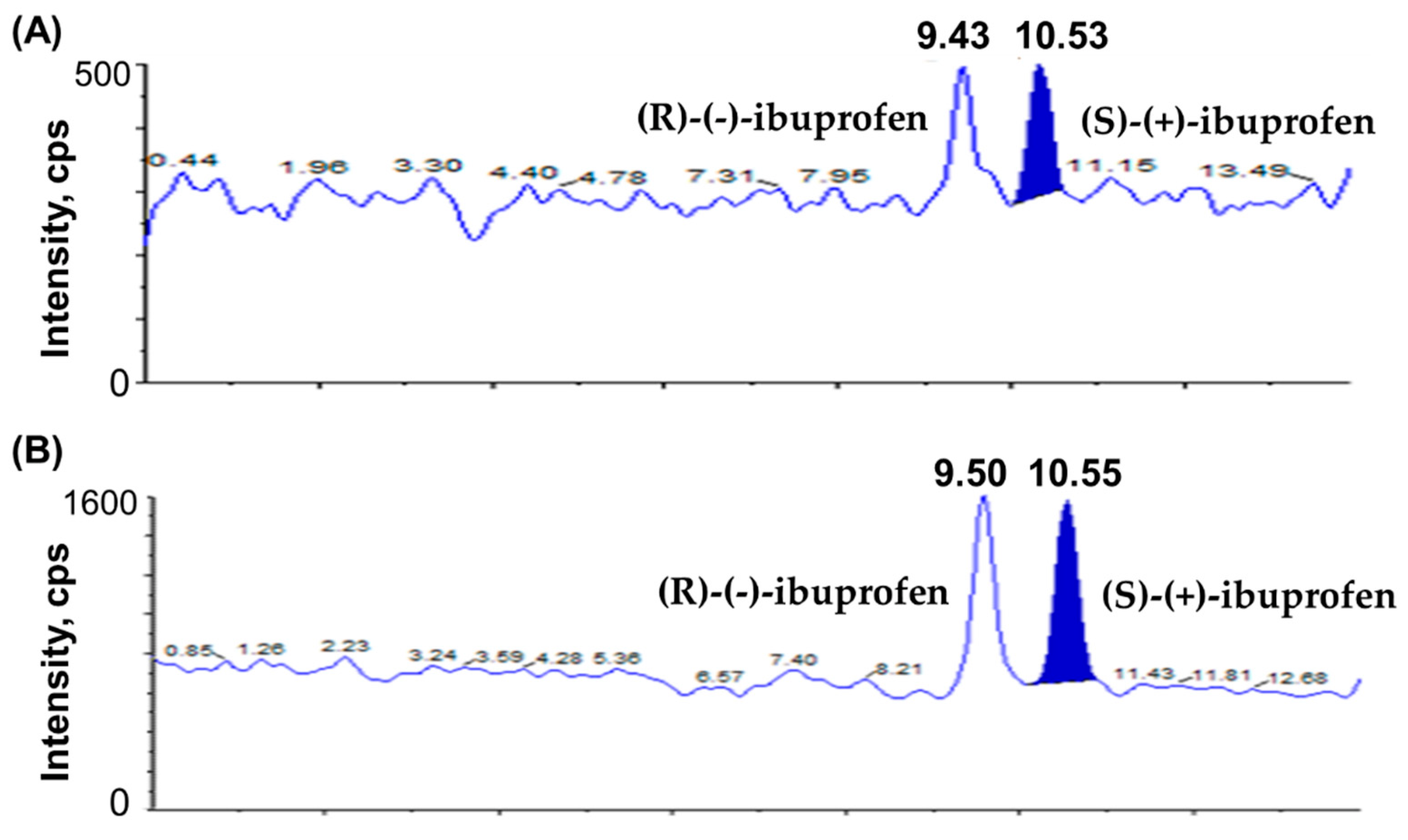
3.2.1. Selectivity and Sensitivity
3.2.2. Linearity and Carryover
3.2.3. Precision and Accuracy
3.2.4. Recovery and Matrix Effect
3.2.5. Stability
3.2.6. Dilution Integrity
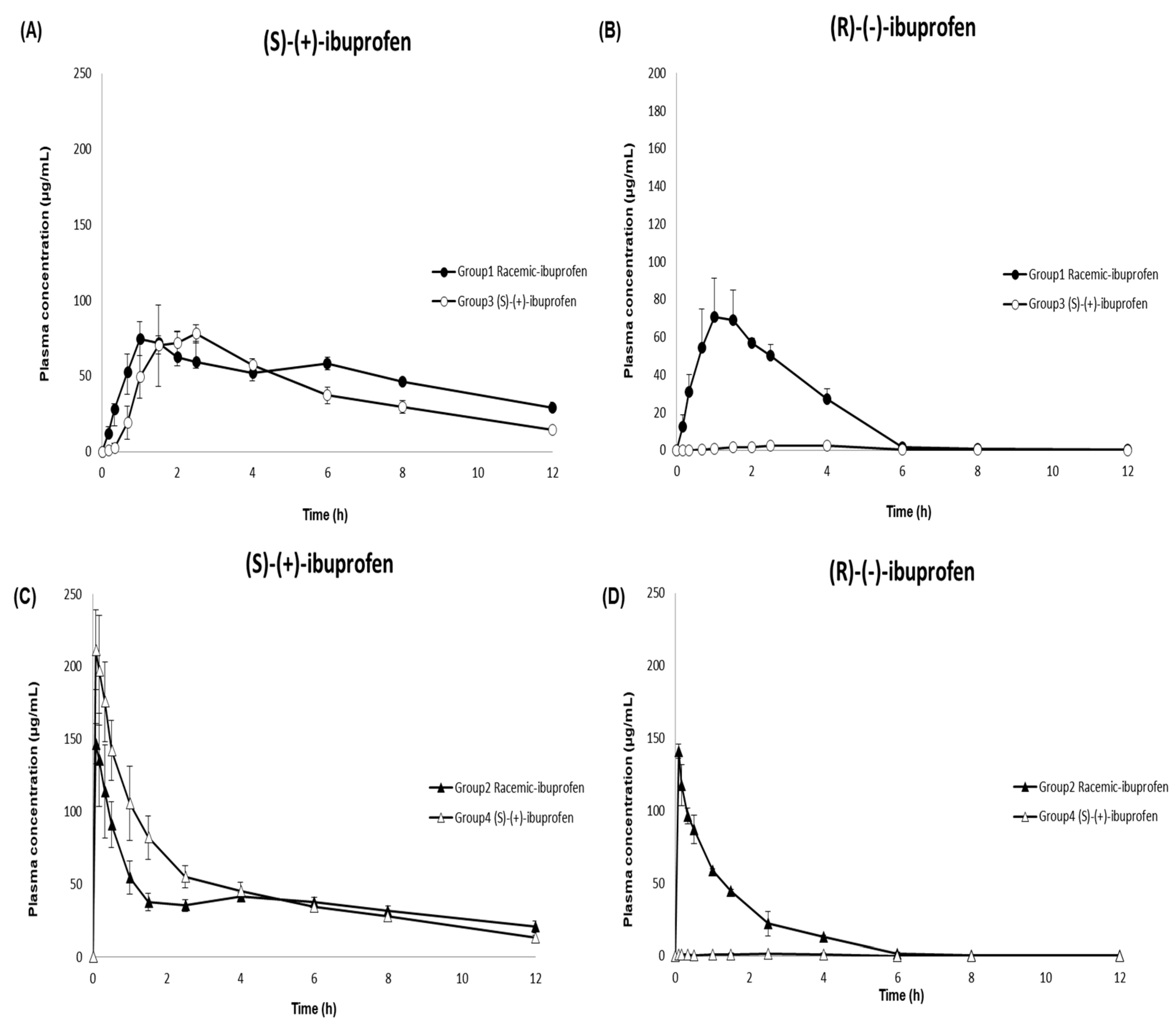
3.3. Application to a Pharmacokinetic Study
3.4. Incurred Sample Reanalysis (ISR)
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bushra, R.; Aslam, N. An overview of clinical pharmacology of ibuprofen. Oman Med. Med. J. 2010, 25, 155. [Google Scholar] [CrossRef]
- Busson, M. Update on ibuprofen. J. Int. Med. Res. 1986, 14, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.M. Clinical pharmacokinetics of ibuprofen. Clin. Pharmacokinet. 1998, 34, 101–154. [Google Scholar] [CrossRef] [PubMed]
- Kantor, T.G. Ibuprofen. Ann. Intern. Med. 1979, 91, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Evans, A.M. Pharmacodynamics and pharmacokinetics of the profens: Enantioselectivity, clinical implications, and special reference to S (+)-ibuprofen. J. Clin. Pharmacol. 1996, 36, 7S–15S. [Google Scholar] [PubMed]
- Evans, A.M. Comparative pharmacology of S (+)-ibuprofen and (RS)-ibuprofen. Clin. Rheumatol. 2001, 20, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Phleps, W. Overview on clinical data of dexibuprofen. Clin. Rheumatol. 2001, 20, 15–21. [Google Scholar] [CrossRef]
- Leising, G.; Resel, R.; Stelzer, F.; Tasch, S.; Lanziner, A.; Hantich, G. Physical aspects of dexibuprofen and racemic ibuprofen. J. Clin. Pharmacol. 1996, 36, 3S. [Google Scholar]
- Gliszczyńska, A.; Sánchez-López, E. Dexibuprofen Therapeutic Advances: Prodrugs and Nanotechnological Formulations. Pharmaceutics 2021, 13, 414. [Google Scholar] [CrossRef]
- Kaehler, S.T.; Phleps, W.; Hesse, E. Dexibuprofen: Pharmacology, therapeutic uses and safety. Inflammopharmacology 2003, 11, 371–383. [Google Scholar] [CrossRef]
- Lee, E.J.; Williams, K.M.; Day, R.; Graham, G.; Champion, D. Stereoselective disposition of ibuprofen enantiomers in man. Br. J. Clin. Pharmacol. 1985, 19, 669–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaiser, D.G.; Vangiessen, G.J.; Reischer, R.J.; Wechter, W.J. Isomeric inversion of ibuprofen (R)-enantiomer in humans. J. Pharm. Sci. 1976, 65, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Knihinicki, R.D.; Williams, K.M.; Day, R.O. Chiral inversion of 2-arylpropionic acid non-steroidal anti-inflammatory drugs—1: In vitro studies of ibuprofen and flurbiprofen. Biochem. Pharmacol. 1989, 38, 4389–4395. [Google Scholar] [CrossRef] [PubMed]
- Rudy, A.C.; Knight, P.M.; Brater, D.C.; Hall, S.D. Stereoselective metabolism of ibuprofen in humans: Administration of R-, S-and racemic ibuprofen. J. Pharmacol. Exp. Ther. 1991, 259, 1133–1139. [Google Scholar]
- Hao, H.; Wang, G.; Sun, J. Enantioselective pharmacokinetics of ibuprofen and involved mechanisms. Drug Metab. Rev. 2005, 37, 215–234. [Google Scholar] [CrossRef]
- Hamman, M.A.; Thompson, G.A.; Hall, S.D. Regioselective and stereoselective metabolism of ibuprofen by human cytochrome P450 2C. Biochem. Pharmacol. 1997, 54, 33–41. [Google Scholar] [CrossRef]
- López-Rodríguez, R.; Novalbos, J.; Gallego-Sandín, S.; Román-Martínez, M.; Torrado, J.; Gisbert, J.P.; Abad-Santos, F. Influence of CYP2C8 and CYP2C9 polymorphisms on pharmacokinetic and pharmacodynamic parameters of racemic and enantiomeric forms of ibuprofen in healthy volunteers. Pharmacol. Res. 2008, 58, 77–84. [Google Scholar] [CrossRef]
- Gabard, B.; Nirnberger, G.; Schiel, H.; Mascher, H.; Kikuta, C.; Mayer, J.M. Comparison of the bioavailability of dexibuprofen administered alone or as part of racemic ibuprofen. Eur. J. Clin. Pharmacol. 1995, 48, 505–511. [Google Scholar] [CrossRef]
- Bookstaver, P.B.; Miller, A.D.; Rudisill, C.N.; Norris, L.B. Intravenous ibuprofen: The first injectable product for the treatment of pain and fever. J. Pain Res. 2010, 3, 67. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Qi, M.; Liu, L.; Fang, L. Determination of ibuprofen in dog plasma by liquid chromatography and application in pharmacokinetic studies of an ibuprofen prodrug in dogs. J. Pharm. Biomed. Anal. 2005, 38, 714–719. [Google Scholar] [CrossRef]
- Jonkman, J.; Schoenmaker, R.; Holtkamp, A.H.; Hempenius, J. Determination of ibuprofen in human plasma by solid phase extraction and reversed-phase high-performance liquid chromatography. J. Pharm. Biomed. Anal. 1985, 3, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Hao, H.; Wang, G.; Sang, G.; Sun, J.; Li, P.; Li, J. Chiral separation of ibuprofen and chiral pharmacokinetics in healthy Chinese volunteers. Eur. J. Drug Metab. Pharmacokinet. 2008, 33, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Naidong, W.; Lee, J.W. Development and validation of a liquid chromatographic method for the quantitation of ibuprofen enantiomers in human plasma. J. Pharm. Biomed. Anal. 1994, 12, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, K.; Olsson, A. Liquid chromatographic determination of the enantiomers of ibuprofen in plasma using a chiral AGP column. J. Chromatogr. B Biomed. Sci. Appl. 1991, 563, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Teng, X.W.; Wang, S.W.; Davies, N.M. Stereospecific high-performance liquid chromatographic analysis of ibuprofen in rat serum. J. Chromatogr. B 2003, 796, 225–231. [Google Scholar] [CrossRef]
- Wright, M.R.; Sattari, S.; Brocks, D.R.; Jamali, F. Improved high-performance liquid chromatographic assay method for the enantiomers of ibuprofen. J. Chromatogr. B Biomed. Sci. Appl. 1992, 583, 259–265. [Google Scholar] [CrossRef]
- Ahn, H.; Shiu, G.K.; Trafton, W.F.; Doyle, T.D. Resolution of the enantiomers of ibuprofen; comparison study of diastereomeric method and chiral stationary phase method. J. Chromatogr. B Biomed. Sci. Appl. 1994, 653, 163–169. [Google Scholar] [CrossRef]
- Lemko, C.H.; Caillé, G.; Foster, R.T. Stereospecific high-performance liquid chromatographic assay of ibuprofen: Improved sensitivity and sample processing efficiency. J. Chromatogr. B Biomed. Sci. Appl. 1993, 619, 330–335. [Google Scholar] [CrossRef]
- Tan, S.C.; Jackson, S.; Swift, C.G.; Hutt, A.J. Enantiospecific analysis of ibuprofen by high performance liquid chromatography: Determination of free and total drug enantiomer concentrations in serum and urine. Chromatographia 1997, 46, 23–32. [Google Scholar] [CrossRef]
- Canaparo, R.; Muntoni, E.; Zara, G.P.; Della Pepa, C.; Berno, E.; Costa, M.; Eandi, M. Determination of Ibuprofen in human plasma by high-performance liquid chromatography: Validation and application in pharmacokinetic study. Biomed. Chromatogr. 2000, 14, 219–226. [Google Scholar] [CrossRef]
- Zambakjian, C.; Sakur, A.A. A new gas chromatographic method development and validation for the simultaneous determination of ibuprofen and caffeine in bulk and pharmaceutical dosage form. Future J. Pharm. Sci. 2020, 6, 110. [Google Scholar] [CrossRef]
- Way, B.A.; Wilhite, T.R.; Smith, C.H.; Landt, M. Measurement of plasma ibuprofen by gas chromatography-mass spectrometry. J. Clin. Lab. Anal. 1997, 11, 336–339. [Google Scholar] [CrossRef]
- Zhao, M.; Peter, C.; Holtz, M.; Hugenell, N.; Koffel, J.; Jung, L. Gas chromatographic-mass spectrometric determination of ibuprofen enantiomers in human plasma using R (−)-2, 2, 2-trifluoro-1-(9-anthryl) ethanol as derivatizing reagent. J. Chromatogr. B Biomed. Sci. Appl. 1994, 656, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, B.; Erdem, A.F. Determination of ibuprofen in human plasma and urine by gas chromatography/mass spectrometry. J. AOAC Int. 2014, 97, 415–420. [Google Scholar] [CrossRef]
- Aucella, F.; Lauriola, V.; Vecchione, G.; Tiscia, G.L.; Grandone, E. Liquid chromatography-tandem mass spectrometry method as the golden standard for therapeutic drug monitoring in renal transplant. J. Pharm. Biomed. Anal. 2013, 86, 123–126. [Google Scholar] [CrossRef]
- Jemal, M. High-throughput quantitative bioanalysis by LC/MS/MS. Biomed. Chromatogr. 2000, 14, 422–429. [Google Scholar] [CrossRef]
- Jemal, M.; Ouyang, Z.; Xia, Y. Systematic LC-MS/MS bioanalytical method development that incorporates plasma phospholipids risk avoidance, usage of incurred sample and well thought-out chromatography. Biomed. Chromatogr. 2010, 24, 2–19. [Google Scholar] [CrossRef]
- Chen, T.; Li, Q.; Lu, J.; Yu, C.; Chen, C.; Li, Z. Determination of ibuprofen enantiomers in human plasma by HPLC–MS/MS: Validation and application in neonates. Bioanalysis 2016, 8, 1237–1250. [Google Scholar] [CrossRef]
- Sharma, P.; Guttikar, S.; Solanki, G.; Patel, D.P.; Shrivastav, P.S. Determination of (S)-(+)-and (R)-(-)-ibuprofen enantiomers in human plasma after chiral precolumn derivatization by reversed-phase LC–ESI-MS/MS. Bioanalysis 2012, 4, 2909–2927. [Google Scholar] [CrossRef]
- Cardoso, J.L.C.; Lanchote, V.L.; Pereira, M.P.M.; de Moraes, N.V.; Lepera, J.S. Analysis of ibuprofen enantiomers in rat plasma by liquid chromatography with tandem mass spectrometry. J. Sep. Sci. 2014, 37, 944–949. [Google Scholar] [CrossRef]
- Nakov, N.; Petkovska, R.; Ugrinova, L.; Kavrakovski, Z.; Dimitrovska, A.; Svinarov, D. Critical development by design of a rugged HPLC-MS/MS method for direct determination of ibuprofen enantiomers in human plasma. J. Chromatogr. B 2015, 992, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Bonato, P.S.; Del Lama, M.P.F.M.; de Carvalho, R. Enantioselective determination of ibuprofen in plasma by high-performance liquid chromatography–electrospray mass spectrometry. J. Chromatogr. B 2003, 796, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Szeitz, A.; Edginton, A.N.; Peng, H.T.; Cheung, B.; Riggs, K.W. A validated enantioselective assay for the determination of ibuprofen in human plasma using ultra performance liquid chromatography with tandem mass spectrometry (UPLC-MS/MS). Am. J. Anal. Chem. 2010, 1, 47. [Google Scholar] [CrossRef] [Green Version]
- Food and Drug Administration. Bioanalytical Method Validation Guidance for Industry. US Department of Health and Human Services. 2018. Available online: https://www.fda.gov/media/70858/download (accessed on 6 December 2021).
- Ministry of Food and Drug Safety. Guideline on Bioanalytical Method Validation. 2013. Available online: https://www.mfds.go.kr/brd/m210/down.do?brd_id=data0010&seq=13054data_tp=A&file_seq=1 (accessed on 6 December 2021).
- Yi, H.G.; Chi, M.H.; Kim, Y.; Woo, J.S.; Park, E. Formulation of a extended release tablet containing dexibuprofen. Arch. Pharm. Res. 2008, 31, 1637–1643. [Google Scholar] [CrossRef] [PubMed]
- Pavliv, L.; Voss, B.; Rock, A. Pharmacokinetics, safety, and tolerability of a rapid infusion of iv ibuprofen in healthy adults. Am. J. Health Syst. Pharm. 2011, 68, 47–51. [Google Scholar] [CrossRef]
- Cheng, H.; Rogers, J.D.; Demetriades, J.L.; Holland, S.D.; Seibold, J.R.; Depuy, E. Pharmacokinetics and bioinversion of ibuprofen enantiomers in humans. Pharm. Res. 1994, 11, 824–830. [Google Scholar] [CrossRef]
- Smith, H.S.; Voss, B. Pharmacokinetics of intravenous ibuprofen. Drugs 2012, 72, 327–337. [Google Scholar] [CrossRef]
- Geisslinger, G.; Schuster, O.; Stock, K.; Loew, D.; Bach, G.L.; Brune, K. Pharmacokinetics of S (+)-and R (−)-ibuprofen in volunteers and first clinical experience of S (+)-ibuprofen in rheumatoid arthritis. Eur. J. Clin. Pharmacol. 1990, 38, 493–497. [Google Scholar] [CrossRef]
- Jamali, F.; Singh, N.N.; Pasutto, F.M.; Russell, A.S.; Coutts, R.T. Pharmacokinetics of ibuprofen enantiomers in humans following oral administration of tablets with different absorption rates. Pharm. Res. 1988, 5, 40–43. [Google Scholar] [CrossRef]
- Frihmat, R.; Cardot, J.; Beyssac, E.; Boucher, M.; Aiache, J. Bioinversion of ibuprofen enantiomers after administration in dogs: Estimation of a novel index. Eur. J. Drug Metab. Pharmacokinet. 2000, 25, 205–211. [Google Scholar] [CrossRef]
- Beck, W.S.; Geisslinger, G.; Engler, H.; Brune, K. Pharmacokinetics of ibuprofen enantiomers in dogs. Chirality 1991, 3, 165–169. [Google Scholar] [CrossRef]
- Sattari, S.; Jamali, F. Evidence of absorption rate dependency of ibuprofen inversion in the rat. Chirality 1994, 6, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Wsol, V.; Skálová, L.; Szotáková, B. Chiral inversion of drugs: Coincidence or principle? Curr. Drug Metab. 2004, 5, 517–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Boer, T.; Wieling, J. Incurred sample accuracy assessment: Design of experiments based on standard addition. Bioanalysis 2011, 3, 983–992. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compounds | Ion Transition (m/z) | DP (V) | EP (V) | CE (V) | CXP (V) | RT (min) |
|---|---|---|---|---|---|---|
| (S)-(+)-Ibuprofen | 205.1 → 160.9 | −62.0 | −10.0 | −12.0 | −9.0 | 10.38 |
| (R)-(-)-Ibuprofen | 205.1 → 160.9 | −62.0 | −8.0 | −10.0 | −9.0 | 9.44 |
| (S)-(+)-Ibuprofen-d3 | 208.1 → 163.9 | −62.0 | −10.0 | −10.0 | −9.0 | 10.31 |
| (S)-(+)-Ketoprofen | 253.1 → 208.9 | −70.0 | −10.0 | −12.0 | −13.0 | 8.91 |
| Compounds | Number | Slope | Intercept | r | r2 |
|---|---|---|---|---|---|
| (S)-(+)-Ibuprofen | 1 | 0.154 | −0.001340 | 0.9995 | 0.9990 |
| 2 | 0.155 | −0.001220 | 0.9990 | 0.9980 | |
| 3 | 0.158 | −0.000825 | 0.9989 | 0.9978 | |
| 4 | 0.150 | −0.000686 | 0.9985 | 0.9970 | |
| 5 | 0.145 | 0.000687 | 0.9988 | 0.9976 | |
| (R)-(-)-Ibuprofen | 1 | 0.0419 | −0.000404 | 0.9984 | 0.9968 |
| 2 | 0.0410 | −0.000674 | 0.9966 | 0.9932 | |
| 3 | 0.0456 | −0.000104 | 0.9971 | 0.9942 | |
| 4 | 0.0479 | −0.000874 | 0.9970 | 0.9940 | |
| 5 | 0.0458 | 0.000545 | 0.9959 | 0.9918 |
| Compounds | Nominal Concentration (µg/mL) | Intra-Day (n = 5) | Inter-Day (n = 15) | ||||
|---|---|---|---|---|---|---|---|
| Mean ± SD (µg/mL) | Precision (CV, %) a | Accuracy (%) b | Mean ± SD (µg/mL) | Precision (CV, %) a | Accuracy (%) b | ||
| (S)-(+)-Ibuprofen | 0.1 | 0.10 ± 0.01 | 7.31 | 103.60 | 0.10 ± 0.01 | 6.60 | 103.00 |
| 0.3 | 0.31 ± 0.01 | 2.03 | 103.60 | 0.31 ± 0.01 | 3.65 | 101.84 | |
| 30 | 28.96 ± 0.42 | 1.46 | 96.53 | 28.93 ± 0.37 | 1.28 | 96.45 | |
| 64 | 66.13 ± 0.35 | 0.53 | 103.33 | 65.04 ± 1.20 | 1.84 | 101.63 | |
| (R)-(-)-Ibuprofen | 0.1 | 0.10 ± 0.01 | 7.19 | 97.60 | 0.10 ± 0.00 | 4.87 | 99.07 |
| 0.3 | 0.30 ± 0.01 | 1.75 | 99.80 | 0.30 ± 0.01 | 3.04 | 100.49 | |
| 30 | 31.16 ± 0.15 | 0.48 | 103.86 | 32.27 ± 0.63 | 1.93 | 107.58 | |
| 64 | 69.45 ± 0.67 | 0.96 | 108.51 | 70.98 ± 0.74 | 1.04 | 110.90 | |
| Compounds | Nominal Concentration (µg/mL) | Recovery (%) | Matrix Effect (%) | ||
|---|---|---|---|---|---|
| Mean ± SD (%) | CV (%) | Mean ± SD (%) | CV (%) | ||
| (S)-(+)-Ibuprofen | 0.3 | 85.28 ± 4.73 | 5.54 | 93.79 ± 3.89 | 4.15 |
| 30 | 82.23 ± 1.44 | 1.75 | 86.74 ± 1.95 | 2.25 | |
| 64 | 82.94 ± 2.29 | 2.76 | 89.54 ± 2.06 | 2.30 | |
| Mean | 83.48 ± 2.82 | 3.35 | 90.02 ± 2.63 | 2.90 | |
| (R)-(-)-Ibuprofen | 0.3 | 87.89 ± 2.59 | 2.94 | 100.99 ± 1.71 | 1.69 |
| 30 | 85.02 ± 2.53 | 2.97 | 94.38 ± 3.14 | 3.33 | |
| 64 | 84.01 ± 2.22 | 2.65 | 94.63 ± 2.54 | 2.69 | |
| Mean | 85.64 ± 2.45 | 2.85 | 96.67 ± 2.46 | 2.57 | |
| (S)-(+)-Ibuprofen-d3 | 10 | 87.49 ± 2.94 | 3.36 | 87.48 ± 1.72 | 1.96 |
| (S)-(+)-Ketoprofen | 10 | 84.56 ± 1.12 | 1.32 | 92.21 ± 0.78 | 0.84 |
| Nominal Concentration (µg/mL) | Solution Stability (Mean ± SD, %) | Plasma Stability (Mean ± SD, %) | ||||||
|---|---|---|---|---|---|---|---|---|
| Stock Room Temperature (3 h) | Working Room Temperature (7 h) | Room Temperature (7 h) | 4 °C (7 h) | −70 °C (7 h) | Freeze-Thaw Stability (3 Cycles) | Autosampler (54 h, 10 °C) | Long-Term (−70 °C, 196 Days) | |
| (S)-(+)-Ibuprofen | ||||||||
| 0.3 | 99.04 ± 3.40 | 98.83 ± 4.07 | 101.78 ± 0.01 | 100.56 ± 0.01 | 99.33 ± 0.01 | 98.00 ± 0.01 | 97.22 ± 0.00 | 99.59 ± 4.21 |
| 30 | - | - | 97.11 ± 0.43 | 97.29 ± 0.47 | 97.76 ± 0.51 | 92.97 ± 0.24 | 91.37 ± 0.05 | 93.32 ± 0.21 |
| 64 | 100.15 ± 2.15 | 99.55 ± 2.64 | 100.69 ± 0.78 | 98.77 ± 0.46 | 99.250 ± 0.65 | 99.61 ± 0.82 | 98.48 ± 0.30 | 97.24 ± 2.53 |
| (R)-(-)-Ibuprofen | ||||||||
| 0.3 | 100.72 ± 3.34 | 101.73 ± 7.57 | 97.78 ± 0.00 | 98.33 ± 0.00 | 100.22 ± 0.01 | 95.22 ± 0.00 | 99.33 ± 0.01 | 96.36 ± 5.34 |
| 30 | - | - | 108.67 ± 0.21 | 109.47 ± 0.20 | 109.90 ± 0.26 | 104.70 ± 0.21 | 108.44 ± 0.18 | 98.05 ± 0.47 |
| 64 | 99.84 ± 1.76 | 99.57 ± 1.51 | 109.75 ± 1.08 | 111.81 ± 0.44 | 109.74 ± 1.53 | 113.38 ± 1.29 | 109.11 ± 0.90 | 94.87 ± 0.63 |
| Parameter | Oral | |||
|---|---|---|---|---|
| (S)-(+)-Ibuprofen (Mean ± SD) | (R)-(-)-Ibuprofen (Mean ± SD) | |||
| Group 1 (Mean ± SD) | Group 3 (Mean ± SD) | Group 1 (Mean ± SD) | Group 3 (Mean ± SD) | |
| Cmax (µg/mL) | 77.76 ± 9.80 | 84.57 ± 12.30 | 74.74 ± 20.02 | - a |
| AUClast (µg·h/mL) | 467.78 ± 20.59 | 588.14 ± 37.12 | 223.48 ± 37.04 | - |
| AUCinf (µg·h/mL) | 555.65 ± 43.78 | 847.34 ± 52.17 | 224.06 ± 37.22 | - |
| Tmax (h) | 1.50 ± 0.50 | 2.17 ± 0.58 | 1.50 ± 0.50 | - |
| t1/2 (h) | 6.12 ± 1.44 | 4.16 ± 0.54 | 2.07 ± 0.18 | - |
| CL/F(L/h) | 0.47 ± 0.03 | 0.54 ± 0.04 | 1.82 ± 0.33 | - |
| Vz/F(L) | 4.14 ± 0.75 | 3.23 ± 0.22 | 5.49 ± 1.51 | - |
| Parameter | Intravenous | |||
| (S)-(+)-Ibuprofen (Mean ± SD) | (R)-(-)-Ibuprofen (Mean ± SD) | |||
| Group 2 (Mean ± SD) | Group 4 (Mean ± SD) | Group 2 (Mean ± SD) | Group 4 (Mean ± SD) | |
| Cmax (µg/mL) | 153.91 ± 18.22 | 211.52 ± 27.52 | 140.96 ± 4.71 | - a |
| AUClast (µg·h/mL) | 461.71 ± 9.42 | 557.58 ± 66.76 | 181.28 ± 13.53 | - |
| AUCinf (µg·h/mL) | 677.43 ± 98.12 | 640.78 ± 63.27 | 181.70 ± 13.36 | - |
| Tmax (h) | 0.11 ± 0.05 | 0.08 ± 0.00 | 0.08 ± 0.00 | - |
| t1/2 (h) | 7.06 ± 2.20 | 4.45 ± 0.80 | 1.81 ± 0.52 | - |
| CL(L/h) | 0.60 ± 0.09 | 0.47 ± 0.05 | 2.21 ± 0.16 | - |
| Vz(L) | 5.92 ± 1.03 | 3.04 ± 0.74 | 5.74 ± 1.53 | - |
| MRTlast (h) | 4.77 ± 0.43 | 3.68 ± 0.23 | 1.56 ± 0.04 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, S.; Shim, W.-S.; Yoon, J.; Choi, D.; Lee, J.; Paik, S.-H.; Chung, E.-K.; Lee, K.-T. A Validated Chiral LC–MS/MS Method for the Enantioselective Determination of (S)-(+)- and (R)-(-)-Ibuprofen in Dog Plasma: Its Application to a Pharmacokinetic Study. Pharmaceutics 2023, 15, 824. https://doi.org/10.3390/pharmaceutics15030824
Choi S, Shim W-S, Yoon J, Choi D, Lee J, Paik S-H, Chung E-K, Lee K-T. A Validated Chiral LC–MS/MS Method for the Enantioselective Determination of (S)-(+)- and (R)-(-)-Ibuprofen in Dog Plasma: Its Application to a Pharmacokinetic Study. Pharmaceutics. 2023; 15(3):824. https://doi.org/10.3390/pharmaceutics15030824
Chicago/Turabian StyleChoi, Sanghee, Wang-Seob Shim, Jiyoung Yoon, Doowon Choi, Jinseong Lee, Soo-Heui Paik, Eun-Kyoung Chung, and Kyung-Tae Lee. 2023. "A Validated Chiral LC–MS/MS Method for the Enantioselective Determination of (S)-(+)- and (R)-(-)-Ibuprofen in Dog Plasma: Its Application to a Pharmacokinetic Study" Pharmaceutics 15, no. 3: 824. https://doi.org/10.3390/pharmaceutics15030824