
Development and Optimisation of Inhalable EGCG Nano-Liposomes as a Potential Treatment for Pulmonary Arterial Hypertension by Implementation of the Design of Experiments Approach
Abstract
:1. Introduction
2. Methods
2.1. Chemicals and Solvents
2.2. Preparation of Inhalable EGCG Nano-Liposome Formulations
2.3. High-Performance Liquid Chromatography (HPLC)
2.4. Implementation of DOE
2.5. Confirming the Predictivity of the Model, and Preparing the Optimum Proposed Liposome Formulation
2.6. Characterisation of the Inhalable EGCG Nano-Liposome Formulations
2.6.1. Inhalable EGCG Nano-Liposome Formulations’ Particle Size, Dispersity, and Zeta Potential Measurements
2.6.2. pH Measurements of the Liposome Formulations
2.6.3. Determination of the Encapsulation Efficiency
2.6.4. Viscosity Measurements of the Optimum EGCG Nano-Liposome Formulation
2.6.5. Osmolality Measurements of the Optimum EGCG Nano-Liposome Formulation
2.6.6. Transmission Electron Microscopy (TEM) of the Optimum EGCG Nano-Liposome Morphology
2.7. Determination of the Aerodynamic Behaviour of the Optimum EGCG Nano-Liposome Formulation Using NGI
2.8. Stability of EGCG Nano-Liposome after Nebulisation
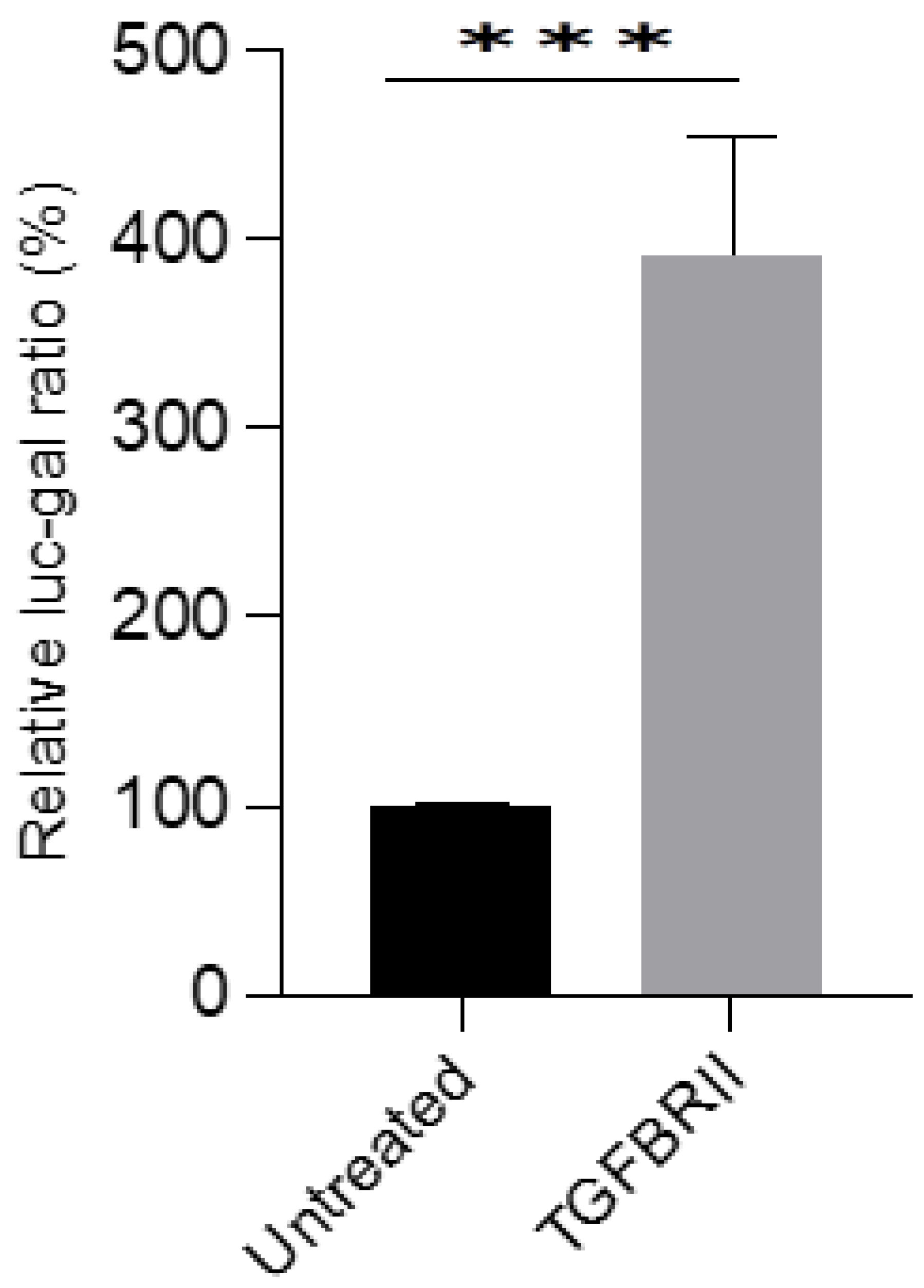
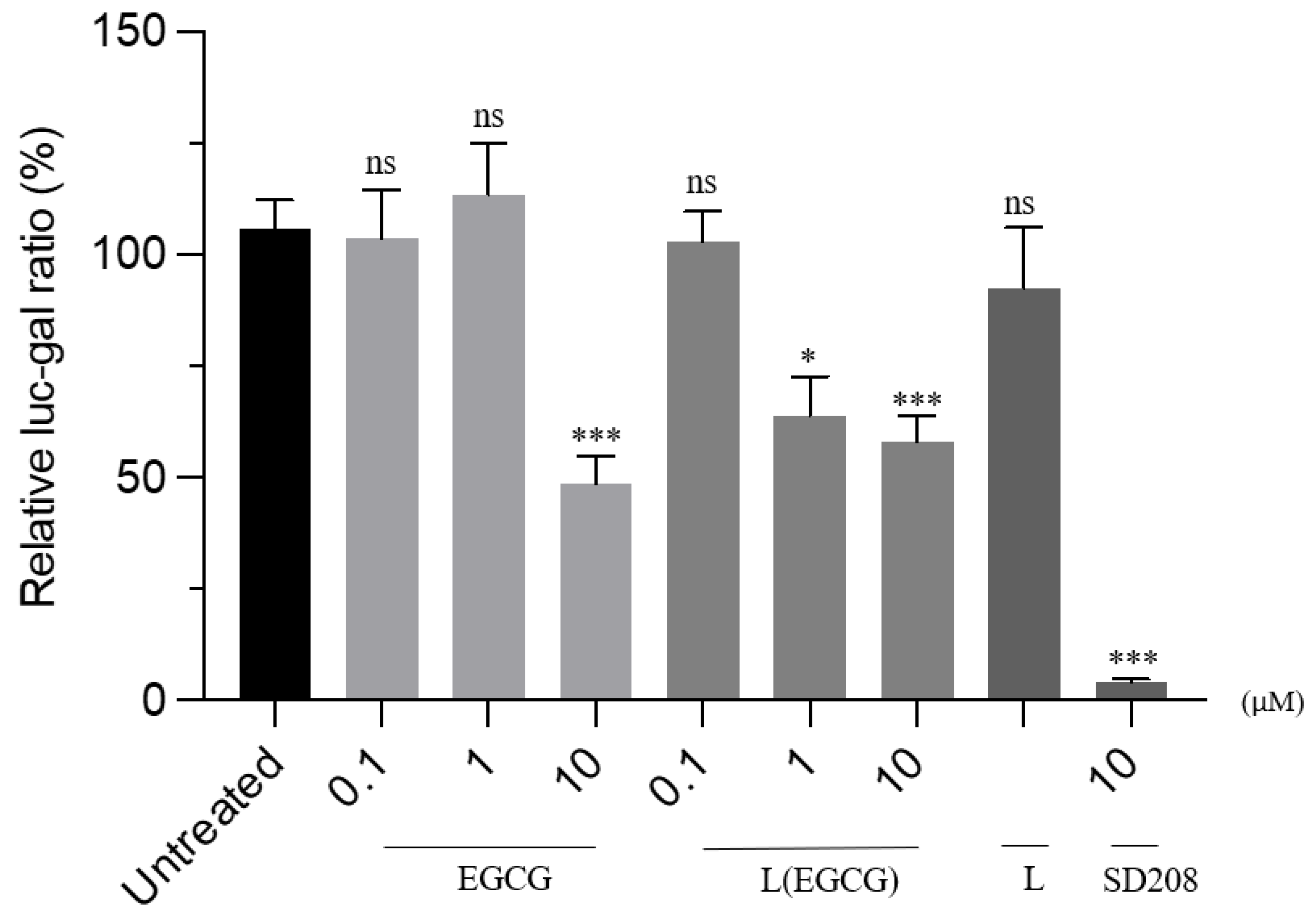
2.9. In Vitro Test of the Effectiveness of the Optimum EGCG Nano-Liposome Formulation and free EGCG on the TGF-β Pathway
2.10. Statistical Analysis
3. Results and Discussion
3.1. Optimisation of the Inhalable EGCG Using DOE
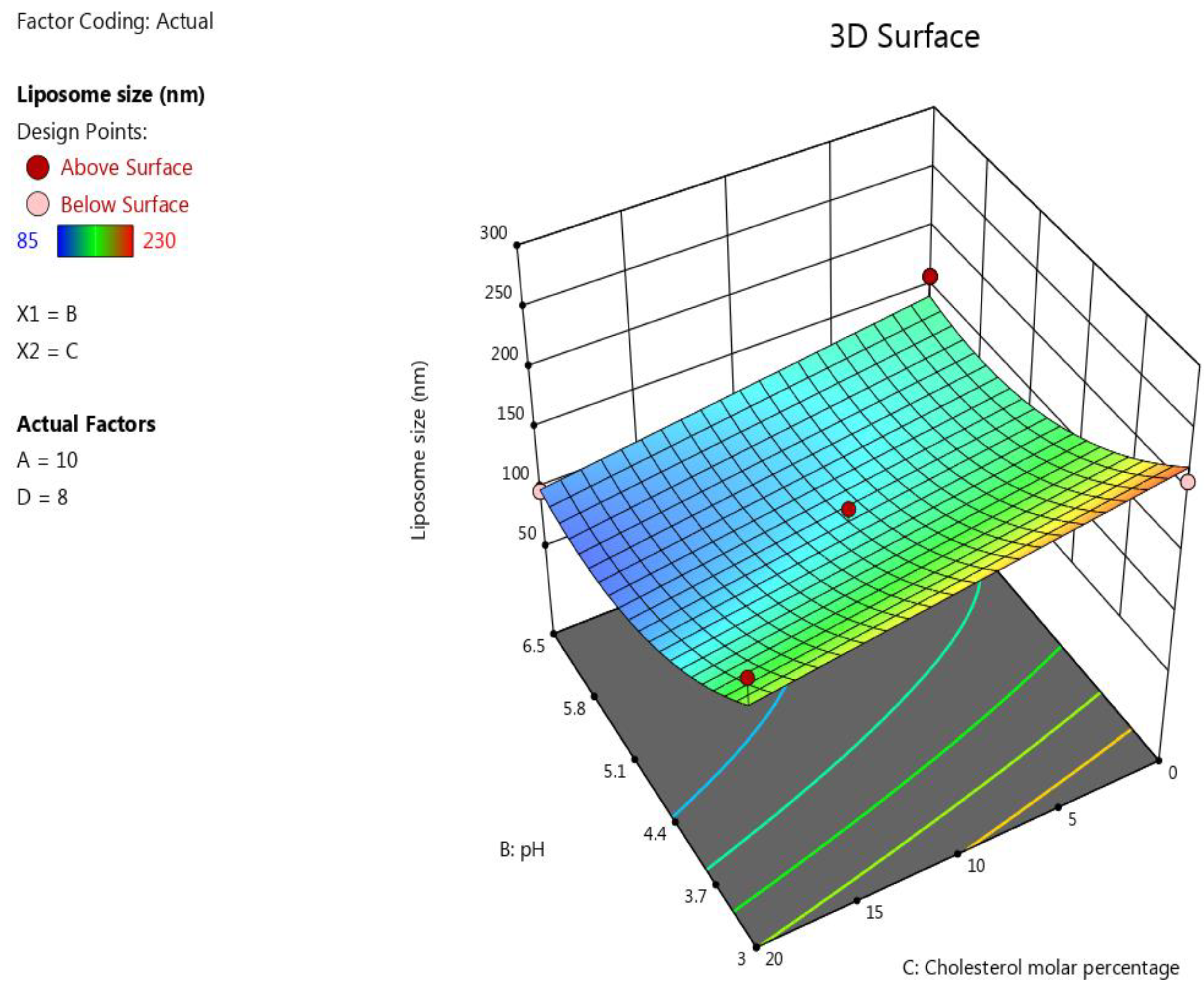
3.1.1. The Impact of the Formulation’s Composition on the Liposomes’ Size
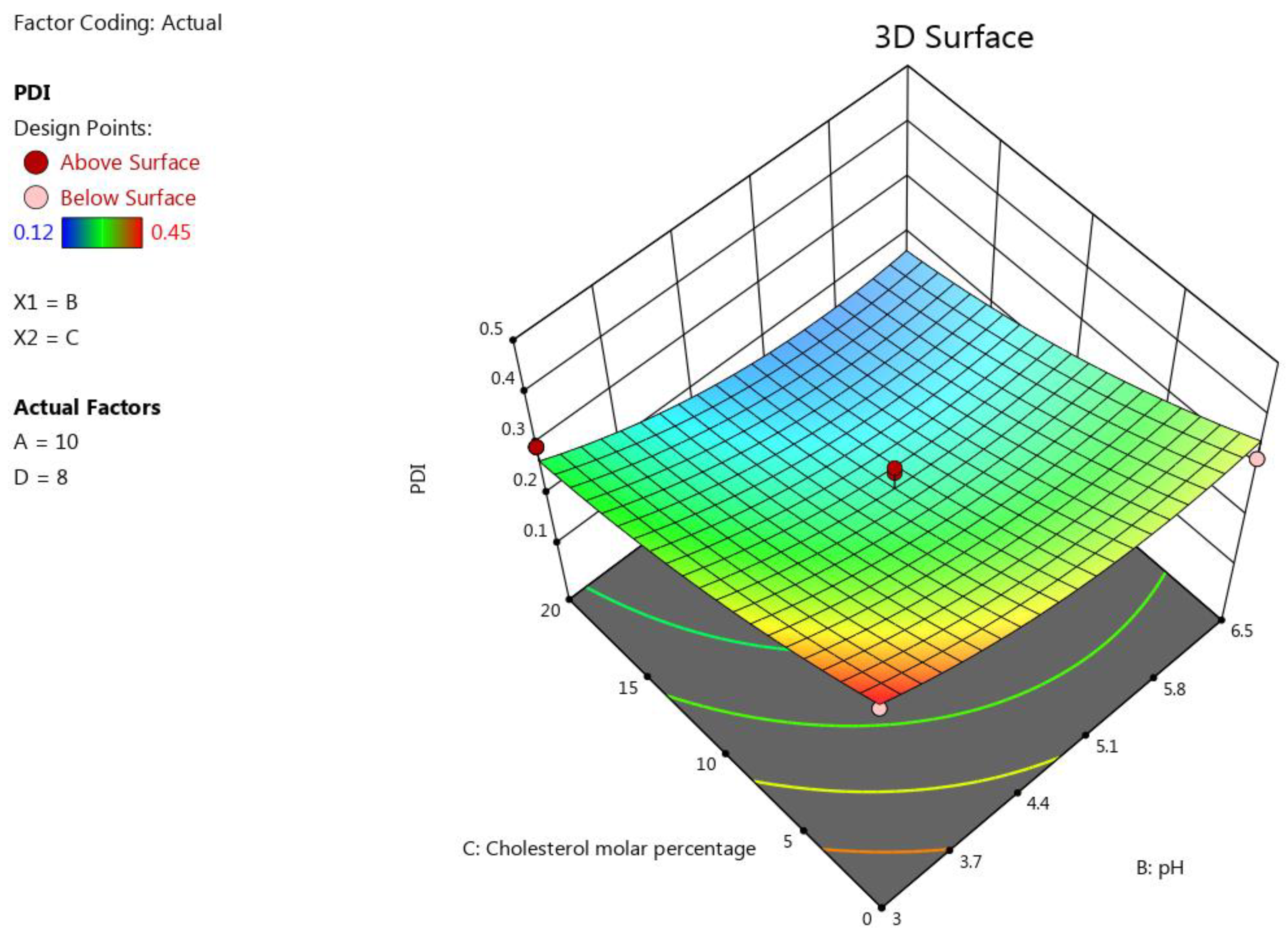
3.1.2. The Impact of the Formulation’s Composition on the Liposomes’ PDI
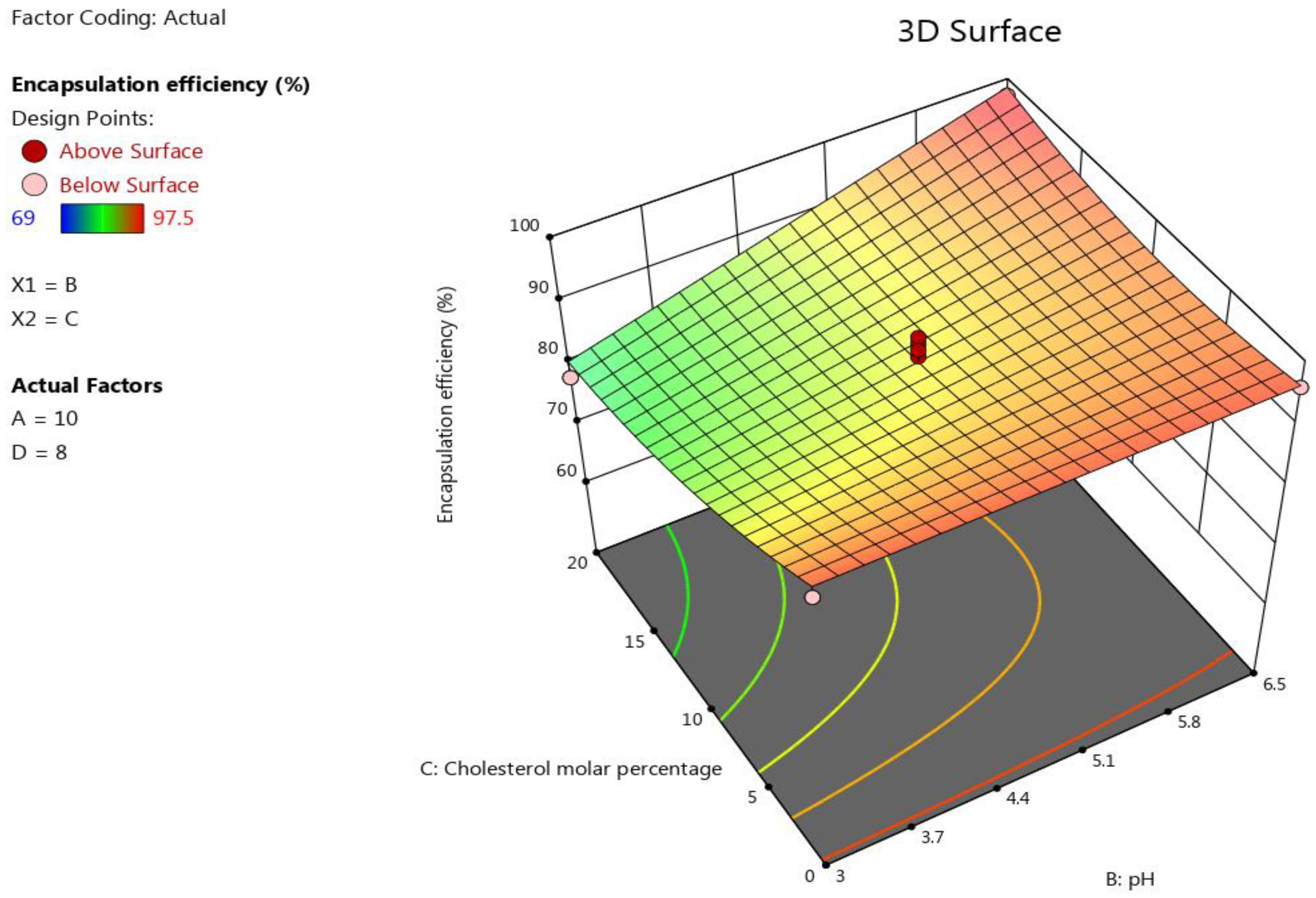
3.1.3. The Impact of the Formulation’s Composition on the Encapsulation Efficiency
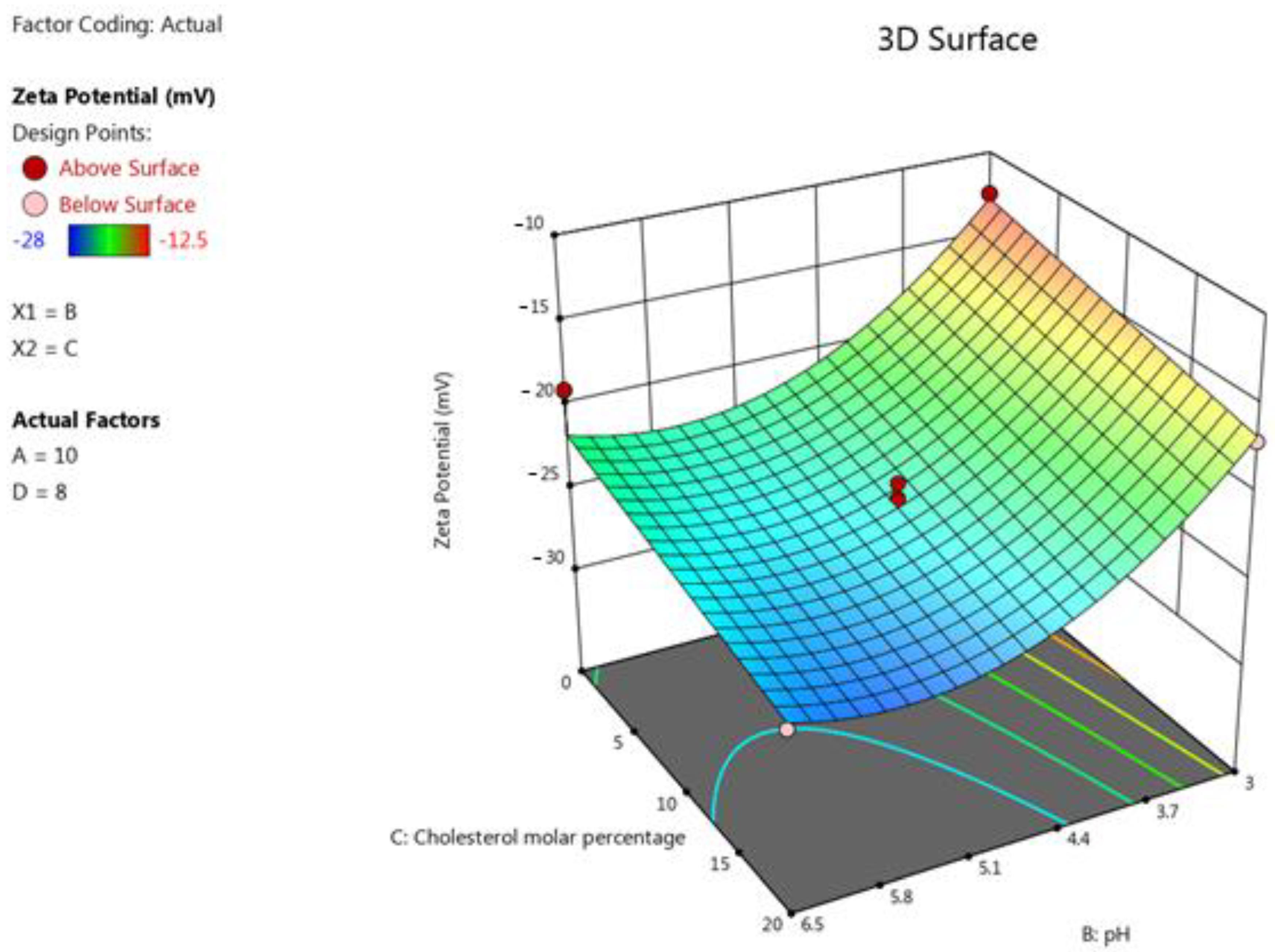
3.1.4. The Impact of the Formulation’s Composition on the Liposomes’ Zeta Potential
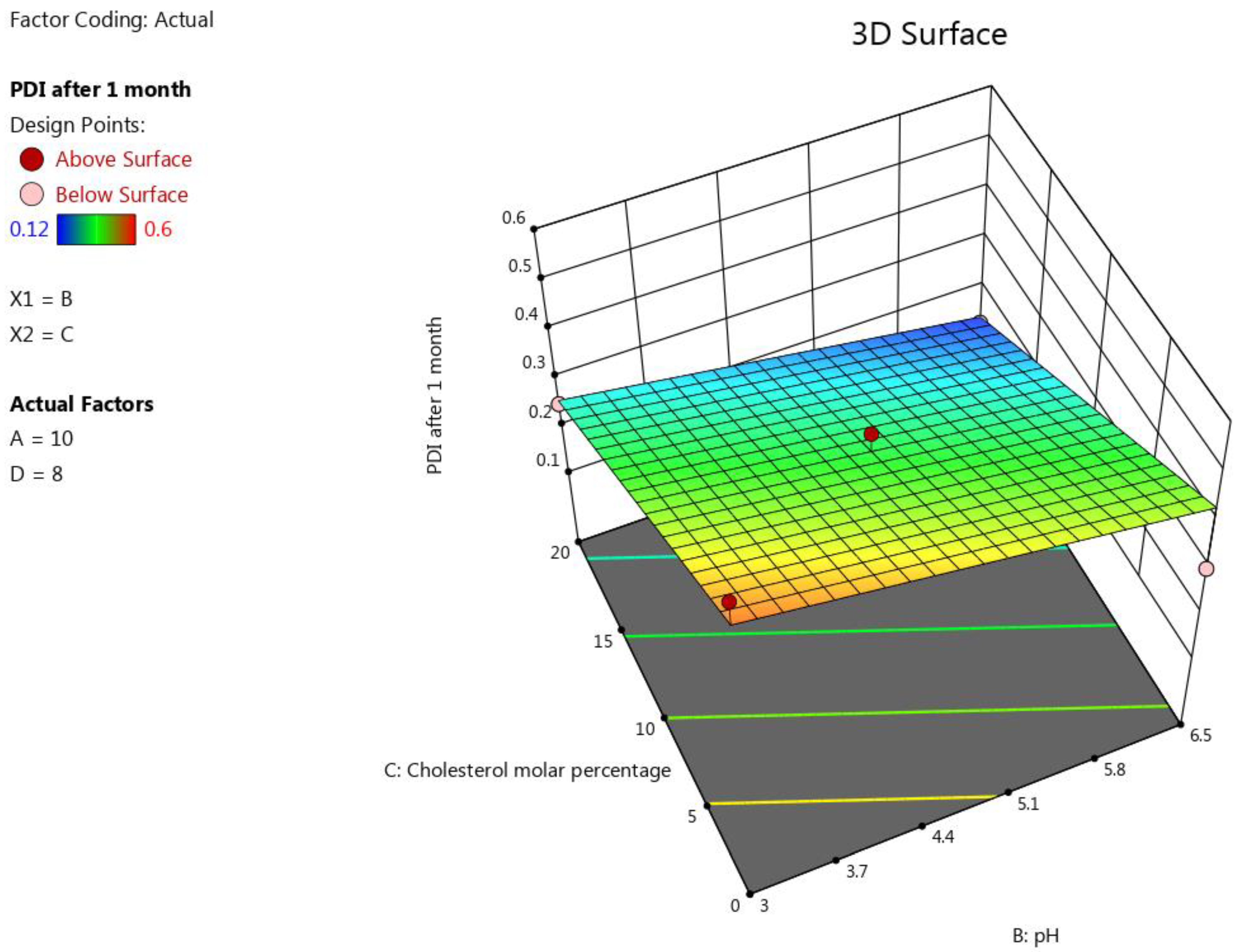
3.1.5. The Impact of the Formulation’s Composition on the Liposomes’ PDI after One Month
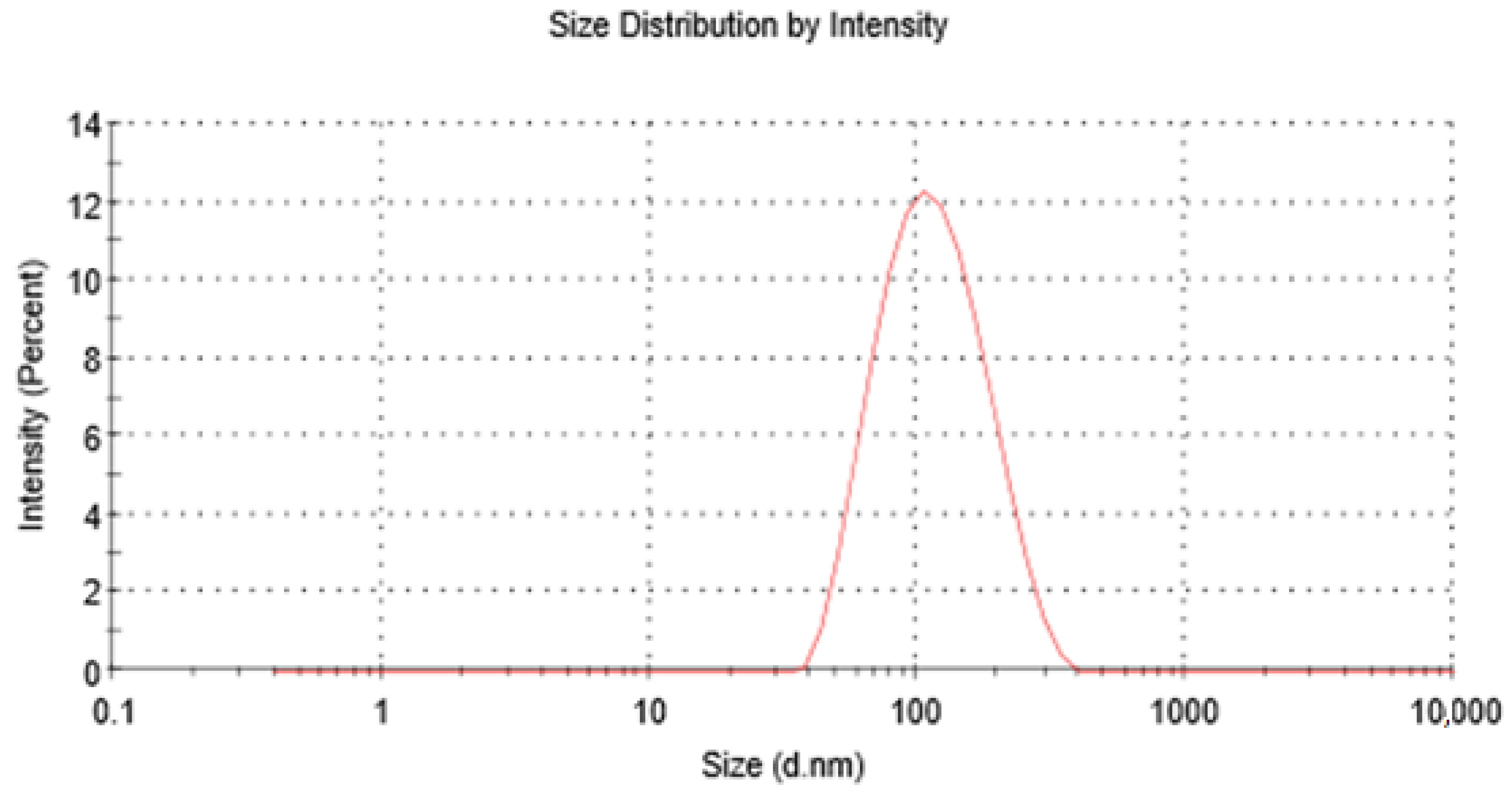
3.2. Preparation and Characterisation of the Optimum Proposed Nano-Liposome Formulation and Confirming the Predictivity of the Model
3.3. Viscosity Measurements of the Optimum EGCG Nano-Liposome Formulation
3.4. Osmolality Measurements of the Optimum EGCG Nano-Liposome Formulation
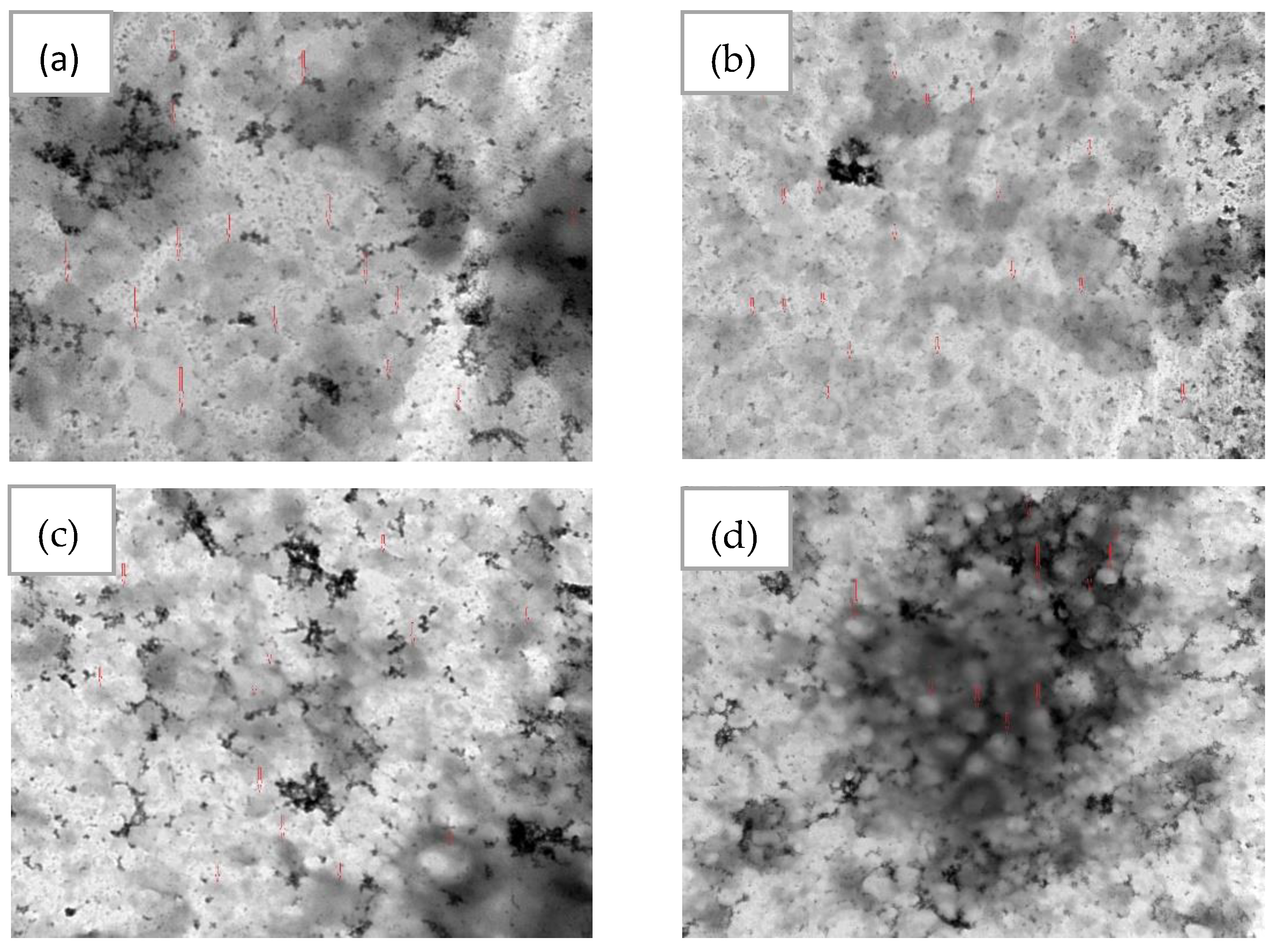
3.5. The Morphology of the Optimum EGCG Nano-Liposome
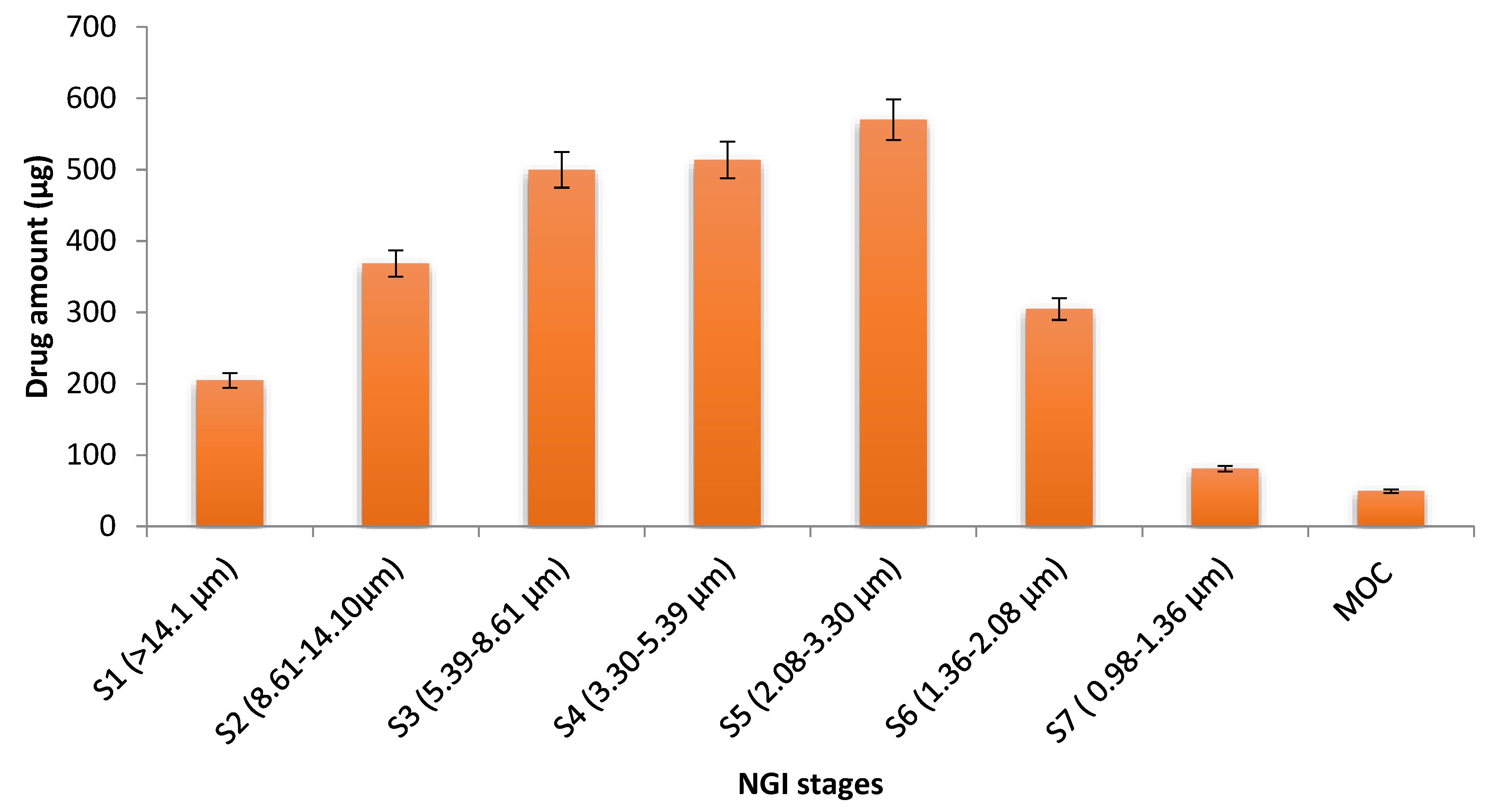
3.6. The Aerodynamic Behaviour of the Optimum EGCG Nano-Liposome Formulation

3.7. Stability of the Nebulised Liposome after Nebulisation
3.8. In Vitro Test of the Effectiveness of the Optimum EGCG Nano-Liposome Formulation and the Free EGCG on the TGF-β Pathway
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMPR2 | Bone morphogenetic protein type 2 receptor |
| CITDAS | Copley inhaler testing data analysis software |
| CV% | Coefficient of variation |
| DOE | Design of experiments |
| DLS | Dynamic light scattering. |
| DPPC | 1,2-dipalmitoyl-sn-glycero-3-phosphocholine |
| DPPG, sodium salt | 1,2-Dipalmitoyl-sn-glycerol-3-phosphate-rac-(1-glycerol) |
| D/L | Drug-to-lipid molar ratio |
| EF | Emitted fraction |
| EGCG | (-)-Epigallocatechin gallate |
| FDA | Food and Drug Administration |
| FPF | Fine particle fraction |
| GSD | Geometric standard deviation |
| HPLC | High-performance liquid chromatography |
| MCT | Monocrotaline |
| MMAD | Mass median aerodynamic diameter |
| MOC | Micro-orifice collector |
| NGI | Next-generation impactor |
| PAH | Pulmonary arterial hypertension |
| PBS | Phosphate-buffered saline |
| PDI | Polydispersity index |
| qPCR | Quantitative polymerase chain reaction |
| R2 | Coefficient of determination |
| TEM | Transmission electron microscopy |
| TGF-β | Transforming growth factor β |
| 2FI | Two-factor model interaction model |
References
- Keshavarz, A.; Kadry, H.; Alobaida, A.; Ahsan, F. Newer approaches and novel drugs for inhalational therapy for pulmonary arterial hypertension. Expert Opin. Drug Deliv. 2020, 17, 439–461. [Google Scholar] [CrossRef] [PubMed]
- Sharmin, N.; Nganwuchu, C.C.; Nasim, M.T. Targeting the TGF-β signaling pathway for resolution of pulmonary arterial hypertension. Trends Pharmacol. Sci. 2021, 42, 510–513. [Google Scholar] [CrossRef]
- Chowdhury, H.M.; Sharmin, N.; Yuzbasioglu Baran, M.; Long, L.; Morrell, N.W.; Trembath, R.C.; Nasim, M.T. BMPRII deficiency impairs apoptosis via the BMPRII-ALK1-BclX-mediated pathway in pulmonary arterial hypertension. Hum. Mol. Genet. 2019, 28, 2161–2173. [Google Scholar] [CrossRef] [PubMed]
- Nasim, T.; Ogo, T.; Ahmed, M.; Randall, R.; Chowdhury, H.M.; Snape, K.M.; Bradshaw, T.Y.; Southgate, L.; Lee, G.J.; Jackson, I.; et al. Molecular genetic characterization of SMAD signaling molecules in pulmonary arterial hypertension. Hum. Mutat. 2011, 32, 1385–1389. [Google Scholar] [CrossRef] [PubMed]
- Luo, Q.; Zhang, J.-R.; Li, H.-B.; Wu, D.-T.; Geng, F.; Corke, H.; Wei, X.-L.; Gan, R.-Y. Green extraction of antioxidant polyphenols from green tea (Camellia sinensis). Antioxidants 2020, 9, 785. [Google Scholar] [CrossRef]
- Reygaert, W.C. Green tea catechins: Their use in treating and preventing infectious diseases. BioMed Res. Int. 2018, 2018, 9105261. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Yan, W. Lipophilization of EGCG and effects on antioxidant activities. Food Chem. 2019, 272, 663–669. [Google Scholar] [CrossRef]
- Jiang, C.; Wang, L.; Huang, X.; Zhu, S.; Ma, C.; Wang, H. Identification and Antioxidant Abilities of Enzymatic-Transesterification (−)-Epigallocatechin-3-O-gallate Stearyl Derivatives in Non-Aqueous Systems. Antioxidants 2021, 10, 1282. [Google Scholar] [CrossRef] [PubMed]
- Elisa Hirsch, G.; Ricardo Nazario Viecili, P.; Spring de Almeida, A.; Nascimento, S.; Garcez Porto, F.; Otero, J.; Schmidt, A.; da Silva, B.; Migliorini Parisi, M.; Zeni Klafke, J. Natural products with antiplatelet action. Curr. Pharm. Des. 2017, 23, 1228–1246. [Google Scholar] [CrossRef] [PubMed]
- Zhu, T.-T.; Zhang, W.-F.; Luo, P.; He, F.; Ge, X.-Y.; Zhang, Z.; Hu, C.-P. Epigallocatechin-3-gallate ameliorates hypoxia-induced pulmonary vascular remodeling by promoting mitofusin-2-mediated mitochondrial fusion. Eur. J. Pharmacol. 2017, 809, 42–51. [Google Scholar] [CrossRef]
- Tabuchi, M.; Hayakawa, S.; Honda, E.; Ooshima, K.; Itoh, T.; Yoshida, K.; Park, A.-M.; Higashino, H.; Isemura, M.; Munakata, H. Epigallocatechin-3-gallate suppresses transforming growth factor-beta signaling by interacting with the transforming growth factor-beta type II receptor. World 2013, 3, 100–107. [Google Scholar] [CrossRef]
- Saeki, K.; Hayakawa, S.; Nakano, S.; Ito, S.; Oishi, Y.; Suzuki, Y.; Isemura, M. In vitro and in silico studies of the molecular interactions of epigallocatechin-3-O-gallate (EGCG) with proteins that explain the health benefits of green tea. Molecules 2018, 23, 1295. [Google Scholar] [CrossRef]
- Chowdhury, A.; Sarkar, J.; Chakraborti, T.; Chakraborti, S. Role of Spm–Cer-S1P signalling pathway in MMP-2 mediated U46619-induced proliferation of pulmonary artery smooth muscle cells: Protective role of epigallocatechin-3-gallate. Cell Biochem. Funct. 2015, 33, 463–477. [Google Scholar] [CrossRef]
- Sarkar, J.; Chakraborti, T.; Chowdhury, A.; Bhuyan, R.; Chakraborti, S. Protective role of epigallocatechin-3-gallate in NADPH oxidase-MMP2-Spm-Cer-S1P signalling axis mediated ET-1 induced pulmonary artery smooth muscle cell proliferation. J. Cell Commun. Signal. 2019, 13, 473–489. [Google Scholar] [CrossRef]
- Granja, A.; Pinheiro, M.; Reis, S. Epigallocatechin gallate nanodelivery systems for cancer therapy. Nutrients 2016, 8, 307. [Google Scholar] [CrossRef] [PubMed]
- Dai, W.; Ruan, C.; Zhang, Y.; Wang, J.; Han, J.; Shao, Z.; Sun, Y.; Liang, J. Bioavailability enhancement of EGCG by structural modification and nano-delivery: A review. J. Funct. Foods 2020, 65, 103732. [Google Scholar] [CrossRef]
- Krupkova, O.; Ferguson, S.J.; Wuertz-Kozak, K. Stability of (−)-epigallocatechin gallate and its activity in liquid formulations and delivery systems. J. Nutr. Biochem. 2016, 37, 1–12. [Google Scholar] [CrossRef]
- Ruengdech, A.; Siripatrawan, U. Application of catechin nanoencapsulation with enhanced antioxidant activity in high pressure processed catechin-fortified coconut milk. Lwt 2021, 140, 110594. [Google Scholar] [CrossRef]
- Widyaningrum, N.; Fudholi, A.; Sudarsono, S.E.; Setyowati, E. Stability of epigallocatechin gallate (EGCG) from green tea (Camellia sinensis) and its antibacterial activity against Staphylococcus epidermidis ATCC 35984 and Propionibacterium acnes ATCC 6919. Asian J. Biol. Sci 2015, 8, 93–101. [Google Scholar] [CrossRef]
- Yang, C.S.; Hong, J.; Hou, Z.; Sang, S. Green tea polyphenols: Antioxidative and prooxidative effects. J. Nutr. 2004, 134, 3181S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mokra, D.; Adamcakova, J.; Mokry, J. Green Tea Polyphenol (-)-Epigallocatechin-3-Gallate (EGCG): A Time for a New Player in the Treatment of Respiratory Diseases? Antioxidants 2022, 11, 1566. [Google Scholar] [CrossRef] [PubMed]
- De Pace, R.C.C.; Liu, X.; Sun, M.; Nie, S.; Zhang, J.; Cai, Q.; Gao, W.; Pan, X.; Fan, Z.; Wang, S. Anticancer activities of (−)-epigallocatechin-3-gallate encapsulated nanoliposomes in MCF7 breast cancer cells. J. Liposome Res. 2013, 23, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Bulbake, U.; Doppalapudi, S.; Kommineni, N.; Khan, W. Liposomal formulations in clinical use: An updated review. Pharmaceutics 2017, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.P.; Ghoshal, D.; Pawar, A.P.; Kadam, S.S.; Dhapte-Pawar, V.S. Recent advances in inhalable liposomes for treatment of pulmonary diseases: Concept to clinical stance. J. Drug Deliv. Sci. Technol. 2020, 56, 101509. [Google Scholar] [CrossRef]
- Zhao, J.; Su, J.; Qin, L.; Zhang, X.; Mao, S. Exploring the influence of inhaled liposome membrane fluidity on its interaction with pulmonary physiological barriers. Biomater. Sci. 2020, 8, 6786–6797. [Google Scholar] [CrossRef]
- Deng, Q.; Deng, L.; Miao, Y.; Guo, X.; Li, Y. Particle deposition in the human lung: Health implications of particulate matter from different sources. Environ. Res. 2019, 169, 237–245. [Google Scholar] [CrossRef]
- Rudokas, M.; Najlah, M.; Alhnan, M.A.; Elhissi, A. Liposome delivery systems for inhalation: A critical review highlighting formulation issues and anticancer applications. Med. Princ. Pract. 2016, 25, 60–72. [Google Scholar] [CrossRef]
- Unida, S.; Ito, Y.; Onodera, R.; Tahara, K.; Takeuchi, H. Inhalation properties of water-soluble drug loaded liposomes atomized by nebulizer. Asian J. Pharm. Sci. 2016, 11, 205–206. [Google Scholar] [CrossRef]
- Luo, X.; Guan, R.; Chen, X.; Tao, M.; Ma, J.; Zhao, J. Optimization on condition of epigallocatechin-3-gallate (EGCG) nanoliposomes by response surface methodology and cellular uptake studies in Caco-2 cells. Nanoscale Res. Lett. 2014, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Laudadio, E.; Minnelli, C.; Amici, A.; Massaccesi, L.; Mobbili, G.; Galeazzi, R. Liposomal formulations for an efficient encapsulation of epigallocatechin-3-gallate: An in-silico/experimental approach. Molecules 2018, 23, 441. [Google Scholar] [CrossRef] [Green Version]
- Barbălată, C.I.; Tomuță, I.; Achim, M.; Boșca, A.B.; Cherecheș, G.; Sorițău, O.; Porfire, A.S. Application of the QbD Approach in the Development of a Liposomal Formulation with EGCG. J. Pharm. Innov. 2021, 17, 867–880. [Google Scholar] [CrossRef]
- Lindenberg, F.; Sichel, F.; Lechevrel, M.; Respaud, R.; Saint-Lorant, G. Evaluation of lung cell toxicity of surfactants for inhalation route. J. Toxicol. Risk Assess 2019, 5, 1–4. [Google Scholar] [CrossRef]
- Fang, J.-Y.; Lee, W.-R.; Shen, S.-C.; Huang, Y.-L. Effect of liposome encapsulation of tea catechins on their accumulation in basal cell carcinomas. J. Dermatol. Sci. 2006, 42, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Zaru, M.; Mourtas, S.; Klepetsanis, P.; Fadda, A.M.; Antimisiaris, S.G. Liposomes for drug delivery to the lungs by nebulization. Eur. J. Pharm. Biopharm. 2007, 67, 655–666. [Google Scholar] [CrossRef]
- Silvius, J.R. Thermotropic phase transitions of pure lipids in model membranes and their modifications by membrane proteins. Lipid-Protein Interact. 1982, 2, 239–281. [Google Scholar]
- Myrdal, P.B.; Sheth, P.; Stein, S.W. Advances in metered dose inhaler technology: Formulation development. Aaps Pharmscitech 2014, 15, 434–455. [Google Scholar] [CrossRef]
- Zhu, B.; Traini, D.; Chan, H.-K.; Young, P.M. The effect of ethanol on the formation and physico-chemical properties of particles generated from budesonide solution-based pressurized metered-dose inhalers. Drug Dev. Ind. Pharm. 2013, 39, 1625–1637. [Google Scholar] [CrossRef]
- Srichana, T.; Chunhachaichana, C.; Suedee, R.; Sawatdee, S.; Changsan, N. Oral inhalation of cannabidiol delivered from a metered dose inhaler to alleviate cytokine production induced by SARS-CoV-2 and pollutants. J. Drug Deliv. Sci. Technol. 2022, 76, 103805. [Google Scholar] [CrossRef]
- Bangham, A.D.; Standish, M.M.; Watkins, J.C. Diffusion of univalent ions across the lamellae of swollen phospholipids. J. Mol. Biol. 1965, 13, 238-IN227. [Google Scholar] [CrossRef] [PubMed]
- Marwah, M.; Perrie, Y.; Badhan, R.K.S.; Lowry, D. Intracellular uptake of EGCG-loaded deformable controlled release liposomes for skin cancer. J. Liposome Res. 2020, 30, 136–149. [Google Scholar] [CrossRef]
- Manohar, M.; Joseph, J.; Selvaraj, T.; Sivakumar, D. Application of Box Behnken design to optimize the parameters for turning Inconel 718 using coated carbide tools. Int. J. Sci. Eng. Res. 2013, 4, 620–644. [Google Scholar]
- Chountoulesi, M.; Naziris, N.; Pippa, N.; Demetzos, C. The significance of drug-to-lipid ratio to the development of optimized liposomal formulation. J. Liposome Res. 2018, 28, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Maritim, S.; Boulas, P.; Lin, Y. Comprehensive analysis of liposome formulation parameters and their influence on encapsulation, stability and drug release in glibenclamide liposomes. Int. J. Pharm. 2021, 592, 120051. [Google Scholar] [CrossRef]
- Deshantri, A.K.; Metselaar, J.M.; Zagkou, S.; Storm, G.; Mandhane, S.N.; Fens, M.H.; Schiffelers, R.M. Development and characterization of liposomal formulation of bortezomib. Int. J. Pharm. X 2019, 1, 100011. [Google Scholar] [CrossRef]
- Roy, B.; Guha, P.; Bhattarai, R.; Nahak, P.; Karmakar, G.; Chettri, P.; Panda, A.K. Influence of lipid composition, pH, and temperature on physicochemical properties of liposomes with curcumin as model drug. J. Oleo Sci. 2016, 65, 399–411. [Google Scholar] [CrossRef]
- Briuglia, M.L.; Rotella, C.; McFarlane, A.; Lamprou, D.A. Influence of cholesterol on liposome stability and on in vitro drug release. Drug Deliv. Transl. Res. 2015, 5, 231–242. [Google Scholar] [CrossRef]
- Carugo, D.; Bottaro, E.; Owen, J.; Stride, E.; Nastruzzi, C. Liposome production by microfluidics: Potential and limiting factors. Sci. Rep. 2016, 6, 1–15. [Google Scholar] [CrossRef]
- Weber, A.; Morlin, G.; Cohen, M.; Williams-Warren, J.; Ramsey, B.; Smith, A. Effect of nebulizer type and antibiotic concentration on device performance. Pediatr. Pulmonol. 1997, 23, 249–260. [Google Scholar] [CrossRef]
- Joseph, E.; Singhvi, G. Multifunctional nanocrystals for cancer therapy: A potential nanocarrier. Nanomater. Drug Deliv. Ther. 2019, 4, 91–116. [Google Scholar]
- da Silva, P.A.; Rodrigues, L.M.; Moes, A. DPPG liposomes as preferential vehicles for" human-identical" ceramides. J. Appl. Cosmetol. 1998, 16, 65–72. [Google Scholar]
- Franken, L.E.; Boekema, E.J.; Stuart, M.C. Transmission electron microscopy as a tool for the characterization of soft materials: Application and interpretation. Adv. Sci. 2017, 4, 1600476. [Google Scholar] [CrossRef]
- Baxa, U. Imaging of liposomes by transmission electron microscopy. In Characterization of Nanoparticles Intended for Drug Delivery; Springer: Berlin/Heidelberg, Germany, 2018; pp. 73–88. [Google Scholar]
- Berg, E.; Svensson, J.O.; Asking, L. Determination of nebulizer droplet size distribution: A method based on impactor refrigeration. J. Aerosol Med. 2007, 20, 97–104. [Google Scholar] [CrossRef]
- Chan, J.G.Y.; Kwok, P.C.L.; Young, P.M.; Chan, H.-K.; Traini, D. Mannitol delivery by vibrating mesh nebulisation for enhancing mucociliary clearance. J. Pharm. Sci. 2011, 100, 2693–2702. [Google Scholar] [CrossRef]
- Chowdhury, H.; Siddiqui, M.; Kanneganti, S.; Sharmin, N.; Chowdhury, M.; Nasim, M.T. Aminoglycoside-mediated promotion of translation readthrough occurs through a non-stochastic mechanism that competes with translation termination. Hum. Mol. Genet. 2018, 27, 373–384. [Google Scholar] [CrossRef] [Green Version]
- Shu, Z.; Yu, M.; Zeng, G.; Zhang, X.; Wu, L.; Tan, X. Epigallocatechin-3-gallate inhibits proliferation of human aortic smooth muscle cells via up-regulating expression of mitofusin 2. Eur. J. Cell Biol. 2014, 93, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Ok, W.-J.; Cho, H.-J.; Kim, H.-H.; Lee, D.-H.; Kang, H.-Y.; Kwon, H.-W.; Rhee, M.H.; Kim, M.; Park, H.-J. Epigallocatechin-3-gallate has an anti-platelet effect in a cyclic AMP-dependent manner. J. Atheroscler. Thromb. 2012, 19, 1204090486. [Google Scholar] [CrossRef] [PubMed]
- Shutava, T.G.; Balkundi, S.S.; Vangala, P.; Steffan, J.J.; Bigelow, R.L.; Cardelli, J.A.; O’Neal, D.P.; Lvov, Y.M. Layer-by-layer-coated gelatin nanoparticles as a vehicle for delivery of natural polyphenols. ACS Nano 2009, 3, 1877–1885. [Google Scholar] [CrossRef]
- Lombardo, D.; Kiselev, M.A. Methods of Liposomes Preparation: Formation and Control Factors of Versatile Nanocarriers for Biomedical and Nanomedicine Application. Pharmaceutics 2022, 14, 543. [Google Scholar] [CrossRef] [PubMed]
- Eskandari, V.; Sadeghi, M.; Hadi, A. Physical and chemical properties of nano-liposome, application in nano medicine. J. Comput. Appl. Mech. 2021, 52, 751–767. [Google Scholar]
- Bozzuto, G.; Molinari, A. Liposomes as nanomedical devices. Int. J. Nanomed. 2015, 10, 975. [Google Scholar] [CrossRef] [PubMed]
- Van Tran, V.; Moon, J.-Y.; Lee, Y.-C. Liposomes for delivery of antioxidants in cosmeceuticals: Challenges and development strategies. J. Control Release 2019, 300, 114–140. [Google Scholar] [CrossRef]
- Kataria, S.; Sandhu, P.; Bilandi, A.; Akanksha, M.; Kapoor, B. Stealth liposomes: A review. Int. J. Res. Ayurveda Pharm. 2011, 2, 1534–1538. [Google Scholar]
- Al Ayoub, Y.; Gopalan, R.C.; Najafzadeh, M.; Mohammad, M.A.; Anderson, D.; Paradkar, A.; Assi, K.H. Development and evaluation of nanoemulsion and microsuspension formulations of curcuminoids for lung delivery with a novel approach to understanding the aerosol performance of nanoparticles. Int. J. Pharm. 2019, 557, 254–263. [Google Scholar] [CrossRef]
- Garidel, P.; Johann, C.; Mennicke, L.; Blume, A. The mixing behavior of pseudobinary phosphatidylcholine-phosphatidylglycerol mixtures as a function of pH and chain length. Eur. Biophys. J. 1997, 26, 447–459. [Google Scholar] [CrossRef]
- Brgles, M.; Jurašin, D.; Sikirić, M.D.; Frkanec, R.; Tomašić, J. Entrapment of ovalbumin into liposomes—Factors affecting entrapment efficiency, liposome size, and zeta potential. J. Liposome Res. 2008, 18, 235–248. [Google Scholar] [CrossRef]
- Pathak, S.K.; Mishra, R.; Kumar, S.; Prakash, G.; Parthasarthy, R. Effect of cholesterol concentration on size of liposome. J. Pharm. Biol. Sci 2013, 1, 50–53. [Google Scholar] [CrossRef]
- Mozafari, M.R. Nanoliposomes: Preparation and analysis. In Liposomes; Springer: Berlin/Heidelberg, Germany, 2010; pp. 29–50. [Google Scholar]
- Popova, A.V.; Hincha, D.K. Effects of cholesterol on dry bilayers: Interactions between phosphatidylcholine unsaturation and glycolipid or free sugar. Biophys. J. 2007, 93, 1204–1214. [Google Scholar] [CrossRef]
- Shokri, M.; Tavallaie, M.; Hosseini, S.M. Effect of lyophilization on the size and polydispersity of unilamellar and multilamellar liposomes. J. Nanotechnol. Mater. Sci. 2016, 3, 37–40. [Google Scholar]
- Danaei, M.; Dehghankhold, M.; Ataei, S.; Hasanzadeh Davarani, F.; Javanmard, R.; Dokhani, A.; Khorasani, S.; Mozafari, M. Impact of particle size and polydispersity index on the clinical applications of lipidic nanocarrier systems. Pharmaceutics 2018, 10, 57. [Google Scholar] [CrossRef] [PubMed]
- Gyamera, B.; Kim, Y.-H. Preparation and Characterization of Liposomes Containing Green Tea and Roselle Extracts to be Used in Cosmetics. J. Int. Dev. Coop. 2019, 14, 131–160. [Google Scholar] [CrossRef]
- Elhissi, A.; Hidayat, K.; Phoenix, D.A.; Mwesigwa, E.; Crean, S.; Ahmed, W.; Faheem, A.; Taylor, K.M. Air-jet and vibrating-mesh nebulization of niosomes generated using a particulate-based proniosome technology. Int. J. Pharm. 2013, 444, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Elhissi, A.M.; Giebultowicz, J.; Stec, A.A.; Wroczynski, P.; Ahmed, W.; Alhnan, M.A.; Phoenix, D.; Taylor, K.M. Nebulization of ultradeformable liposomes: The influence of aerosolization mechanism and formulation excipients. Int. J. Pharm. 2012, 436, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Elhissi, A.; Faizi, M.; Naji, W.; Gill, H.; Taylor, K. Physical stability and aerosol properties of liposomes delivered using an air-jet nebulizer and a novel micropump device with large mesh apertures. Int. J. Pharm. 2007, 334, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Bridges, P.A.; Taylor, K.M. An investigation of some of the factors influencing the jet nebulisation of liposomes. Int. J. Pharm. 2000, 204, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Nimmano, N.; Somavarapu, S.; Taylor, K.M. Aerosol characterisation of nebulised liposomes co-loaded with erlotinib and genistein using an abbreviated cascade impactor method. Int. J. Pharm. 2018, 542, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Beck-Broichsitter, M.; Prüfer, N.; Oesterheld, N.; Seeger, W.; Schmehl, T. Nebulization of active pharmaceutical ingredients with the eFlow® rapid: Impact of formulation variables on aerodynamic characteristics. J. Pharm. Sci. 2014, 103, 2585–2589. [Google Scholar] [CrossRef]
- Carvalho, T.C.; Peters, J.I.; Williams, R.O., III. Influence of particle size on regional lung deposition—What evidence is there? Int. J. Pharm. 2011, 406, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Fischer, D. APV Focus Group Drug Delivery. APV Drug Delivery Focus Group Newsletter. 3 November 2018. Available online: https://www.apv-mainz.de/fileadmin/dateiablage/apv-mainz/Newsletter_Drug_Delivery/APV-DD-Newsletter_2018-03_final1.pdf (accessed on 24 January 2023).
- Li, Z.; Perkins, W.; Cipolla, D. Robustness of aerosol delivery of amikacin liposome inhalation suspension using the eFlow® Technology. Eur. J. Pharm. Biopharm. 2021, 166, 10–18. [Google Scholar] [CrossRef] [PubMed]
- O’Callaghan, C.; Barry, P.W. The science of nebulised drug delivery. Thorax 1997, 52, S31. [Google Scholar] [CrossRef]
- Heyder, J.; Gebhart, J.; Rudolf, G.; Schiller, C.F.; Stahlhofen, W. Deposition of particles in the human respiratory tract in the size range 0.005–15 μm. J. Aerosol Sci. 1986, 17, 811–825. [Google Scholar] [CrossRef]
- Marple, V.A.; Olson, B.A.; Santhanakrishnan, K.; Roberts, D.L.; Mitchell, J.P.; Hudson-Curtis, B.L. Next generation pharmaceutical impactor: A new impactor for pharmaceutical inhaler testing. Part III. Extension of archival calibration to 15 L/min. J. Aerosol Med. 2004, 17, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Waters, V.; Ratjen, F. Inhaled liposomal amikacin. Expert Rev. Respir. Med. 2014, 8, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, S.; Khan, I.; Korale, O.; Alhnan, M.A.; Ahmed, W.; Najlah, M.; Taylor, K.M.; Elhissi, A. A simple approach to predict the stability of phospholipid vesicles to nebulization without performing aerosolization studies. Int. J. Pharm. 2016, 502, 18–27. [Google Scholar] [CrossRef] [PubMed]
- de Jesús Valle, M.J.; Gil González, P.; Prata Ribeiro, M.; Araujo, A.R.; Sánchez Navarro, A. Sildenafil citrate liposomes for pulmonary delivery by ultrasonic nebulization. Appl. Sci. 2018, 8, 1291. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Independent Variables | Levels | |||
|---|---|---|---|---|
| Low (−1) | Mid-Point (0) | High (+1) | ||
| A | Total lipid concentration (mg/mL) | 5 | 10 | 15 |
| B | The pH of the dispersion media | 3 | 4.75 | 6.5 |
| C | Molar percentage of cholesterol (%) | 0 | 10 | 20 |
| D | D/L molar ratio (%) | 5 | 8 | 11 |
| F1 | F2 | F3 | F4 | R1 | R2 | R3 | R4 | R5 | |
|---|---|---|---|---|---|---|---|---|---|
| Run | A (mg/mL) | B | C (%) | D (%) | Liposome Size (nm)± SD | PDI ± SD | EE (%) | Zeta Potential (mV) | PDI after 1 Month ± SD |
| 1 | 10 | 6.5 | 20 | 8 | 98 ± 1.3 | 0.12 ± 0.01 | 95 | −26 | 0.12 ± 0.01 |
| 2 | 10 | 4.75 | 0 | 5 | 94 ± 0.4 | 0.33 ± 0.01 | 96.5 | −28 | 0.55 ± 0.12 |
| 3 | 10 | 3 | 20 | 8 | 200 ± 1.6 | 0.30 ± 0.02 | 78 | −17 | 0.25 ± 0.06 |
| 4 | 10 | 4.75 | 20 | 11 | 102 ± 0.4 | 0.16 ± 0.00 | 87.3 | −26 | 0.28 ± 0.01 |
| 5 | 10 | 3 | 10 | 11 | 230 ± 10.3 | 0.40 ± 0.05 | 80.3 | −15 | 0.50 ± 0.05 |
| 6 | 10 | 6.5 | 10 | 5 | 85 ± 0.60 | 0.25 ± 0.01 | 88.5 | −24 | 0.38 ± 0.02 |
| 7 | 15 | 4.75 | 10 | 5 | 105 ± 1.5 | 0.27 ± 0.00 | 86 | −24 | 0.38 ± 0.01 |
| 8 | 10 | 3 | 10 | 5 | 165 ± 1.6 | 0.28 ± 0.01 | 91.5 | −15 | 0.26 ± 0.01 |
| 9 | 10 | 6.5 | 10 | 11 | 144 ± 1.4 | 0.26 ± 0.02 | 94 | −21.5 | 0.25 ± 0.02 |
| 10 | 15 | 6.5 | 10 | 8 | 120 ± 0.5 | 0.26 ± 0.00 | 94 | −26.5 | 0.38 ± 0.01 |
| 11 | 10 | 4.75 | 10 | 8 | 135 ± 9.5 | 0.22 ± 0.01 | 90 | −22.9 | 0.38 ± 0.01 |
| 12 | 10 | 4.75 | 10 | 8 | 112 ± 1.9 | 0.28 ± 0.03 | 91 | −26 | 0.30 ± 0.03 |
| 13 | 5 | 4.75 | 10 | 5 | 120 ± 1.0 | 0.17 ± 0.05 | 82.5 | −26 | 0.30 ± 0.03 |
| 14 | 5 | 3 | 10 | 8 | 220 ± 3.5 | 0.40 ± 0.03 | 69 | −13 | 0.50 ± 0.03 |
| 15 | 10 | 4.75 | 0 | 11 | 170 ± 2.7 | 0.40 ± 0.05 | 95.5 | −18 | 0.60 ± 0.03 |
| 16 | 15 | 3 | 10 | 8 | 174 ± 2.3 | 0.25 ± 0.02 | 96 | −16 | 0.33 ± 0.02 |
| 17 | 5 | 4.75 | 10 | 11 | 119 ± 0.3 | 0.22 ± 0.01 | 77.5 | −25 | 0.29 ± 0.03 |
| 18 | 10 | 6.5 | 0 | 8 | 160 ± 1.1 | 0.32 ± 0.02 | 96 | −19 | 0.30 ± 0.01 |
| 19 | 15 | 4.75 | 10 | 11 | 138 ± 0.2 | 0.21 ± 0.01 | 95 | −22 | 0.21 ± 0.01 |
| 20 | 15 | 4.75 | 0 | 8 | 167 ± 2.3 | 0.36 ± 0.01 | 95.5 | −21.5 | 0.50 ± 0.05 |
| 21 | 5 | 4.75 | 0 | 8 | 180 ± 1.7 | 0.39 ± 0.02 | 93 | −18.5 | 0.50 ± 0.02 |
| 22 | 15 | 4.75 | 20 | 8 | 109 ± 0.4 | 0.20 ± 0.01 | 92.5 | −24 | 0.21 ± 0.01 |
| 23 | 5 | 4.75 | 20 | 8 | 110 ± 0.3 | 0.19 ± 0.01 | 81 | −24 | 0.21 ± 0.01 |
| 24 | 5 | 6.5 | 10 | 8 | 120 ± 0.5 | 0.25 ± 0.00 | 92 | −25 | 0.26 ± 0.01 |
| 25 | 10 | 4.75 | 20 | 5 | 100 ± 1.2 | 0.16 ± 0.01 | 93.5 | −24 | 0.20 ± 0.02 |
| 26 | 10 | 4.75 | 10 | 8 | 116 ± 1.1 | 0.22 ± 0.01 | 94 | −24 | 0.28 ± 0.02 |
| 27 | 10 | 3 | 0 | 8 | 210 ± 11.7 | 0.45 ± 0.07 | 94.4 | −12.5 | 0.60 ± 0.04 |
| 28 | 10 | 4.75 | 10 | 8 | 118 ± 2.4 | 0.27 ± 0.04 | 93 | −22 | 0.34 ± 0.04 |
| 29 | 10 | 4.75 | 10 | 8 | 122 ± 8.3 | 0.22 ± 0.01 | 92 | −23 | 0.30 ± 0.02 |
| Response | Minimum | Maximum | Mean | SD | Model |
|---|---|---|---|---|---|
| Liposome size (nm) | 85 | 230 | 139.41 | 40.22 | Quadratic |
| PDI | 0.12 | 0.45 | 0.2693 | 0.0836 | Quadratic |
| Encapsulation efficiency (%) | 69 | 97.5 | 90.03 | 7.08 | Quadratic |
| Zeta potential (mV) | −28 | −12.5 | −21.70 | 4.35 | Quadratic |
| PDI after 1 month | 0.12 | 0.6 | 0.3434 | 0.1270 | Modified 2FI |
| Responses | R2 | Adjusted R2 | Predicted R2 | % CV |
|---|---|---|---|---|
| Liposome size (nm) | 0.868 | 0.839 | 0.785 | 11.56 |
| PDI | 0.826 | 0.788 | 0.690 | 14.29 |
| Encapsulation efficiency (%) | 0.874 | 0.814 | 0.676 | 3.32 |
| Zeta potential (mV) | 0.875 | 0.841 | 0.767 | 7.97 |
| PDI after 1 month | 0.811 | 0.761 | 0.679 | 18.10 |
| Goal | Lower Limit | Upper Limit | Importance | |
|---|---|---|---|---|
| A: Lipid concentration (mg/mL) | is in range | 5 | 10 | 3 |
| B: pH | is target = 6 | 3 | 6.5 | 3 |
| C: Cholesterol (%) | is in range | 0 | 20 | 3 |
| D: D/L molar ratio | maximise | 5 | 11 | 3 |
| Liposome size(nm) | minimise | 85 | 120 | 3 |
| PDI | minimise | 0.1 | 0.3 | 3 |
| Encapsulation efficiency (%) | maximise | 80 | 97.5 | 3 |
| Zeta potential (mV) | minimise | −28 | −12.5 | 3 |
| PDI after 1 month | minimise | 0.1 | 0.3 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haddad, F.; Mohammed, N.; Gopalan, R.C.; Ayoub, Y.A.; Nasim, M.T.; Assi, K.H. Development and Optimisation of Inhalable EGCG Nano-Liposomes as a Potential Treatment for Pulmonary Arterial Hypertension by Implementation of the Design of Experiments Approach. Pharmaceutics 2023, 15, 539. https://doi.org/10.3390/pharmaceutics15020539
Haddad F, Mohammed N, Gopalan RC, Ayoub YA, Nasim MT, Assi KH. Development and Optimisation of Inhalable EGCG Nano-Liposomes as a Potential Treatment for Pulmonary Arterial Hypertension by Implementation of the Design of Experiments Approach. Pharmaceutics. 2023; 15(2):539. https://doi.org/10.3390/pharmaceutics15020539
Chicago/Turabian StyleHaddad, Fatma, Nura Mohammed, R. C. Gopalan, Yousef Al Ayoub, Md Talat Nasim, and K. H. Assi. 2023. "Development and Optimisation of Inhalable EGCG Nano-Liposomes as a Potential Treatment for Pulmonary Arterial Hypertension by Implementation of the Design of Experiments Approach" Pharmaceutics 15, no. 2: 539. https://doi.org/10.3390/pharmaceutics15020539