
Sustained Release of Tacrolimus Embedded in a Mixed Thermosensitive Hydrogel for Improving Functional Recovery of Injured Peripheral Nerves in Extremities
 , , , , and
, , , , and 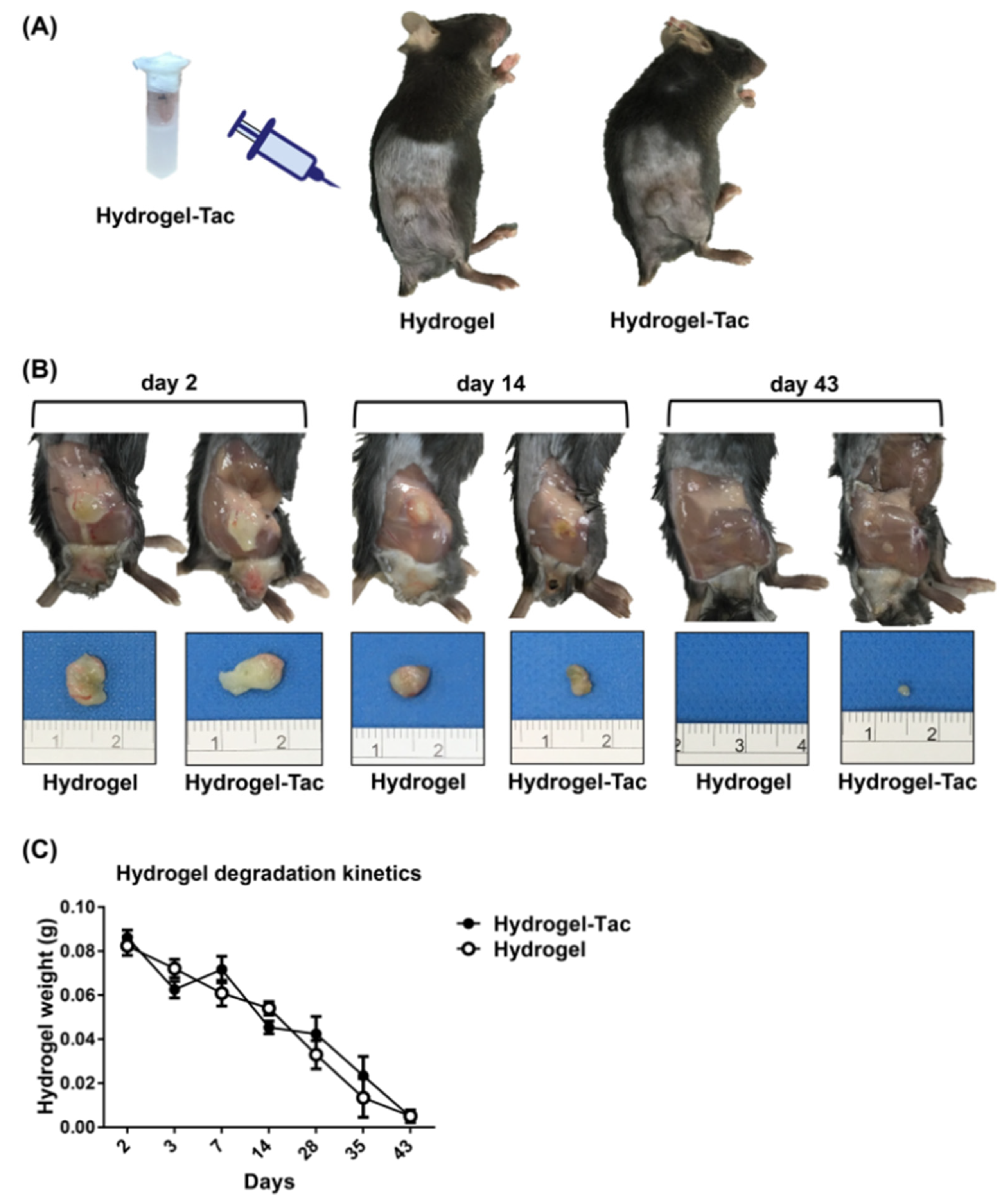{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Mice
2.2. Tacrolimus-Laden Mixed Thermosensitive Hydrogel System
2.3. Flow Cytometry
2.4. Cytometric Bead Array Assay
2.5. Quantification of Tacrolimus Concentration in Tissues
2.6. Mouse Sciatic Nerve Transection Model
2.7. Topical Administration of Hydrogel Control and Hydrogel-Tacrolimus
2.8. Functional Recovery by Five-Toe Spread Analysis
2.9. Functional Recovery by Video Gait Angle Analysis
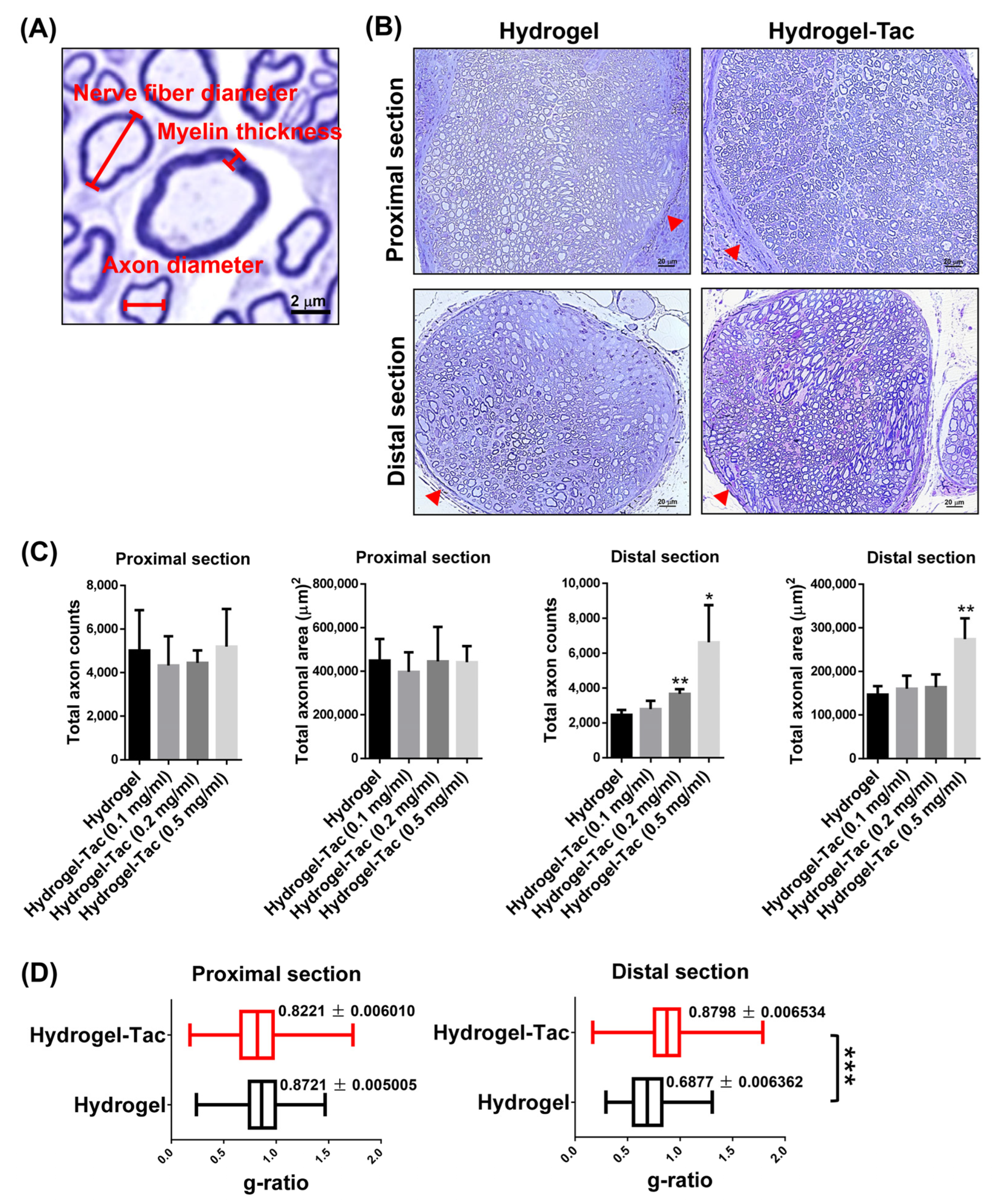
2.10. Nerve Regeneration by the Analysis of Toluidine Blue Staining
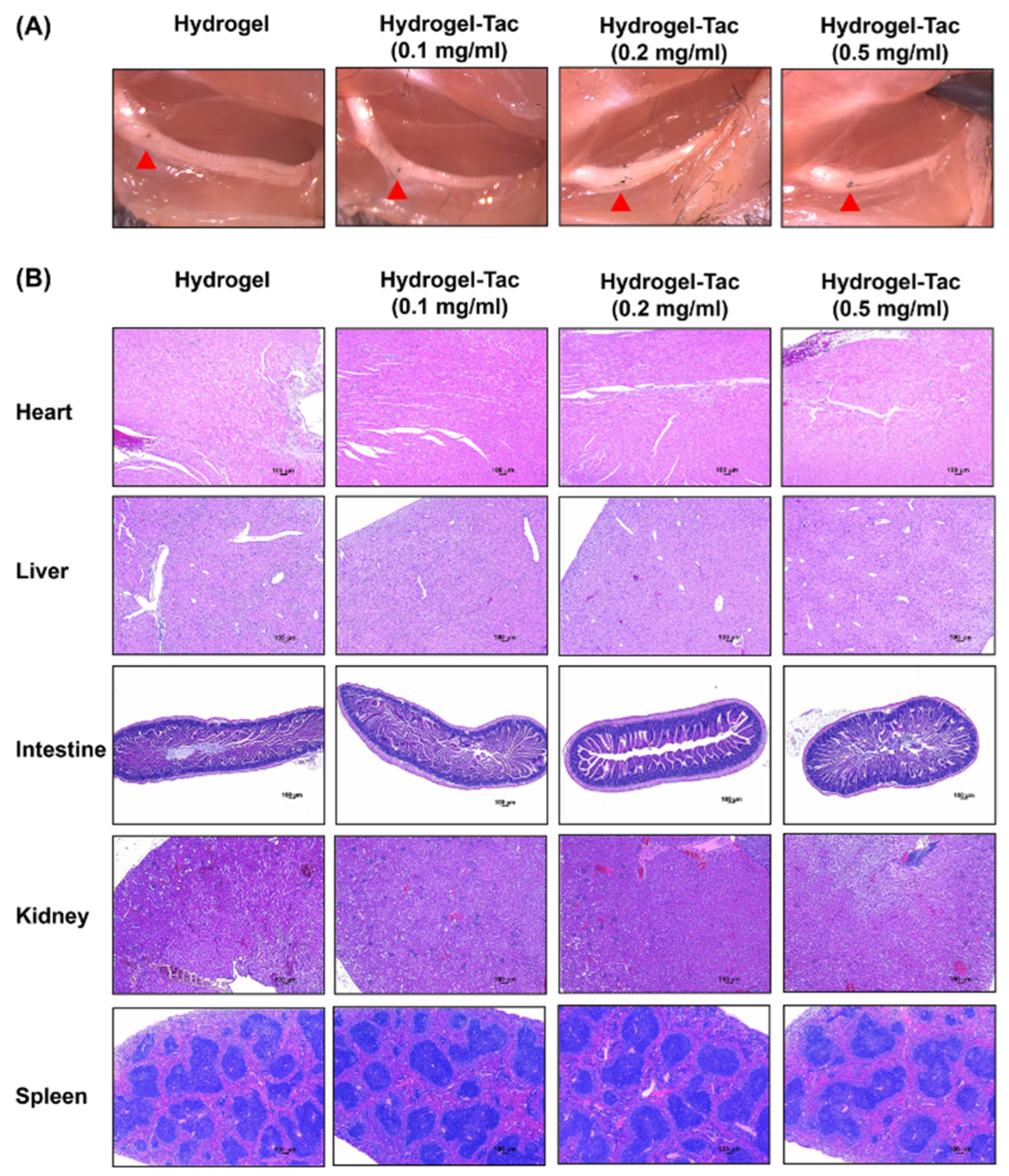
2.11. Histological Examination by Hematoxylin and Eosin Staining
2.12. Statistical Analysis
3. Results
3.1. Hydrogel Degradation Kinetics
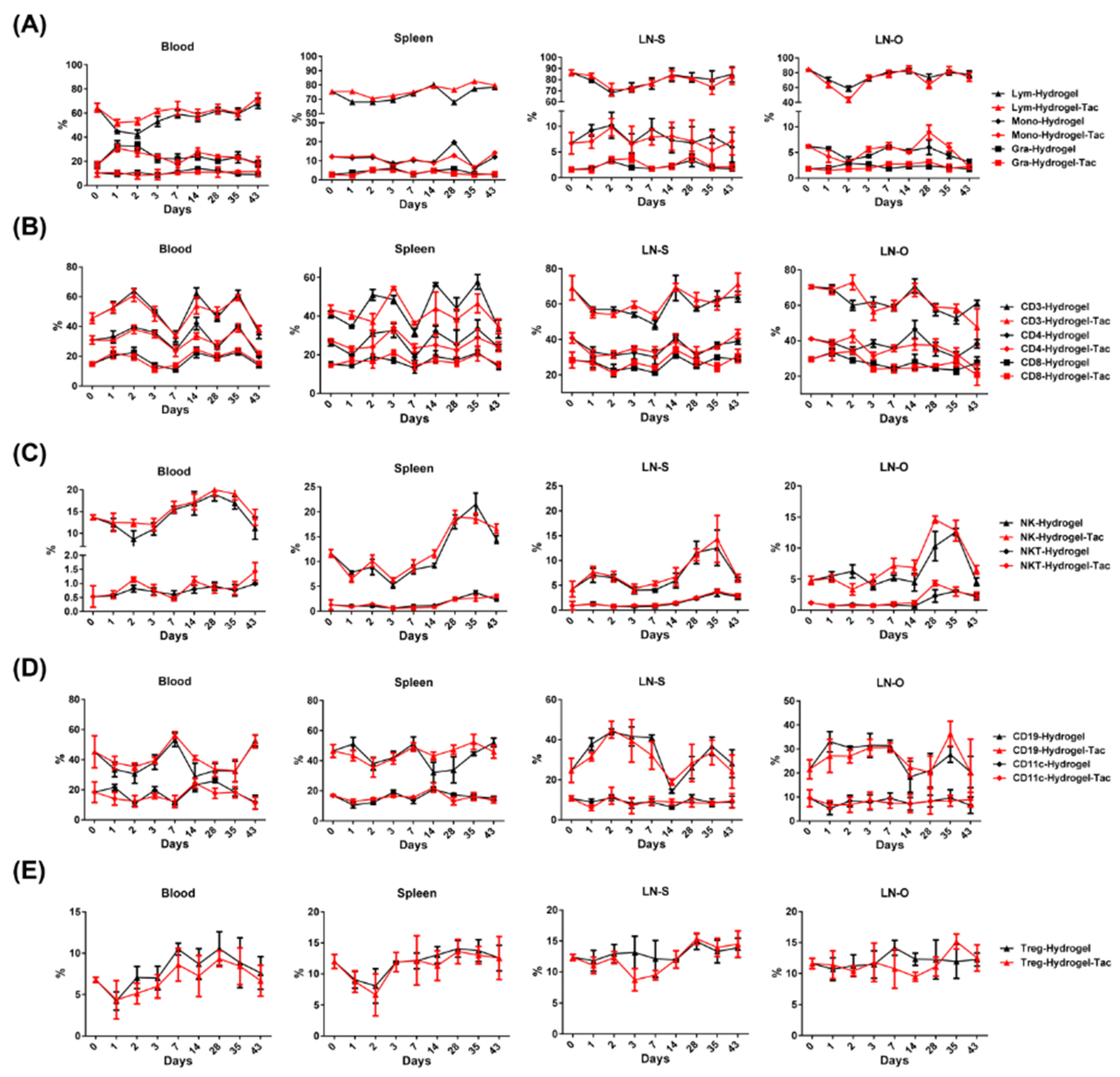
3.2. In Vivo Effects of Hydrogel-Tac Local Administration on the Systemic Immunomodulation
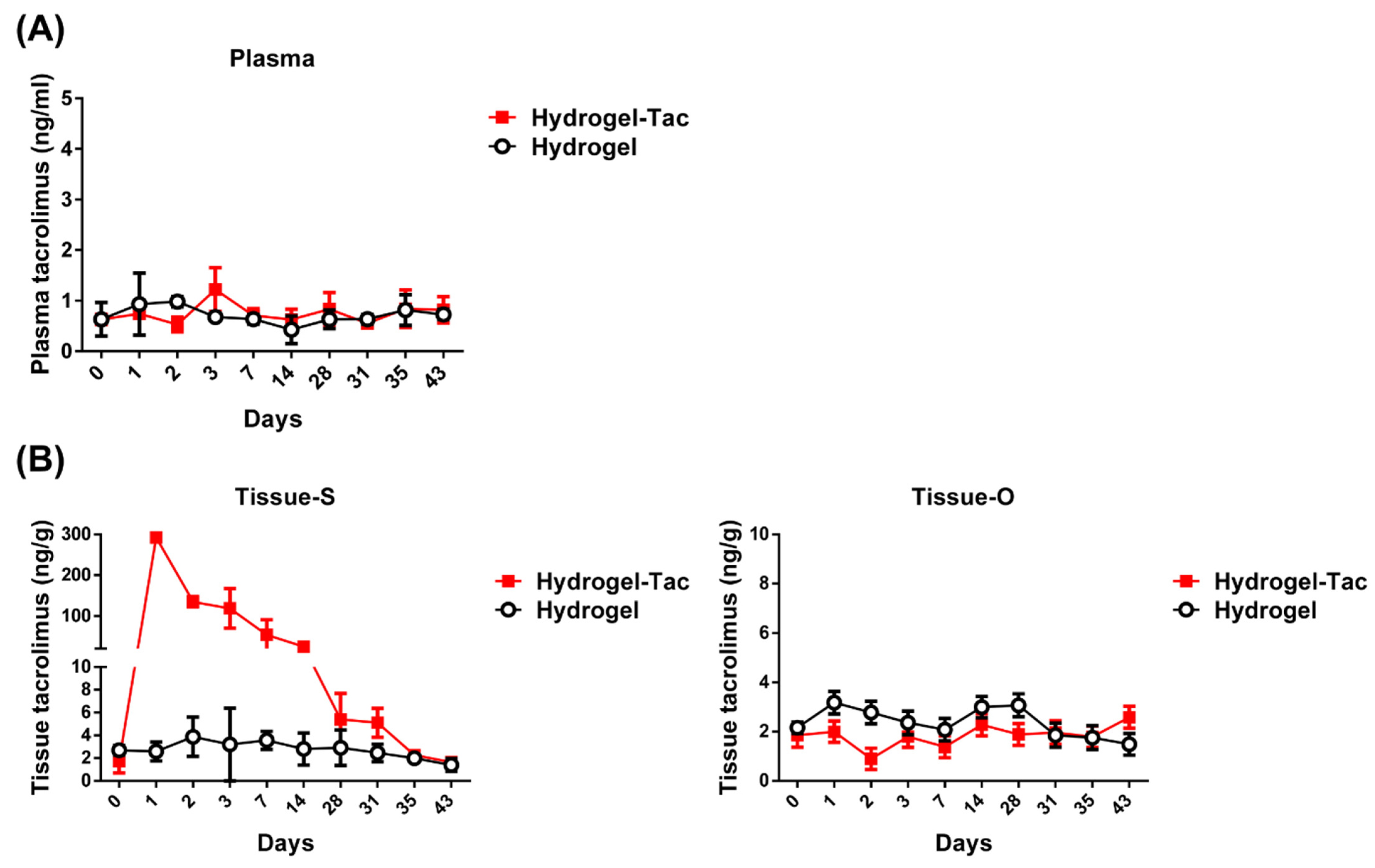
3.3. In Vivo Sustained-Release Pharmacokinetics in Hydrogel-Tac Topical Application
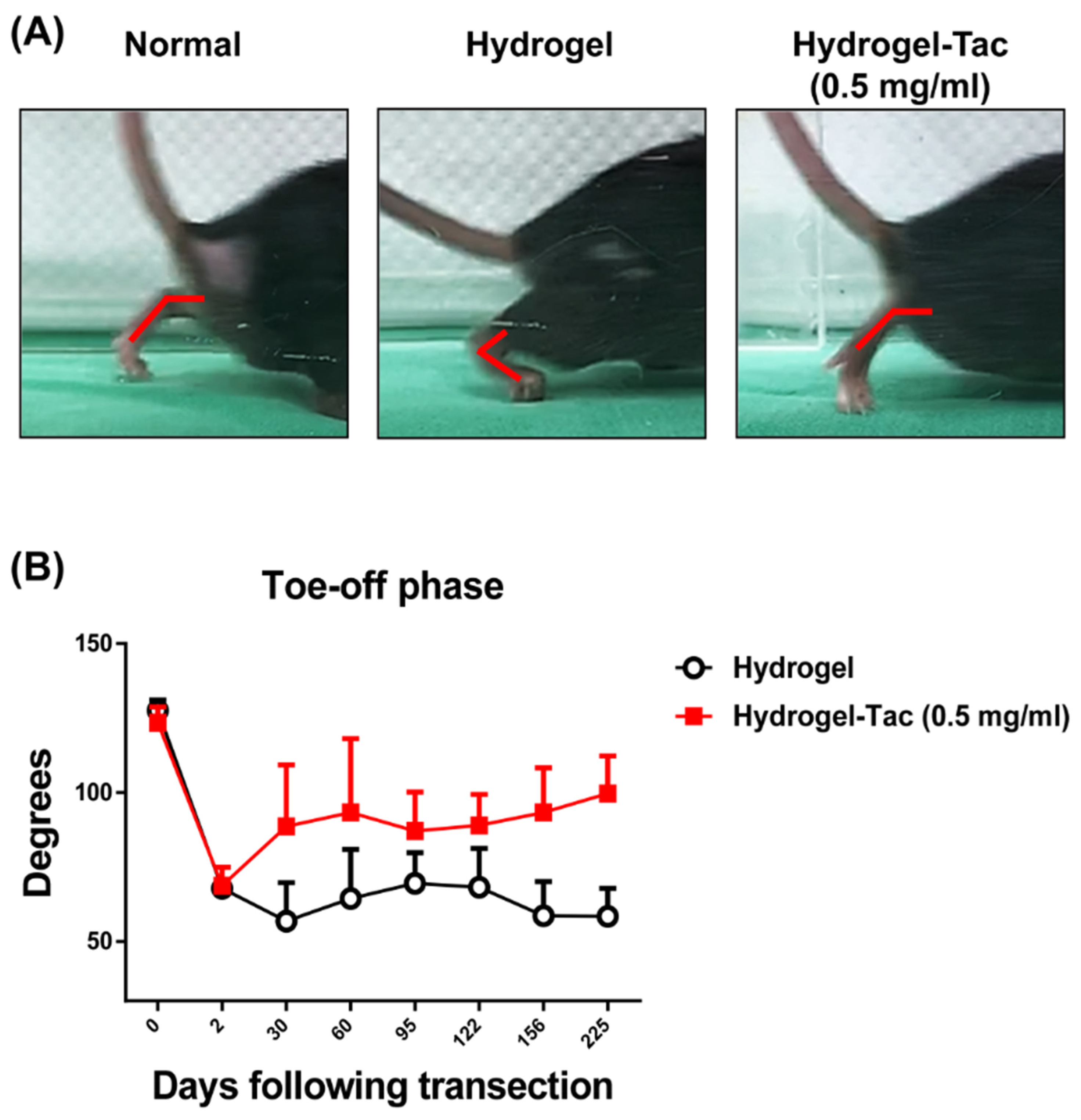
3.4. Efficacy of Hydrogel-Tac Topical Administration for Injured Sciatic Nerve Recovery
3.5. Efficacy of Hydrogel-Tac Topical Administration for Axonal Regeneration
3.6. Long-Term Systemic Effects of Local Hydrogel-Tac Treatment
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Landin, L.; Bonastre, J.; Casado-Sanchez, C.; Diez, J.; Ninkovic, M.; Lanzetta, M.; del Bene, M.; Schneeberger, S.; Hautz, T.; Lovic, A.; et al. Outcomes with respect to disabilities of the upper limb after hand allograft transplantation: A systematic review. Transpl. Int. 2012, 25, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Carlsen, B.T.; Prigge, P.; Peterson, J. Upper extremity limb loss: Functional restoration from prosthesis and targeted reinnervation to transplantation. J. Hand Ther. 2014, 27, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Glaus, S.W.; Johnson, P.J.; Mackinnon, S.E. Clinical strategies to enhance nerve regeneration in composite tissue allotransplantation. Hand Clin. 2011, 27, 495–509. [Google Scholar] [CrossRef] [PubMed]
- Schlaepfer, W.W. Calcium-induced degeneration of axoplasm in isolated segments of rat peripheral nerve. Brain Res. 1974, 69, 203–215. [Google Scholar] [CrossRef]
- Francois, C.G.; Breidenbach, W.C.; Maldonado, C.; Kakoulidis, T.P.; Hodges, A.; Dubernard, J.M.; Owen, E.; Pei, G.; Ren, X.; Barker, J.H. Hand transplantation: Comparisons and observations of the first four clinical cases. Microsurgery 2000, 20, 360–371. [Google Scholar] [CrossRef]
- Fu, S.Y.; Gordon, T. The cellular and molecular basis of peripheral nerve regeneration. Mol. Neurobiol. 1997, 14, 67–116. [Google Scholar] [CrossRef]
- Chaudhry, V.; Cornblath, D.R. Wallerian degeneration in human nerves: Serial electrophysiological studies. Muscle Nerve 1992, 15, 687–693. [Google Scholar] [CrossRef]
- Reichert, F.; Levitzky, R.; Rotshenker, S. Interleukin 6 in intact and injured mouse peripheral nerves. Eur. J. Neurosci. 1996, 8, 530–535. [Google Scholar] [CrossRef]
- Loh, C.Y.; Wang, A.Y.; Kao, H.K.; Cardona, E.; Chuang, S.H.; Wei, F.C. Episomal Induced Pluripotent Stem Cells Promote Functional Recovery of Transected Murine Peripheral Nerve. PLoS ONE 2016, 11, e0164696. [Google Scholar] [CrossRef]
- Wang, A.Y.L.; Loh, C.Y.Y. Episomal Induced Pluripotent Stem Cells: Functional and Potential Therapeutic Applications. Cell Transplant. 2019, 28 (Suppl. S1), 112S–131S. [Google Scholar] [CrossRef]
- Wang, A.Y.L.; Loh, C.Y.Y.; Shen, H.H.; Hsieh, S.Y.; Wang, I.K.; Chuang, S.H.; Wei, F.C. Topical Application of Human Wharton’s Jelly Mesenchymal Stem Cells Accelerates Mouse Sciatic Nerve Recovery and is Associated with Upregulated Neurotrophic Factor Expression. Cell Transplant. 2019, 28, 1560–1572. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.Y.L.; Loh, C.Y.Y.; Shen, H.H.; Hsieh, S.Y.; Wang, I.K.; Lee, C.M.; Lin, C.H. Human Wharton’s Jelly Mesenchymal Stem Cell-Mediated Sciatic Nerve Recovery Is Associated with the Upregulation of Regulatory T Cells. Int. J. Mol. Sci. 2020, 21, 6310. [Google Scholar] [CrossRef]
- Schreiber, S.L. Chemistry and biology of the immunophilins and their immunosuppressive ligands. Science 1991, 251, 283–287. [Google Scholar] [CrossRef]
- Liu, J.; Farmer, J.D., Jr.; Lane, W.S.; Friedman, J.; Weissman, I.; Schreiber, S.L. Calcineurin is a common target of cyclophilin-cyclosporin A and FKBP-FK506 complexes. Cell 1991, 66, 807–815. [Google Scholar] [CrossRef]
- Grand, A.G.; Myckatyn, T.M.; Mackinnon, S.E.; Hunter, D.A. Axonal regeneration after cold preservation of nerve allografts and immunosuppression with tacrolimus in mice. J. Neurosurg. 2002, 96, 924–932. [Google Scholar] [CrossRef]
- Udina, E.; Ceballos, D.; Verdu, E.; Gold, B.G.; Navarro, X. Bimodal dose-dependence of FK506 on the rate of axonal regeneration in mouse peripheral nerve. Muscle Nerve 2002, 26, 348–355. [Google Scholar] [CrossRef]
- Yang, R.K.; Lowe, J.B., 3rd; Sobol, J.B.; Sen, S.K.; Hunter, D.A.; Mackinnon, S.E. Dose-dependent effects of FK506 on neuroregeneration in a rat model. Plast. Reconstr. Surg. 2003, 112, 1832–1840. [Google Scholar] [CrossRef]
- Konofaos, P.; Terzis, J.K. FK506 and nerve regeneration: Past, present, and future. J. Reconstr. Microsurg. 2013, 29, 141–148. [Google Scholar] [CrossRef]
- Gold, B.G.; Densmore, V.; Shou, W.; Matzuk, M.M.; Gordon, H.S. Immunophilin FK506-binding protein 52 (not FK506-binding protein 12) mediates the neurotrophic action of FK506. J. Pharmacol. Exp. Ther. 1999, 289, 1202–1210. [Google Scholar]
- Gold, B.G.; Zeleny-Pooley, M.; Wang, M.S.; Chaturvedi, P.; Armistead, D.M. A nonimmunosuppressant FKBP-12 ligand increases nerve regeneration. Exp. Neurol. 1997, 147, 269–278. [Google Scholar] [CrossRef]
- Navarro, X.; Udina, E.; Ceballos, D.; Gold, B.G. Effects of FK506 on nerve regeneration and reinnervation after graft or tube repair of long nerve gaps. Muscle Nerve 2001, 24, 905–915. [Google Scholar] [CrossRef]
- Zawadzka, M.; Dabrowski, M.; Gozdz, A.; Szadujkis, B.; Sliwa, M.; Lipko, M.; Kaminska, B. Early steps of microglial activation are directly affected by neuroprotectant FK506 in both in vitro inflammation and in rat model of stroke. J. Mol. Med. 2012, 90, 1459–1471. [Google Scholar] [CrossRef]
- Udina, E.; Ceballos, D.; Gold, B.G.; Navarro, X. FK506 enhances reinnervation by regeneration and by collateral sprouting of peripheral nerve fibers. Exp. Neurol. 2003, 183, 220–231. [Google Scholar] [CrossRef]
- Udina, E.; Voda, J.; Gold, B.G.; Navarro, X. Comparative dose-dependence study of FK506 on transected mouse sciatic nerve repaired by allograft or xenograft. J. Peripher. Nerv. Syst. 2003, 8, 145–154. [Google Scholar] [CrossRef]
- Gold, B.G.; Storm-Dickerson, T.; Austin, D.R. The immunosuppressant FK506 increases functional recovery and nerve regeneration following peripheral nerve injury. Restor. Neurol. Neurosci. 1994, 6, 287–296. [Google Scholar] [CrossRef]
- Udina, E.; Gold, B.G.; Navarro, X. Comparison of continuous and discontinuous FK506 administration on autograft or allograft repair of sciatic nerve resection. Muscle Nerve 2004, 29, 812–822. [Google Scholar] [CrossRef]
- Gold, B.G. FK506 and the role of immunophilins in nerve regeneration. Mol. Neurobiol. 1997, 15, 285–306. [Google Scholar] [CrossRef]
- Udina, E.; Rodriguez, F.J.; Verdu, E.; Espejo, M.; Gold, B.G.; Navarro, X. FK506 enhances regeneration of axons across long peripheral nerve gaps repaired with collagen guides seeded with allogeneic Schwann cells. Glia 2004, 47, 120–129. [Google Scholar] [CrossRef]
- Sulaiman, O.A.; Voda, J.; Gold, B.G.; Gordon, T. FK506 increases peripheral nerve regeneration after chronic axotomy but not after chronic schwann cell denervation. Exp. Neurol. 2002, 175, 127–137. [Google Scholar] [CrossRef]
- Gold, B.G.; Armistead, D.M.; Wang, M.S. Non-FK506-binding protein-12 neuroimmunophilin ligands increase neurite elongation and accelerate nerve regeneration. J. Neurosci. Res. 2005, 80, 56–65. [Google Scholar] [CrossRef]
- Gold, B.G.; Zeleny-Pooley, M.; Chaturvedi, P.; Wang, M.S. Oral administration of a nonimmunosuppressant FKBP-12 ligand speeds nerve regeneration. Neuroreport 1998, 9, 553–558. [Google Scholar] [CrossRef]
- Varghese, J.; Reddy, M.S.; Venugopal, K.; Perumalla, R.; Narasimhan, G.; Arikichenin, O.; Shanmugam, V.; Shanmugam, N.; Srinivasan, V.; Jayanthi, V.; et al. Tacrolimus-related adverse effects in liver transplant recipients: Its association with trough concentrations. Indian J. Gastroenterol. 2014, 33, 219–225. [Google Scholar] [CrossRef]
- Yamazoe, K.; Yamazoe, K.; Yamaguchi, T.; Omoto, M.; Shimazaki, J. Efficacy and safety of systemic tacrolimus in high-risk penetrating keratoplasty after graft failure with systemic cyclosporine. Cornea 2014, 33, 1157–1163. [Google Scholar] [CrossRef]
- Bentata, Y. Tacrolimus: 20 years of use in adult kidney transplantation. What we should know about its nephrotoxicity. Artif. Organs 2020, 44, 140–152. [Google Scholar] [CrossRef]
- Yadav, D.K.; Gera, D.N.; Gumber, M.R.; Kute, V.B.; Patel, M.P.; Vanikar, A.V.; Trivedi, H.L. Tacrolimus-induced severe cholestasis complicating renal transplantation. Ren. Fail. 2013, 35, 735–737. [Google Scholar] [CrossRef]
- Rangel, E.B. Tacrolimus in pancreas transplant: A focus on toxicity, diabetogenic effect and drug-drug interactions. Expert Opin Drug Metab. Toxicol. 2014, 10, 1585–1605. [Google Scholar] [CrossRef]
- De Rycke, A.; Dierickx, D.; Kuypers, D.R. Tacrolimus-induced neutropenia in renal transplant recipients. Clin. J. Am. Soc. Nephrol. 2011, 6, 690–694. [Google Scholar] [CrossRef]
- Hoare, T.R.K.D.S. Hydrogels in drug delivery: Progress and challenges. Polymer 2008, 49, 1993–2007. [Google Scholar] [CrossRef]
- Drury, J.L.; Mooney, D.J. Hydrogels for tissue engineering: Scaffold design variables and applications. Biomaterials 2003, 24, 4337–4351. [Google Scholar] [CrossRef]
- Kopecek, J. Hydrogel biomaterials: A smart future? Biomaterials 2007, 28, 5185–5192. [Google Scholar] [CrossRef]
- Lin, H.C.; Anggelia, M.R.; Cheng, C.C.; Ku, K.L.; Cheng, H.Y.; Wen, C.J.; Wang, A.Y.L.; Lin, C.H.; Chu, I.M. A Mixed Thermosensitive Hydrogel System for Sustained Delivery of Tacrolimus for Immunosuppressive Therapy. Pharmaceutics 2019, 11, 413. [Google Scholar] [CrossRef] [Green Version]
- Kojarunchitt, T.; Hook, S.; Rizwan, S.; Rades, T.; Baldursdottir, S. Development and characterisation of modified poloxamer 407 thermoresponsive depot systems containing cubosomes. Int. J. Pharm. 2011, 408, 20–26. [Google Scholar] [CrossRef]
- Ge, J.; Zhu, S.; Yang, Y.; Liu, Z.; Hu, X.; Huang, L.; Quan, X.; Wang, M.; Huang, J.; Li, Y.; et al. Experimental immunological demyelination enhances regeneration in autograft-repaired long peripheral nerve gaps. Sci. Rep. 2016, 6, 39828. [Google Scholar] [CrossRef]
- Triolo, D.; Dina, G.; Taveggia, C.; Vaccari, I.; Porrello, E.; Rivellini, C.; Domi, T.; La Marca, R.; Cerri, F.; Bolino, A.; et al. Vimentin regulates peripheral nerve myelination. Development 2012, 139, 1359–1367. [Google Scholar] [CrossRef]
- Chomiak, T.; Hu, B. What is the optimal value of the g-ratio for myelinated fibers in the rat CNS? A theoretical approach. PLoS ONE 2009, 4, e7754. [Google Scholar] [CrossRef]
- Benninger, Y.; Colognato, H.; Thurnherr, T.; Franklin, R.J.; Leone, D.P.; Atanasoski, S.; Nave, K.A.; Ffrench-Constant, C.; Suter, U.; Relvas, J.B. Beta1-integrin signaling mediates premyelinating oligodendrocyte survival but is not required for CNS myelination and remyelination. J. Neurosci. 2006, 26, 7665–7673. [Google Scholar] [CrossRef]
- Duval, T.; Le Vy, S.; Stikov, N.; Campbell, J.; Mezer, A.; Witzel, T.; Keil, B.; Smith, V.; Wald, L.L.; Klawiter, E.; et al. g-Ratio weighted imaging of the human spinal cord in vivo. Neuroimage 2017, 145, 11–23. [Google Scholar] [CrossRef]
- Campbell, J.S.W.; Leppert, I.R.; Narayanan, S.; Boudreau, M.; Duval, T.; Cohen-Adad, J.; Pike, G.B.; Stikov, N. Promise and pitfalls of g-ratio estimation with MRI. Neuroimage 2018, 182, 80–96. [Google Scholar] [CrossRef]
- Wang, M.S.; Zeleny-Pooley, M.; Gold, B.G. Comparative dose-dependence study of FK506 and cyclosporin A on the rate of axonal regeneration in the rat sciatic nerve. J. Pharmacol. Exp. Ther. 1997, 282, 1084–1093. [Google Scholar]
- Felldin, M.; Backman, L.; Brattstrom, C.; Bentdal, O.; Nordal, K.; Claesson, K.; Persson, N.H. Rescue therapy with tacrolimus (FK 506) in renal transplant recipients--a Scandinavian multicenter analysis. Transpl. Int. 1997, 10, 13–18. [Google Scholar] [CrossRef]
- Gold, B.G.; Katoh, K.; Storm-Dickerson, T. The immunosuppressant FK506 increases the rate of axonal regeneration in rat sciatic nerve. J. Neurosci. 1995, 15, 7509–7516. [Google Scholar] [CrossRef]
- De Paz, D.; Avina, A.E.; Cardona, E.; Lee, C.M.; Lin, C.H.; Lin, C.H.; Wei, F.C.; Wang, A.Y.L. The Mandible Ameliorates Facial Allograft Rejection and Is Associated with the Development of Regulatory T Cells and Mixed Chimerism. Int. J. Mol. Sci. 2021, 22, 11104. [Google Scholar] [CrossRef]
- Cardona, E.; Wang, A.Y.L.; Loh, C.Y.Y.; Chuang, S.H.; Lee, C.M.; ALDeek, N.; Lin, C.H.; Wei, F.C. A New Face Subunit Transplant Model in Mice, Containing Skin, Mandible, and Oral Mucosa for Future Face Vascularized Composite Allotransplantation Studies. Plast. Reconstr. Surg. 2019, 144, 115–123. [Google Scholar] [CrossRef]
- Wang AYL, L.C. Reviewing immunosuppressive regimens in animal models for vascularized composite allotransplantation. Plast. Aesthet. Res. 2018, 5, 1. [Google Scholar] [CrossRef] [Green Version]
- Chu, I.M.; Lin, H.-C.; Cheng, C.C.; Ku, K.L. Drug Carrier and Drug Delivery System Using the Same. Patent I649096, 1 February 2019. [Google Scholar]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, A.Y.L.; Chen, K.-H.; Lin, H.-C.; Loh, C.Y.Y.; Chang, Y.-C.; Aviña, A.E.; Lee, C.-M.; Chu, I.-M.; Wei, F.-C. Sustained Release of Tacrolimus Embedded in a Mixed Thermosensitive Hydrogel for Improving Functional Recovery of Injured Peripheral Nerves in Extremities. Pharmaceutics 2023, 15, 508. https://doi.org/10.3390/pharmaceutics15020508
Wang AYL, Chen K-H, Lin H-C, Loh CYY, Chang Y-C, Aviña AE, Lee C-M, Chu I-M, Wei F-C. Sustained Release of Tacrolimus Embedded in a Mixed Thermosensitive Hydrogel for Improving Functional Recovery of Injured Peripheral Nerves in Extremities. Pharmaceutics. 2023; 15(2):508. https://doi.org/10.3390/pharmaceutics15020508
Chicago/Turabian StyleWang, Aline Yen Ling, Kuan-Hung Chen, Hsiu-Chao Lin, Charles Yuen Yung Loh, Yun-Ching Chang, Ana Elena Aviña, Chin-Ming Lee, I-Ming Chu, and Fu-Chan Wei. 2023. "Sustained Release of Tacrolimus Embedded in a Mixed Thermosensitive Hydrogel for Improving Functional Recovery of Injured Peripheral Nerves in Extremities" Pharmaceutics 15, no. 2: 508. https://doi.org/10.3390/pharmaceutics15020508