

Scaling Pharmacodynamics from Rats to Humans to Support Erythropoietin and Romiplostim Combination Therapy to Treat Erythropoietin-Resistant Anemia

Abstract
:1. Introduction
2. Materials and Methods
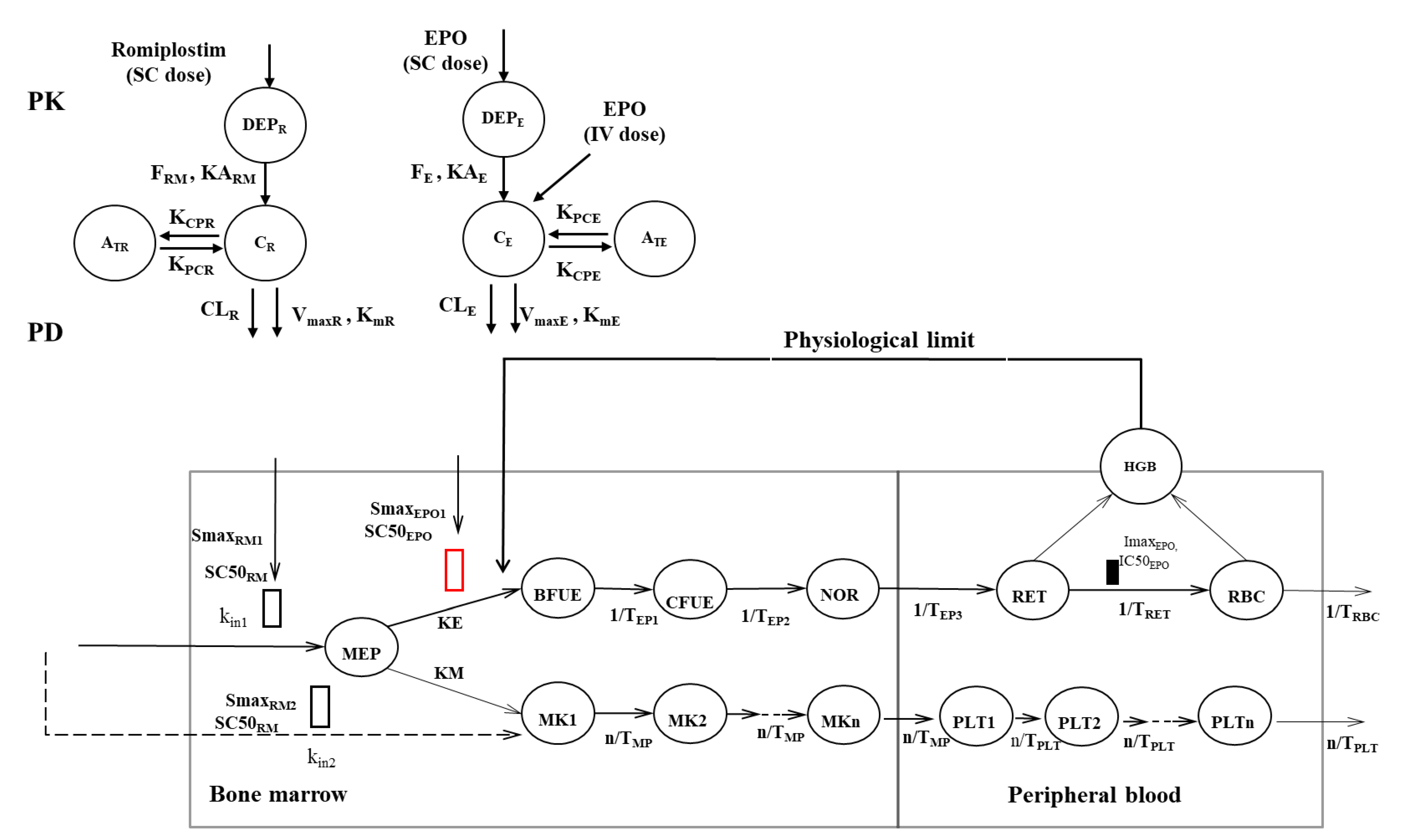
2.1. Michaelis–Menten Approximation of Target-Mediated Drug Disposition PK/PD Model Development
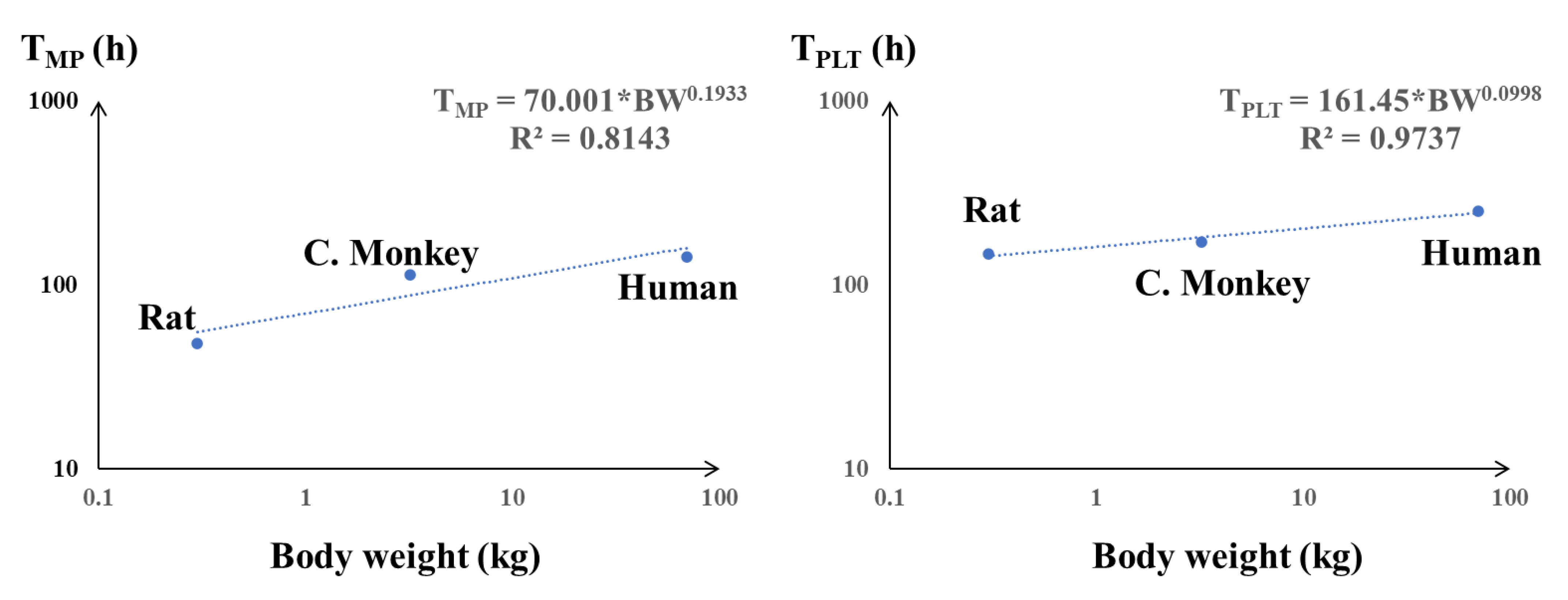
2.2. Allometric Scaling and Validation
2.3. Model-Based Simulation of rHuEPO IV and Romiplostim SC Administration PD in Humans
2.4. Software
3. Results
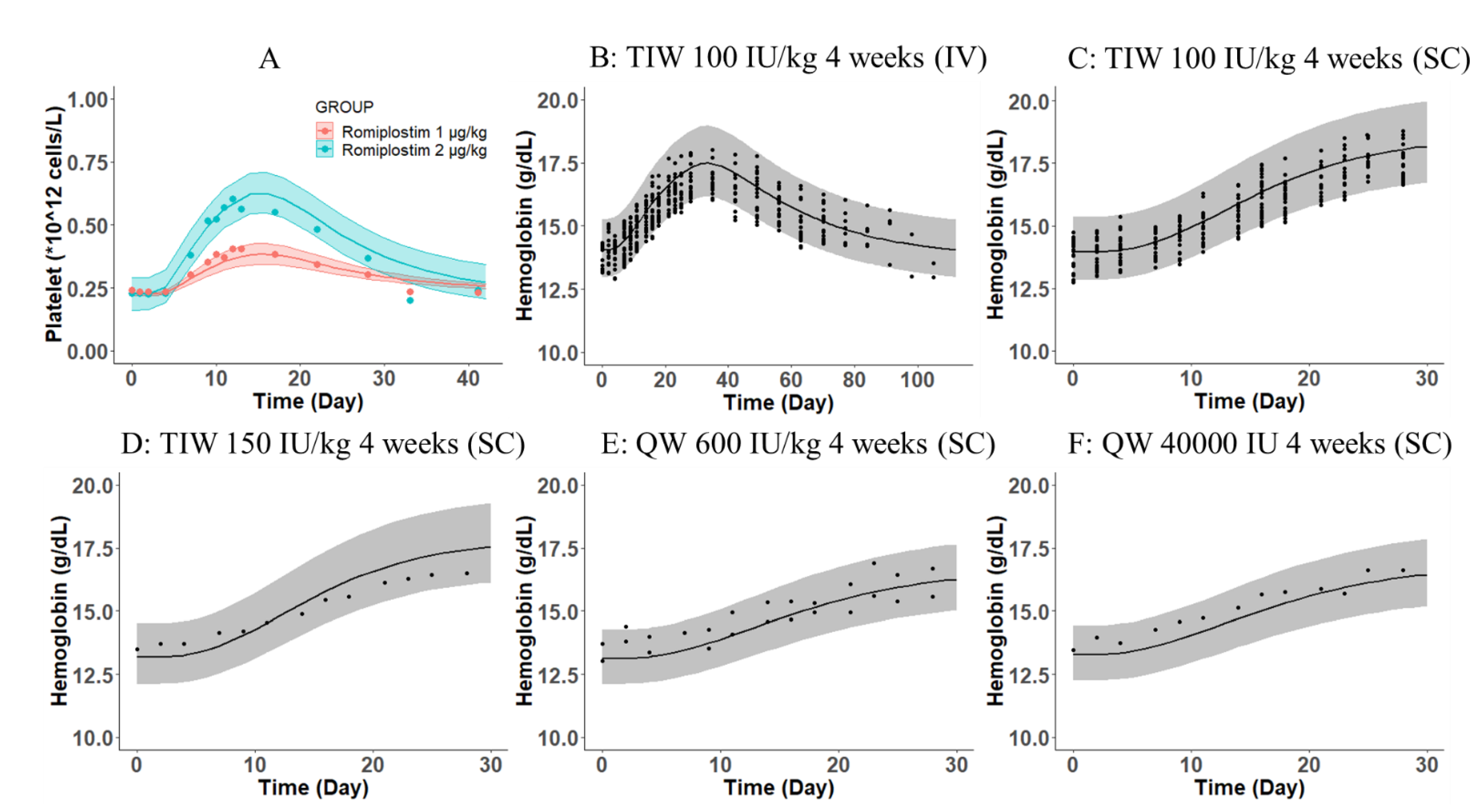
3.1. Michaelis–Menten Approximation of a Target-Mediated Drug Disposition PK/PD Model Reasonably Characterizes the PK and PD Profiles of Romiplostim and rHuEPO as Monotherapy and Combination Therapy
3.2. Extrapolation and VALIDATION of the PK/PD Model to Humans
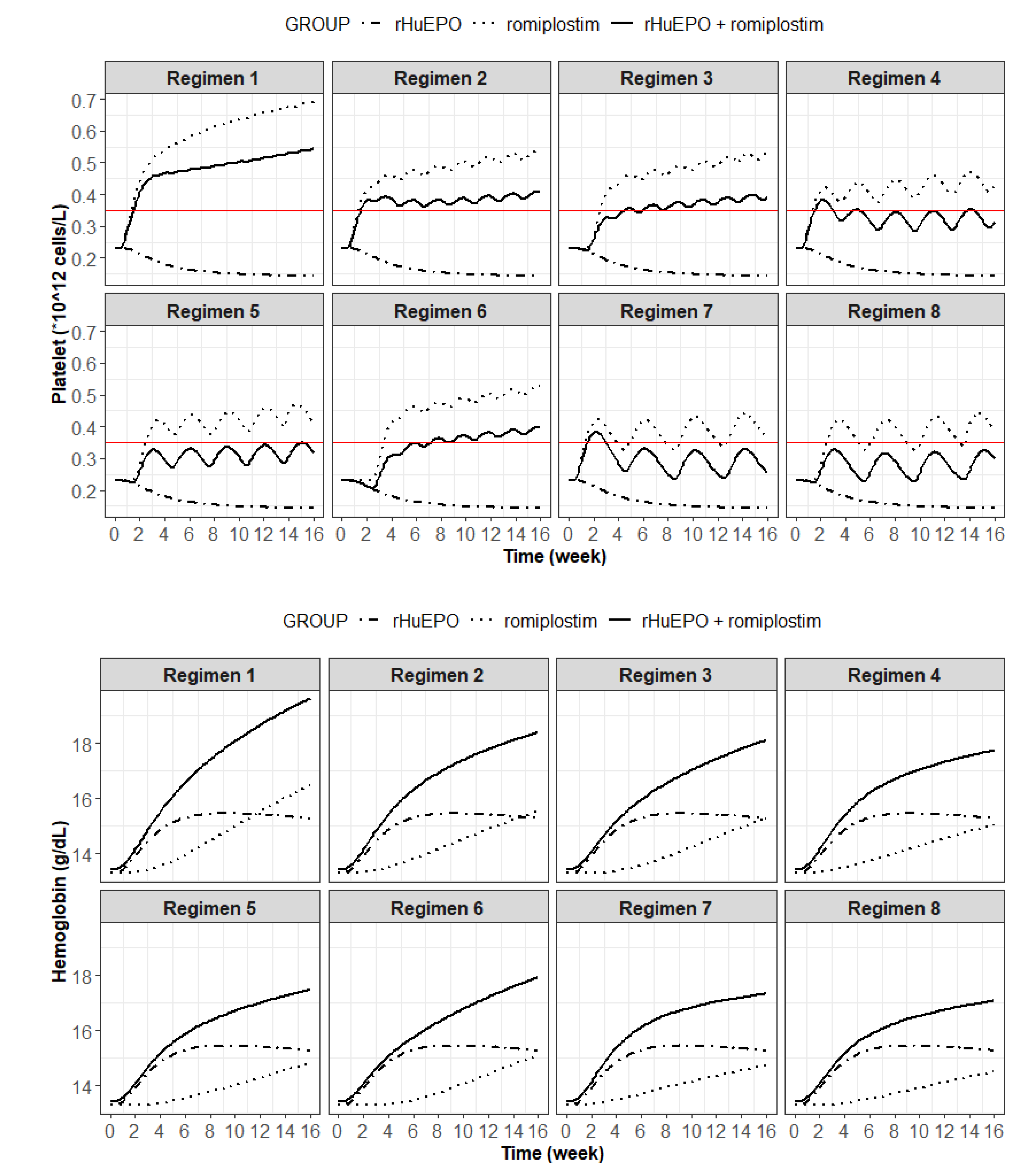
3.3. Prediction of an Optimal Combination Dosing Regimen in Humans
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Babitt, J.L.; Lin, H.Y. Mechanisms of anemia in CKD. J. Am. Soc. Nephrol. 2012, 23, 1631–1634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliott, S. Erythropoiesis-stimulating agents. Cancer Treat. Res. 2011, 157, 55–74. [Google Scholar] [CrossRef] [PubMed]
- Gutti, U.; Pasupuleti, S.R.; Sahu, I.; Kotipalli, A.; Undi, R.B.; Kandi, R.; Venakata Saladi, R.G.; Gutti, R.K. Erythropoietin and thrombopoietin mimetics: Natural alternatives to erythrocyte and platelet disorders. Crit. Rev. Oncol. Hematol. 2016, 108, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Fukuma, S.; Yamaguchi, T.; Hashimoto, S.; Nakai, S.; Iseki, K.; Tsubakihara, Y.; Fukuhara, S. Erythropoiesis-stimulating agent responsiveness and mortality in hemodialysis patients: Results from a cohort study from the dialysis registry in Japan. Am. J. Kidney Dis. 2012, 59, 108–116. [Google Scholar] [CrossRef]
- Zhang, Y.; Thamer, M.; Kaufman, J.S.; Cotter, D.J.; Hernán, M.A. High doses of epoetin do not lower mortality and cardiovascular risk among elderly hemodialysis patients with diabetes. Kidney Int. 2011, 80, 663–669. [Google Scholar] [CrossRef] [Green Version]
- Santos, P.R.; Melo, A.D.; Lima, M.M.; Negreiros, I.M.; Miranda, J.S.; Pontes, L.S.; Rabelo, G.M.; Viana, A.C.; Alexandrino, M.T.; Barros, F.A.; et al. Mortality risk in hemodialysis patients according to anemia control and erythropoietin dosing. Hemodial. Int. 2011, 15, 493–500. [Google Scholar] [CrossRef]
- Costa, E.; Rocha, S.; Rocha-Pereira, P.; Nascimento, H.; Castro, E.; Miranda, V.; Faria Mdo, S.; Loureiro, A.; Quintanilha, A.; Belo, L.; et al. Neutrophil activation and resistance to recombinant human erythropoietin therapy in hemodialysis patients. Am. J. Nephrol. 2008, 28, 935–940. [Google Scholar] [CrossRef] [Green Version]
- Icardi, A.; Paoletti, E.; De Nicola, L.; Mazzaferro, S.; Russo, R.; Cozzolino, M. Renal anaemia and EPO hyporesponsiveness associated with vitamin D deficiency: The potential role of inflammation. Nephrol Dial. Transplant. 2013, 28, 1672–1679. [Google Scholar] [CrossRef] [Green Version]
- Kilpatrick, R.D.; Critchlow, C.W.; Fishbane, S.; Besarab, A.; Stehman-Breen, C.; Krishnan, M.; Bradbury, B.D. Greater epoetin alfa responsiveness is associated with improved survival in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2008, 3, 1077–1083. [Google Scholar] [CrossRef] [Green Version]
- Kainz, A.; Mayer, B.; Kramar, R.; Oberbauer, R. Association of ESA hypo-responsiveness and haemoglobin variability with mortality in haemodialysis patients. Nephrol. Dial. Transplant. 2010, 25, 3701–3706. [Google Scholar] [CrossRef]
- Suttorp, M.M.; Hoekstra, T.; Rotmans, J.I.; Ott, I.; Mittelman, M.; Krediet, R.T.; Dekker, F.W. Erythropoiesis-stimulating agent resistance and mortality in hemodialysis and peritoneal dialysis patients. BMC Nephrol. 2013, 14, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, X.; Ait-Oudhia, S.; Krzyzanski, W. Erythropoietin-induced erythroid precursor pool depletion causes erythropoietin hyporesponsiveness. Pharm. Res. 2013, 30, 1026–1036. [Google Scholar] [CrossRef]
- Fan, X.; Krzyzanski, W.; Wong, R.S.M.; Yan, X. Fate determination role of erythropoietin and romiplostim in the lineage commitment of hematopoietic progenitors. J. Pharmacol. Exp. Ther. 2022, 382, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Zou, H.; Xu, P.; Wong, R.S.M.; Yan, X. A Novel Combination Therapy of Erythropoietin and Thrombopoietin to Treat Erythropoietin-Resistance anemia. Pharm. Res. 2022, 39, 1249–1265. [Google Scholar] [CrossRef]
- Mager, D.E.; Woo, S.; Jusko, W.J. Scaling pharmacodynamics from in vitro and preclinical animal studies to humans. Drug Metab. Pharmacokinet 2009, 24, 16–24. [Google Scholar] [CrossRef] [Green Version]
- Van Wijk, R.C.; Hu, W.; Dijkema, S.M.; van den Berg, D.J.; Liu, J.; Bahi, R.; Verbeek, F.J.; Simonsson, U.S.H.; Spaink, H.P.; van der Graaf, P.H.; et al. Anti-tuberculosis effect of isoniazid scales accurately from zebrafish to humans. Br. J. Pharmacol. 2020, 177, 5518–5533. [Google Scholar] [CrossRef] [PubMed]
- Jolling, K.; Perez Ruixo, J.J.; Hemeryck, A.; Vermeulen, A.; Greway, T. Mixed-effects modelling of the interspecies pharmacokinetic scaling of pegylated human erythropoietin. Eur. J. Pharm. Sci. 2005, 24, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Knibbe, C.A.; Zuideveld, K.P.; Aarts, L.P.; Kuks, P.F.; Danhof, M. Allometric relationships between the pharmacokinetics of propofol in rats, children and adults. Br. J. Clin. Pharmacol. 2005, 59, 705–711. [Google Scholar] [CrossRef] [Green Version]
- Boxenbaum, H. Interspecies scaling, allometry, physiological time, and the ground plan of pharmacokinetics. J. Pharmacokinet Biopharm. 1982, 10, 201–227. [Google Scholar] [CrossRef]
- Dedrick, R.L. Animal scale-up. J. Pharmacokinet Biopharm. 1973, 1, 435–461. [Google Scholar] [CrossRef]
- Yan, X.; Ruixo, J.J.P.; Krzyzanski, W. Dose Correction for a Michaelis-Menten Approximation of a Target-Mediated Drug Disposition Model with a Multiple Intravenous Dosing Regimens. AAPS J. 2020, 22, 30. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.M.; Krzyzanski, W.; Doshi, S.; Xiao, J.J.; Pérez-Ruixo, J.J.; Chow, A.T. Pharmacodynamics-mediated drug disposition (PDMDD) and precursor pool lifespan model for single dose of romiplostim in healthy subjects. AAPS J. 2010, 12, 729–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krzyzanski, W.; Ramakrishnan, R.; Jusko, W.J. Basic pharmacodynamic models for agents that alter production of natural cells. J. Pharmacokinet Biopharm. 1999, 27, 467–489. [Google Scholar] [CrossRef]
- Yan, X.; Lowe, P.J.; Fink, M.; Berghout, A.; Balser, S.; Krzyzanski, W. Population pharmacokinetic and pharmacodynamic model-based comparability assessment of a recombinant human Epoetin Alfa and the Biosimilar HX575. J. Clin. Pharmacol. 2012, 52, 1624–1644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, S.; Jusko, W.J. Interspecies comparisons of pharmacokinetics and pharmacodynamics of recombinant human erythropoietin. Drug Metab. Dispos. 2007, 35, 1672–1678. [Google Scholar] [CrossRef] [PubMed]
- Krzyzanski, W.; Sutjandra, L.; Perez-Ruixo, J.J.; Sloey, B.; Chow, A.T.; Wang, Y.M. Pharmacokinetic and pharmacodynamic modeling of romiplostim in animals. Pharm. Res. 2013, 30, 655–669. [Google Scholar] [CrossRef]
- Corrons, J.L.V.; Casafont, L.B.; Frasnedo, E.F. Concise review: How do red blood cells born, live, and die? Ann. Hematol. 2021, 100, 2425–2433. [Google Scholar] [CrossRef]
- Gremmel, T.; Frelinger, A.L., 3rd; Michelson, A.D. Platelet Physiology. Semin. Thromb. Hemost. 2016, 42, 191–204. [Google Scholar] [CrossRef] [Green Version]
- Krzyzanski, W.; Jusko, W.J.; Wacholtz, M.C.; Minton, N.; Cheung, W.K. Pharmacokinetic and pharmacodynamic modeling of recombinant human erythropoietin after multiple subcutaneous doses in healthy subjects. Eur. J. Pharm. Sci. 2005, 26, 295–306. [Google Scholar] [CrossRef]
- Ramakrishnan, R.; Cheung, W.K.; Wacholtz, M.C.; Minton, N.; Jusko, W.J. Pharmacokinetic and pharmacodynamic modeling of recombinant human erythropoietin after single and multiple doses in healthy volunteers. J. Clin. Pharmacol. 2004, 44, 991–1002. [Google Scholar] [CrossRef]
- Ait-Oudhia, S.; Scherrmann, J.M.; Krzyzanski, W. Simultaneous pharmacokinetics/pharmacodynamics modeling of recombinant human erythropoietin upon multiple.e intravenous dosing in rats. J. Pharmacol. Exp. Ther. 2010, 334, 897–910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Ruixo, J.J.; Krzyzanski, W.; Hing, J. Pharmacodynamic analysis of recombinant human erythropoietin effect on reticulocyte production rate and age distribution in healthy subjects. Clin. Pharmacokinet 2008, 47, 399–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harker, L.A.; Roskos, L.K.; Marzec, U.M.; Carter, R.A.; Cherry, J.K.; Sundell, B.; Cheung, E.N.; Terry, D.; Sheridan, W. Effects of megakaryocyte growth and development factor on platelet production, platelet life span, and platelet function in healthy human volunteers. Blood 2000, 95, 2514–2522. [Google Scholar] [CrossRef] [PubMed]
- Chiou, W.L.; Robbie, G.; Chung, S.M.; Wu, T.C.; Ma, C. Correlation of plasma clearance of 54 extensively metabolized drugs between humans and rats: Mean allometric coefficient of 0.66. Pharm. Res. 1998, 15, 1474–1479. [Google Scholar] [CrossRef]
- Stevens, J.; Ploeger, B.A.; Hammarlund-Udenaes, M.; Osswald, G.; van der Graaf, P.H.; Danhof, M.; de Lange, E.C. Mechanism-based PK-PD model for the prolactin biological system response following an acute dopamine inhibition challenge: Quantitative extrapolation to humans. J. Pharm. Pharm. 2012, 39, 463–477. [Google Scholar] [CrossRef]
- West, G.B.; Brown, J.H.; Enquist, B.J. A general model for the origin of allometric scaling laws in biology. Science 1997, 276, 122–126. [Google Scholar] [CrossRef]
- Kagan, L.; Abraham, A.K.; Harrold, J.M.; Mager, D.E. Interspecies scaling of receptor-mediated pharmacokinetics and pharmacodynamics of type I interferons. Pharm. Res. 2010, 27, 920–932. [Google Scholar] [CrossRef]
- Huh, Y.; Smith, D.E.; Feng, M.R. Interspecies scaling and prediction of human clearance: Comparison of small- and macro-molecule drugs. Xenobiotica 2011, 41, 972–987. [Google Scholar] [CrossRef]
- Bussel, J.B.; Soff, G.; Balduzzi, A.; Cooper, N.; Lawrence, T.; Semple, J.W. A Review of Romiplostim Mechanism of Action and Clinical Applicability. Drug Des. Devel. Ther. 2021, 15, 2243–2268. [Google Scholar] [CrossRef]
- Major, A.; Bauer, C.; Breymann, C.; Huch, A.; Huch, R. rh-Erythropoietin stimulates immature reticulocyte release in man. Br. J. Haematol. 1994, 87, 605–608. [Google Scholar] [CrossRef]
- Risso, A.; Ciana, A.; Achilli, C.; Antonutto, G.; Minetti, G. Neocytolysis: None, one or many? A reappraisal and future perspectives. Front. Physiol. 2014, 5, 54. [Google Scholar] [CrossRef] [Green Version]
- Wiczling, P.; Krzyzanski, W.; Zychlińska, N.; Lewandowski, K.; Kaliszan, R. The quantification of reticulocyte maturation and neocytolysis in normal and erythropoietin stimulated rats. Biopharm. Drug Dispos. 2014, 35, 330–340. [Google Scholar] [CrossRef]
- Belurkar, S.; Shastry, I. The spectrum of red blood cell parameters in chronic kidney disease: A study of 300 cases. J. Appl. Hematol. 2019, 10, 61. [Google Scholar] [CrossRef]
- Prica, A.; Buckstein, R. Myelodysplastic syndrome.e.e.e successfully treated with adalimumab. J. Clin. Oncol. 2015, 33, e4–e6. [Google Scholar] [CrossRef]
- Capecchi, M.; Serpenti, F.; Giannotta, J.; Pettine, L.; Reda, G.; Martinelli, I.; Artoni, A.; Barcellini, W.; Fattizzo, B. Off-Label Use of Thrombopoietin Receptor Agonists: Case Series and Review of the Literature. Front. Oncol. 2021, 11, 680411. [Google Scholar] [CrossRef]
- Arora, N.; Gupta, A.; Li, H.C.; Sadeghi, N. Use of platelet and erythroid growth factors during induction chemotherapy for acute lymphoblastic leukaemia in a Jehovah’s Witness. BMJ Case Rep. 2018, 11, e226497. [Google Scholar] [CrossRef]
- KDOQI Clinical Practice Guideline and Clinical Practice Recommendations for anemia in chronic kidney disease: 2007 update of hemoglobin target. Am. J. Kidney Dis. 2007, 50, 471–530. [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter (Unit) | Description | Value | References |
|---|---|---|---|
| CLE (L/h) | Clearance of rHuEPO | 0.379 | [21,24] |
| KAE (1/h) | Absorption rate of rHuEPO | 0.0269 | |
| FE | Bioavailability of rHuEPO | 0.513 | |
| V2E (L) | Volume of distribution of the central compartment of rHuEPO | 3.25 | |
| V3E (L) | Volume of distribution of the peripheral compartment of rHuEPO | 1.64 | |
| QE (L/h) | Tissue distribution clearance of rHuEPO | 0.0993 | |
| RTOT (IU/L) | Baseline total receptor | 154.7 | |
| KME (IU/L) | Michaelis constant of rHuEPO | 48.1 | |
| KINTE (1/h) | Internalization rate constant of rHuEPO | 0.171 | |
| KDEGE (1/h) | Degradation rate constant | 0.392 | |
| CLR (L/h) | Clearance of romiplostim | 0.183 | [22] |
| V2R (L) | Volume of distribution of the central compartment of romiplostim | 4.781 | |
| KCPR (1/h) | Intercompartment rate constant of romiplostim | 0.0806 | |
| KPCR (1/h) | Intercompartment rate constant of romiplostim | 0.0148 | |
| KARM (1/h) | Absorption rate of romiplostim | 0.0254 | |
| FRM | Bioavailability of romiplostim | 0.499 | |
| KMR (ng/mL) | Michaelis constant of romiplostim | 0.131 | |
| ξR (fg/platelet) | Total c-Mpl receptor concentration | 0.0215 | |
| KINTR (1/h) | Internalization rate constant of romiplostim | 0.173 |
| Regimen Number | Dosing Regimen | Results | Comments |
|---|---|---|---|
| 1 | Romiplostim QW 1 μg/kg for 16 weeks | Platelet count exceeds 0.35 × 1012/L on day 11 | Unacceptable |
| 2 | Romiplostim 1 μg/kg Q2W from the first week (weeks 1, 3, 5, 7, 9, 11, 13, 15) | Platelet count exceeds 0.35 × 1012/L on day 11 | Unacceptable |
| 3 | Romiplostim 1μg/kg Q2W from the second week (weeks 2, 4, 6, 8, 10, 12, 14, 16) | Platelet count exceeds 0.35 × 1012/L on day 31 | Unacceptable |
| 4 | Romiplostim 1 μg/kg Q3W from the first week (weeks 1, 4, 7, 10, 13, 16) | Platelet count exceeds 0.35 × 1012/L on day 11 | Unacceptable |
| 5 | Romiplostim 1 μg/kg Q3W from the second week (weeks 2, 5, 8, 11, 14) | Platelet count will not exceed 0.35 × 1012/L | Acceptable |
| 6 | Romiplostim 1 μg/kg Q2W from the third week (weeks 3, 5, 7, 9, 11, 13, 15) | Platelet count exceeds 0.35 × 1012/L on day 50 | Unacceptable |
| 7 | Romiplostim 1 μg/kg Q4W from the first week (weeks 1, 5, 9, 13) | Platelet count exceeds 0.35 × 1012/L on day 11 | Unacceptable |
| 8 | Romiplostim 1 μg/kg Q4W from the second week (weeks 2, 6, 10, 14) | Platelet count will not exceed 0.35 × 1012/L | Acceptable (Recommended) |
| Parameter | Unit | Estimated Value (Rat) | Scaled Value (Humans) | The Observed Value in Humans |
|---|---|---|---|---|
| TMP | h | 47.8 [26] | 137.1 | 142 [22] |
| TPLT | day | 6.17 [26] | 10.6 | 8–12 [22,33] |
| PLT0 | ×1012 cells/L | 0.869 [26] | Fixed to human value | 0.23 [22,28] |
| TRET | h | 20 [14] | 44.8 | 57.3 [24,32] |
| TRBC | day | 60.8 [14] | 119.6 | 120 [29] |
| RBC0 | ×1012 cells/L | 7.38 [14] | Fixed to human value | 4.4 [24,27] |
| Parameter | Parameter Explanation | Unit | Value |
|---|---|---|---|
| TMP | Mean lifespan of megakaryocyte cells | h | 137.1 (scaled) |
| TPLT | Mean lifespan of platelets | h | 254.4 (scaled) |
| PLT0 | Baseline platelets in blood | ×1012 cells/L | 0.23 (fixed to human value) |
| TRBC | Mean residence time for mature RBCs | day | 119.6 (scaled) |
| TRET | Mean residence time for RETs | h | 44.8 (scaled) |
| RBC0 | Baseline RBCs concentration | ×1012 cells/L | 4.4 (fixed to human value) |
| KE | First-order rate constant of MEPs differentiate into BFU-E | ×10−4/h | 6.84 (not scaled) |
| KM | First-order rate constant of MEPs differentiate into MK1 | ×10−4/h | 1.18 (not scaled) |
| SmaxRM1 | Maximal stimulus of romiplostim on MEPs | Dimensionless | 1.67 (not scaled) |
| SmaxRM2 | Maximal stimulus of romiplostim on MK-committed pathway | Dimensionless | 27.8 (not scaled) |
| SmaxEPO1 | Maximal stimulus of rHuEPO on MEPs | Dimensionless | 11.3 (not scaled) |
| SC50RM | The concentrations of romiplostim that induce a half-maximum effect | ng/mL | 11.9 (not scaled) |
| SC50EPO | The concentrations of rHuEPO that induce a half-maximum effect | mIU/mL | 46.9 (not scaled) |
| ImaxEPO | Maximal inhibition of rHuEPO on RETs aging rates | Dimensionless | 0.422 (not scaled) |
| IC50EPO | The concentration of rHuEPO that induces half-maximum inhibition | mIU/mL | 5.59 (not scaled) |
| MCH | Mean corpuscular hemoglobin | pg/cell | 30.2 (fixed to human value) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, X.; Krzyzanski, W.; Liu, D.; Wong, R.S.M.; Yan, X. Scaling Pharmacodynamics from Rats to Humans to Support Erythropoietin and Romiplostim Combination Therapy to Treat Erythropoietin-Resistant Anemia. Pharmaceutics 2023, 15, 344. https://doi.org/10.3390/pharmaceutics15020344
Fan X, Krzyzanski W, Liu D, Wong RSM, Yan X. Scaling Pharmacodynamics from Rats to Humans to Support Erythropoietin and Romiplostim Combination Therapy to Treat Erythropoietin-Resistant Anemia. Pharmaceutics. 2023; 15(2):344. https://doi.org/10.3390/pharmaceutics15020344
Chicago/Turabian StyleFan, Xiaoqing, Wojciech Krzyzanski, Dongyang Liu, Raymond S. M. Wong, and Xiaoyu Yan. 2023. "Scaling Pharmacodynamics from Rats to Humans to Support Erythropoietin and Romiplostim Combination Therapy to Treat Erythropoietin-Resistant Anemia" Pharmaceutics 15, no. 2: 344. https://doi.org/10.3390/pharmaceutics15020344