
Recent Advances in Functionalized Electrospun Membranes for Periodontal Regeneration
 , , , , , , ,
, , , , , , ,  and
and
Abstract
:1. Introduction
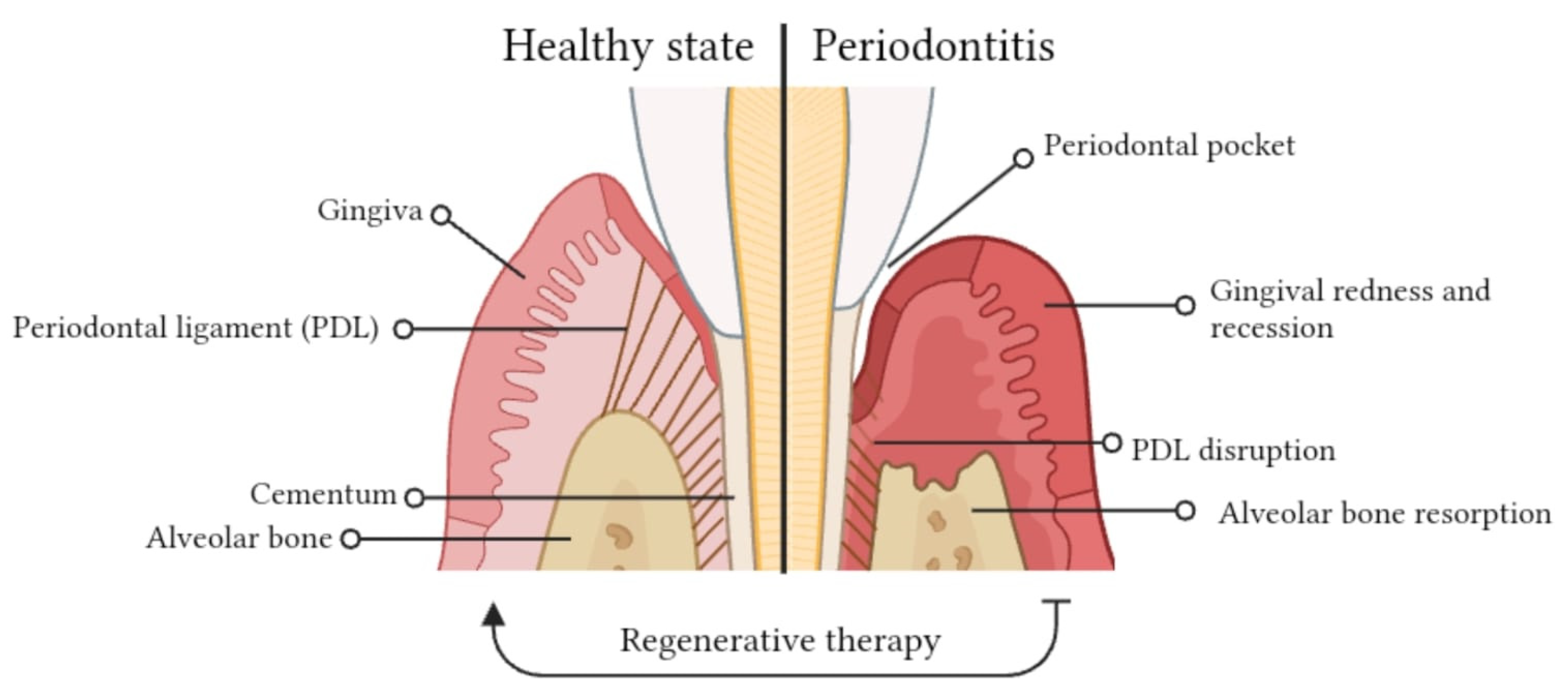
2. Complex Architecture of the Periodontium
2.1. Gingiva: Composition of Periodontal Tissues
2.2. Periodontal Ligament (PDL): The Tooth’s Anchor and Guardian
2.3. Alveolar Bone: Tooth Socket and Protector
2.4. Cementum: Tooth Support and Connection
3. Periodontitis Onset and Progression
3.1. Stages of Periodontitis
3.2. Microbial Factors in Periodontitis
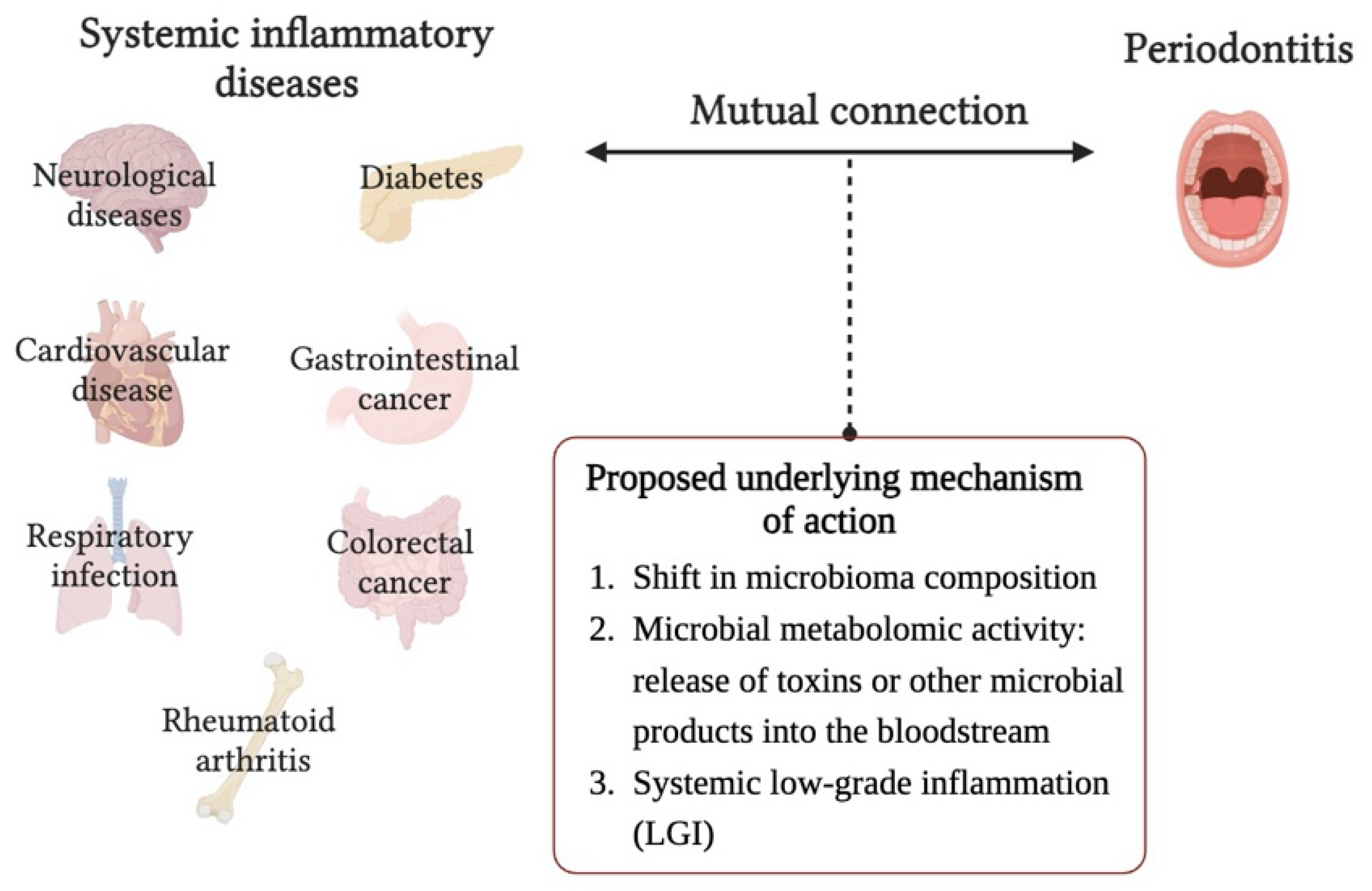
3.3. Systemic Implications of Periodontitis
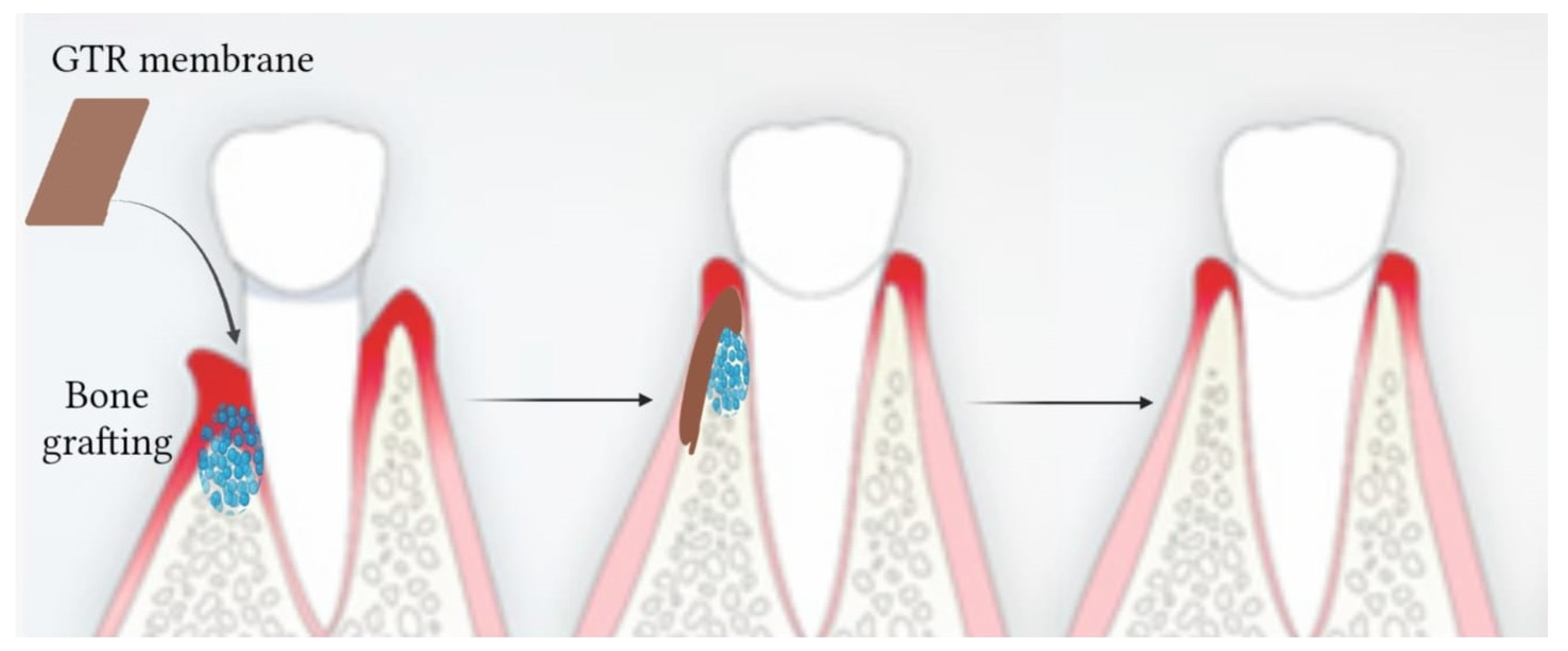
4. The Innovation of Tissue Engineering and Regenerative Medicine in Periodontal Therapy
4.1. Tissue Engineering (TE) and Regenerative Medicine (RM)
4.2. TE and RM in Periodontal Therapy
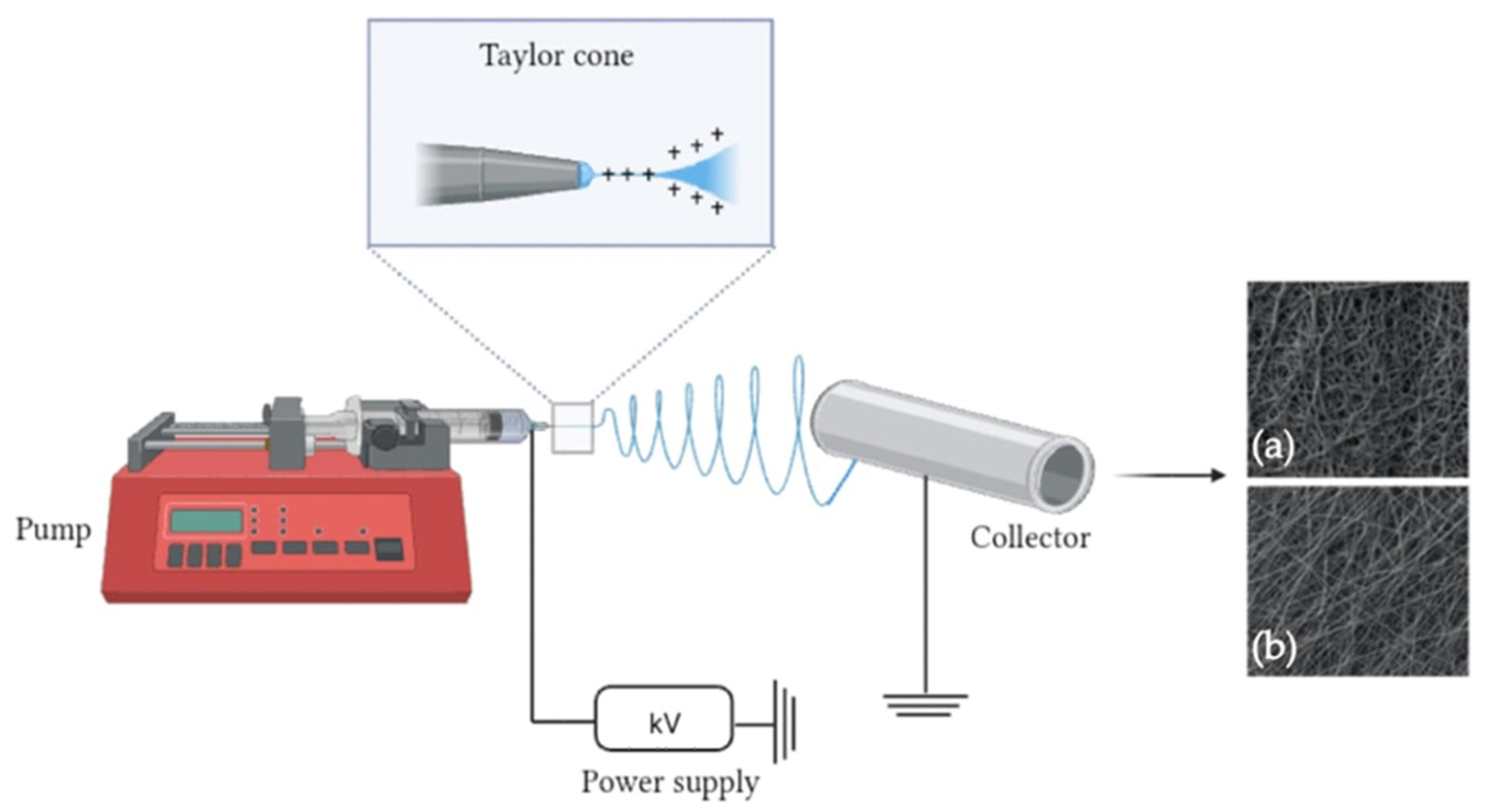
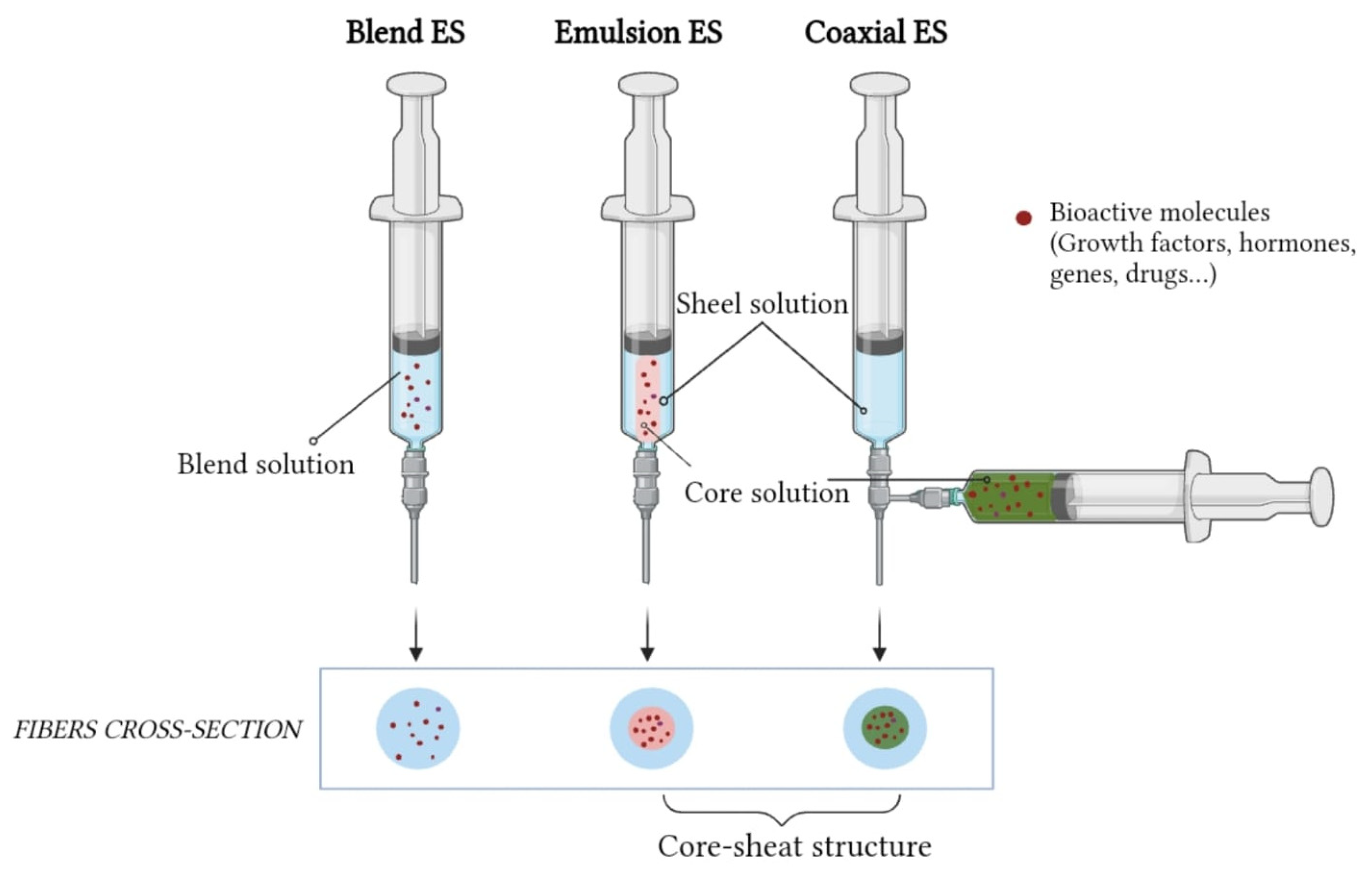
5. Electrospinning Technique
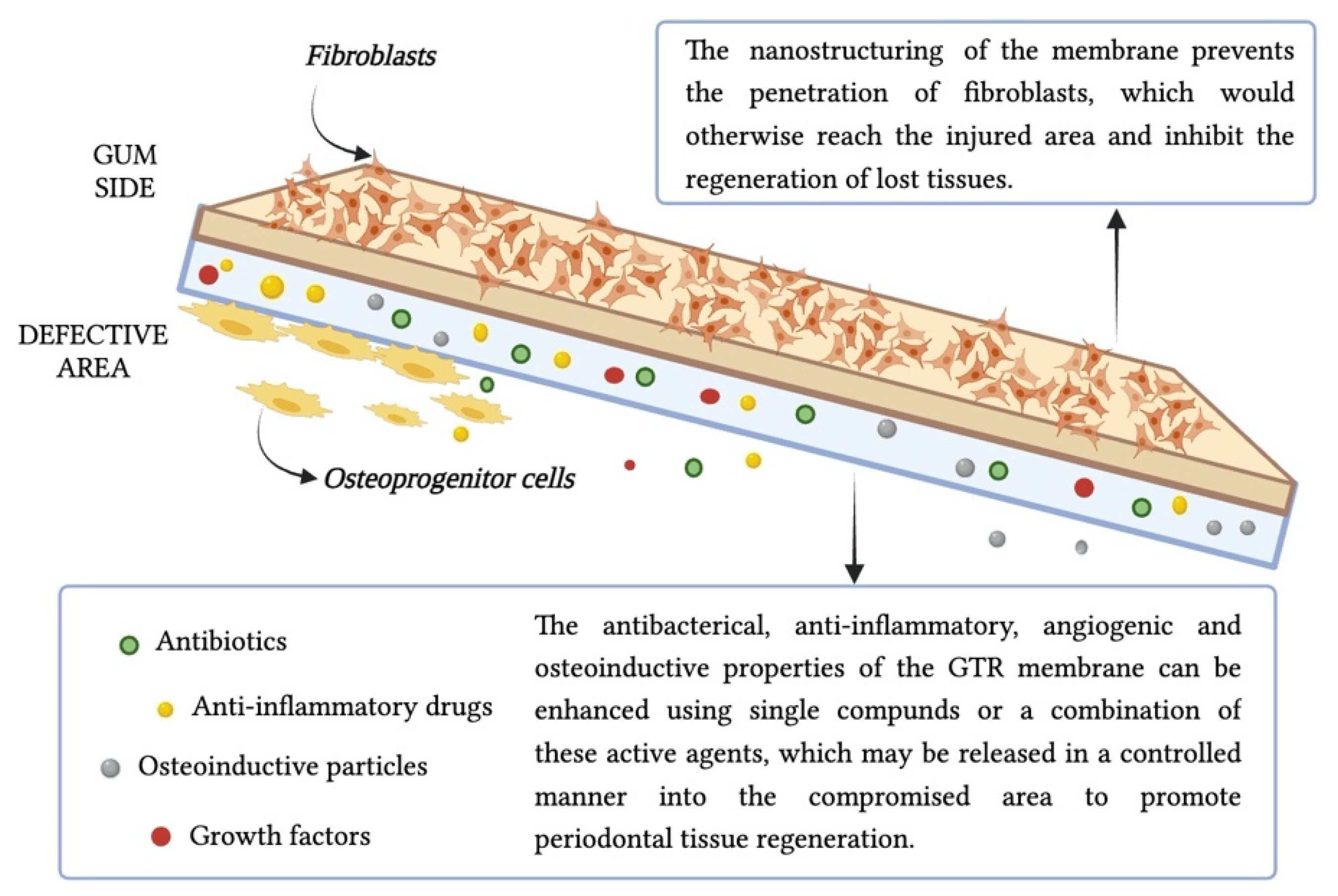
6. Functionalization of Electrospun Membranes to Potentiate Periodontal Regeneration
6.1. Anti-Infective Drugs
6.2. Immune Response Modulation
6.3. Other Bioactive Agents and Innovative Approaches
6.4. Multilayered Electrospun Mats
7. Conclusions and Future Prospective
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| GTR | GuidedTissue Regeneration |
| GBR | GuidedBone Regeneration |
| ECM | ExtracellularMatrix |
| PDL | PeriodontalLigaments |
| TE | TissueEngineering |
| ES | Electrospinning |
| HA | Hyaluronicacid |
| PVA | Poly(vinylalcohol) |
| PGA | Poly(glycolicacid) |
| OM | OralMicrobiome |
| LGI | Low-GradeInflammation |
| RM | RegenerativeMedicine |
| ePTFE | expandedpolytetrafluoroethylene |
| SEM | ScanningElectron Microscopy |
| CAL | ClinicalAttachment Level |
| MNZ | Metronidazole |
| PCL | Polycaprolactone |
| DOX | doxycycline |
| mPCL | medicalgrade PCL |
| NSAIDs | Non-steroidalanti-inflammatory drugs |
| PG | prostaglandin |
| BMPs | bonemorphogenetic proteins |
| PDGF | platelet-derivedgrowth factor |
| ALP | alkalinephosphatase |
| GAM | gene-activatedmatrix |
| nHA | nano-hydroxyapatite |
| BG | bioglasses |
| AuNPs | goldnanoparticles |
| GNs | gelatinnanospheres |
| AMX | Amoxicilline |
| PLGA | poly(lactic-co-glycolicacid) |
| PTH | parathyroidhormone |
| MgONPs | Magnesiumoxide nanoparticles |
| 2D | two-dimensional |
| 3D | three-dimensional |
References
- Hou, K.; Wu, Z.-X.; Chen, X.-Y.; Wang, J.-Q.; Zhang, D.; Xiao, C.; Zhu, D.; Koya, J.B.; Wei, L.; Li, J.; et al. Microbiota in Health and Diseases. Sig. Transduct. Target. Ther. 2022, 7, 135. [Google Scholar] [CrossRef]
- Manos, J. The Human Microbiome in Disease and Pathology. APMIS 2022, 130, 690–705. [Google Scholar] [CrossRef]
- Aggarwal, N.; Kitano, S.; Puah, G.R.Y.; Kittelmann, S.; Hwang, I.Y.; Chang, M.W. Microbiome and Human Health: Current Understanding, Engineering, and Enabling Technologies. Chem. Rev. 2023, 123, 31–72. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Bello, M.G.; Godoy-Vitorino, F.; Knight, R.; Blaser, M.J. Role of the Microbiome in Human Development. Gut 2019, 68, 1108–1114. [Google Scholar] [CrossRef]
- Willis, J.R.; Gabaldón, T. The Human Oral Microbiome in Health and Disease: From Sequences to Ecosystems. Microorganisms 2020, 8, 308. [Google Scholar] [CrossRef] [PubMed]
- Mendes, L.; Azevedo, N.F.; Felino, A.; Pinto, M.G. Relationship between Invasion of the Periodontium by Periodontal Pathogens and Periodontal Disease: A Systematic Review. Virulence 2015, 6, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Di Benedetto, A.; Gigante, I.; Colucci, S.; Grano, M. Periodontal Disease: Linking the Primary Inflammation to Bone Loss. Clin. Dev. Immunol. 2013, 2013, 503754. [Google Scholar] [CrossRef]
- Kwon, T.; Lamster, I.B.; Levin, L. Current Concepts in the Management of Periodontitis. Int. Dent. J. 2021, 71, 462–476. [Google Scholar] [CrossRef]
- Chen, F.-M.; Jin, Y. Periodontal Tissue Engineering and Regeneration: Current Approaches and Expanding Opportunities. Tissue Eng. Part B Rev. 2010, 16, 219–255. [Google Scholar] [CrossRef]
- Chen, F.-M.; Zhang, J.; Zhang, M.; An, Y.; Chen, F.; Wu, Z.-F. A Review on Endogenous Regenerative Technology in Periodontal Regenerative Medicine. Biomaterials 2010, 31, 7892–7927. [Google Scholar] [CrossRef]
- Muthukrishnan, L. An Overview on Electrospinning and Its Advancement toward Hard and Soft Tissue Engineering Applications. Colloid Polym. Sci. 2022, 300, 875–901. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Wang, J.; Guo, H.; Liu, L.; Xu, W.; Duan, G. Structural Design toward Functional Materials by Electrospinning: A Review. e-Polymers 2020, 20, 682–712. [Google Scholar] [CrossRef]
- Al-Abduljabbar, A.; Farooq, I. Electrospun Polymer Nanofibers: Processing, Properties, and Applications. Polymers 2022, 15, 65. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.C.; Haider, A.; Choi, Y.; Kang, I. Nanofibrous Scaffolds in Biomedical Applications. Biomater. Res. 2014, 18, 1–11. [Google Scholar] [CrossRef]
- Fadil, F.; Affandi, N.D.N.; Misnon, M.I.; Bonnia, N.N.; Harun, A.M.; Alam, M.K. Review on Electrospun Nanofiber-Applied Products. Polymers 2021, 13, 2087. [Google Scholar] [CrossRef]
- Ferraris, S.; Spriano, S.; Scalia, A.C.; Cochis, A.; Rimondini, L.; Cruz-Maya, I.; Guarino, V.; Varesano, A.; Vineis, C. Topographical and Biomechanical Guidance of Electrospun Fibers for Biomedical Applications. Polymers 2020, 12, 2896. [Google Scholar] [CrossRef]
- Ramakrishna, S.; Zamani, M.; Molamma, P. Prabhakaran Advances in Drug Delivery via Electrospun and Electrosprayed Nanomaterials. IJN 2013, 8, 2997. [Google Scholar] [CrossRef]
- Berezow, A.B.; Darveau, R.P. Microbial Shift and Periodontitis: Microbial Shift. Periodontology 2000 2011, 55, 36–47. [Google Scholar] [CrossRef]
- Mamidi, N.; Flores Otero, J.F. Metallic and Carbonaceous Nanoparticles for Dentistry Applications. Curr. Opin. Biomed. Eng. 2023, 25, 100436. [Google Scholar] [CrossRef]
- Nanci, A.; Bosshardt, D.D. Structure of Periodontal Tissues in Health and Disease. Periodontol 2000 2006, 40, 11–28. [Google Scholar] [CrossRef]
- De Jong, T.; Bakker, A.D.; Everts, V.; Smit, T.H. The Intricate Anatomy of the Periodontal Ligament and Its Development: Lessons for Periodontal Regeneration. J. Periodont. Res. 2017, 52, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Orban, B. Histology and Physiology of the Gingiva. J. Am. Dent. Assoc. 1952, 44, 624–628. [Google Scholar] [CrossRef] [PubMed]
- Aisenberg, M.S. Adaptability of the Periodontal Membrane. J. Dent. Res. 1947, 26, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Ainamo, J.; Löe, H. Anatomical Characteristics of Gingiva. A Clinical and Microscopic Study of the Free and Attached Gingiva. J. Periodontol. 1966, 37, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Shirmohammadi, A.; Faramarzie, M.; Lafzi, A. A Clinical Evaluation of Anatomic Features of Gingiva in Dental Students in Tabriz, Iran. J. Dent. Res. Dent. Clin. Dent. Prospect. 2008, 2, 90. [Google Scholar]
- Hemalatha, D.M. Attached Giniva- A Reliable Factor to Cling-To: Review Article. Int. J. Drug Res. Dent. Sci. 2022, 4, 9–16. [Google Scholar]
- Trulsson, M. Sensory-Motor Function of Human Periodontal Mechanoreceptors. J. Oral. Rehabil. 2006, 33, 262–273. [Google Scholar] [CrossRef] [PubMed]
- Melcher, A.H. On the Repair Potential of Periodontal Tissues. J. Periodontol. 1976, 47, 256–260. [Google Scholar] [CrossRef]
- Beertsen, W.; McCulloch, C.A.G.; Sodek, J. The Periodontal Ligament: A Unique, Multifunctional Connective Tissue. Periodontol 2000 1997, 13, 20–40. [Google Scholar] [CrossRef]
- Li, Y.; Zhan, Q.; Bao, M.; Yi, J.; Li, Y. Biomechanical and Biological Responses of Periodontium in Orthodontic Tooth Movement: Up-Date in a New Decade. Int. J. Oral Sci. 2021, 13, 20. [Google Scholar] [CrossRef]
- Willis, R.D.; DiCosimo, C.J. The Absence of Proprioceptive Nerve Endings in the Human Periodontal Ligament: The Role of Periodontal Mechanoreceptors in the Reflex Control of Mastication. Oral Surg. Oral Med. Oral Pathol. 1979, 48, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Hathaway-Schrader, J.D.; Novince, C.M. Maintaining Homeostatic Control of Periodontal Bone Tissue. Periodontology 2000 2021, 86, 157–187. [Google Scholar] [CrossRef] [PubMed]
- Blum, I.R. Contemporary Views on Dry Socket (Alveolar Osteitis): A Clinical Appraisal of Standardization, Aetiopathogenesis and Management: A Critical Review. Int. J. Oral Maxillofac. Surg. 2002, 31, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Wen, D.; Qing, L.; Harrison, G.; Golub, E.; Akintoye, S. Anatomic Site Variability in Rat Skeletal Uptake and Desorption of Fluorescently Labeled Bisphosphonate: Variable Bisphosphonate Skeletal Uptake and Release. Oral Dis. 2011, 17, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, M.; Yuen, T.; Sun, L.; Rosen, C.J. Regulation of Skeletal Homeostasis. Endocr. Rev. 2018, 39, 701–718. [Google Scholar] [CrossRef] [PubMed]
- Saito, M.M.; Onuma, K.; Yamakoshi, Y. Cementum Is Key to Periodontal Tissue Regeneration: A Review on Apatite Microstructures for Creation of Novel Cementum-based Dental Implants. Genesis 2023, 61, e23514. [Google Scholar] [CrossRef]
- Yamamoto, T.; Hasegawa, T.; Yamamoto, T.; Hongo, H.; Amizuka, N. Histology of Human Cementum: Its Structure, Function, and Development. Jpn. Dent. Sci. Rev. 2016, 52, 63–74. [Google Scholar] [CrossRef]
- Liu, B.; Faller, L.L.; Klitgord, N.; Mazumdar, V.; Ghodsi, M.; Sommer, D.D.; Gibbons, T.R.; Treangen, T.J.; Chang, Y.-C.; Li, S.; et al. Deep Sequencing of the Oral Microbiome Reveals Signatures of Periodontal Disease. PLoS ONE 2012, 7, e37919. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Chavakis, T. Local and Systemic Mechanisms Linking Periodontal Disease and Inflammatory Comorbidities. Nat. Rev. Immunol. 2021, 21, 426–440. [Google Scholar] [CrossRef]
- Nazir, M.A. Prevalence of Periodontal Disease, Its Association with Systemic Diseases and Prevention. Int. J. Health Sci. 2017, 11, 72. [Google Scholar]
- Bamashmous, S.; Kotsakis, G.A.; Kerns, K.A.; Leroux, B.G.; Zenobia, C.; Chen, D.; Trivedi, H.M.; McLean, J.S.; Darveau, R.P. Human Variation in Gingival Inflammation. Proc. Natl. Acad. Sci. USA 2021, 118, e2012578118. [Google Scholar] [CrossRef] [PubMed]
- Garlet, G.P. Destructive and Protective Roles of Cytokines in Periodontitis: A Re-Appraisal from Host Defense and Tissue Destruction Viewpoints. J. Dent. Res. 2010, 89, 1349–1363. [Google Scholar] [CrossRef] [PubMed]
- Griffen, A.L.; Beall, C.J.; Campbell, J.H.; Firestone, N.D.; Kumar, P.S.; Yang, Z.K.; Podar, M.; Leys, E.J. Distinct and Complex Bacterial Profiles in Human Periodontitis and Health Revealed by 16S Pyrosequencing. ISME J. 2012, 6, 1176–1185. [Google Scholar] [CrossRef] [PubMed]
- Arzate, H.; Zeichner-David, M.; Mercado-Celis, G. Cementum Proteins: Role in Cementogenesis, Biomineralization, Periodontium Formation and Regeneration. Periodontol 2000 2015, 67, 211–233. [Google Scholar] [CrossRef]
- Gasner, N.S.; Schure, R.S. Periodontal Disease. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK554590/ (accessed on 10 April 2023).
- Meuric, V.; Le Gall-David, S.; Boyer, E.; Acuña-Amador, L.; Martin, B.; Fong, S.B.; Barloy-Hubler, F.; Bonnaure-Mallet, M. Signature of Microbial Dysbiosis in Periodontitis. Appl. Environ. Microbiol. 2017, 83, e00462-17. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and Grading of Periodontitis: Framework and Proposal of a New Classification and Case Definition. J. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef]
- Cecoro, G.; Annunziata, M.; Iuorio, M.T.; Nastri, L.; Guida, L. Periodontitis, Low-Grade Inflammation and Systemic Health: A Scoping Review. Medicina 2020, 56, 272. [Google Scholar] [CrossRef]
- Lenartova, M.; Tesinska, B.; Janatova, T.; Hrebicek, O.; Mysak, J.; Janata, J.; Najmanova, L. The Oral Microbiome in Periodontal Health. Front. Cell. Infect. Microbiol. 2021, 11, 629723. [Google Scholar] [CrossRef]
- Takahashi, Y.; Watanabe, N.; Kamio, N.; Kobayashi, R.; Iinuma, T.; Imai, K. Aspiration of Periodontopathic Bacteria Due to Poor Oral Hygiene Potentially Contributes to the Aggravation of COVID-19. J. Oral Sci. 2021, 63, 1–3. [Google Scholar] [CrossRef]
- Huang, S.; He, T.; Yue, F.; Xu, X.; Wang, L.; Zhu, P.; Teng, F.; Sun, Z.; Liu, X.; Jing, G.; et al. Longitudinal Multi-Omics and Microbiome Meta-Analysis Identify an Asymptomatic Gingival State That Links Gingivitis, Periodontitis, and Aging. mBio 2021, 12, e03281-20. [Google Scholar] [CrossRef]
- Lang, N.P.; Bartold, P.M. Periodontal Health. J. Periodontol. 2018, 89, S9–S16. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, M.; Polizzi, A.; Santonocito, S.; Romano, A.; Lombardi, T.; Isola, G. Impact of Oral Microbiome in Periodontal Health and Periodontitis: A Critical Review on Prevention and Treatment. Int. J. Mol. Sci. 2022, 23, 5142. [Google Scholar] [CrossRef] [PubMed]
- Harrison, R.H.; St-Pierre, J.-P.; Stevens, M.M. Tissue Engineering and Regenerative Medicine: A Year in Review. Tissue Eng. Part B Rev. 2014, 20, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Arjunan, A.; Baroutaji, A.; Robinson, J.; Praveen, A.S.; Pollard, A.; Wang, C. Future Directions and Requirements for Tissue Engineering Biomaterials. Encycl. Smart Mater. 2021, 1, 195–218. [Google Scholar]
- Eldeeb, A.E.; Salah, S.; Elkasabgy, N.A. Biomaterials for Tissue Engineering Applications and Current Updates in the Field: A Comprehensive Review. AAPS PharmSciTech 2022, 23, 267. [Google Scholar] [CrossRef]
- Vacanti, C.A. The History of Tissue Engineering. J. Cell. Mol. Med. 2006, 10, 569–576. [Google Scholar] [CrossRef]
- Han, F.; Wang, J.; Ding, L.; Hu, Y.; Li, W.; Yuan, Z.; Guo, Q.; Zhu, C.; Yu, L.; Wang, H.; et al. Tissue Engineering and Regenerative Medicine: Achievements, Future, and Sustainability in Asia. Front. Bioeng. Biotechnol. 2020, 8, 83. [Google Scholar] [CrossRef]
- Esdaille, C.J.; Washington, K.S.; Laurencin, C.T. Regenerative Engineering: A Review of Recent Advances and Future Directions. Regen. Med. 2021, 16, 495–512. [Google Scholar] [CrossRef]
- Salgado, A.J.; Oliveira, J.M.; Martins, A.; Teixeira, F.G.; Silva, N.A.; Neves, N.M.; Sousa, N.; Reis, R.L. Chapter One—Tissue Engineering and Regenerative Medicine: Past, Present, and Future. In International Review of Neurobiology; Geuna, S., Perroteau, I., Tos, P., Battiston, B., Eds.; Academic Press: Cambridge, MA, USA, 2013; Volume 108, pp. 1–33. ISBN 0074-7742. [Google Scholar]
- Ikada, Y. Challenges in Tissue Engineering. J. R. Soc. Interface 2006, 3, 589–601. [Google Scholar] [CrossRef]
- Eltom, A.; Zhong, G.; Muhammad, A. Scaffold Techniques and Designs in Tissue Engineering Functions and Purposes: A Review. Adv. Mater. Sci. Eng. 2019, 2019, 3429527. [Google Scholar] [CrossRef]
- Marques, D.; Teixeira, L.N.; Elias, C.N.; Lemos, A.B.; Martinez, E.F. Surface Topography of Resorbable Porcine Collagen Membranes, and Their Effect on Early Osteogenesis: An in Vitro Study. J. Stomatol. Oral Maxillofac. Surg. 2023, 124, 101607. [Google Scholar] [CrossRef]
- Bianchi, S.; Bernardi, S.; Simeone, D.; Torge, D.; Macchiarelli, G.; Marchetti, E. Proliferation and Morphological Assessment of Human Periodontal Ligament Fibroblast towards Bovine Pericardium Membranes: An in Vitro Study. Materials 2022, 15, 8284. [Google Scholar] [CrossRef] [PubMed]
- Socci, M.C.; Rodríguez, G.; Oliva, E.; Fushimi, S.; Takabatake, K.; Nagatsuka, H.; Felice, C.J.; Rodríguez, A.P. Polymeric Materials, Advances and Applications in Tissue Engineering: A Review. Bioengineering 2023, 10, 218. [Google Scholar] [CrossRef] [PubMed]
- Altyar, A.E.; El-Sayed, A.; Abdeen, A.; Piscopo, M.; Mousa, S.A.; Najda, A.; Abdel-Daim, M.M. Future Regenerative Medicine Developments and Their Therapeutic Applications. Biomed. Pharmacother. 2023, 158, 114131. [Google Scholar] [CrossRef] [PubMed]
- Naahidi, S.; Jafari, M.; Logan, M.; Wang, Y.; Yuan, Y.; Bae, H.; Dixon, B.; Chen, P. Biocompatibility of Hydrogel-Based Scaffolds for Tissue Engineering Applications. Biotechnol. Adv. 2017, 35, 530–544. [Google Scholar] [CrossRef] [PubMed]
- Ma, P.X. Scaffolds for Tissue Fabrication. Mater. Today 2004, 7, 30–40. [Google Scholar] [CrossRef]
- Sultana, N. 1-Mechanical and Biological Properties of Scaffold Materials. In Functional 3D Tissue Engineering Scaffolds; Deng, Y., Kuiper, J., Eds.; Woodhead Publishing: Sawston, UK, 2018; pp. 1–21. ISBN 978-0-08-100979-6. [Google Scholar]
- Tajvar, S.; Hadjizadeh, A.; Samandari, S.S. Scaffold Degradation in Bone Tissue Engineering: An Overview. Int. Biodeterior. Biodegrad. 2023, 180, 105599. [Google Scholar] [CrossRef]
- Joyce, K.; Buljovcic, Z.; Rosic, G.; Kaszkin-Bettag, M.; Pandit, A. Issues with Tissues: Trends in Tissue-Engineered Products in Clinical Trials in the European Union. Tissue Eng. Part B Rev. 2023, 29, 78–88. [Google Scholar] [CrossRef]
- Charbe, N.B.; Tambuwala, M.; Palakurthi, S.S.; Warokar, A.; Hromić-Jahjefendić, A.; Bakshi, H.; Zacconi, F.; Mishra, V.; Khadse, S.; Aljabali, A.A.; et al. Biomedical Applications of Three-Dimensional Bioprinted Craniofacial Tissue Engineering. Bioeng. Transl. Med. 2023, 8, e10333. [Google Scholar] [CrossRef]
- de Assis, A.C.C.; Reis, A.L.S.; Nunes, L.V.; Ferreira, L.F.R.; Bilal, M.; Iqbal, H.M.N.; Soriano, R.N. Stem Cells and Tissue Engineering-Based Therapeutic Interventions: Promising Strategies to Improve Peripheral Nerve Regeneration. Cell. Mol. Neurobiol. 2023, 43, 433–454. [Google Scholar] [CrossRef]
- Heath, C.A. Cells for Tissue Engineering. Trends Biotechnol. 2000, 18, 17–19. [Google Scholar] [CrossRef]
- Rosso, F.; Giordano, A.; Barbarisi, M.; Barbarisi, A. From Cell–ECM Interactions to Tissue Engineering. J. Cell. Physiol. 2004, 199, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Nitti, P.; Narayanan, A.; Pellegrino, R.; Villani, S.; Madaghiele, M.; Demitri, C. Cell-Tissue Interaction: The Biomimetic Approach to Design Tissue Engineered Biomaterials. Bioengineering 2023, 10, 1122. [Google Scholar] [CrossRef] [PubMed]
- Cornelius Timothius, C.J.; Kilic, H.N.; Gandhi, K.K.; Kakar, A.; John, V. Particulate Bone Graft Materials for Periodontal and Implant Surgery: A Narrative Review and Case Series. Dent. Rev. 2023, 3, 100068. [Google Scholar] [CrossRef]
- Mancini, L.; Romandini, M.; Fratini, A.; Americo, L.M.; Panda, S.; Marchetti, E. Biomaterials for Periodontal and Peri-Implant Regeneration. Materials 2021, 14, 3319. [Google Scholar] [CrossRef] [PubMed]
- Ho-Shui-Ling, A.; Bolander, J.; Rustom, L.E.; Johnson, A.W.; Luyten, F.P.; Picart, C. Bone Regeneration Strategies: Engineered Scaffolds, Bioactive Molecules and Stem Cells Current Stage and Future Perspectives. Biomaterials 2018, 180, 143–162. [Google Scholar] [CrossRef] [PubMed]
- Abdo, V.L.; Suarez, L.J.; de Paula, L.G.; Costa, R.C.; Shibli, J.; Feres, M.; Barão, V.A.R.; Bertolini, M.; Souza, J.G.S. Underestimated Microbial Infection of Resorbable Membranes on Guided Regeneration. Colloids Surf. B Biointerfaces 2023, 226, 113318. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhao, L.; Ngai, T. Multiphasic Membranes/Scaffolds for Periodontal Guided Tissue Regeneration. Macromol. Mater. Eng. 2023, 308, 2300081. [Google Scholar] [CrossRef]
- Calciolari, E.; Corbella, S.; Gkranias, N.; Viganó, M.; Sculean, A.; Donos, N. Efficacy of Biomaterials for Lateral Bone Augmentation Performed with Guided Bone Regeneration. A Network Meta-Analysis. Periodontology 2000 2023, 11, 624. [Google Scholar] [CrossRef]
- Mizraji, G.; Davidzohn, A.; Gursoy, M.; Gursoy, U.K.; Shapira, L.; Wilensky, A. Membrane Barriers for Guided Bone Regeneration: An Overview of Available Biomaterials. Periodontology 2000 2023. [Google Scholar] [CrossRef]
- Ma, Y.-F.; Yan, X.-Z. Periodontal Guided Tissue Regeneration Membranes: Limitations and Possible Solutions for the Bottleneck Analysis. Tissue Eng. Part B Rev. 2023, 29, 532–544. [Google Scholar] [CrossRef]
- Gu, P.; Wang, Z.; Xie, Q.; Sun, H.; Huang, Y.; Yu, Z.; Bi, X.; Zhang, D.; Chen, J.; Wang, J.; et al. Electrospun Silk Fibroin/Poly(Lactide-Co-ε-Caprolactone) Nanofibrous Scaffolds for Bone Regeneration. IJN 2016, 11, 1483–1500. [Google Scholar] [CrossRef]
- Huebsch, N.; Mooney, D.J. Inspiration and Application in the Evolution of Biomaterials. Nature 2009, 462, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Qasim, S.B.; Najeeb, S.; Delaine-Smith, R.M.; Rawlinson, A.; Ur Rehman, I. Potential of Electrospun Chitosan Fibers as a Surface Layer in Functionally Graded GTR Membrane for Periodontal Regeneration. Dent. Mater. 2017, 33, 71–83. [Google Scholar] [CrossRef] [PubMed]
- Lotfi, G.; Shokrgozar, M.A.; Mofid, R.; Abbas, F.M.; Ghanavati, F.; Baghban, A.A.; Yavari, S.K.; Pajoumshariati, S. Biological Evaluation (In Vitro and In Vivo) of Bilayered Collagenous Coated (Nano Electrospun and Solid Wall) Chitosan Membrane for Periodontal Guided Bone Regeneration. Ann. Biomed. Eng. 2016, 44, 2132–2144. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Chen, W.; Feng, Z.; Liu, Y.; Liu, P.; Xie, Y.; Yu, D.-G. Electrospun Nanofibers for Periodontal Treatment: A Recent Progress. IJN 2022, 17, 4137–4162. [Google Scholar] [CrossRef] [PubMed]
- Teng, S.-H.; Lee, E.-J.; Wang, P.; Shin, D.-S.; Kim, H.-E. Three-Layered Membranes of Collagen/Hydroxyapatite and Chitosan for Guided Bone Regeneration. J. Biomed. Mater. Res. 2008, 87B, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Bottino, M.C.; Thomas, V.; Schmidt, G.; Vohra, Y.K.; Chu, T.-M.G.; Kowolik, M.J.; Janowski, G.M. Recent Advances in the Development of GTR/GBR Membranes for Periodontal Regeneration—A Materials Perspective. Dent. Mater. 2012, 28, 703–721. [Google Scholar] [CrossRef]
- Shields, K.J.; Beckman, M.J.; Bowlin, G.L.; Wayne, J.S. Mechanical Properties and Cellular Proliferation of Electrospun Collagen Type II. Tissue Eng. 2004, 10, 1510–1517. [Google Scholar] [CrossRef]
- Rabea, E.I.; Badawy, M.E.-T.; Stevens, C.V.; Smagghe, G.; Steurbaut, W. Chitosan as Antimicrobial Agent: Applications and Mode of Action. Biomacromolecules 2003, 4, 1457–1465. [Google Scholar] [CrossRef]
- Pang, E.; Paik, J.; Kim, S.; Jung, U.; Kim, C.; Cho, K.; Kim, C.; Choi, S. Effects of Chitosan on Human Periodontal Ligament Fibroblasts In Vitro and on Bone Formation in Rat Calvarial Defects. J. Periodontol. 2005, 76, 1526–1533. [Google Scholar] [CrossRef]
- VandeVord, P.J.; Matthew, H.W.T.; DeSilva, S.P.; Mayton, L.; Wu, B.; Wooley, P.H. Evaluation of the Biocompatibility of a Chitosan Scaffold in Mice. J. Biomed. Mater. Res. 2002, 59, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Nitti, P.; Palazzo, B.; Gallo, N.; Scalera, F.; Sannino, A.; Gervaso, F. Smooth-rough Asymmetric PLGA Structure Made of Dip Coating Membrane and Electrospun Nanofibrous Scaffolds Meant to Be Used for Guided Tissue Regeneration of Periodontium. Polym. Eng. Sci. 2022, 62, 2061–2069. [Google Scholar] [CrossRef]
- Zhang, X.; Williams, D. Definitions of Biomaterials for the Twenty-First Century; Elsevier: Amsterdam, The Netherlands, 2019; ISBN 0-12-818292-X. [Google Scholar]
- Cao, D.; Ding, J. Recent Advances in Regenerative Biomaterials. Regen. Biomater. 2022, 9, rbac098. [Google Scholar] [CrossRef] [PubMed]
- Xianmiao, C.; Yubao, L.; Yi, Z.; Li, Z.; Jidong, L.; Huanan, W. Properties and in Vitro Biological Evaluation of Nano-Hydroxyapatite/Chitosan Membranes for Bone Guided Regeneration. Mater. Sci. Eng. C 2009, 29, 29–35. [Google Scholar] [CrossRef]
- Lim, G.; Lin, G.-H.; Monje, A.; Chan, H.-L.; Wang, H.-L. Wound Healing Complications Following Guided Bone Regeneration for Ridge Augmentation: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implants 2018, 33, 50–51. [Google Scholar] [CrossRef] [PubMed]
- Denchai, A.; Tartarini, D.; Mele, E. Cellular Response to Surface Morphology: Electrospinning and Computational Modeling. Front. Bioeng. Biotechnol. 2018, 6, 155. [Google Scholar] [CrossRef]
- Martins, A.; Reis, R.L.; Neves, N.M. Electrospinning: Processing Technique for Tissue Engineering Scaffolding. Int. Mater. Rev. 2008, 53, 257–274. [Google Scholar] [CrossRef]
- Hong, J.; Yeo, M.; Yang, G.H.; Kim, G. Cell-Electrospinning and Its Application for Tissue Engineering. IJMS 2019, 20, 6208. [Google Scholar] [CrossRef]
- Barnes, C.P.; Sell, S.A.; Boland, E.D.; Simpson, D.G.; Bowlin, G.L. Nanofiber Technology: Designing the next Generation of Tissue Engineering Scaffolds. Adv. Drug Deliv. Rev. 2007, 59, 1413–1433. [Google Scholar] [CrossRef]
- Zulkifli, M.Z.A.; Nordin, D.; Shaari, N.; Kamarudin, S.K. Overview of Electrospinning for Tissue Engineering Applications. Polymers 2023, 15, 2418. [Google Scholar] [CrossRef]
- Haider, A.; Haider, S.; Kang, I.-K. A Comprehensive Review Summarizing the Effect of Electrospinning Parameters and Potential Applications of Nanofibers in Biomedical and Biotechnology. Arab. J. Chem. 2018, 11, 1165–1188. [Google Scholar] [CrossRef]
- Ma, Z.; He, W.; Yong, T.; Ramakrishna, S. Grafting of Gelatin on Electrospun Poly(Caprolactone) Nanofibers to Improve Endothelial Cell Spreading and Proliferation and to Control Cell Orientation. Tissue Eng. 2005, 11, 1149–1158. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Li, C.; Zhao, Y.; Hu, J.; Zhang, L.-M. Co-Electrospun Nanofibrous Membranes of Collagen and Zein for Wound Healing. ACS Appl. Mater. Interfaces 2012, 4, 1050–1057. [Google Scholar] [CrossRef] [PubMed]
- Humaira; Raza Bukhari, S.A.; Shakir, H.A.; Khan, M.; Saeed, S.; Ahmad, I.; Muzammil, K.; Franco, M.; Irfan, M.; Li, K. Hyaluronic Acid-Based Nanofibers: Electrospun Synthesis and Their Medical Applications; Recent Developments and Future Perspective. Front. Chem. 2022, 10, 1092123. [Google Scholar] [CrossRef] [PubMed]
- Sarmento, B.; das Neves, J. Chitosan-Based Systems for Biopharmaceuticals: Delivery, Targeting and Polymer Therapeutics; John Wiley & Sons: Chichester, UK, 2012; pp. 10–14. [Google Scholar] [CrossRef]
- Khajavi, R.; Abbasipour, M.; Bahador, A. Electrospun Biodegradable Nanofibers Scaffolds for Bone Tissue Engineering. J. Appl. Polym. Sci. 2016, 133, app.42883. [Google Scholar] [CrossRef]
- Cipitria, A.; Skelton, A.; Dargaville, T.R.; Dalton, P.D.; Hutmacher, D.W. Design, Fabrication and Characterization of PCL Electrospun Scaffolds—A Review. J. Mater. Chem. 2011, 21, 9419. [Google Scholar] [CrossRef]
- Gentile, P.; Chiono, V.; Carmagnola, I.; Hatton, P. An Overview of Poly(Lactic-Co-Glycolic) Acid (PLGA)-Based Biomaterials for Bone Tissue Engineering. IJMS 2014, 15, 3640–3659. [Google Scholar] [CrossRef] [PubMed]
- Casalini, T.; Rossi, F.; Castrovinci, A.; Perale, G. A Perspective on Polylactic Acid-Based Polymers Use for Nanoparticles Synthesis and Applications. Front. Bioeng. Biotechnol. 2019, 7, 259. [Google Scholar] [CrossRef]
- Park, J.-C.; Ito, T.; Kim, K.-O.; Kim, K.-W.; Kim, B.-S.; Khil, M.-S.; Kim, H.-Y.; Kim, I.-S. Electrospun Poly(Vinyl Alcohol) Nanofibers: Effects of Degree of Hydrolysis and Enhanced Water Stability. Polym. J. 2010, 42, 273–276. [Google Scholar] [CrossRef]
- Sam, G. Evolution of Barrier Membranes in Periodontal Regeneration-“Are the Third Generation Membranes Really Here?”. JCDR 2014, 8, ZE14. [Google Scholar] [CrossRef]
- Malam, Y.; Loizidou, M.; Seifalian, A.M. Liposomes and Nanoparticles: Nanosized Vehicles for Drug Delivery in Cancer. Trends Pharmacol. Sci. 2009, 30, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.H.; Lin, C.-T.; Yu, Y.-H.; Chou, Y.-C.; Liu, S.-J.; Chan, E.-C. Dual Delivery of Active Antibactericidal Agents and Bone Morphogenetic Protein at Sustainable High Concentrations Using Biodegradable Sheath-Core-Structured Drug-Eluting Nanofibers. IJN 2016, 11, 3927–3937. [Google Scholar] [CrossRef] [PubMed]
- Janjic, M.; Pappa, F.; Karagkiozaki, V.; Gitas, C.; Ktenidis, K.; Logothetidis, S. Surface Modification of Endovascular Stents with Rosuvastatin and Heparin-Loaded Biodegradable Nanofibers by Electrospinning. IJN 2017, 12, 6343–6355. [Google Scholar] [CrossRef] [PubMed]
- McClellan, P.; Landis, W.J. Recent Applications of Coaxial and Emulsion Electrospinning Methods in the Field of Tissue Engineering. BioRes. Open Access 2016, 5, 212–227. [Google Scholar] [CrossRef] [PubMed]
- Nikmaram, N.; Roohinejad, S.; Hashemi, S.; Koubaa, M.; Barba, F.J.; Abbaspourrad, A.; Greiner, R. Emulsion-Based Systems for Fabrication of Electrospun Nanofibers: Food, Pharmaceutical and Biomedical Applications. RSC Adv. 2017, 7, 28951–28964. [Google Scholar] [CrossRef]
- McGowan, K.; McGowan, T.; Ivanovski, S. Optimal Dose and Duration of Amoxicillin-plus-metronidazole as an Adjunct to Non-surgical Periodontal Therapy: A Systematic Review and Meta-analysis of Randomized, Placebo-controlled Trials. J. Clinic. Periodontol. 2018, 45, 56–67. [Google Scholar] [CrossRef]
- Bonito, A.J.; Lux, L.; Lohr, K.N. Impact of Local Adjuncts to Scaling and Root Planing in Periodontal Disease Therapy: A Systematic Review. J. Periodontol. 2005, 76, 1227–1236. [Google Scholar] [CrossRef]
- Xue, J.; He, M.; Liang, Y.; Crawford, A.; Coates, P.; Chen, D.; Shi, R.; Zhang, L. Fabrication and Evaluation of Electrospun PCL–Gelatin Micro-/Nanofiber Membranes for Anti-Infective GTR Implants. J. Mater. Chem. B 2014, 2, 6867–6877. [Google Scholar] [CrossRef]
- Shi, R.; Ye, J.; Li, W.; Zhang, J.; Li, J.; Wu, C.; Xue, J.; Zhang, L. Infection-Responsive Electrospun Nanofiber Mat for Antibacterial Guided Tissue Regeneration Membrane. Mater. Sci. Eng. C 2019, 100, 523–534. [Google Scholar] [CrossRef]
- Lian, M.; Sun, B.; Qiao, Z.; Zhao, K.; Zhou, X.; Zhang, Q.; Zou, D.; He, C.; Zhang, X. Bi-Layered Electrospun Nanofibrous Membrane with Osteogenic and Antibacterial Properties for Guided Bone Regeneration. Colloids Surf. B Biointerfaces 2019, 176, 219–229. [Google Scholar] [CrossRef]
- Gomes, K.D.N.; Alves, A.P.N.N.; Dutra, P.G.P.; Viana, G.S.D.B. Doxycycline Induces Bone Repair and Changes in Wnt Signalling. Int. J. Oral Sci. 2017, 9, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Mathew, A.; Vaquette, C.; Hashimi, S.; Rathnayake, I.; Huygens, F.; Hutmacher, D.W.; Ivanovski, S. Antimicrobial and Immunomodulatory Surface-Functionalized Electrospun Membranes for Bone Regeneration. Adv. Healthcare Mater. 2017, 6, 1601345. [Google Scholar] [CrossRef] [PubMed]
- Graves, D.T.; Li, J.; Cochran, D.L. Inflammation and Uncoupling as Mechanisms of Periodontal Bone Loss. J. Dent. Res. 2011, 90, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Y.; Lin, K.; Yu, H. Advance of Nano-Composite Electrospun Fibers in Periodontal Regeneration. Front. Chem. 2019, 7, 495. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.; Fok, M.R.; Zhang, Y.; Han, B.; Lin, Y. The Role of Non-Steroidal Anti-Inflammatory Drugs as Adjuncts to Periodontal Treatment and in Periodontal Regeneration. J. Transl. Med. 2023, 21, 149. [Google Scholar] [CrossRef] [PubMed]
- Golub, L.M.; Lee, H. Periodontal Therapeutics: Current Host-modulation Agents and Future Directions. Periodontology 2000 2020, 82, 186–204. [Google Scholar] [CrossRef] [PubMed]
- Dereka, X.E.; Markopoulou, C.E.; Vrotsos, I.A. Role of Growth Factors on Periodontal Repair. Growth Factors 2006, 24, 260–267. [Google Scholar] [CrossRef]
- Tsai, S.-W.; Hsu, Y.-W.; Pan, W.-L.; Hsu, F.-Y. The Effect of Strontium-Substituted Hydroxyapatite Nanofibrous Matrix on Osteoblast Proliferation and Differentiation. Membranes 2021, 11, 624. [Google Scholar] [CrossRef]
- Muthukuru, M.; Sun, J. Doxycycline Counteracts Bone Morphogenic Protein 2–Induced Osteogenic Mediators. J. Periodontol. 2013, 84, 656–665. [Google Scholar] [CrossRef]
- Gantenbein, B.; Tang, S.; Guerrero, J.; Higuita-Castro, N.; Salazar-Puerta, A.I.; Croft, A.S.; Gazdhar, A.; Purmessur, D. Non-Viral Gene Delivery Methods for Bone and Joints. Front. Bioeng. Biotechnol. 2020, 8, 598466. [Google Scholar] [CrossRef]
- Zu, H.; Gao, D. Non-Viral Vectors in Gene Therapy: Recent Development, Challenges, and Prospects. AAPS J. 2021, 23, 78. [Google Scholar] [CrossRef] [PubMed]
- Shido, R.; Sumita, Y.; Hara, M.; Iwatake, M.; Narahara, S.; Umebayashi, M.; Miura, K.; Kodama, Y.; Asahina, I. Gene-Activated Matrix Harboring a miR20a-Expressing Plasmid Promotes Rat Cranial Bone Augmentation. Regen. Biomater. 2021, 8, rbaa060. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Ding, Z.; Xia, S.; Liu, Y.; Lei, S.; Zhong, M.; Chen, X. Poly Lactic-co-glycolic Acid Scaffold Loaded with Plasmid DNA Encoding Fibroblast Growth Factor-2 Promotes Periodontal Ligament Regeneration of Replanted Teeth. J. Periodontal Res. 2020, 55, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Xie, Q.; Jia, L.; Xu, H.; Hu, X.; Wang, W.; Jia, J. Fabrication of Core-Shell PEI/pBMP2-PLGA Electrospun Scaffold for Gene Delivery to Periodontal Ligament Stem Cells. Stem Cells Int. 2016, 2016, 5385137. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.; Zhou, Y.; Zheng, K.; Xu, X.; Yang, J.; Wang, X.; Miao, L.; Wei, H.; Xu, Y. Cerium Oxide Nanoparticles Loaded Nanofibrous Membranes Promote Bone Regeneration for Periodontal Tissue Engineering. Bioact. Mater. 2022, 7, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Zong, C.; Bronckaers, A.; Willems, G.; He, H.; Cadenas De Llano-Pérula, M. Nanomaterials for Periodontal Tissue Regeneration: Progress, Challenges and Future Perspectives. JFB 2023, 14, 290. [Google Scholar] [CrossRef]
- Kavasi, R.-M.; Coelho, C.C.; Platania, V.; Quadros, P.A.; Chatzinikolaidou, M. In Vitro Biocompatibility Assessment of Nano-Hydroxyapatite. Nanomaterials 2021, 11, 1152. [Google Scholar] [CrossRef]
- Motta, C.; Cavagnetto, D.; Amoroso, F.; Baldi, I.; Mussano, F. Bioactive Glass for Periodontal Regeneration: A Systematic Review. BMC Oral Health 2023, 23, 264. [Google Scholar] [CrossRef]
- Sirelkhatim, A.; Mahmud, S.; Seeni, A.; Kaus, N.H.M.; Ann, L.C.; Bakhori, S.K.M.; Hasan, H.; Mohamad, D. Review on Zinc Oxide Nanoparticles: Antibacterial Activity and Toxicity Mechanism. Nano-Micro Lett. 2015, 7, 219–242. [Google Scholar] [CrossRef]
- Singh, P.; Ahn, S.; Kang, J.-P.; Veronika, S.; Huo, Y.; Singh, H.; Chokkaligam, M.; El-Agamy Farh, M.; Aceituno, V.C.; Kim, Y.J.; et al. In Vitro Anti-Inflammatory Activity of Spherical Silver Nanoparticles and Monodisperse Hexagonal Gold Nanoparticles by Fruit Extract of Prunus Serrulata: A Green Synthetic Approach. Artif. Cells Nanomed. Biotechnol. 2017, 46, 2022–2032. [Google Scholar] [CrossRef]
- Ni, C.; Zhou, J.; Kong, N.; Bian, T.; Zhang, Y.; Huang, X.; Xiao, Y.; Yang, W.; Yan, F. Gold Nanoparticles Modulate the Crosstalk between Macrophages and Periodontal Ligament Cells for Periodontitis Treatment. Biomaterials 2019, 206, 115–132. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Kong, N.; Zhang, Y.; Yang, W.; Yan, F. Size-Dependent Effects of Gold Nanoparticles on Osteogenic Differentiation of Human Periodontal Ligament Progenitor Cells. Theranostics 2017, 7, 1214–1224. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Jiang, H.; Wang, R.; Xie, Y.; Zhao, C. Fabrication of Metronidazole Loaded Poly (ε-Caprolactone)/Zein Core/Shell Nanofiber Membranes via Coaxial Electrospinning for Guided Tissue Regeneration. J. Colloid Interface Sci. 2017, 490, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Schkarpetkin, D.; Reise, M.; Wyrwa, R.; Völpel, A.; Berg, A.; Schweder, M.; Schnabelrauch, M.; Watts, D.C.; Sigusch, B.W. Development of Novel Electrospun Dual-Drug Fiber Mats Loaded with a Combination of Ampicillin and Metronidazole. Dent. Mater. 2016, 32, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Klymov, A.; Shao, J.; Zhang, Y.; Ji, W.; Kolwijck, E.; Jansen, J.A.; Leeuwenburgh, S.C.G.; Yang, F. Electrospun Nanofibrous Silk Fibroin Membranes Containing Gelatin Nanospheres for Controlled Delivery of Biomolecules. Adv Healthc. Mater. 2017, 6, 1700014. [Google Scholar] [CrossRef] [PubMed]
- Furtos, G.; Rivero, G.; Rapuntean, S.; Abraham, G.A. Amoxicillin-Loaded Electrospun Nanocomposite Membranes for Dental Applications: ELECTROSPUN NANOCOMPOSITE MATRICES. J. Biomed. Mater. Res. 2017, 105, 966–976. [Google Scholar] [CrossRef] [PubMed]
- Batool, F.; Morand, D.-N.; Thomas, L.; Bugueno, I.; Aragon, J.; Irusta, S.; Keller, L.; Benkirane-Jessel, N.; Tenenbaum, H.; Huck, O. Synthesis of a Novel Electrospun Polycaprolactone Scaffold Functionalized with Ibuprofen for Periodontal Regeneration: An In Vitro andIn Vivo Study. Materials 2018, 11, 580. [Google Scholar] [CrossRef]
- Ghavimi, M.A.; Bani Shahabadi, A.; Jarolmasjed, S.; Memar, M.Y.; Maleki Dizaj, S.; Sharifi, S. Nanofibrous Asymmetric Collagen/Curcumin Membrane Containing Aspirin-Loaded PLGA Nanoparticles for Guided Bone Regeneration. Sci. Rep. 2020, 10, 18200. [Google Scholar] [CrossRef]
- Higuchi, J.; Klimek, K.; Wojnarowicz, J.; Opalińska, A.; Chodara, A.; Szałaj, U.; Dąbrowska, S.; Fudala, D.; Ginalska, G. Electrospun Membrane Surface Modification by Sonocoating with HA and ZnO:Ag Nanoparticles—Characterization and Evaluation of Osteoblasts and Bacterial Cell Behavior In Vitro. Cells 2022, 11, 1582. [Google Scholar] [CrossRef]
- Dong, Y.; Yao, L.; Cai, L.; Jin, M.; Forouzanfar, T.; Wu, L.; Liu, J.; Wu, G. Antimicrobial and Pro-Osteogenic Coaxially Electrospun Magnesium Oxide Nanoparticles-Polycaprolactone /Parathyroid Hormone-Polycaprolactone Composite Barrier Membrane for Guided Bone Regeneration. IJN 2023, 18, 369–383. [Google Scholar] [CrossRef]
- Deng, Y.; Liang, Y.; Liu, X. Biomaterials for Periodontal Regeneration. Dent. Clin. N. Am. 2022, 66, 659–672. [Google Scholar] [CrossRef] [PubMed]
- Hua, W.; Xiang, J.; Wu, Y.; Yang, W.; Zhao, L. Growth Factor-Encapsulated Triphasic Scaffolds of Electrospun Polylactic Acid–Polycaprolactone (PLA–PCL) Nanofibrous Mats Combined with a Directionally Freeze-Dried Chitosan Hydrogel for Periodontal Tissue Regeneration. Mater. Adv. 2023, 4, 4798–4811. [Google Scholar] [CrossRef]
- Habanjar, O.; Diab-Assaf, M.; Caldefie-Chezet, F.; Delort, L. 3D Cell Culture Systems: Tumor Application, Advantages, and Disadvantages. IJMS 2021, 22, 12200. [Google Scholar] [CrossRef] [PubMed]
- Li, F.-C.; Kishen, A. 3D Organoids for Regenerative Endodontics. Biomolecules 2023, 13, 900. [Google Scholar] [CrossRef]
- Passos, P.C.; Moro, J.; Barcelos, R.C.S.; Da Rosa, H.Z.; Vey, L.T.; Bürguer, M.E.; Maciel, R.M.; Danesi, C.C.; Edwards, P.C.; Bottino, M.C.; et al. Nanofibrous Antibiotic-eluting Matrices: Biocompatibility Studies in a Rat Model. J. Biomed. Mater. Res. 2020, 108, 306–315. [Google Scholar] [CrossRef]
- Pajoumshariati, S.; Shirali, H.; Yavari, S.K.; Sheikholeslami, S.N.; Lotfi, G.; Mashhadi Abbas, F.; Abbaspourrad, A. GBR Membrane of Novel Poly (Butylene Succinate-Co-Glycolate) Co-Polyester Co-Polymer for Periodontal Application. Sci. Rep. 2018, 8, 7513. [Google Scholar] [CrossRef]
- Chen, C.-C.; Lee, S.-Y.; Teng, N.-C.; Hu, H.-T.; Huang, P.-C.; Yang, J.-C. In Vitro and In Vivo Studies of Hydrophilic Electrospun PLA95/β-TCP Membranes for Guided Tissue Regeneration (GTR) Applications. Nanomaterials 2019, 9, 599. [Google Scholar] [CrossRef]
- Wang, J.; Wang, L.; Zhou, Z.; Lai, H.; Xu, P.; Liao, L.; Wei, J. Biodegradable Polymer Membranes Applied in Guided Bone/Tissue Regeneration: A Review. Polymers 2016, 8, 115. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Polymers | Advantages | Drawbacks | Ref. |
|---|---|---|---|
| Naturals | |||
| Collagen | Excellent biocompatibility Promotion of cell adhesion | Poor mechanical properties Rapid degradation in vivo | [92] |
| Gelatin | Integrin-binding sites for cell adhesion Good biocompatibility Low immunogenicity Plasticity Low cost | Poor mechanical properties Fast degradation | [107] |
| Zein | Good electrospinnability Non-toxic character of its by-products Enhanced cell viability, proliferation, and attachment Suitable for drug delivery | May have immunogenic problem | [108] |
| HA | High water retention capacity Binding sites for cell adhesion | Inadequate mechanical properties High viscoelasticity High surface tension | [109] |
| Chitosan | Biocompatible Breakdown by lysozyme Antibacterial, antiplaque activities | Low biodegradation Poor mechanical properties | [93,94,95,110] 12 April 2023 9:58:00 a.m. |
| PCL | Good mechanical properties Suitable for drug delivery and TE Mechanical strength Biodegradability No acidic degradation products Promotion of osteogenic differentiation | Absence of functional groups, so low cell adhesion and proliferation Slow degradation rate and hydrophobicity | [111] 12 April 2023 9:58:00 a.m. |
| Synthetics | |||
| Poly (lactic-co-glycolic acid) (PLGA) | Biocompatible and biodegradable Optimal mechanical properties Manageability, flexibility Controllable degradability for GBR applications Suitable for drug delivery | Rapid releases of oligomers and acid by-products may cause significant inflammation reactions in vivo Intrinsically hydrophobic Not optimal for cell adhesion and proliferation | [112] 12 April 2023 9:58:00 a.m. |
| Polylactic acid (PLA) | Biocompatible Optimal mechanical strength Processability | Slow degradation kinetics Releases acidic degradation products that may induce inflammation Hydrophobicity | [113] |
| PVA | Water-soluble Absence of toxicity Good mechanical property | Poor cell adhesion High hydrophilicity | [114] |
| Compounds | Electrospun Polymers | Outcomes | Ref. |
|---|---|---|---|
| Antibiotics | |||
| MNZ | PCL/zein core/shell nanofibers | MNZ-loaded mats were produced by coaxial ES. The MNA was distributed homogeneously in the core layer of the fibers and incorporation of hydrophobic zein allowed to decrease the initial burst release and prolong drug release period. Notable efficiency against anaerobic bacteria. | [148] |
| Ampicillin/MNZ | Polylactide fibers | Strong in vitro suppression of oral pathogens such as A. actinomycetemcomitans, F. nucleatum, P. gingivalis was obtained thanks to a synergistic effect of the two drugs. | [149] |
| Vancomycin | Silk fibroin nanofibers | Negatively charged gelatin nanospheres (GNs) were used in combination with silk fibroin nanofibers, for vancomycin delivery. Biocompatibility and antibacterial effects against Staphylococcus aureus were confirmed. | [150] |
| Amoxicilline (AMX) | PCL nanofibers | Fibrous PCL nanocomposites membranes loaded with various nHAp and AMX contents, to induce possessing osteogenic and antimicrobial activity in vivo. | [151] |
| NSAIDs | |||
| Ibuprofen (IBU) | PCL nanofibers | The in vivo efficacy of the IBU-PCL membrane was assessed in an experimental periodontitis mouse model, revealing that the IBU-PCL membrane could efficiently and differentially control inflammatory and migratory gingival cell responses and potentially promote periodontal regeneration. | [152] |
| Aspirin + curcumin | The presence of curcumin and aspirin in the asymmetric membrane enhanced osteogenic potential of the membranes. The results of the animal test showed that the defected area was filled with new bone after 28 days. | [153] | |
| Nanostructure | |||
| Nano zinc oxide–silver biomaterial (nZnO:Ag) | Poly (D,L-lactic acid)(PLA)/poly(lactic-co-glycolic acid) (PLGA) fibers | Unique combination of HA, nZnO, and nAgs reduced cytotoxicity towards osteoblasts, enhanced the biological performance and antibacterial function of the fibers’ coating. | [154] |
| Magnesium oxide nanoparticles (MgONPs) | PCL | Dual-functional coaxially electrospun membranes by encapsulating parathyroid hormone (PTH) in the core layer and MgONPs in the shell layer were produced. In vivo and in vitro studies demonstrated that MgONPs incorporation has outstanding antibacterial potential, but also significantly prolonged the release of PTH. | [155] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Epicoco, L.; Pellegrino, R.; Madaghiele, M.; Friuli, M.; Giannotti, L.; Di Chiara Stanca, B.; Palermo, A.; Siculella, L.; Savkovic, V.; Demitri, C.; et al. Recent Advances in Functionalized Electrospun Membranes for Periodontal Regeneration. Pharmaceutics 2023, 15, 2725. https://doi.org/10.3390/pharmaceutics15122725
Epicoco L, Pellegrino R, Madaghiele M, Friuli M, Giannotti L, Di Chiara Stanca B, Palermo A, Siculella L, Savkovic V, Demitri C, et al. Recent Advances in Functionalized Electrospun Membranes for Periodontal Regeneration. Pharmaceutics. 2023; 15(12):2725. https://doi.org/10.3390/pharmaceutics15122725
Chicago/Turabian StyleEpicoco, Luana, Rebecca Pellegrino, Marta Madaghiele, Marco Friuli, Laura Giannotti, Benedetta Di Chiara Stanca, Andrea Palermo, Luisa Siculella, Vuk Savkovic, Christian Demitri, and et al. 2023. "Recent Advances in Functionalized Electrospun Membranes for Periodontal Regeneration" Pharmaceutics 15, no. 12: 2725. https://doi.org/10.3390/pharmaceutics15122725