
Aerogels as Carriers for Oral Administration of Drugs: An Approach towards Colonic Delivery


Abstract
:1. Introduction
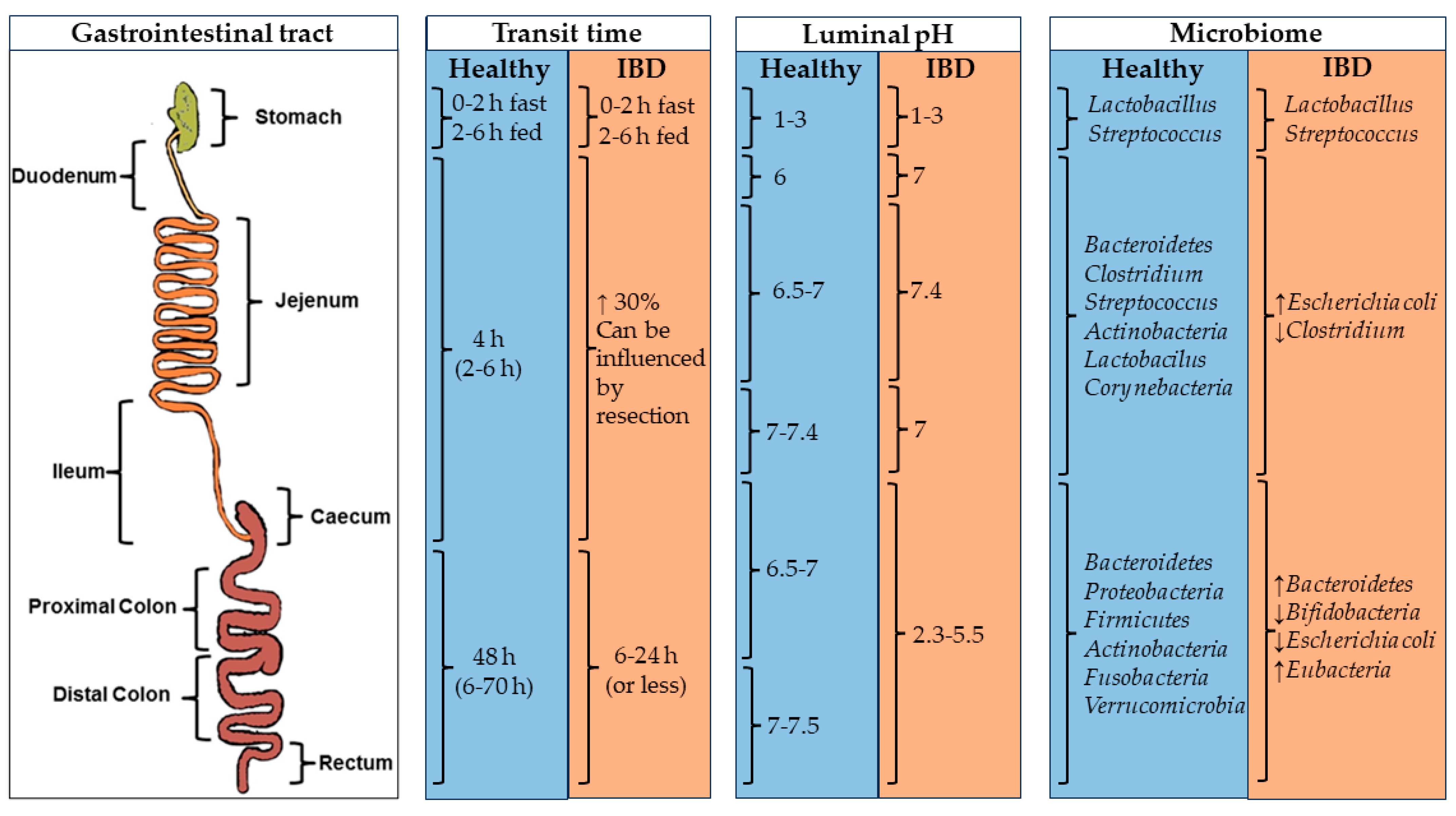
2. Gastrointestinal Conditions: An Overview and Essential Considerations

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Nutrient (Substrate) | Enzyme | Section of GIT | References |
|---|---|---|---|
| Polysaccharides and oligosaccharides | α-amylase (lingual and pancreatic) | Oral cavity and duodenum | [3] |
| Oligosaccharidases | Small intestine | [3] | |
| β-D-galactosidases | Colon | [33] | |
| β-D-xilosidases | Colon | [33] | |
| α-L-arabinofuranosidase | Colon | [33] | |
| Lipids | Lipase (lingual, gastric and pancreatic) | Oral cavity, stomach, duodenum | [3,34] |
| Colipase | Duodenum | [3,34,35] | |
| Proteins and aminoacids | Pepsin (pepsinogen) | Stomach | [35] |
| Enteropeptidases | Small intestine | [3,34] | |
| Trypsin (trypsinogen) | Duodenum | [34,35] | |
| Chymotrypsin | Duodenum | [34,35] | |
| Elastase | Duodenum | [34,35] | |
| Carboxypeptidases (A and B) | Duodenum | [34,35] | |
| Other | Azoreductases | Colon | [33] |
| Nitroreductases | Colon | [33] |
3. Polysaccharides as Carriers for Colonic Delivery
3.1. Alginate (Alg)
3.2. Chitosan (CS)
3.3. Pectin
3.4. Cellulose
3.5. Starch
3.6. Konjac Glucomannan (KGM)
3.7. Other Polysaccharides
4. Polysaccharide-Based Aerogels as Dry Carriers for Colonic Delivery
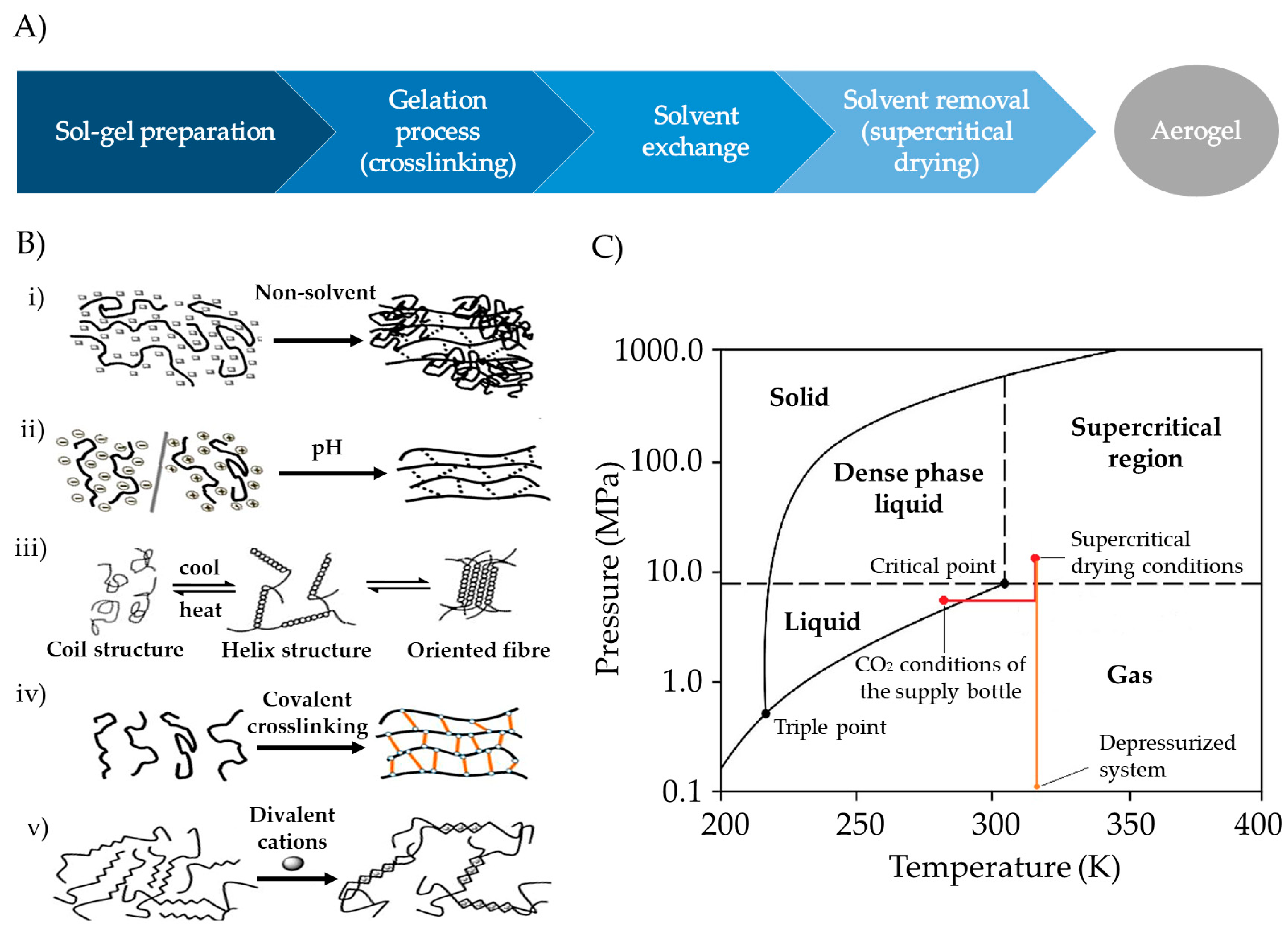
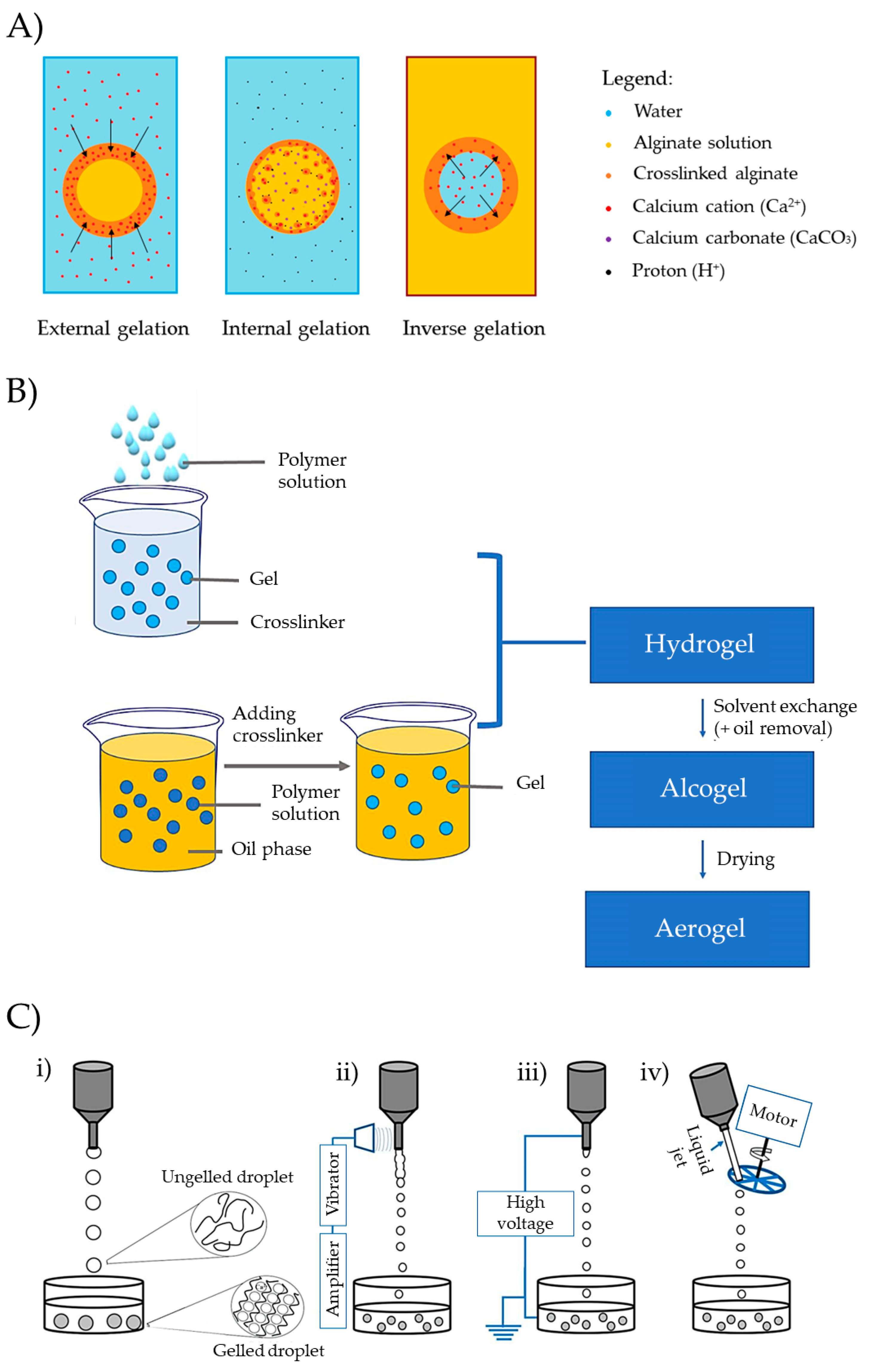
4.1. Polysaccharide-Based Aerogel Preparation

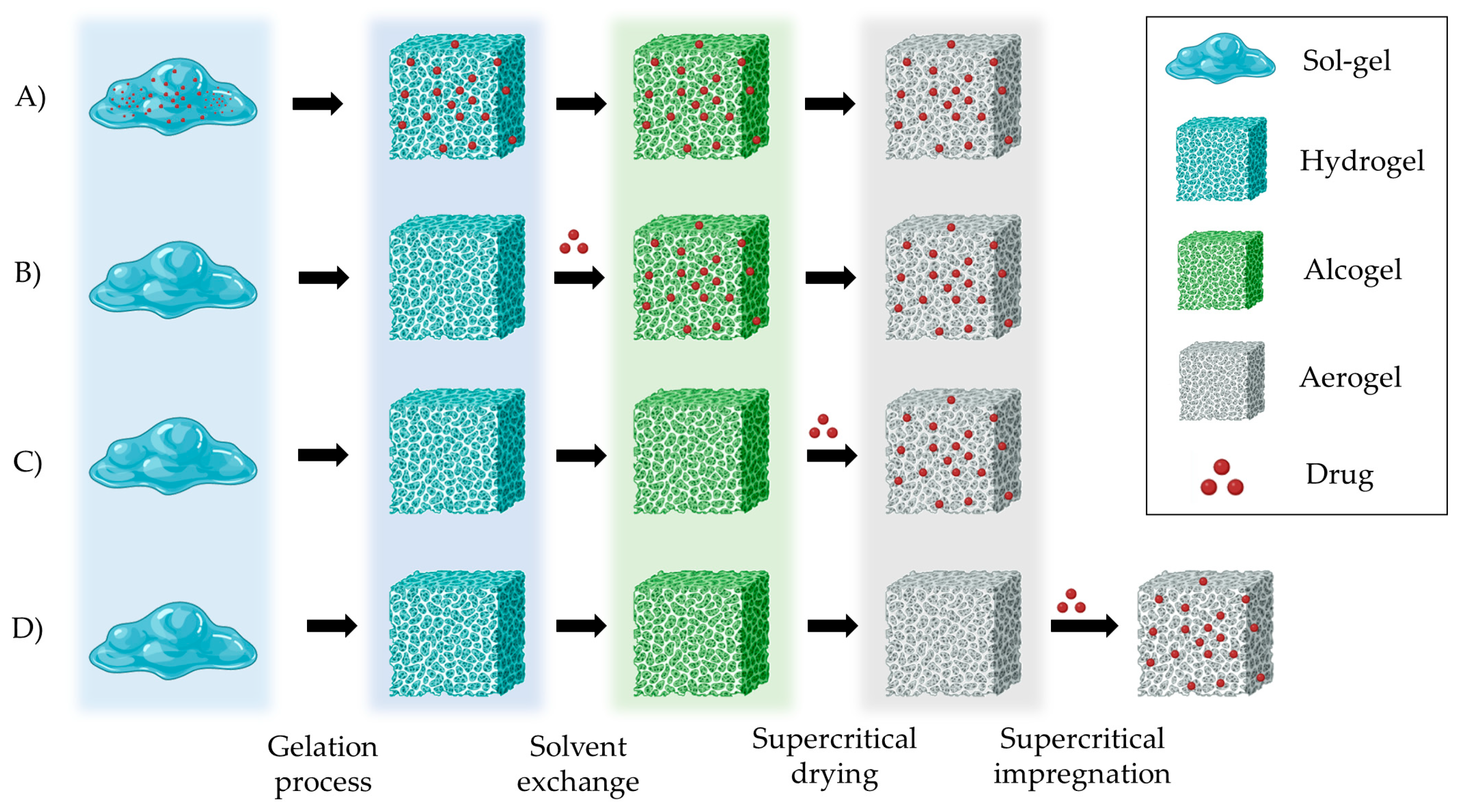
4.2. Drug Loading within Aerogels Impregnation Technique
4.3. Polysaccharide-Based Aerogel Dosage Systems: Production and Release Properties
4.4. Coating of Polysaccharide-Based Aerogels for Colonic Applications
5. Future Trends in Research on Aerogels as Colonic Drug Delivery Systems
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Alqahtani, M.S.; Kazi, M.; Alsenaidy, M.A.; Ahmad, M.Z. Advances in Oral Drug Delivery. Front. Pharmacol. 2021, 12, 618411. [Google Scholar] [CrossRef]
- Sathish, D.; Himabindu, S.; Shravan Kumar, Y.; Shayeda; Madhusudan Rao, Y. Floating Drug Delivery Systems for Prolonging Gastric Residence Time: A Review. Curr. Drug Deliv. 2011, 8, 494–510. [Google Scholar] [CrossRef] [PubMed]
- Hua, S. Advances in Oral Drug Delivery for Regional Targeting in the Gastrointestinal Tract—Influence of Physiological, Pathophysiological and Pharmaceutical Factors. Front. Pharmacol. 2020, 11, 524. [Google Scholar] [CrossRef]
- Arévalo-Pérez, R.; Maderuelo, C.; Lanao, J.M. Recent Advances in Colon Drug Delivery Systems. J. Control. Release 2020, 327, 703–724. [Google Scholar] [CrossRef]
- Cai, Z.; Wang, S.; Li, J. Treatment of Inflammatory Bowel Disease: A Comprehensive Review. Front. Med. 2021, 8, 765474. [Google Scholar] [CrossRef]
- Amidon, S.; Brown, J.E.; Dave, V.S. Colon-Targeted Oral Drug Delivery Systems: Design Trends and Approaches. AAPS PharmSciTech 2015, 16, 731–741. [Google Scholar] [CrossRef] [PubMed]
- Basit, A.W. Advances in Colonic Drug Delivery. Drugs 2005, 65, 1991–2007. [Google Scholar] [CrossRef]
- Dening, T.J.; Amidon, G.E.; He, X.; Hageman, M.J. Physicochemical Characterization and Oral Dosage Form Design and Selection. In Burger’s Medicinal Chemistry and Drug Discovery; John Wiley & Sons: Hoboken, NJ, USA, 2021; pp. 1–49. ISBN 978-0-471-26694-5. [Google Scholar]
- Vinarov, Z.; Abdallah, M.; Agundez, J.A.G.; Allegaert, K.; Basit, A.W.; Braeckmans, M.; Ceulemans, J.; Corsetti, M.; Griffin, B.T.; Grimm, M.; et al. Impact of Gastrointestinal Tract Variability on Oral Drug Absorption and Pharmacokinetics: An UNGAP Review. Eur. J. Pharm. Sci. 2021, 162, 105812. [Google Scholar] [CrossRef] [PubMed]
- Sensoy, I. A Review on the Food Digestion in the Digestive Tract and the Used In Vitro Models. Curr. Res. Food Sci. 2021, 4, 308–319. [Google Scholar] [CrossRef]
- Vandamme, T.F.; Lenourry, A.; Charrueau, C.; Chaumeil, J.-C. The Use of Polysaccharides to Target Drugs to the Colon. Carbohydr. Polym. 2002, 48, 219–231. [Google Scholar] [CrossRef]
- Shah, N.; Shah, T.; Amin, A. Polysaccharides: A Targeting Strategy for Colonic Drug Delivery. Expert Opin. Drug Deliv. 2011, 8, 779–796. [Google Scholar] [CrossRef] [PubMed]
- Sinha, V.R.; Kumria, R. Polysaccharides in Colon-Specific Drug Delivery. Int. J. Pharm. 2001, 224, 19–38. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.; Colombo, G.; Sonvico, F. Pectin Matrix as Oral Drug Delivery Vehicle for Colon Cancer Treatment. AAPS PharmSciTech 2010, 12, 201–214. [Google Scholar] [CrossRef]
- Peppas, N.A.; Hilt, J.Z.; Khademhosseini, A.; Langer, R. Hydrogels in Biology and Medicine: From Molecular Principles to Bionanotechnology. Adv. Mater. 2006, 18, 1345–1360. [Google Scholar] [CrossRef]
- Paukkonen, H.; Kunnari, M.; Laurén, P.; Hakkarainen, T.; Auvinen, V.-V.; Oksanen, T.; Koivuniemi, R.; Yliperttula, M.; Laaksonen, T. Nanofibrillar Cellulose Hydrogels and Reconstructed Hydrogels as Matrices for Controlled Drug Release. Int. J. Pharm. 2017, 532, 269–280. [Google Scholar] [CrossRef]
- Auriemma, G.; Russo, P.; Del Gaudio, P.; García-González, C.A.; Landín, M.; Aquino, R.P. Technologies and Formulation Design of Polysaccharide-Based Hydrogels for Drug Delivery. Molecules 2020, 25, 3156. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Malfait, W.J.; Guerrero-Alburquerque, N.; Koebel, M.M.; Nyström, G. Biopolymer Aerogels and Foams: Chemistry, Properties, and Applications. Angew. Chem. Int. Ed. 2018, 57, 7580–7608. [Google Scholar] [CrossRef]
- Costa, J.S.R.; de Oliveira Cruvinel, K.; Oliveira-Nascimento, L. A Mini-Review on Drug Delivery through Wafer Technology: Formulation and Manufacturing of Buccal and Oral Lyophilizates. J. Adv. Res. 2019, 20, 33–41. [Google Scholar] [CrossRef]
- García-González, C.A.; Sosnik, A.; Kalmár, J.; De Marco, I.; Erkey, C.; Concheiro, A.; Alvarez-Lorenzo, C. Aerogels in Drug Delivery: From Design to Application. J. Control. Release 2021, 332, 40–63. [Google Scholar] [CrossRef]
- García-González, C.A.; Budtova, T.; Durães, L.; Erkey, C.; Del Gaudio, P.; Gurikov, P.; Koebel, M.; Liebner, F.; Neagu, M.; Smirnova, I. An Opinion Paper on Aerogels for Biomedical and Environmental Applications. Molecules 2019, 24, 1815. [Google Scholar] [CrossRef]
- García-González, C.A.; Jin, M.; Gerth, J.; Alvarez-Lorenzo, C.; Smirnova, I. Polysaccharide-Based Aerogel Microspheres for Oral Drug Delivery. Carbohydr. Polym. 2015, 117, 797–806. [Google Scholar] [CrossRef]
- Duong, T.; López-Iglesias, C.; Szewczyk, P.K.; Stachewicz, U.; Barros, J.; Alvarez-Lorenzo, C.; Alnaief, M.; García-González, C.A. A Pathway From Porous Particle Technology Toward Tailoring Aerogels for Pulmonary Drug Administration. Front. Bioeng. Biotechnol. 2021, 9, 671381. [Google Scholar] [CrossRef]
- López-Iglesias, C.; Barros, J.; Ardao, I.; Monteiro, F.J.; Alvarez-Lorenzo, C.; Gómez-Amoza, J.L.; García-González, C.A. Vancomycin-Loaded Chitosan Aerogel Particles for Chronic Wound Applications. Carbohydr. Polym. 2019, 204, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Maleki, H.; Durães, L.; García-González, C.A.; del Gaudio, P.; Portugal, A.; Mahmoudi, M. Synthesis and Biomedical Applications of Aerogels: Possibilities and Challenges. Adv. Colloid Interface Sci. 2016, 236, 1–27. [Google Scholar] [CrossRef]
- Wang, X.; Wang, J.; Feng, S.; Zhang, Z.; Wu, C.; Zhang, X.; Kang, F. Nano-Porous Silica Aerogels as Promising Biomaterials for Oral Drug Delivery of Paclitaxel. J. Biomed. Nanotechnol. 2019, 15, 1532–1545. [Google Scholar] [CrossRef]
- Wang, J.; Yadav, V.; Smart, A.L.; Tajiri, S.; Basit, A.W. Stability of Peptide Drugs in the Colon. Eur. J. Pharm. Sci. 2015, 78, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Yadav, V.; Smart, A.L.; Tajiri, S.; Basit, A.W. Toward Oral Delivery of Biopharmaceuticals: An Assessment of the Gastrointestinal Stability of 17 Peptide Drugs. Mol. Pharm. 2015, 12, 966–973. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, V.; Arduino, I.; Vacca, M.; Iacobazzi, R.M.; Altamura, D.; Lopalco, A.; Rizzi, R.; Cutrignelli, A.; Laquintana, V.; Massimo, F.; et al. Colonic Budesonide Delivery by Multistimuli Alginate/Eudragit® FS 30D/Inulin-Based Microspheres as a Paediatric Formulation. Carbohydr. Polym. 2023, 302, 120422. [Google Scholar] [CrossRef] [PubMed]
- Mudie, D.M.; Amidon, G.L.; Amidon, G.E. Physiological Parameters for Oral Delivery and In Vitro Testing. Mol. Pharm. 2010, 7, 1388–1405. [Google Scholar] [CrossRef]
- Hua, S.; Marks, E.; Schneider, J.J.; Keely, S. Advances in Oral Nano-Delivery Systems for Colon Targeted Drug Delivery in Inflammatory Bowel Disease: Selective Targeting to Diseased versus Healthy Tissue. Nanomed. Nanotechnol. Biol. Med. 2015, 11, 1117–1132. [Google Scholar] [CrossRef]
- Anil, K.; Philip, B.P. Colon Targeted Drug Delivery Systems: A Review on Primary and Novel Approaches. Oman Med. J. 2010, 25, 19–87. [Google Scholar] [CrossRef]
- Sinha, V.R.; Kumria, R. Colonic Drug Delivery: Prodrug Approach. Pharm. Res. 2001, 18, 557–564. [Google Scholar] [CrossRef]
- Minekus, M.; Alminger, M.; Alvito, P.; Ballance, S.; Bohn, T.; Bourlieu, C.; Carrière, F.; Boutrou, R.; Corredig, M.; Dupont, D.; et al. A Standardised Static In Vitro Digestion Method Suitable for Food—An International Consensus. Food Funct. 2014, 5, 1113–1124. [Google Scholar] [CrossRef] [PubMed]
- Brodkorb, A.; Egger, L.; Alminger, M.; Alvito, P.; Assunção, R.; Ballance, S.; Bohn, T.; Bourlieu-Lacanal, C.; Boutrou, R.; Carrière, F.; et al. INFOGEST Static In Vitro Simulation of Gastrointestinal Food Digestion. Nat. Protoc. 2019, 14, 991–1014. [Google Scholar] [CrossRef]
- Klünemann, M.; Andrejev, S.; Blasche, S.; Mateus, A.; Phapale, P.; Devendran, S.; Vappiani, J.; Simon, B.; Scott, T.A.; Kafkia, E.; et al. Bioaccumulation of Therapeutic Drugs by Human Gut Bacteria. Nature 2021, 597, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Freedberg, D.E.; Lebwohl, B.; Abrams, J.A. The Impact of Proton Pump Inhibitors on the Human Gastrointestinal Microbiome. Hum. Microbiome 2014, 34, 771–785. [Google Scholar] [CrossRef]
- Hold, G.L.; Hansen, R. Impact of the Gastrointestinal Microbiome in Health and Disease: Co-Evolution with the Host Immune System. In Molecular Mechanisms of Inflammation: Induction, Resolution and Escape by Helicobacter pylori; Backert, S., Ed.; Springer International Publishing: Cham, Switzerland, 2019; pp. 303–318. ISBN 978-3-030-15138-6. [Google Scholar]
- Halfvarson, J.; Brislawn, C.J.; Lamendella, R.; Vázquez-Baeza, Y.; Walters, W.A.; Bramer, L.M.; D’Amato, M.; Bonfiglio, F.; McDonald, D.; Gonzalez, A.; et al. Dynamics of the Human Gut Microbiome in Inflammatory Bowel Disease. Nat. Microbiol. 2017, 2, 17004. [Google Scholar] [CrossRef] [PubMed]
- Lubomski, M.; Tan, A.H.; Lim, S.-Y.; Holmes, A.J.; Davis, R.L.; Sue, C.M. Parkinson’s Disease and the Gastrointestinal Microbiome. J. Neurol. 2020, 267, 2507–2523. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-Y.; Qin, H.-Y.; Li, T.-T. Advances in the Study of the Relationship between Alzheimer’s Disease and the Gastrointestinal Microbiome. Ibrain 2022, 8, 465–475. [Google Scholar] [CrossRef]
- Ruan, W.; Engevik, M.A.; Spinler, J.K.; Versalovic, J. Healthy Human Gastrointestinal Microbiome: Composition and Function after a Decade of Exploration. Dig. Dis. Sci. 2020, 65, 695–705. [Google Scholar] [CrossRef] [PubMed]
- Nardone, G.; Compare, D. The Human Gastric Microbiota: Is It Time to Rethink the Pathogenesis of Stomach Diseases? United Eur. Gastroenterol. J. 2015, 3, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Sender, R.; Fuchs, S.; Milo, R. Revised Estimates for the Number of Human and Bacteria Cells in the Body. PLoS Biol. 2016, 14, e1002533. [Google Scholar] [CrossRef] [PubMed]
- Scheppach, W. Effects of Short Chain Fatty Acids on Gut Morphology and Function. Gut 1994, 35, 35–38. [Google Scholar] [CrossRef]
- Rasmussen, H.S.; Holtug, K.; Mortensen, P.B. Degradation of Amino Acids to Short-Chain Fatty Acids in Humans: An In Vitro Study. Scand. J. Gastroenterol. 1988, 23, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Awad, A.; Madla, C.M.; McCoubrey, L.E.; Ferraro, F.; Gavins, F.K.H.; Buanz, A.; Gaisford, S.; Orlu, M.; Siepmann, F.; Siepmann, J.; et al. Clinical Translation of Advanced Colonic Drug Delivery Technologies. Adv. Drug Deliv. Rev. 2022, 181, 114076. [Google Scholar] [CrossRef]
- Cockburn, D.W.; Koropatkin, N.M. Polysaccharide Degradation by the Intestinal Microbiota and Its Influence on Human Health and Disease. J. Mol. Biol. (JMB) 2016, 428, 3230–3252. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Ha, W.; Gao, K.; Shi, Y. Precisely Traceable Drug Delivery of Azoreductase-Responsive Prodrug for Colon Targeting via Multimodal Imaging. Anal. Chem. 2020, 92, 9039–9047. [Google Scholar] [CrossRef] [PubMed]
- Schiller, C.; Fröglich, C.P.; Giessmann, T.; Siegmund, W.; Mönnikes, H.; Hosten, N.; Weitschies, W. Intestinal Fluid Volumes and Transit of Dosage Forms as Assessed by Magnetic Resonance Imaging. Aliment. Pharmacol. Ther. 2005, 22, 971–979. [Google Scholar] [CrossRef]
- Mudie, D.M.; Murray, K.; Hoad, C.L.; Pritchard, S.E.; Garnett, M.C.; Amidon, G.L.; Gowland, P.A.; Spiller, R.C.; Amidon, G.E.; Marciani, L. Quantification of Gastrointestinal Liquid Volumes and Distribution Following a 240 mL Dose of Water in the Fasted State. Mol. Pharm. 2014, 11, 3039–3047. [Google Scholar] [CrossRef]
- Thakral, S.; Thakral, N.K.; Majumdar, D.K. Eudragit®: A Technology Evaluation. Expert Opin. Drug Deliv. 2013, 10, 131–149. [Google Scholar] [CrossRef]
- Fülöpová, N.; Pavloková, S.; DeBono, I.; Vetchý, D.; Franc, A. Development and Comparison of Various Coated Hard Capsules Suitable for Enteric Administration to Small Patient Cohorts. Pharmaceutics 2022, 14, 1577. [Google Scholar] [CrossRef]
- Xu, W.; Gao, Q.; Xu, Y.; Wu, D.; Sun, Y. pH-Controlled Drug Release from Mesoporous Silica Tablets Coated with Hydroxypropyl Methylcellulose Phthalate. Mater. Res. Bull. 2009, 44, 606–612. [Google Scholar] [CrossRef]
- Kumar, S.; Jeet, K.; Baldi, A. Recent Technological Advancements in Multiparticulate Formulations: The Smart Drug Delivery Systems. Asian J. Pharm. 2015, 9, S13–S25. [Google Scholar]
- Yang, Y.; Aloysius, H.; Inoyama, D.; Chen, Y.; Hu, L. Enzyme-Mediated Hydrolytic Activation of Prodrugs. Acta Pharm. Sin. B 2011, 1, 143–159. [Google Scholar] [CrossRef]
- Markovic, M.; Ben-Shabat, S.; Dahan, A. Prodrugs for Improved Drug Delivery: Lessons Learned from Recently Developed and Marketed Products. Pharmaceutics 2020, 12, 1031. [Google Scholar] [CrossRef]
- Mohammed, A.S.A.; Naveed, M.; Jost, N. Polysaccharides; Classification, Chemical Properties, and Future Perspective Applications in Fields of Pharmacology and Biological Medicine (A Review of Current Applications and Upcoming Potentialities). J. Polym. Environ. 2021, 29, 2359–2371. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Lorenzo, C.; Blanco-Fernandez, B.; Puga, A.M.; Concheiro, A. Crosslinked Ionic Polysaccharides for Stimuli-Sensitive Drug Delivery. Adv. Drug Deliv. Rev. 2013, 65, 1148–1171. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Rodriguez, P.; Garcia-Triñanes, P.; Echezarreta López, M.M.; Santoveña, A.; Landin, M. Mineralized Alginate Hydrogels Using Marine Carbonates for Bone Tissue Engineering Applications. Carbohydr. Polym. 2018, 195, 235–242. [Google Scholar] [CrossRef]
- Kou, S.; Peters, L.M.; Mucalo, M.R. Chitosan: A Review of Sources and Preparation Methods. Int. J. Biol. Macromol. 2021, 169, 85–94. [Google Scholar] [CrossRef]
- Seddiqi, H.; Oliaei, E.; Honarkar, H.; Jin, J.; Geonzon, L.C.; Bacabac, R.G.; Klein-Nulend, J. Cellulose and Its Derivatives: Towards Biomedical Applications. Cellulose 2021, 28, 1893–1931. [Google Scholar] [CrossRef]
- Tagliapietra, B.L.; Felisberto, M.H.F.; Sanches, E.A.; Campelo, P.H.; Clerici, M.T.P.S. Non-Conventional Starch Sources. Curr. Opin. Food Sci. 2021, 39, 93–102. [Google Scholar] [CrossRef]
- Apriyanto, A.; Compart, J.; Fettke, J. A Review of Starch, a Unique Biopolymer—Structure, Metabolism and in Planta Modifications. Plant Sci. 2022, 318, 111223. [Google Scholar] [CrossRef] [PubMed]
- Salimi, M.; Channab, B.-E.; Ayoub, E.I.; Zahouily, M.; Motamedi, E. A Comprehensive Review on Starch: Structure, Modification, and Applications in Slow/Controlled-Release Fertilizers in Agriculture. Carbohydr. Polym. 2023, 322, 121326. [Google Scholar] [CrossRef] [PubMed]
- Devaraj, R.D.; Reddy, C.K.; Xu, B. Health-Promoting Effects of Konjac Glucomannan and Its Practical Applications: A Critical Review. Int. J. Biol. Macromol. 2019, 126, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Manceñido, F.; Braeckmans, K.; De Smedt, S.C.; Demeester, J.; Landin, M.; Martínez-Pacheco, R. Characterization of Diffusion of Macromolecules in Konjac Glucomannan Solutions and Gels by Fluorescence Recovery after Photobleaching Technique. Int. J. Pharm. 2006, 316, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; He, P.; Lin, X. The Mechanism of Sodium Hydroxide Solution Promoting the Gelation of Konjac Glucomannan (KGM). Food Hydrocoll. 2013, 30, 92–99. [Google Scholar] [CrossRef]
- Khoobbakht, F.; Khorshidi, S.; Bahmanyar, F.; Hosseini, S.M.; Aminikhah, N.; Farhoodi, M.; Mirmoghtadaie, L. Modification of Mechanical, Rheological and Structural Properties of Agar Hydrogel Using Xanthan and Locust Bean Gum. Food Hydrocoll. 2024, 147, 109411. [Google Scholar] [CrossRef]
- Bixler, H.J.; Porse, H. A Decade of Change in the Seaweed Hydrocolloids Industry. J. Appl. Phycol. 2011, 23, 321–335. [Google Scholar] [CrossRef]
- Mandal, S.; Hwang, S.; Shi, S.Q. Guar Gum, a Low-Cost Sustainable Biopolymer, for Wastewater Treatment: A Review. Int. J. Biol. Macromol. 2023, 226, 368–382. [Google Scholar] [CrossRef]
- Barak, S.; Mudgil, D. Locust Bean Gum: Processing, Properties and Food Applications—A Review. Int. J. Biol. Macromol. 2014, 66, 74–80. [Google Scholar] [CrossRef]
- Raghav, S.; Jain, P.; Kumar, D. Alginates: Properties and Applications. In Polysaccharides; Scrivener Publishing: Beverly, MA, USA, 2021; pp. 399–422. ISBN 978-1-119-71141-4. [Google Scholar]
- Chawla, A.; Sharma, P.; Pawar, P. Eudragit S-100 Coated Sodium Alginate Microspheres of Naproxen Sodium: Formulation, Optimization and In Vitro Evaluation. Acta Pharm. 2013, 62, 529–545. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, T.; Narayana, S.N.G.H.; Pal, K.; Pramanik, K.; Giri, S.; Banerjee, I. Calcium Alginate-Carboxymethyl Cellulose Beads for Colon-Targeted Drug Delivery. Int. J. Biol. Macromol. 2015, 75, 409–417. [Google Scholar] [CrossRef]
- Guastaferro, M.; Reverchon, E.; Baldino, L. Agarose, Alginate and Chitosan Nanostructured Aerogels for Pharmaceutical Applications: A Short Review. Front. Bioeng. Biotechnol. 2021, 9, 688477. [Google Scholar] [CrossRef] [PubMed]
- Gulbake, A.; Jain, S.K. Chitosan: A Potential Polymer for Colon-Specific Drug Delivery System. Expert Opin. Drug Deliv. 2012, 9, 713–729. [Google Scholar] [CrossRef]
- Schipper, N.G.M.; Vårum, K.M.; Stenberg, P.; Ocklind, G.; Lennernäs, H.; Artursson, P. Chitosans as Absorption Enhancers of Poorly Absorbable Drugs: 3: Influence of Mucus on Absorption Enhancement. Eur. J. Pharm. Sci. 1999, 8, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Artursson, P.; Lindmark, T.; Davis, S.S.; Illum, L. Effect of Chitosan on the Permeability of Monolayers of Intestinal Epithelial Cells (Caco-2). Pharm. Res. 1994, 11, 1358–1361. [Google Scholar] [CrossRef]
- Samprasit, W.; Opanasopit, P.; Chamsai, B. Mucoadhesive Chitosan and Thiolated Chitosan Nanoparticles Containing Alpha Mangostin for Possible Colon-Targeted Delivery. Pharm. Dev. Technol. 2021, 26, 362–372. [Google Scholar] [CrossRef]
- Veronovski, A.; Tkalec, G.; Knez, Ž.; Novak, Z. Characterisation of Biodegradable Pectin Aerogels and Their Potential Use as Drug Carriers. Carbohydr. Polym. 2014, 113, 272–278. [Google Scholar] [CrossRef]
- Auriemma, G.; Cerciello, A.; Aquino, R.P.; Del Gaudio, P.; Fusco, B.M.; Russo, P. Pectin and Zinc Alginate: The Right Inner/Outer Polymer Combination for Core-Shell Drug Delivery Systems. Pharmaceutics 2020, 12, 87. [Google Scholar] [CrossRef]
- Günter, E.A.; Markov, P.A.; Melekhin, A.K.; Belozerov, V.S.; Martinson, E.A.; Litvinets, S.G.; Popov, S.V. Preparation and Release Characteristics of Mesalazine Loaded Calcium Pectin-Silica Gel Beads Based on Callus Cultures Pectins for Colon-Targeted Drug Delivery. Int. J. Biol. Macromol. 2018, 120, 2225–2233. [Google Scholar] [CrossRef]
- Desai, N.; Momin, M. Colon Targeted Bioadhesive Pellets of Curcumin and Cyclosporine for Improved Management of Inflammatory Bowel Disease. Drug Deliv. Transl. Res. 2020, 10, 1288–1301. [Google Scholar] [CrossRef] [PubMed]
- Varum, F.; Freire, A.C.; Bravo, R.; Basit, A.W. OPTICORE™, an Innovative and Accurate Colonic Targeting Technology. Int. J. Pharm. 2020, 583, 119372. [Google Scholar] [CrossRef] [PubMed]
- Qin, Z.; Pang, Y.; Lu, C.; Yang, Y.; Gao, M.; Zheng, L.; Zhao, J. Photo-Crosslinkable Methacrylated Konjac Glucomannan (KGMMA) Hydrogels as a Promising Bioink for 3D Bioprinting. Biomater. Sci. 2022, 10, 6549–6557. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghazzewi, F.H.; Tester, R.F. Effect of Konjac Glucomannan Hydrolysates and Probiotics on the Growth of the Skin Bacterium Propionibacterium Acnes In Vitro. Int. J. Cosmet. Sci. 2010, 32, 139–142. [Google Scholar] [CrossRef]
- Wattanaprasert, S.; Borompichaichartkul, C.; Vaithanomsat, P.; Srzednicki, G. Konjac Glucomannan Hydrolysate: A Potential Natural Coating Material for Bioactive Compounds in Spray Drying Encapsulation. Eng. Life Sci. 2017, 17, 145–152. [Google Scholar] [CrossRef]
- Alvarez-Manceñido, F.; Landin, M.; Martínez-Pacheco, R. Konjac Glucomannan/Xanthan Gum Enzyme Sensitive Binary Mixtures for Colonic Drug Delivery. Eur. J. Pharm. Biopharm. 2008, 69, 573–581. [Google Scholar] [CrossRef]
- Putro, J.N.; Soetaredjo, F.E.; Lunardi, V.B.; Irawaty, W.; Yuliana, M.; Santoso, S.P.; Puspitasari, N.; Wenten, I.G.; Ismadji, S. Polysaccharides Gums in Drug Delivery Systems: A Review. Int. J. Biol. Macromol. 2023, 253, 127020. [Google Scholar] [CrossRef]
- Bertasa, M.; Dodero, A.; Alloisio, M.; Vicini, S.; Riedo, C.; Sansonetti, A.; Scalarone, D.; Castellano, M. Agar Gel Strength: A Correlation Study between Chemical Composition and Rheological Properties. Eur. Polym. J. 2020, 123, 109442. [Google Scholar] [CrossRef]
- Albadran, H.A.; Monteagudo-Mera, A.; Khutoryanskiy, V.V.; Charalampopoulos, D. Development of Chitosan-Coated Agar-Gelatin Particles for Probiotic Delivery and Targeted Release in the Gastrointestinal Tract. Appl. Microbiol. Biotechnol. 2020, 104, 5749–5757. [Google Scholar] [CrossRef]
- Jadav, M.; Pooja, D.; Adams, D.J.; Kulhari, H. Advances in Xanthan Gum-Based Systems for the Delivery of Therapeutic Agents. Pharmaceutics 2023, 15, 402. [Google Scholar] [CrossRef]
- Krishnaiah, Y.S.R.; Satyanarayana, V.; Dinesh Kumar, B.; Karthikeyan, R.S.; Bhaskar, P. In Vivo Evaluation of Guargum-Based Colon-Targeted Oral Drug Delivery Systems of Celecoxib in Human Volunteers. Eur. J. Drug Metab. Pharmacokinet. 2002, 27, 273–280. [Google Scholar] [CrossRef]
- Kenyon, C.J.; Nardi, R.V.; Wong, D.; Hooper, G.; Wilding, I.R.; Friend, D.R. Colonic Delivery of Dexamethasone: A Pharmacoscintigraphic Evaluation. Aliment. Pharmacol. Ther. 1997, 11, 205–213. [Google Scholar] [CrossRef]
- Shahid, M.; Bukhari, S.A.; Gul, Y.; Munir, H.; Anjum, F.; Zuber, M.; Jamil, T.; Zia, K.M. Graft Polymerization of Guar Gum with Acryl Amide Irradiated by Microwaves for Colonic Drug Delivery. Int. J. Biol. Macromol. 2013, 62, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Seeli, D.S.; Prabaharan, M. Guar Gum Succinate as a Carrier for Colon-Specific Drug Delivery. Int. J. Biol. Macromol. 2016, 84, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.M.; Nunes, C.; Pereira, I.; Moreira, A.S.P.; Domingues, M.R.M.; Coimbra, M.A.; Gama, F.M. Structural Analysis of Dextrins and Characterization of Dextrin-Based Biomedical Hydrogels. Carbohydr. Polym. 2014, 114, 458–466. [Google Scholar] [CrossRef]
- Chen, H.; Zheng, D.; Liu, J.; Kuang, Y.; Li, Q.; Zhang, M.; Ye, H.; Qin, H.; Xu, Y.; Li, C.; et al. pH-Sensitive Drug Delivery System Based on Modified Dextrin Coated Mesoporous Silica Nanoparticles. Int. J. Biol. Macromol. 2016, 85, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Teruel, A.H.; Gonzalez-Alvarez, I.; Bermejo, M.; Merino, V.; Marcos, M.D.; Sancenon, F.; Gonzalez-Alvarez, M.; Martinez-Mañez, R. New Insights of Oral Colonic Drug Delivery Systems for Inflammatory Bowel Disease Therapy. Int. J. Mol. Sci. 2020, 21, 6502. [Google Scholar] [CrossRef]
- Payanda Konuk, O.; Alsuhile, A.A.A.M.; Yousefzadeh, H.; Ulker, Z.; Bozbag, S.E.; García-González, C.A.; Smirnova, I.; Erkey, C. The Effect of Synthesis Conditions and Process Parameters on Aerogel Properties. Front. Chem. 2023, 11, 1294520. [Google Scholar] [CrossRef]
- Nita, L.E.; Ghilan, A.; Rusu, A.G.; Neamtu, I.; Chiriac, A.P. New Trends in Bio-Based Aerogels. Pharmaceutics 2020, 12, 449. [Google Scholar] [CrossRef]
- García-González, C.A.; Alnaief, M.; Smirnova, I. Polysaccharide-Based Aerogels—Promising Biodegradable Carriers for Drug Delivery Systems. Carbohydr. Polym. 2011, 86, 1425–1438. [Google Scholar] [CrossRef]
- Patel, S.M.; Doen, T.; Pikal, M.J. Determination of End Point of Primary Drying in Freeze-Drying Process Control. AAPS PharmSciTech 2010, 11, 73–84. [Google Scholar] [CrossRef]
- Kankala, R.K.; Xu, P.-Y.; Chen, B.-Q.; Wang, S.-B.; Chen, A.-Z. Supercritical Fluid (SCF)-Assisted Fabrication of Carrier-Free Drugs: An Eco-Friendly Welcome to Active Pharmaceutical Ingredients (APIs). Adv. Drug Deliv. Rev. 2021, 176, 113846. [Google Scholar] [CrossRef]
- García-González, C.A.; Camino-Rey, M.C.; Alnaief, M.; Zetzl, C.; Smirnova, I. Supercritical Drying of Aerogels Using CO2: Effect of Extraction Time on the End Material Textural Properties. J. Supercrit. Fluids 2012, 66, 297–306. [Google Scholar] [CrossRef]
- Witkowski, A.; Majkut, M.; Rulik, S. Analysis of Pipeline Transportation Systems for Carbon Dioxide Sequestration. Arch. Thermodyn. 2014, 35, 117–140. [Google Scholar] [CrossRef]
- Kravanja, K.A.; Finšgar, M.; Knez, Ž.; Knez Marevci, M. Supercritical Fluid Technologies for the Incorporation of Synthetic and Natural Active Compounds into Materials for Drug Formulation and Delivery. Pharmaceutics 2022, 14, 1670. [Google Scholar] [CrossRef]
- Gurikov, P.; Smirnova, I. Amorphization of Drugs by Adsorptive Precipitation from Supercritical Solutions: A Review. J. Supercrit. Fluids 2018, 132, 105–125. [Google Scholar] [CrossRef]
- Abdul Khalil, H.P.S.; Bashir Yahya, E.; Jummaat, F.; Adnan, A.S.; Olaiya, N.G.; Rizal, S.; Abdullah, C.K.; Pasquini, D.; Thomas, S. Biopolymers Based Aerogels: A Review on Revolutionary Solutions for Smart Therapeutics Delivery. Prog. Mater. Sci. 2023, 131, 101014. [Google Scholar] [CrossRef]
- Mohammadi, A.; Moghaddas, J. Mesoporous Tablet-Shaped Potato Starch Aerogels for Loading and Release of the Poorly Water-Soluble Drug Celecoxib. Chin. J. Chem. Eng. 2020, 28, 1778–1787. [Google Scholar] [CrossRef]
- Tkalec, G.; Knez, Ž.; Novak, Z. Fast Production of High-Methoxyl Pectin Aerogels for Enhancing the Bioavailability of Low-Soluble Drugs. J. Supercrit. Fluids 2015, 106, 16–22. [Google Scholar] [CrossRef]
- Lin, W.-H.; Jana, S.C. Analysis of Porous Structures of Cellulose Aerogel Monoliths and Microparticles. Microporous Mesoporous Mater. 2021, 310, 110625. [Google Scholar] [CrossRef]
- Tkalec, G.; Knez, Ž.; Novak, Z. PH Sensitive Mesoporous Materials for Immediate or Controlled Release of NSAID. Microporous Mesoporous Mater. 2016, 224, 190–200. [Google Scholar] [CrossRef]
- Méndez, D.A.; Schroeter, B.; Martínez-Abad, A.; Fabra, M.J.; Gurikov, P.; López-Rubio, A. Pectin-Based Aerogel Particles for Drug Delivery: Effect of Pectin Composition on Aerogel Structure and Release Properties. Carbohydr. Polym. 2023, 306, 120604. [Google Scholar] [CrossRef] [PubMed]
- Groult, S.; Buwalda, S.; Budtova, T. Tuning Bio-Aerogel Properties for Controlling Drug Delivery. Part 2: Cellulose-Pectin Composite Aerogels. Biomater. Adv. 2022, 135, 212732. [Google Scholar] [CrossRef] [PubMed]
- Karimzadeh, Z.; Namazi, H. Nontoxic Double-Network Polymeric Hybrid Aerogel Functionalized with Reduced Graphene Oxide: Preparation, Characterization, and Evaluation as Drug Delivery Agent. J. Polym. Res. 2022, 29, 37. [Google Scholar] [CrossRef]
- Li, Y.; Fan, R.; Xing, H.; Fei, Y.; Cheng, J.; Lu, L. Study on Swelling and Drug Releasing Behaviors of Ibuprofen-Loaded Bimetallic Alginate Aerogel Beads with pH-Responsive Performance. Colloids Surf. B Biointerfaces 2021, 205, 111895. [Google Scholar] [CrossRef]
- Groult, S.; Buwalda, S.; Budtova, T. Tuning Bio-Aerogel Properties for Controlling Theophylline Delivery. Part 1: Pectin Aerogels. Mater. Sci. Eng. C 2021, 126, 112148. [Google Scholar] [CrossRef] [PubMed]
- Pantić, M.; Kravanja, K.A.; Knez, Ž.; Novak, Z. Influence of the Impregnation Technique on the Release of Esomeprazole from Various Bioaerogels. Polymers 2021, 13, 1882. [Google Scholar] [CrossRef]
- Agostinho, D.A.S.; Paninho, A.I.; Cordeiro, T.; Nunes, A.V.M.; Fonseca, I.M.; Pereira, C.; Matias, A.; Ventura, M.G. Properties of κ-Carrageenan Aerogels Prepared by Using Different Dissolution Media and Its Application as Drug Delivery Systems. Mater. Chem. Phys. 2020, 253, 123290. [Google Scholar] [CrossRef]
- Veres, P.; Sebők, D.; Dékány, I.; Gurikov, P.; Smirnova, I.; Fábián, I.; Kalmár, J. A Redox Strategy to Tailor the Release Properties of Fe(III)-Alginate Aerogels for Oral Drug Delivery. Carbohydr. Polym. 2018, 188, 159–167. [Google Scholar] [CrossRef]
- Veronovski, A.; Knez, Ž.; Novak, Z. Comparison of Ionic and Non-Ionic Drug Release from Multi-Membrane Spherical Aerogels. Int. J. Pharm. 2013, 454, 58–66. [Google Scholar] [CrossRef]
- Del Gaudio, P.; Auriemma, G.; Mencherini, T.; Porta, G.D.; Reverchon, E.; Aquino, R.P. Design of Alginate-Based Aerogel for Nonsteroidal Anti-Inflammatory Drugs Controlled Delivery Systems Using Prilling and Supercritical-Assisted Drying. J. Pharm. Sci. 2013, 102, 185–194. [Google Scholar] [CrossRef]
- López-Iglesias, C.; Casielles, A.M.; Altay, A.; Bettini, R.; Alvarez-Lorenzo, C.; García-González, C.A. From the Printer to the Lungs: Inkjet-Printed Aerogel Particles for Pulmonary Delivery. Chem. Eng. J. 2019, 357, 559–566. [Google Scholar] [CrossRef]
- Alnaief, M.; Alzaitoun, M.A.; García-González, C.A.; Smirnova, I. Preparation of Biodegradable Nanoporous Microspherical Aerogel Based on Alginate. Carbohydr. Polym. 2011, 84, 1011–1018. [Google Scholar] [CrossRef]
- Gonçalves, V.S.S.; Gurikov, P.; Poejo, J.; Matias, A.A.; Heinrich, S.; Duarte, C.M.M.; Smirnova, I. Alginate-Based Hybrid Aerogel Microparticles for Mucosal Drug Delivery. Eur. J. Pharm. Biopharm. 2016, 107, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Russo, P.; Zacco, R.; Rekkas, D.M.; Politis, S.; Garofalo, E.; Del Gaudio, P.; Aquino, R.P. Application of Experimental Design for the Development of Soft-Capsules through a Prilling, Inverse Gelation Process. J. Drug Deliv. Sci. Technol. 2019, 49, 577–585. [Google Scholar] [CrossRef]
- Ganesan, K.; Budtova, T.; Ratke, L.; Gurikov, P.; Baudron, V.; Preibisch, I.; Niemeyer, P.; Smirnova, I.; Milow, B. Review on the Production of Polysaccharide Aerogel Particles. Materials 2018, 11, 2144. [Google Scholar] [CrossRef] [PubMed]
- Brandenberger, H.; Widmer, F. A New Multinozzle Encapsulation/Immobilisation System to Produce Uniform Beads of Alginate. J. Biotechnol. 1998, 63, 73–80. [Google Scholar] [CrossRef]
- Akgün, I.S.; Ulker, Z.; Demir, E.; Işık, M.; Ekmekçiyan, N.; Darvishi, S.; Karaz, S.; Şenses, E.; Erkey, C. Enteric Coating of Drug Loaded Aerogel Particles in a Wurster Fluidized Bed and Its Effect on Release Behaviour. J. Drug Deliv. Sci. Technol. 2023, 82, 104279. [Google Scholar] [CrossRef]
- Schroeter, B.; Yonkova, V.P.; Goslinska, M.; Orth, M.; Pietsch, S.; Gurikov, P.; Smirnova, I.; Heinrich, S. Spray Coating of Cellulose Aerogel Particles in a Miniaturized Spouted Bed. Cellulose 2021, 28, 7795–7812. [Google Scholar] [CrossRef]
- Antonyuk, S.; Heinrich, S.; Gurikov, P.; Raman, S.; Smirnova, I. Influence of Coating and Wetting on the Mechanical Behaviour of Highly Porous Cylindrical Aerogel Particles. Powder Technol. 2015, 285, 34–43. [Google Scholar] [CrossRef]
- Schroeter, B.; Jung, I.; Bauer, K.; Gurikov, P.; Smirnova, I. Hydrophobic Modification of Biopolymer Aerogels by Cold Plasma Coating. Polymers 2021, 13, 3000. [Google Scholar] [CrossRef] [PubMed]
- Veronovski, A.; Knez, Ž.; Novak, Z. Preparation of Multi-Membrane Alginate Aerogels Used for Drug Delivery. J. Supercrit. Fluids 2013, 79, 209–215. [Google Scholar] [CrossRef]
- De Cicco, F.; Russo, P.; Reverchon, E.; García-González, C.A.; Aquino, R.P.; Del Gaudio, P. Prilling and Supercritical Drying: A Successful Duo to Produce Core-Shell Polysaccharide Aerogel Beads for Wound Healing. Carbohydr. Polym. 2016, 147, 482–489. [Google Scholar] [CrossRef]
- Colorectal Cancer. World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/colorectal-cancer (accessed on 7 November 2023).
- Jones, G.R.; Lyons, M.; Plevris, N.; Jenkinson, P.W.; Bisset, C.; Burgess, C.; Din, S.; Fulforth, J.; Henderson, P.; Ho, G.-T.; et al. IBD Prevalence in Lothian, Scotland, Derived by Capture–Recapture Methodology. Gut 2019, 68, 1953–1960. [Google Scholar] [CrossRef] [PubMed]
- Coward, S.; Clement, F.; Benchimol, E.I.; Bernstein, C.N.; Avina-Zubieta, J.A.; Bitton, A.; Carroll, M.W.; Hazlewood, G.; Jacobson, K.; Jelinski, S.; et al. Past and Future Burden of Inflammatory Bowel Diseases Based on Modeling of Population-Based Data. Gastroenterology 2019, 156, 1345–1353. [Google Scholar] [CrossRef]
- Ramos, G.P.; Papadakis, K.A. Mechanisms of Disease: Inflammatory Bowel Diseases. Mayo Clin. Proc. 2019, 94, 155–165. [Google Scholar] [CrossRef]
- Seyedian, S.; Nokhostin, F.; Dargahi, M. A Review of the Diagnosis, Prevention, and Treatment Methods of Inflammatory Bowel Disease. J. Med. Life 2019, 12, 113–122. [Google Scholar] [CrossRef]
- Burisch, J.; Vardi, H.; Schwartz, D.; Friger, M.; Kiudelis, G.; Kupčinskas, J.; Fumery, M.; Gower-Rousseau, C.; Lakatos, L.; Lakatos, P.L.; et al. Health-Care Costs of Inflammatory Bowel Disease in a Pan-European, Community-Based, Inception Cohort during 5 Years of Follow-Up: A Population-Based Study. Lancet Gastroenterol. Hepatol. 2020, 5, 454–464. [Google Scholar] [CrossRef]
- Wang, D.; Wang, W.; Wang, P.; Wang, C.; Niu, J.; Liu, Y.; Chen, Y. Research Progress of Colon-Targeted Oral Hydrogel System Based on Natural Polysaccharides. Int. J. Pharm. 2023, 643, 123222. [Google Scholar] [CrossRef]
- Sellitto, M.R.; Amante, C.; Aquino, R.P.; Russo, P.; Rodríguez-Dorado, R.; Neagu, M.; García-González, C.A.; Adami, R.; Del Gaudio, P. Hollow Particles Obtained by Prilling and Supercritical Drying as a Potential Conformable Dressing for Chronic Wounds. Gels 2023, 9, 492. [Google Scholar] [CrossRef]
- Del Gaudio, P.; Amante, C.; Civale, R.; Bizzarro, V.; Petrella, A.; Pepe, G.; Campiglia, P.; Russo, P.; Aquino, R.P. In Situ Gelling Alginate-Pectin Blend Particles Loaded with Ac2-26: A New Weapon to Improve Wound Care Armamentarium. Carbohydr. Polym. 2020, 227, 115305. [Google Scholar] [CrossRef] [PubMed]
- Sauer, D.; Cerea, M.; DiNunzio, J.; McGinity, J. Dry Powder Coating of Pharmaceuticals: A Review. Prog. Film Coat. 2013, 457, 488–502. [Google Scholar] [CrossRef] [PubMed]












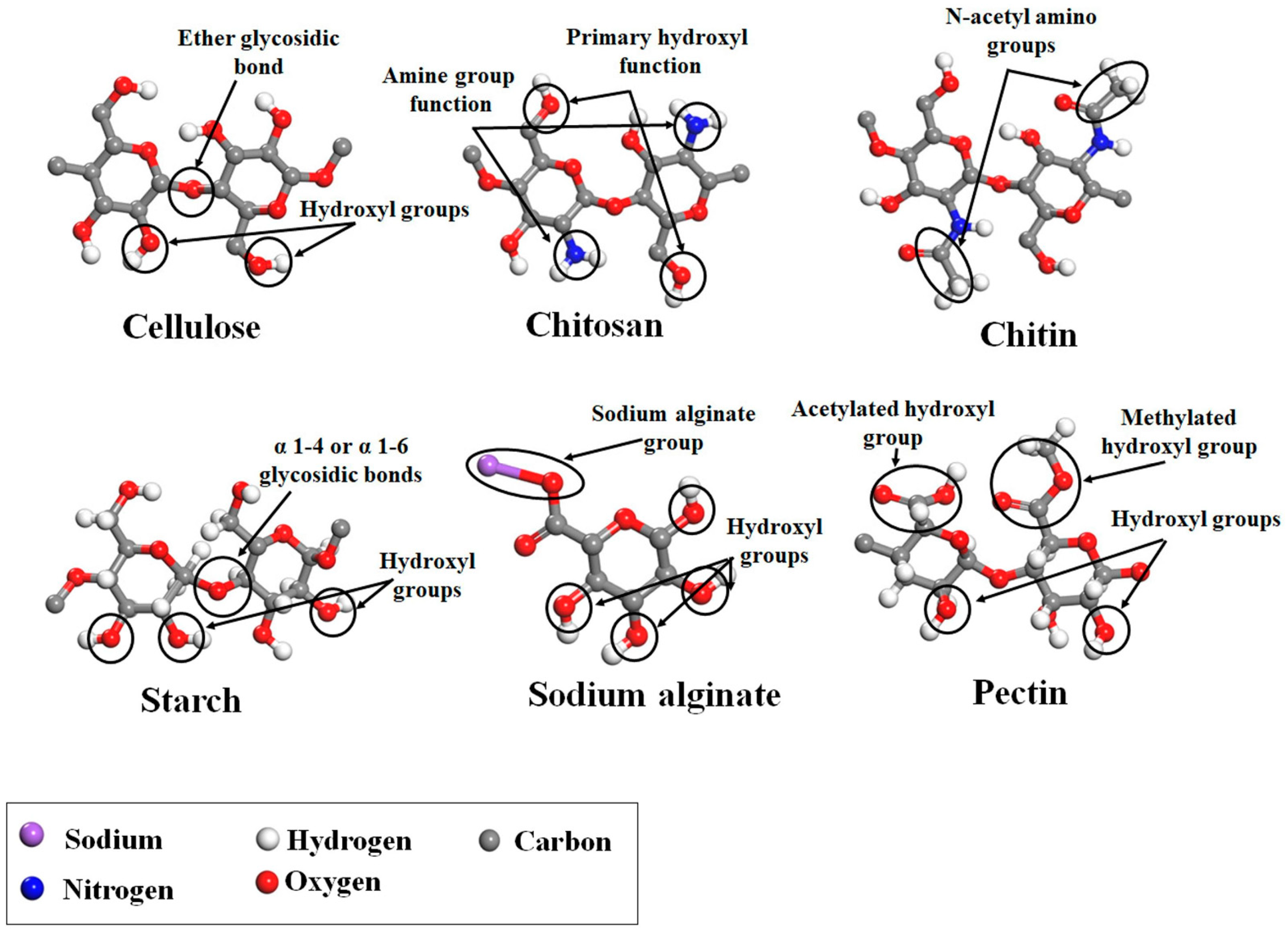
| Polysaccharide | Structure | Composition | Sources | References |
|---|---|---|---|---|
| Alginate (Alg) |  | β-(1→4)-D-mannuronic acid (M) and α-(1→4)-D-guluronic acid (G) are linked by β-(1-4)-glycosidic bonds in different ratios, according to the source. | Marine brown algae and microorganisms | [59,60] |
| Chitosan (CS) |  | N-acetyl-2-amino-2-deoxy-d-glucopyranose (acetylated unit) and 2-amino 2-deoxyd-glucopyranose (deacetylated unit) are linked by β-(1→4)-glycosidic bonds. DD (70–98%) and viscosity in specific conditions (100–5000 mPa∙s). | Chitin deacetylation of exo- and endoskeletons of crustaceans, cephalopods, and insects | [59,61] |
| Pectin |  | α-D-galacturonic acid is linked by α-(1-4)-glycosidic bonds and a variety of neutral sugars such as rhamnose, arabinose, and others. Pectins can be extracted in the form of acid, simple salt, esterified, methylated, or amidated, depending on the source and growth conditions. | Higher plant cell walls | [59] |
| Cellulose and derivatives |  | Anhydro-β-D-glucopyranose is linked by β-1,4-glycosidic bonds. Derivatives typically consist of semisynthetic ether or ester-substituted cellulose. | Higher plant cell walls and microorganisms | [59,62] |
| Starch |  | α-(1-4)-D-glucopyranose units are linked by α-1,4-glycosidic bonds. Amylose (lineal, 70%) and amylopectin (branched, 30%) chains | High variety of tubers, cereals, fruits, and stems | [63,64,65] |
| Konjac Glucomannan (KGM) |  | β-(1-4)-glucopiranose (G) and β-(1-4)-mannose units (M) are randomly linked by β-(1-4)-glycosidic bonds, with a ratio of 1:1.4–1.6 G/M ratios. Little ramifications in C3, and acetyl groups in C6 every 10–20 hexoses | Tubers of Amorphophallus konjac | [66,67,68] |
| Agar-Agar |  | Agarose (70%, β-D-galactose and 3,6-anhydro-α-L-galactose units) and agaropectin (30%, β-D-galactose and L-galactose-6-sulfate groups). Units are linked by α-(1-3) and β-(1-4) glycosidic bonds. | Seaweeds from Gracilaria and Gelidium (red algae) | [59,69,70] |
| Xanthan gum |  | β-(1-4)-D-glucopiranose is linked by β-(1-4) glycosidic bonds, with trisaccharide chains of glucuronic acids on C3. | Fermentation processes of Xanthomonas campestris | [59,69] |
| Guar gum |  | β-(1-4)-D-mannose (Man) is linked by β-(1-4) glycosidic bonds with α-(1-6)-D-galactopyranosyl (Gal) residues (1.37–2.0 Man/Gal ratio). | Seed endosperm of Cyamopsis tetragonolobus | [59,71] |
| Locust Bean gum |  | β-(1-4)-D-mannan is linked by β-(1-4) glycosidic bonds with branches of α-(1-6)-galactose | Seed endosperm of Ceratonia silique | [69,72] |
| Entry | Aerogel Composition and Gelation Technique | Drug | Preparation Method | Loading Method | Drug Release Conditions and Kinetic Models | Ref. |
|---|---|---|---|---|---|---|
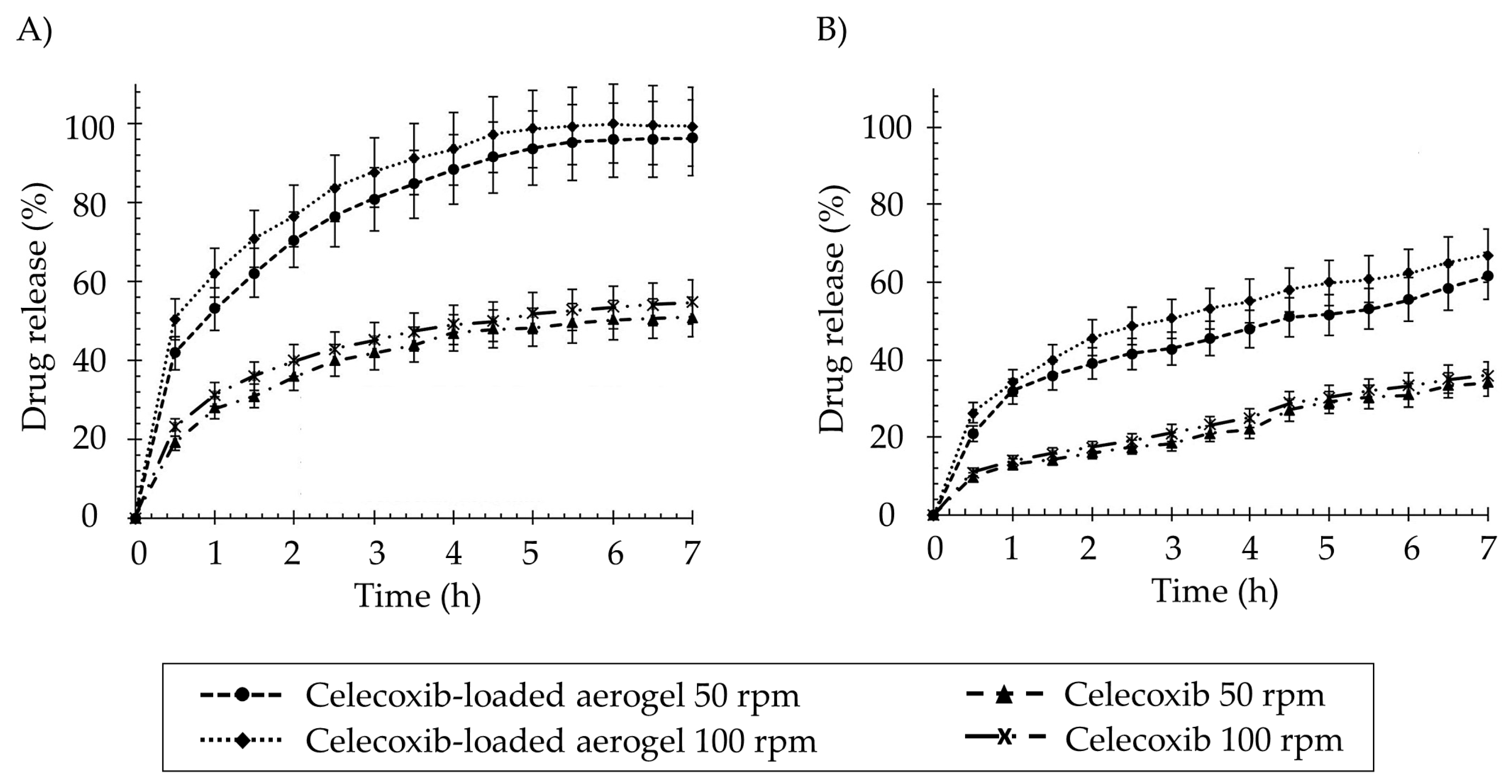
| 1 | Potato starch (14.1% w/v). Gelation by retrogradation | Celecoxib | Sol–gel method in molds. Monolithic shapes. | Solvent exchange in drug-saturated ethanol solution | SGF (pH 1.2) for 7 h and SIF (pH 7.4) for 7 h Korsmeyer–Peppas model. | [111] |
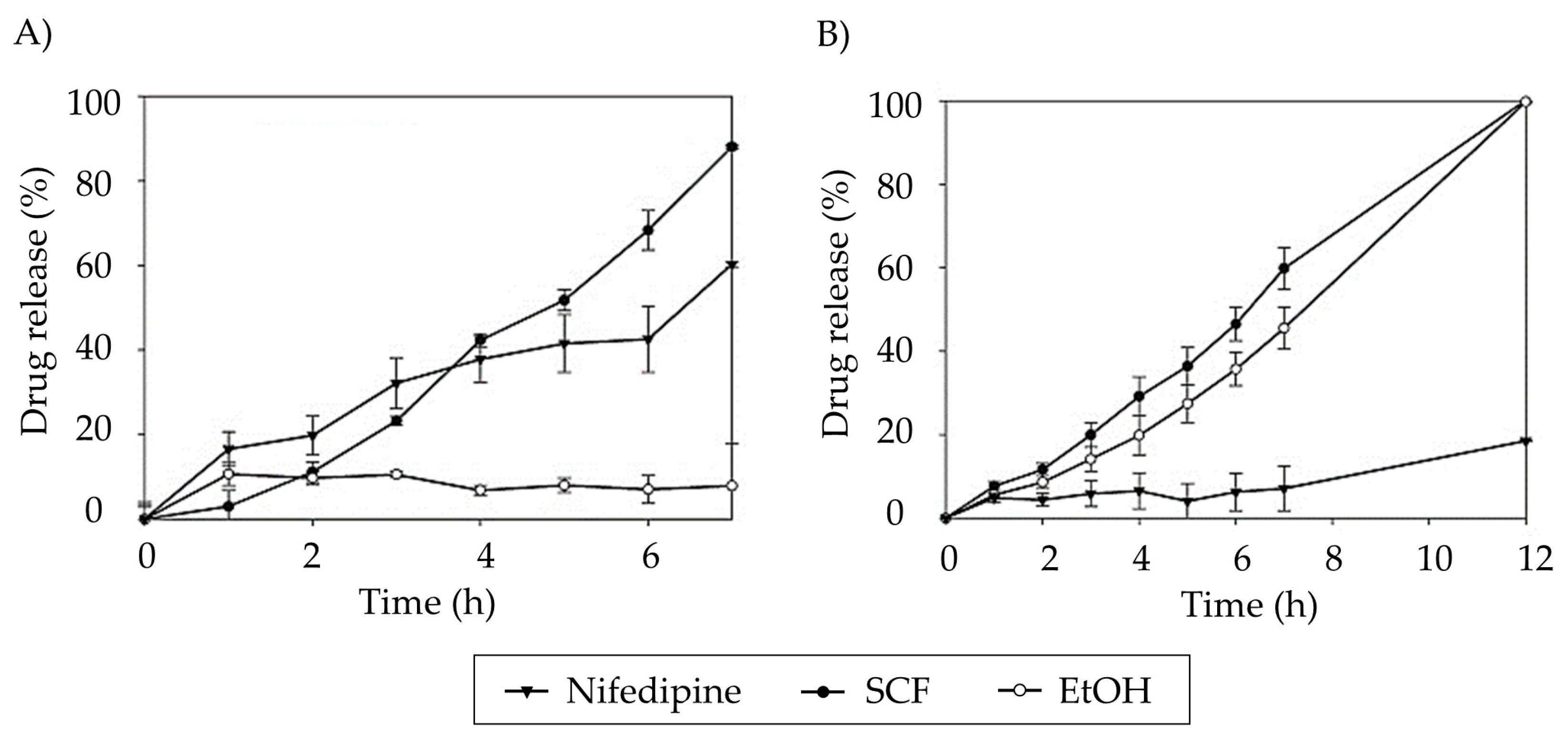
| 2 | High-methoxyl pectin (1, 2, 4% w/v). Crosslinking by coagulation with EtOH. | Nifedipine | Sol–gel method in molds. Monolithic shapes | Solvent exchange in drug-saturated EtOH solution or supercritical impregnation | SGF (pH 1.2) for 1 h and PBS (pH 6.8) for 11 h. Korsmeyer–Peppas model. Higher drug release in PBS than SFG. | [112] |
| 3 | MCC. Gelation by non-solvent-induced phase separation. | Acetaminophen | Emulsion method and gelation in molds. Multiparticle and monolithic shapes. | Solvent exchange in drug-saturated EtOH solution | PBS (pH 7.4) at 37 °C. First-order kinetics release. | [113] |
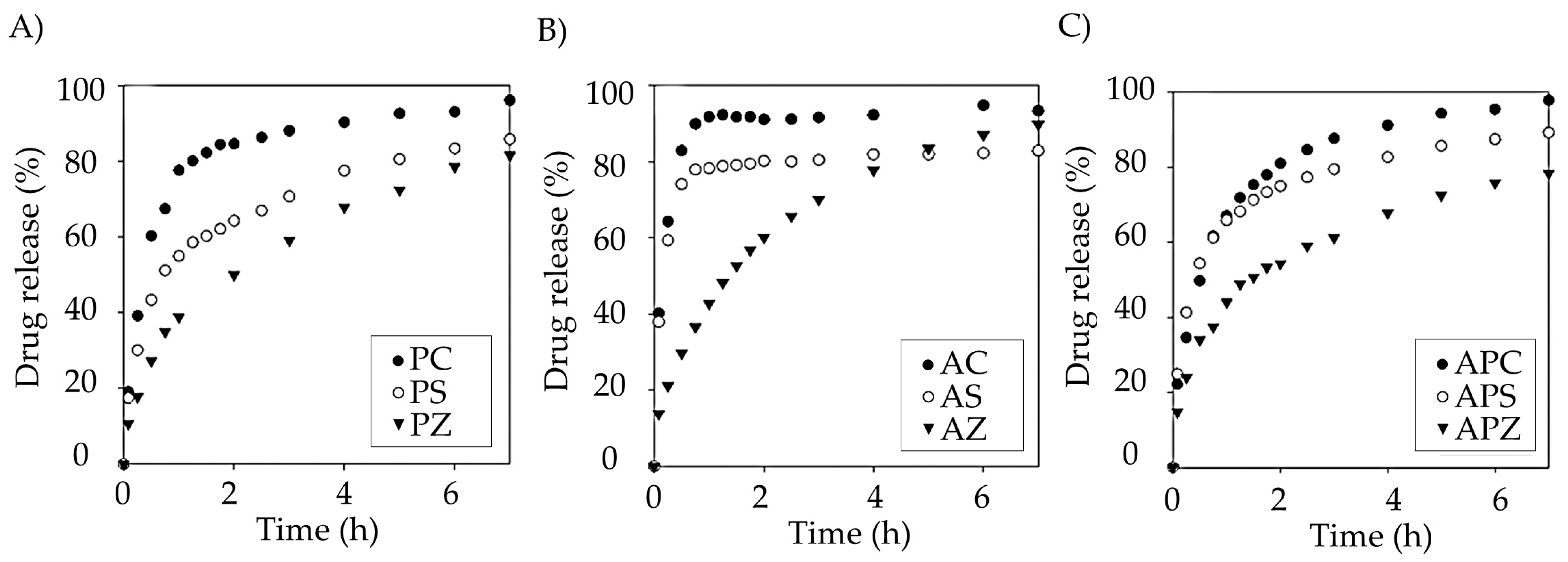
| 4 | Alg, pectin, and mixtures (2% w/v). Ionic gelation (Ca2+, Zn2+, or Sr2+) | Diclofenac sodium | Dripping gelation. Multiparticle shapes. | Sol–gel dissolution | HCl media (pH 1.2), PBS (pH 6.8), and SGF. Korsmeyer–Peppas model. | [114] |
| 5 | Pectin. Ionic gelation (CaCl2 0.5% w/w) | Vanillin | Jet cutting and dripping methods Multiparticle shapes. | SCF impregnation | Distilled water at 30, 40, and 50 °C. Weibull model. | [115] |
| 6 | Citrus pectin and MCC. Thermal and ionic gelation (CaCl2 0.5 M) | Theophylline | Thermally induced gelation of MCC in molds, followed by pectin solution immersion. Monolithic shapes. | Solvent exchange in drug-saturated EtOH solution | SGF (pH 1.2) and SIF (pH 6.8) for 12 h. Korsmeyer–Peppas model. Formulations crosslinked with CaCl2 have longer sustained release than no crosslinked. | [116] |
| 7 | K-carrageenan, Alg, and reduced graphene oxide. Ionic gelation (CaCl2 0.44% w/w) | Amoxicillin | Sol–gel method in molds. Monolithic shapes. | Sol–gel dissolution | Buffer (pHs 4.0, 5.5, 7.4 and 9.0). Korsmeyer–Peppas model. The cumulative drug release increases with the pH. | [117] |
| 8 | Alg 2% w/w. Ionic gelation (Ca2+ 4% w/w, and Ba2+ 4–12% w/w) | Ibuprofen | Dripping gelation. Multiparticle shapes. | Sol–gel dissolution | SGF (pH 1.2) and SIF (pH 7.2). Korsmeyer–Peppas release model | [118] |
| 9 | Pectin (2, 4 and 6% w/v). pH reduction and ionic gelation (CaCl2, Ca2+/COO− ratios, from 0.05 to 0.2 according to the pectin concentration) | Theophylline | Sol–gel method in molds. Monolithic shapes | Solvent exchange in drug-saturated EtOH solution | SGF (pH 1.0) for 1 h, followed by SIF (pH 6.8) for 5 h. Peppas-Sahlin model: diffusional mechanism up to 60% released. Gallagher-Corrigan model: full release period | [119] |
| 10 | Alg 2% w/v, CS 1.5% w/v, and pectin 2% w/v. Gelation by non-solvent-induced phase separation (EtOH). | Esomeprazole | Sol–gel method in molds. Monolithic shapes | Solvent exchange in drug-saturated EtOH solution | SGF (pH 1.2) for 2 h and SIF (pH 6.8) for 2 h. Differences in release according to the loading procedure. | [120] |
| 11 | Kappa-carrageenan (2, 10% w/v). Ionic gelation (KCl 0.6 M, potassium thiocyanate 0.6 M, imidazolium cation). | Tetracycline | Sol–gel method in molds. Monolithic shapes | Impregnation in drug-saturated EtOH solution | Solution (pH 7.4) for 3 h. Korsmeyer–Peppas model. A total of 90% released in 60 min | [121] |
| 12 | Alg 2% w/v (low and high guluronic. Ionic gelation (Fe3+ 0.05 M). | Ibuprofen Ascorbic acid | Dripping gelation. Multiparticle shapes. | SCF impregnation | HCl media (pH 2.0) and PBS (pH 7.4). Korsmeyer–Peppas release model in acid medium | [122] |
| 13 | Silica, alg (1.5% w/v), pectin (6% w/v), or starch (15% w/v). Thermal or chemical gelation. | Ketoprofen or benzoic acid | Emulsion–gelation method. Multiparticle shapes | SCF impregnation | PBS (pH 6.8) and SGF (pH 1.2) for 24 h. Korsmeyer–Peppas and Gallagher-Corrigan models | [22] |
| 14 | Alg. Ionic gelation (Ca2+, Ba2+ 0.2 M). | Nicotinic acid and theophylline | Dripping gelation and additional gelation by immersion. Multilayer particles. | Sol–gel dissolution | SIF (pH 6.5) for 24 h. Korsmeyer–Peppas model. The number of layers increases the drug loading and the sustained release time | [123] |
| 15 | Alg. Ionic gelation (CaCl2 0.3 M). | Ketoprofen and ketoprofen lysinate | Prilling (vibration, 300 Hz). Multiparticle shapes. | Sol–gel dissolution. | SGF (pH 1.2) for 2 h, and SIF (pH 6.8) for 4 h | [124] |
| Entry | Core Material | Coating Material | Coating Method | Advantages in Colonic Delivery | Reference |
|---|---|---|---|---|---|
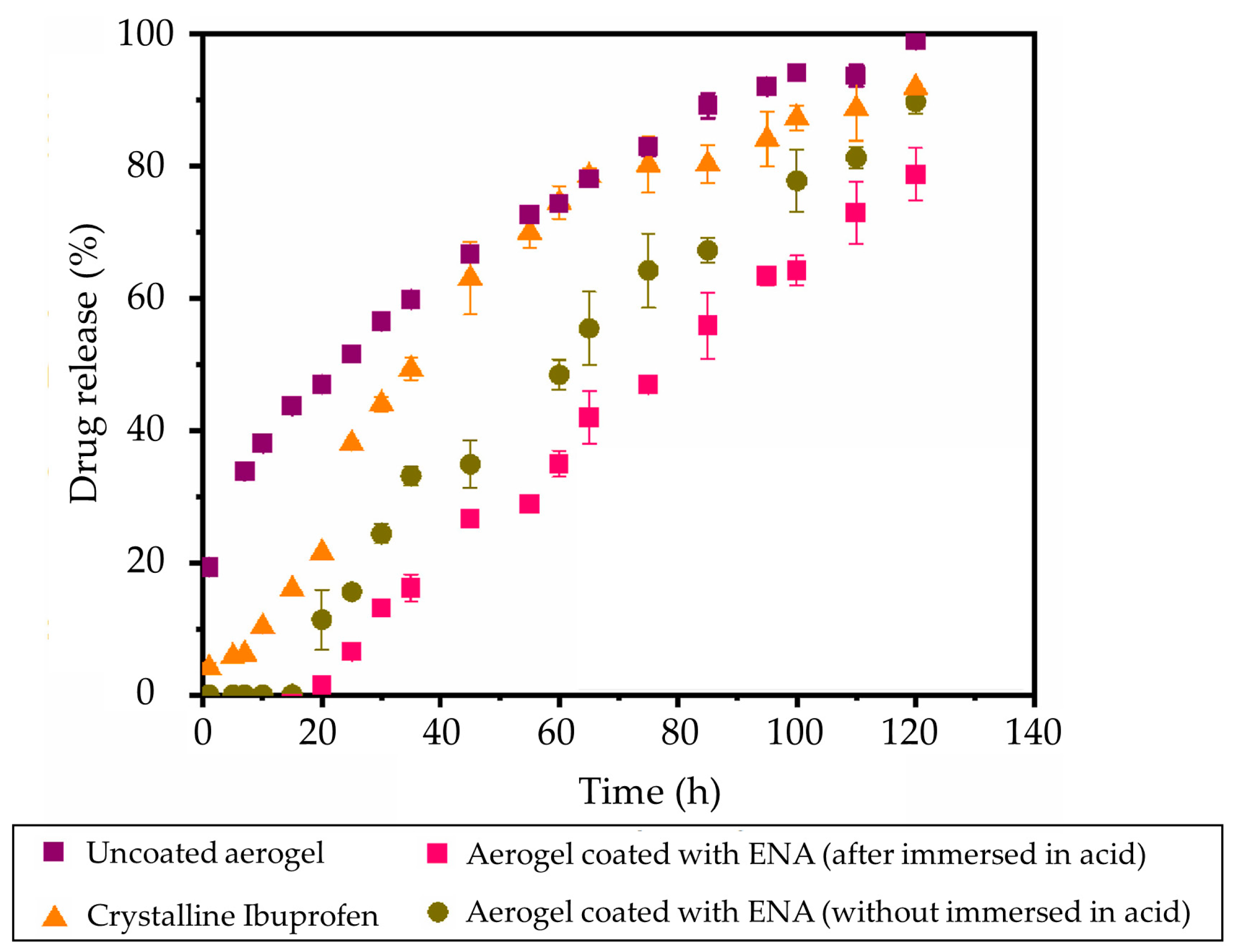
| 1 | Alg aerogel. Ibuprofen loaded by SCF impregnation | Aqueous methacrylic acid-ethyl acrylate polymer solution | Wurster fluidized bed | pH response and controlled drug release | [131] |
| 2 | Cellulose aerogel. Vanillin loaded by SCF impregnation | Ethanol shellac solutions | Spouted bed | Controlled drug release | [132] |
| 3 | Alg–starch aerogels | Eudragit® 30 D-55 (30% w/v) | Fluidized bed | pH response. Unconstrained water uptake at basic pH | [133] |
| 4 | Alg or cellulose aerogels | Perfluoro-acrylates | Cold plasma | Modulate the aerogel surface wettability | [134] |
| 5 | Alg beads | Alg solutions (0.75% w/v) | Multi-step sol–gel process | Controlled release of hydrophilic drug | [135] |
| 6 | Pectin solution | Alg solution (1.5–1.75% w/v) | Coaxial prilling | Sustained drug release | [136] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Illanes-Bordomás, C.; Landin, M.; García-González, C.A. Aerogels as Carriers for Oral Administration of Drugs: An Approach towards Colonic Delivery. Pharmaceutics 2023, 15, 2639. https://doi.org/10.3390/pharmaceutics15112639
Illanes-Bordomás C, Landin M, García-González CA. Aerogels as Carriers for Oral Administration of Drugs: An Approach towards Colonic Delivery. Pharmaceutics. 2023; 15(11):2639. https://doi.org/10.3390/pharmaceutics15112639
Chicago/Turabian StyleIllanes-Bordomás, Carlos, Mariana Landin, and Carlos A. García-González. 2023. "Aerogels as Carriers for Oral Administration of Drugs: An Approach towards Colonic Delivery" Pharmaceutics 15, no. 11: 2639. https://doi.org/10.3390/pharmaceutics15112639