

Lipophosphonoxins—A Novel Group of Broad Spectrum Antibacterial Compounds


Abstract
:1. Introduction
2. Lipophosphonoxins
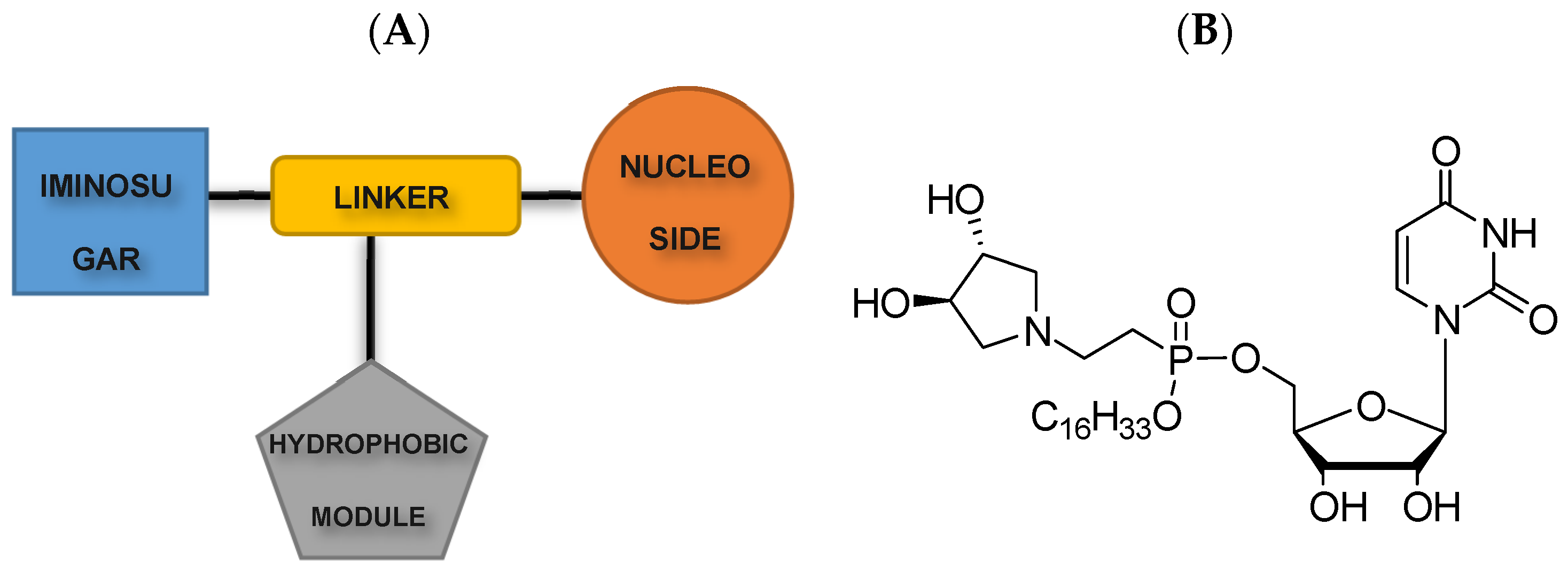
2.1. First-Generation Lipophosphonoxins
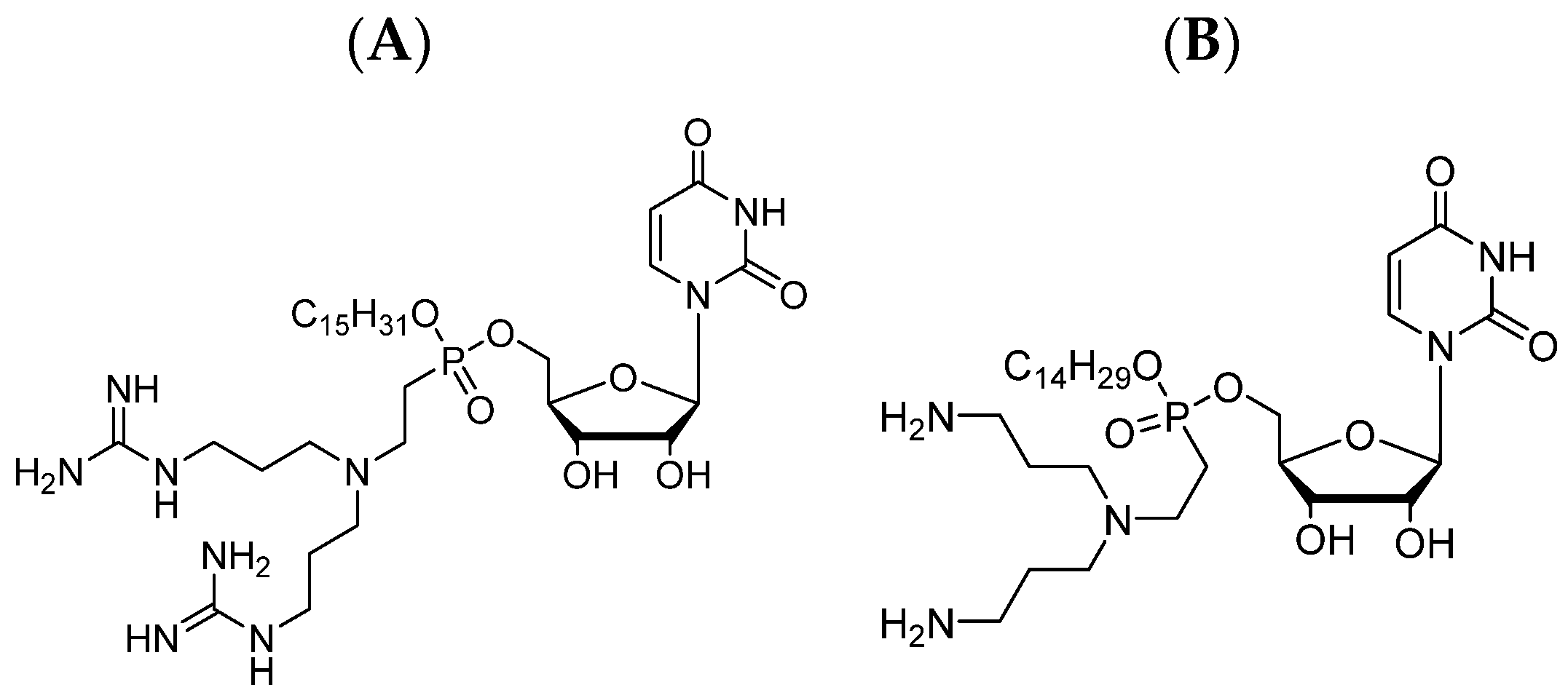
2.2. Second-Generation Lipophosphonoxins
2.2.1. Second-Generation LPPOs as Antimicrobial Additives in Bone Cement
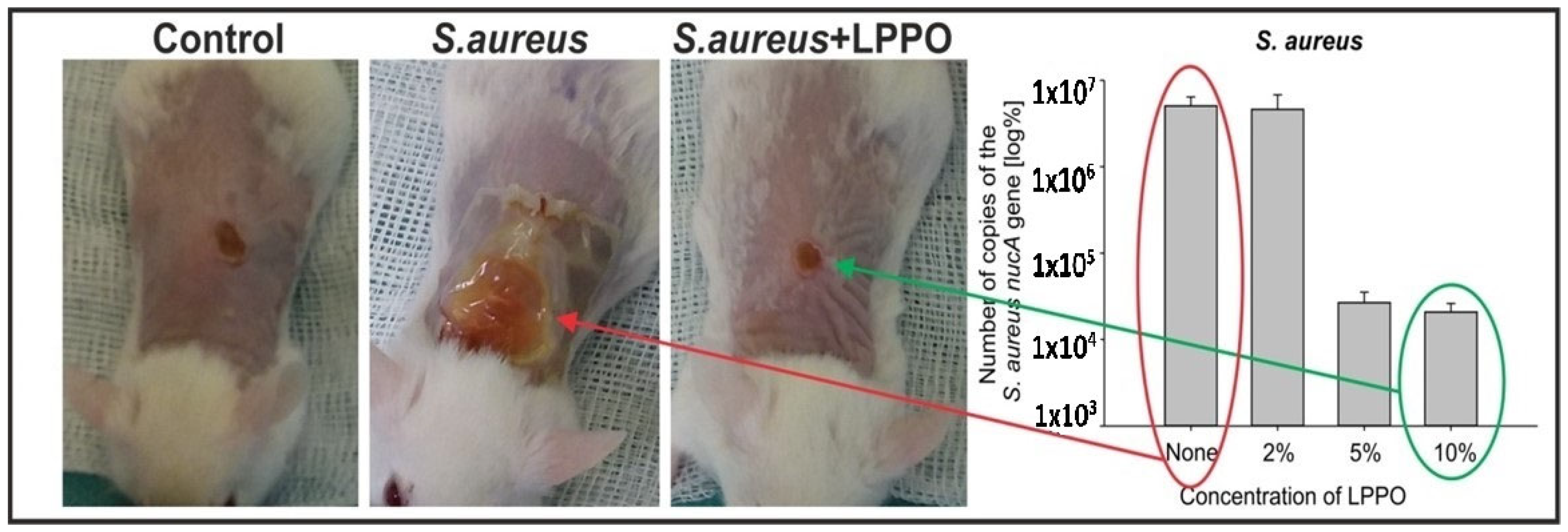
2.2.2. Nanofiber Dressing Loaded with Second-Generation LPPO in Treatment of Wound Infection Induced by Staphylococcus aureus
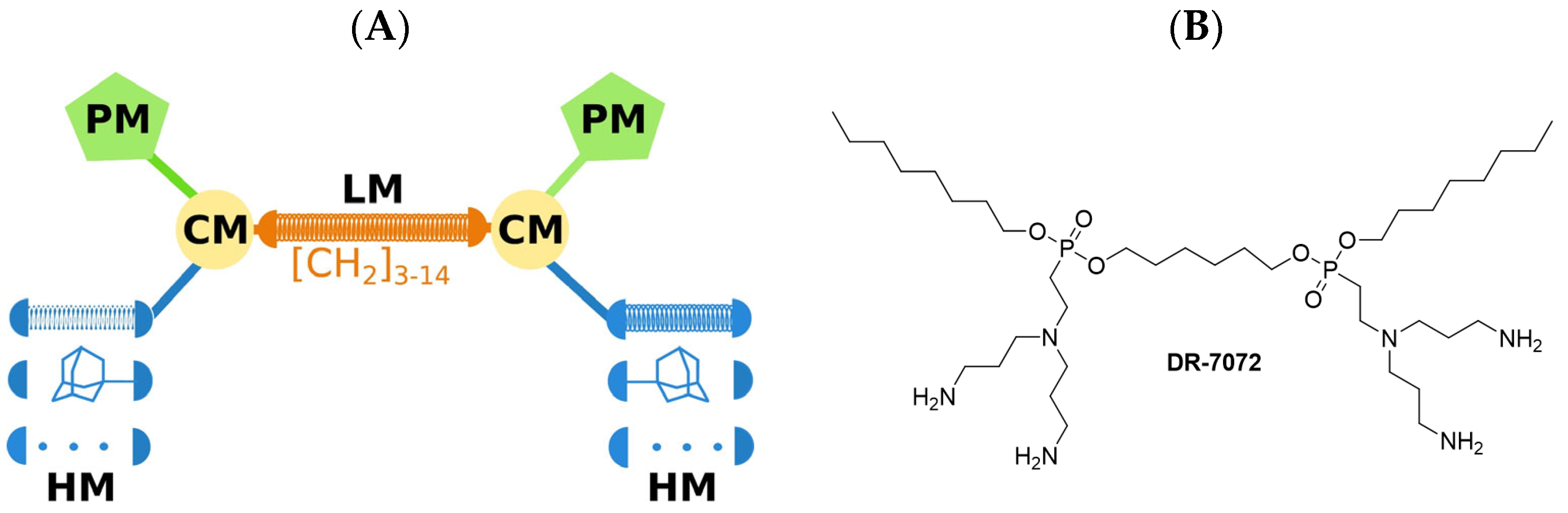
2.3. LEGO–Lipophosphonoxins
Second-Generation and LEGO–LPPOs Ex Vivo Effect on Root Canal Biofilm Produced by Enterococcus faecalis
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aminov, R.I. A brief history of the antibiotic era: Lessons learned and challenges for the future. Front. Microbiol. 2010, 1, 134. [Google Scholar] [CrossRef] [PubMed]
- Levy, S.B. The Antibiotic Paradox. In From Tragedy the Antibiotic Age Is Born; Springer: Berlin/Heidelberg, Germany, 1992; pp. 1–12. [Google Scholar]
- Davies, J. Where have All the Antibiotics Gone? Can. J. Infect. Dis. Med. Microbiol. 2006, 17, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Fleming, A. Nobel Lecture, Alexander Fleming—Nobel Lecture. Available online: nobelprize.org (accessed on 11 December 2022).
- Kesselheim, A.S.; Outterson, K. Fighting Antibiotic Resistance: Marrying New Financial Incentives to Meeting Public Health Goals. Health Aff. 2010, 29, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Press Release, 35,000 Annual Deaths from Antimicrobial Resistance in the EU/EEA. Available online: europa.eu (accessed on 17 November 2022).
- Enabling Breakthroughs in Antimicrobials. Available online: https://www.amractionfund.com/ (accessed on 2 January 2023).
- Scott, W.R.; Tew, N.G. Mimics of host defense proteins; strategies for translation to therapeutic applications. Curr. Top. Med. Chem. 2017, 17, 576–589. [Google Scholar] [CrossRef]
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations; Government of the United Kingdom: London, UK, 2016; pp. 1–84. Available online: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf (accessed on 24 September 2023).
- Hurdle, J.G.; O’neill, A.J.; Chopra, I.; Lee, R.E. Targeting bacterial membrane function: An underexploited mechanism for treating persistent infections. Nat. Rev. Microbiol. 2011, 9, 62–75. [Google Scholar] [CrossRef]
- Ghosh, C.; Haldar, J. Membrane-active small molecules: Designs inspired by antimicrobial peptides. ChemMedChem 2015, 10, 1606–1624. [Google Scholar] [CrossRef]
- Huan, Y.; Kong, Q.; Mou, H.; Yi, H. Antimicrobial Peptides: Classification, Design, Application and Research Progress in Multiple Fields. Front. Microbiol. 2020, 11, 582779. [Google Scholar] [CrossRef]
- Alavi, S.E.; Cabot, P.J.; Moyle, P.M. Glucagon-Like Peptide-1 Receptor Agonists and Strategies to Improve Their Efficiency. Mol. Pharm. 2019, 16, 2278–2295. [Google Scholar] [CrossRef]
- Do Pham, D.D.; Mojr, V.; Helusová, M.; Mikusova, G.; Pohl, R.; Dávidová, E.; Sanderova, H.; Vítovská, D.; Bogdanova, K.; Vecerova, R.; et al. LEGO-Lipophosphonoxins: A Novel Approach in Designing Membrane Targeting Antimicrobials. J. Med. Chem. 2022, 65, 10045–10078. [Google Scholar] [CrossRef]
- Nilsson, A.C.; Janson, H.; Wold, H.; Fugelli, A.; Andersson, K.; Håkangård, C.; Olsson, P.; Olsen, W.M. LTX-109 is a novel agent for nasal decolonization of methicillin-resistant and -sensitive Staphylococcus aureus. Antimicrob. Agents Chemother. 2015, 59, 145. [Google Scholar] [CrossRef]
- Chin, J.N.; Rybak, M.J.; Cheung, C.M.; Savage, P.B. Antimicrobial activities of ceragenins against clinical isolates of resistant Staphylococcus aureus. Antimicrob. Agents Chemother. 2007, 51, 1268–1273. [Google Scholar] [CrossRef] [PubMed]
- Bucki, R.; Niemirowicz, K.; Wnorowska, U.; Byfield, F.J.; Piktel, E.; Wątek, M.; Janmey, P.A.; Savage, P.B. Bactericidal activity of ceragenin CSA-13 in cell culture and in an animal model of peritoneal infection. Antimicrob. Agents Chemother. 2015, 59, 6274. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, A.; Dj, P.; Mn, G.; Dj, H.; Dl, P. Drugs for bad bugs: Confronting the challenges of antibacterial discovery. Nat. Rev. Drug Discov. 2007, 6, 29–40. [Google Scholar]
- Rejman, D.; Rabatinová, A.; Pombinho, A.R.; Kovačková, S.; Pohl, R.; Zborníková, E.; Kolář, M.; Bogdanová, K.; Nyč, O.; Šanderová, H.; et al. Lipophosphonoxins: New Modular Molecular Structures with Significant Antibacterial Properties. J. Med. Chem. 2011, 54, 7884–7898. [Google Scholar] [CrossRef]
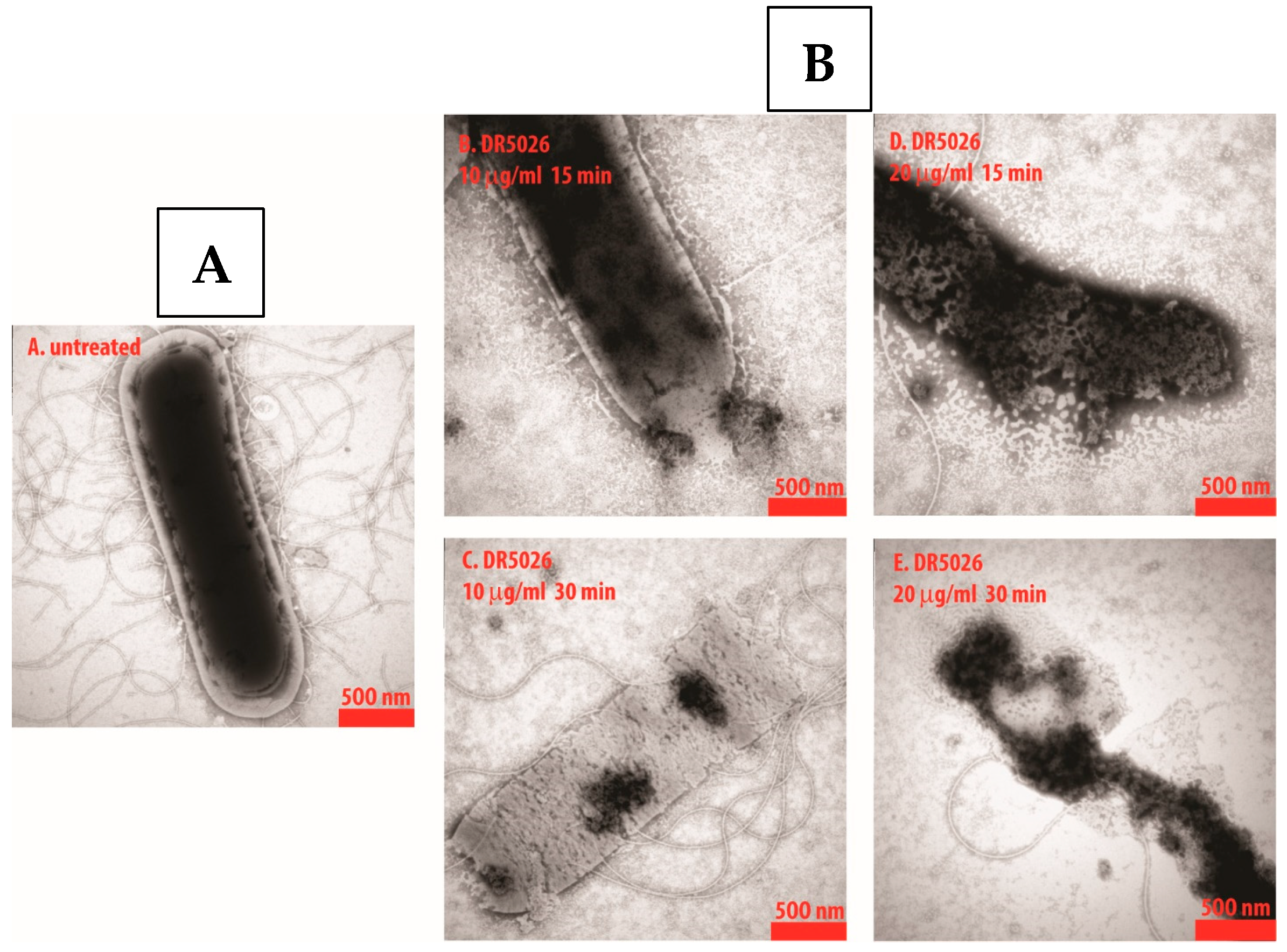
- Panova, N.; Zborníková, E.; Šimák, O.; Pohl, R.; Kolář, M.; Bogdanová, K.; Večeřová, R.; Seydlová, G.; Fišer, R.; Hadravová, R.; et al. Insights into the mechanism of action of bactericidal lipophosphonoxins. PLoS ONE 2015, 10, e0145918. [Google Scholar] [CrossRef]
- Glukhov, E.; Stark, M.; Burrows, L.L.; Deber, C.M. Basis for selectivity of cationic antimicrobial peptides for bacterial versus mammalian membranes. J. Biol. Chem. 2005, 280, 33960–33967. [Google Scholar] [CrossRef]
- Seydlová, G.; Pohl, R.; Zbornikova, E.; Ehn, M.; Šimák, O.; Panova, N.; Kolář, M.; Bogdanová, K.; Večceřrová, R.; Fišser, R.; et al. Lipophosphonoxins II: Design, synthesis, and properties of novel broad spectrum antibacterial agents. J. Med. Chem. 2017, 60, 6098–6118. [Google Scholar] [CrossRef]
- Fernandes, A.; Dias, M. The microbiological profiles of infected prosthetic implants with an emphasis on the organisms which form biofilms. J. Clin. Diagn. Res. 2013, 7, 219–223. [Google Scholar] [CrossRef]
- Ribeiro, M.; Monteiro, F.J.; Ferraz, M.P. Infection of orthopedic implants with emphasis on bacterial adhesion process and techniques used in studying bacterial-material interactions. Biomatter 2012, 2, 176–194. [Google Scholar] [CrossRef]
- Anagnostakos, K.; Fink, B. Antibiotic-loaded cement spacers-lessons learned from the past 20 years. Expert Rev. Med. Devices 2018, 15, 231–245. [Google Scholar] [CrossRef]
- Zbornikova, E.; Gallo, J.; Vecerova, R.; Bogdanova, K.; Kolar, M.; Vitovska, D.; Do Pham, D.D.; Paces, O.; Mojr, V.; Sanderova, H.; et al. Evaluation of second-generation lipophosphonoxins as antimicrobial additives in bone cement. ACS Omega 2020, 5, 3165–3171. [Google Scholar] [CrossRef] [PubMed]
- Cartotto, R. Topical antimicrobial agents for pediatric burns. Burn. Trauma 2017, 5, 33. [Google Scholar] [CrossRef] [PubMed]
- Al-Enizi, A.M.; Zagho, M.M.; Elzatahry, A.A. Polymer-based electrospun nanofibers for biomedical applications. Nanomaterials 2018, 8, 259. [Google Scholar] [CrossRef] [PubMed]
- Do Pham, D.D.; Jenčová, V.; Kaňuchová, M.; Bayram, J.; Grossová, I.; Šuca, H.; Urban, L.; Havlíčková, K.; Novotný, V.; Mikeš, P.; et al. Novel lipophosphonoxin-loaded polycaprolactone electrospun nanofiber dressing reduces Staphylococcus aureus induced wound infection in mice. Sci. Rep. 2021, 11, 17688. [Google Scholar] [CrossRef]
- Jafari, A.; Amirsadeghi, A.; Hassanajili, S.; Azarpira, N. Bioactive antibacterial bilayer PCL/gelatin nanofibrous scaffold promotes full-thickness wound healing. Int. J. Pharm. 2020, 583, 119413. [Google Scholar] [CrossRef]
- Strahl, H.; Hamoen, L.W. Membrane potential is important for bacterial cell division. Proc. Natl. Acad. Sci. USA 2010, 107, 12281–12286. [Google Scholar] [CrossRef]
- Haapasalo, M.; Qian, W.; Portenier, I.; Waltimo, T. Effects of Dentin on the Antimicrobial Properties of Endodontic Medicaments. J. Endod. 2007, 33, 917–925. [Google Scholar] [CrossRef]
- Do, Q.L.; Gaudin, A. The Efficiency of the Er: YAG Laser and Photon Induced Photoacoustic Streaming (PIPS) as an Activation Method in Endodontic Irrigation: A Literature Review. J. Lasers Med. Sci. 2020, 11, 316–334. [Google Scholar] [CrossRef]
- Morozova, Y.; Voborná, I.; Žižka, R.; Bogdanová, K.; Večeřová, R.; Rejman, D.; Kolář, M.; Pham, D.D.D.; Holík, P.; Moštěk, R.; et al. Ex Vivo Effect of Novel Lipophosphonoxins on Root Canal Biofilm Produced by Enterococcus faecalis: Pilot Study. Life 2022, 12, 129. [Google Scholar] [CrossRef]
- Guengerich, F.P. Inhibition of cytochrome P450 enzymes by drugs—Molecular basis and practical applications. Biomol. Therap. 2022, 30, 1–18. [Google Scholar] [CrossRef]
- Guthrie, B.; Makubate, B.; Hernandez-Santiago, V.; Dreischulte, T. The rising tide of polypharmacy and drug-drug interactions: Population database analysis 1995–2010. BMC Med. 2015, 13, 74. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cytotoxicity against | MIC | Activity in the Presence of Albumin | Resistance Development | |
| 1st generation LPPOs | G+ | 1–12 mg/L | NO | not observed |
| 2nd generation LPPOs | G+ and G− | <1 to 6 mg/L | NO | not observed |
| LEGO-LPPOs | G+ and G− | <1 to 8 mg/L | YES | not observed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Šebek, V.; Anzenbacher, P.; Rejman, D.; Špičáková, A.; Kolář, M. Lipophosphonoxins—A Novel Group of Broad Spectrum Antibacterial Compounds. Pharmaceutics 2023, 15, 2395. https://doi.org/10.3390/pharmaceutics15102395
Šebek V, Anzenbacher P, Rejman D, Špičáková A, Kolář M. Lipophosphonoxins—A Novel Group of Broad Spectrum Antibacterial Compounds. Pharmaceutics. 2023; 15(10):2395. https://doi.org/10.3390/pharmaceutics15102395
Chicago/Turabian StyleŠebek, Viktor, Pavel Anzenbacher, Dominik Rejman, Alena Špičáková, and Milan Kolář. 2023. "Lipophosphonoxins—A Novel Group of Broad Spectrum Antibacterial Compounds" Pharmaceutics 15, no. 10: 2395. https://doi.org/10.3390/pharmaceutics15102395