
Comparative Safety Analysis of Empagliflozin in Type 2 Diabetes Mellitus Patients with Chronic Kidney Disease versus Normal Kidney Function: A Nationwide Cohort Study in Korea

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sources
2.2. Ethical Approval
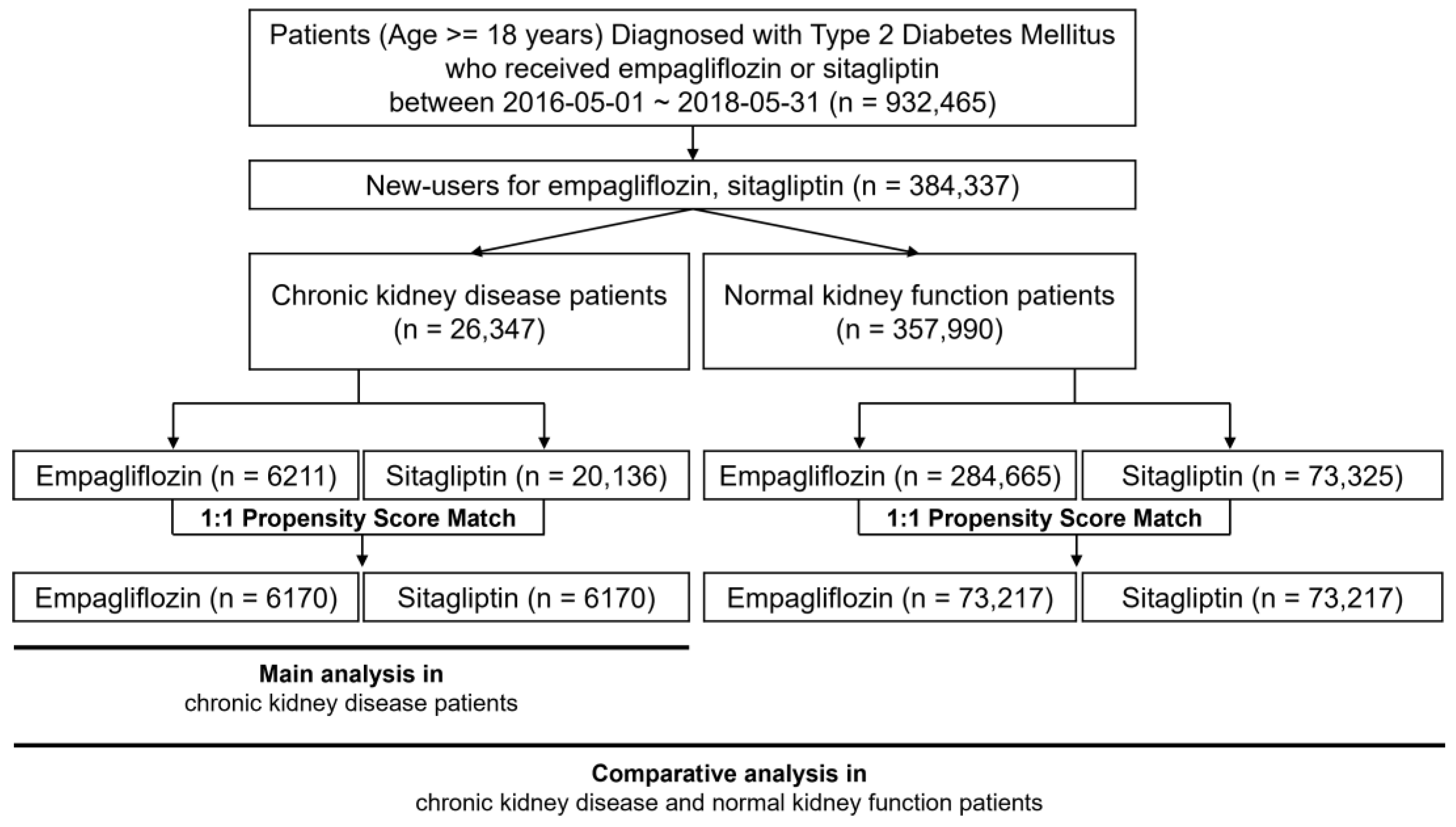
2.3. Study Patients
2.4. Key Variables
2.5. Statistical Analysis
2.6. Comparative Analysis
3. Results
3.1. Demographics
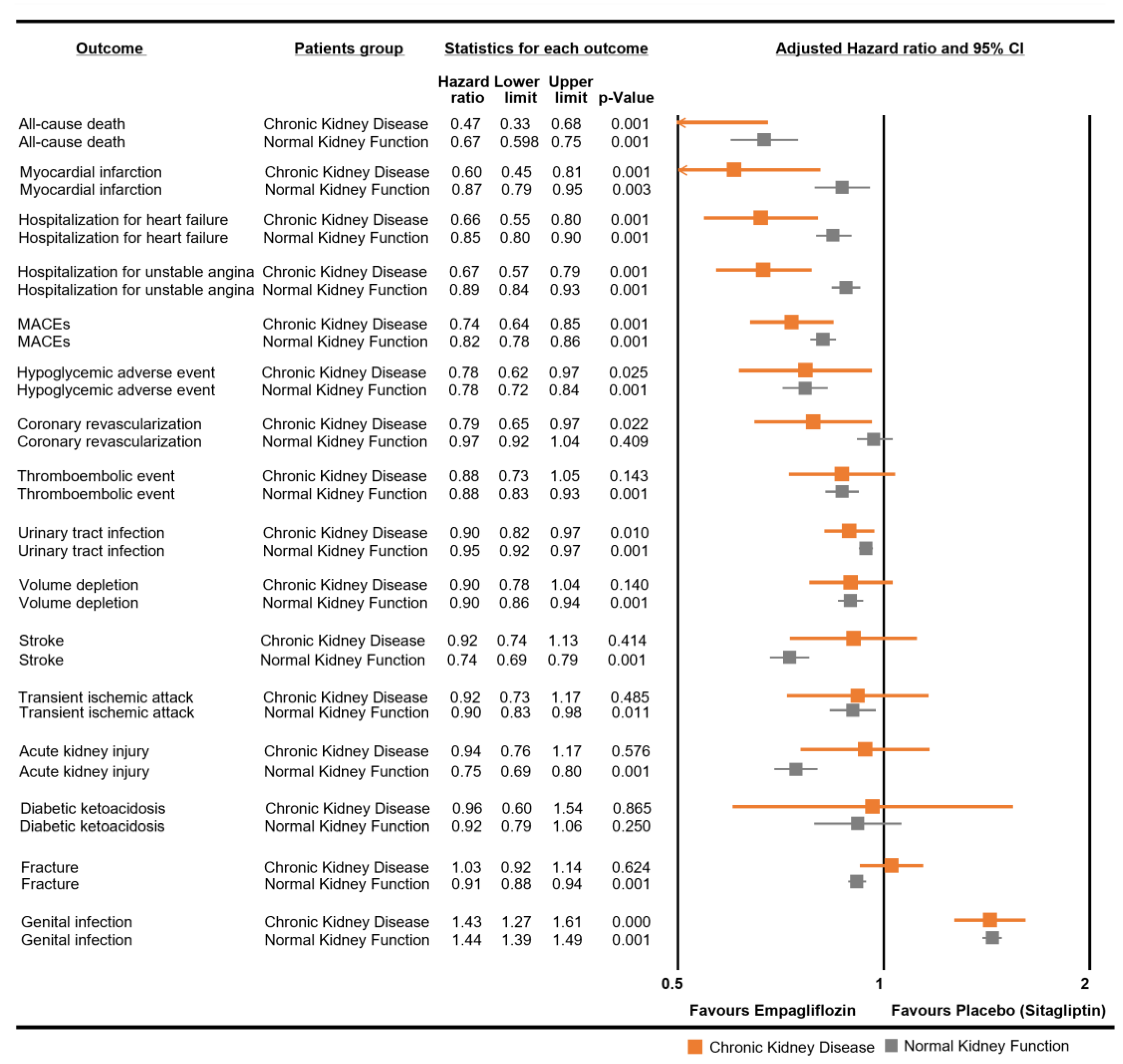
3.2. Risk of Safety Outcomes
3.3. Sensitivity Analysis
3.4. Comparative Analysis: CKD Group versus NKF Group
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes, A. Standards of Medical Care in Diabetes-2018 Abridged for Primary Care Providers. Clin. Diabetes 2018, 36, 14–37. [Google Scholar] [CrossRef] [PubMed]
- Das, S.R.; Everett, B.M.; Birtcher, K.K.; Brown, J.M.; Cefalu, W.T.; Januzzi, J.L., Jr.; Kalyani, R.R.; Kosiborod, M.; Magwire, M.L.; Morris, P.B.; et al. 2018 ACC Expert Consensus Decision Pathway on Novel Therapies for Cardiovascular Risk Reduction in Patients with Type 2 Diabetes and Atherosclerotic Cardiovascular Disease: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J. Am. Coll. Cardiol. 2018, 72, 3200–3223. [Google Scholar] [CrossRef] [PubMed]
- DailyMed. Drug Label: Empagliflozin (JARDIANCE). Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=faf3dd6a-9cd0-39c2-0d2e-232cb3f67565 (accessed on 1 June 2023).
- Afkarian, M.; Zelnick, L.R.; Hall, Y.N.; Heagerty, P.J.; Tuttle, K.; Weiss, N.S.; de Boer, I.H. Clinical Manifestations of Kidney Disease Among US Adults with Diabetes, 1988–2014. JAMA 2016, 316, 602–610. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Wanner, C.; Inzucchi, S.E.; Zinman, B. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1801–1802. [Google Scholar] [CrossRef] [PubMed]
- Collaborative-Group, E.-K.; Herrington, W.G.; Staplin, N.; Wanner, C.; Green, J.B.; Hauske, S.J.; Emberson, J.R.; Preiss, D.; Judge, P.; Mayne, K.J.; et al. Empagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2023, 388, 117–127. [Google Scholar] [CrossRef]
- Tuttle, K.R.; Levin, A.; Nangaku, M.; Kadowaki, T.; Agarwal, R.; Hauske, S.J.; Elsasser, A.; Ritter, I.; Steubl, D.; Wanner, C.; et al. Safety of Empagliflozin in Patients with Type 2 Diabetes and Chronic Kidney Disease: Pooled Analysis of Placebo-Controlled Clinical Trials. Diabetes Care 2022, 45, 1445–1452. [Google Scholar] [CrossRef]
- Zelniker, T.A.; Wiviott, S.D.; Raz, I.; Im, K.; Goodrich, E.L.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Furtado, R.H.M.; et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: A systematic review and meta-analysis of cardiovascular outcome trials. Lancet 2019, 393, 31–39. [Google Scholar] [CrossRef]
- Wheeler, D.C.; James, J.; Patel, D.; Viljoen, A.; Ali, A.; Evans, M.; Fernando, K.; Hicks, D.; Milne, N.; Newland-Jones, P.; et al. SGLT2 Inhibitors: Slowing of Chronic Kidney Disease Progression in Type 2 Diabetes. Diabetes Ther. 2020, 11, 2757–2774. [Google Scholar] [CrossRef]
- Sugiyama, S.; Jinnouchi, H.; Yoshida, A.; Hieshima, K.; Kurinami, N.; Jinnouchi, K.; Tanaka, M.; Suzuki, T.; Miyamoto, F.; Kajiwara, K.; et al. Renoprotective Effects of Additional SGLT2 inhibitor Therapy in Patients With Type 2 Diabetes Mellitus and Chronic Kidney Disease Stages 3b-4: A Real World Report From A Japanese Specialized Diabetes Care Center. J. Clin. Med. Res. 2019, 11, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Htoo, P.T.; Tesfaye, H.; Schneeweiss, S.; Wexler, D.J.; Everett, B.M.; Glynn, R.J.; Kim, S.C.; Najafzadeh, M.; Koeneman, L.; Farsani, S.F.; et al. Comparative Effectiveness of Empagliflozin vs Liraglutide or Sitagliptin in Older Adults With Diverse Patient Characteristics. JAMA Netw. Open 2022, 5, e2237606. [Google Scholar] [CrossRef] [PubMed]
- Durcan, E.; Ozkan, S.; Saygi, H.I.; Dincer, M.T.; Korkmaz, O.P.; Sahin, S.; Karaca, C.; Sulu, C.; Bakir, A.; Ozkaya, H.M.; et al. Effects of SGLT2 inhibitors on patients with diabetic kidney disease: A preliminary study on the basis of podocyturia. J. Diabetes 2022, 14, 236–246. [Google Scholar] [CrossRef]
- Jung, K.J.; Jang, Y.; Oh, D.J.; Oh, B.H.; Lee, S.H.; Park, S.W.; Seung, K.B.; Kim, H.K.; Yun, Y.D.; Choi, S.H.; et al. The ACC/AHA 2013 pooled cohort equations compared to a Korean Risk Prediction Model for atherosclerotic cardiovascular disease. Atherosclerosis 2015, 242, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Bakker, L.E.; Sleddering, M.A.; Schoones, J.W.; Meinders, A.E.; Jazet, I.M. Pathogenesis of type 2 diabetes in South Asians. Eur. J. Endocrinol. 2013, 169, R99–R114. [Google Scholar] [CrossRef] [PubMed]
- Yabe, D.; Seino, Y.; Fukushima, M.; Seino, S. beta cell dysfunction versus insulin resistance in the pathogenesis of type 2 diabetes in East Asians. Curr. Diabetes Rep. 2015, 15, 602. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef]
- Yeung, R.O.; Zhang, Y.; Luk, A.; Yang, W.; Sobrepena, L.; Yoon, K.H.; Aravind, S.R.; Sheu, W.; Nguyen, T.K.; Ozaki, R.; et al. Metabolic profiles and treatment gaps in young-onset type 2 diabetes in Asia (the JADE programme): A cross-sectional study of a prospective cohort. Lancet Diabetes Endocrinol. 2014, 2, 935–943. [Google Scholar] [CrossRef]
- Chan, J.C.; So, W.Y.; Yeung, C.Y.; Ko, G.T.; Lau, I.T.; Tsang, M.W.; Lau, K.P.; Siu, S.C.; Li, J.K.; Yeung, V.T.; et al. Effects of structured versus usual care on renal endpoint in type 2 diabetes: The SURE study: A randomized multicenter translational study. Diabetes Care 2009, 32, 977–982. [Google Scholar] [CrossRef]
- Ma, R.C.; Chan, J.C. Type 2 diabetes in East Asians: Similarities and differences with populations in Europe and the United States. Ann. N. Y. Acad. Sci. 2013, 1281, 64–91. [Google Scholar] [CrossRef]
- Shah, A.; Kanaya, A.M. Diabetes and associated complications in the South Asian population. Curr. Cardiol. Rep. 2014, 16, 476. [Google Scholar] [CrossRef] [PubMed]
- Food-and-Drug-Administration-(FDA). Framework for FDA’s Real-World Evidence Program; FDA: Silver Spring, MD, USA, 2018.
- Food-and-Drug-Administration-(FDA). Submitting Documents Utilizing Real-World Data and Real-World Evidence to FDA for Drugs and Biologics. Available online: https://www.fda.gov/media/124795/download (accessed on 24 September 2021).
- Kim, J.A.; Yoon, S.; Kim, L.Y.; Kim, D.S. Towards Actualizing the Value Potential of Korea Health Insurance Review and Assessment (HIRA) Data as a Resource for Health Research: Strengths, Limitations, Applications, and Strategies for Optimal Use of HIRA Data. J. Korean Med. Sci. 2017, 32, 718–728. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Food-and-Drug-Administration-(FDA). Best Practices for Conducting and Reporting Pharmacoepidemiologic Safety Studies Using Electronic Healthcare Data; Guidance for Industry and FDA Staff; FDA: Silver Spring, MD, USA, 2013.
- Kim, Y.G.; Jeon, J.Y.; Han, S.J.; Kim, D.J.; Lee, K.W.; Kim, H.J. Sodium-glucose co-transporter-2 inhibitors and the risk of ketoacidosis in patients with type 2 diabetes mellitus: A nationwide population-based cohort study. Diabetes Obes. Metab. 2018, 20, 1852–1858. [Google Scholar] [CrossRef] [PubMed]
- Douros, A.; Lix, L.M.; Fralick, M.; Dell’Aniello, S.; Shah, B.R.; Ronksley, P.E.; Tremblay, E.; Hu, N.; Alessi-Severini, S.; Fisher, A.; et al. Sodium-Glucose Cotransporter-2 Inhibitors and the Risk for Diabetic Ketoacidosis: A Multicenter Cohort Study. Ann. Intern. Med. 2020, 173, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.F.; Chen, S.W.; Liu, J.R.; Li, P.R.; Wu, L.S.; Chang, S.H.; Yeh, Y.H.; Kuo, C.T.; Chan, Y.H.; See, L.C. Major adverse cardiovascular and limb events in patients with diabetes and concomitant peripheral artery disease treated with sodium glucose cotransporter 2 inhibitor versus dipeptidyl peptidase-4 inhibitor. Cardiovasc. Diabetol. 2020, 19, 160. [Google Scholar] [CrossRef] [PubMed]
- Seong, J.M.; Kim, J.J.; Kim, H.J.; Sohn, H.S. Comparison of heart failure risk and medical costs between patients with type 2 diabetes mellitus treated with dapagliflozin and dipeptidyl peptidase-4 inhibitors: A nationwide population-based cohort study. Cardiovasc. Diabetol. 2020, 19, 95. [Google Scholar] [CrossRef]
- Han, S.J.; Ha, K.H.; Lee, N.; Kim, D.J. Effectiveness and safety of sodium-glucose co-transporter-2 inhibitors compared with dipeptidyl peptidase-4 inhibitors in older adults with type 2 diabetes: A nationwide population-based study. Diabetes Obes. Metab. 2021, 23, 682–691. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice, C. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S125–S143. [Google Scholar] [CrossRef]
- Parsons, L.S. Reducing Bias in a Propensity Score Matched-Pair Sample Using Greedy Matching Techniques. Available online: http://www2.sas.com/proceedings/sugi26/p214-26.pdf (accessed on 1 January 2017).
- NCSS-Statistical-Software. Data Matching—Optimal and Greedy. Available online: http://ncss.wpengine.netdna-cdn.com/wp-content/themes/ncss/pdf/Procedures/NCSS/Data_Matching-Optimal_and_Greedy.pdf (accessed on 1 July 2017).
- Gerich, J.E. Role of the kidney in normal glucose homeostasis and in the hyperglycaemia of diabetes mellitus: Therapeutic implications. Diabet. Med. 2010, 27, 136–142. [Google Scholar] [CrossRef]
- Abdul-Ghani, M.A.; Norton, L.; DeFronzo, R.A. Renal sodium-glucose cotransporter inhibition in the management of type 2 diabetes mellitus. Am. J. Physiol. Renal Physiol. 2015, 309, F889–F900. [Google Scholar] [CrossRef] [PubMed]
- Bjornstad, P.; Laffel, L.; Tamborlane, W.V.; Simons, G.; Hantel, S.; von Eynatten, M.; George, J.; Marquard, J.; Cherney, D.Z.I. Acute Effect of Empagliflozin on Fractional Excretion of Sodium and eGFR in Youth with Type 2 Diabetes. Diabetes Care 2018, 41, e129–e130. [Google Scholar] [CrossRef] [PubMed]
- Vallon, V.; Richter, K.; Blantz, R.C.; Thomson, S.; Osswald, H. Glomerular hyperfiltration in experimental diabetes mellitus: Potential role of tubular reabsorption. J. Am. Soc. Nephrol. 1999, 10, 2569–2576. [Google Scholar] [CrossRef] [PubMed]
- Dahlquist, G.; Stattin, E.L.; Rudberg, S. Urinary albumin excretion rate and glomerular filtration rate in the prediction of diabetic nephropathy; a long-term follow-up study of childhood onset type-1 diabetic patients. Nephrol. Dial. Transplant. 2001, 16, 1382–1386. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Ghani, M.A.; DeFronzo, R.A. Inhibition of renal glucose reabsorption: A novel strategy for achieving glucose control in type 2 diabetes mellitus. Endocr. Pract. 2008, 14, 782–790. [Google Scholar] [CrossRef] [PubMed]
- Afkarian, M.; Sachs, M.C.; Kestenbaum, B.; Hirsch, I.B.; Tuttle, K.R.; Himmelfarb, J.; de Boer, I.H. Kidney disease and increased mortality risk in type 2 diabetes. J. Am. Soc. Nephrol. 2013, 24, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Neeland, I.J.; McGuire, D.K.; Chilton, R.; Crowe, S.; Lund, S.S.; Woerle, H.J.; Broedl, U.C.; Johansen, O.E. Empagliflozin reduces body weight and indices of adipose distribution in patients with type 2 diabetes mellitus. Diab Vasc. Dis. Res. 2016, 13, 119–126. [Google Scholar] [CrossRef]
- Lin, B.; Koibuchi, N.; Hasegawa, Y.; Sueta, D.; Toyama, K.; Uekawa, K.; Ma, M.; Nakagawa, T.; Kusaka, H.; Kim-Mitsuyama, S. Glycemic control with empagliflozin, a novel selective SGLT2 inhibitor, ameliorates cardiovascular injury and cognitive dysfunction in obese and type 2 diabetic mice. Cardiovasc. Diabetol. 2014, 13, 148. [Google Scholar] [CrossRef]
- Aroor, A.R.; Das, N.A.; Carpenter, A.J.; Habibi, J.; Jia, G.; Ramirez-Perez, F.I.; Martinez-Lemus, L.; Manrique-Acevedo, C.M.; Hayden, M.R.; Duta, C.; et al. Glycemic control by the SGLT2 inhibitor empagliflozin decreases aortic stiffness, renal resistivity index and kidney injury. Cardiovasc. Diabetol. 2018, 17, 108. [Google Scholar] [CrossRef]
- Vallon, V.; Gerasimova, M.; Rose, M.A.; Masuda, T.; Satriano, J.; Mayoux, E.; Koepsell, H.; Thomson, S.C.; Rieg, T. SGLT2 inhibitor empagliflozin reduces renal growth and albuminuria in proportion to hyperglycemia and prevents glomerular hyperfiltration in diabetic Akita mice. Am. J. Physiol. Renal Physiol. 2014, 306, F194–F204. [Google Scholar] [CrossRef]
- Lee, W.C.; Chau, Y.Y.; Ng, H.Y.; Chen, C.H.; Wang, P.W.; Liou, C.W.; Lin, T.K.; Chen, J.B. Empagliflozin Protects HK-2 Cells from High Glucose-Mediated Injuries via a Mitochondrial Mechanism. Cells 2019, 8, 1085. [Google Scholar] [CrossRef] [PubMed]
- Ndibalema, A.R.; Kabuye, D.; Wen, S.; Li, L.; Li, X.; Fan, Q. Empagliflozin Protects Against Proximal Renal Tubular Cell Injury Induced by High Glucose via Regulation of Hypoxia-Inducible Factor 1-Alpha. Diabetes Metab. Syndr. Obes. 2020, 13, 1953–1967. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.Y.L.; Low, S.; Yeoh, E.; Lim, E.K.; Renaud, C.J.; Teoh, S.T.Y.; Tan, G.F.L.; Chai, C.C.; Liu, B.; Subramaniam, T.; et al. A real-world study on SGLT2 inhibitors and diabetic kidney disease progression. Clin. Kidney J. 2022, 15, 1403–1414. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.C.; Wat, N.M.; So, W.Y.; Lam, K.S.; Chua, C.T.; Wong, K.S.; Morad, Z.; Dickson, T.Z.; Hille, D.; Zhang, Z.; et al. Renin angiotensin aldosterone system blockade and renal disease in patients with type 2 diabetes. An Asian perspective from the RENAAL Study. Diabetes Care 2004, 27, 874–879. [Google Scholar] [CrossRef] [PubMed]
- Tu, W.; Eckert, G.J.; Hannon, T.S.; Liu, H.; Pratt, L.M.; Wagner, M.A.; Dimeglio, L.A.; Jung, J.; Pratt, J.H. Racial differences in sensitivity of blood pressure to aldosterone. Hypertension 2014, 63, 1212–1218. [Google Scholar] [CrossRef] [PubMed]
- Kadowaki, T.; Nangaku, M.; Hantel, S.; Okamura, T.; von Eynatten, M.; Wanner, C.; Koitka-Weber, A. Empagliflozin and kidney outcomes in Asian patients with type 2 diabetes and established cardiovascular disease: Results from the EMPA-REG OUTCOME((R)) trial. J. Diabetes Investig. 2019, 10, 760–770. [Google Scholar] [CrossRef] [PubMed]
- Sarashina, A.; Ueki, K.; Sasaki, T.; Tanaka, Y.; Koiwai, K.; Sakamoto, W.; Woerle, H.J.; Salsali, A.; Broedl, U.C.; Macha, S. Effect of renal impairment on the pharmacokinetics, pharmacodynamics, and safety of empagliflozin, a sodium glucose cotransporter 2 inhibitor, in Japanese patients with type 2 diabetes mellitus. Clin. Ther. 2014, 36, 1606–1615. [Google Scholar] [CrossRef]
- Macha, S.; Mattheus, M.; Halabi, A.; Pinnetti, S.; Woerle, H.J.; Broedl, U.C. Pharmacokinetics, pharmacodynamics and safety of empagliflozin, a sodium glucose cotransporter 2 (SGLT2) inhibitor, in subjects with renal impairment. Diabetes Obes. Metab. 2014, 16, 215–222. [Google Scholar] [CrossRef]
- Jang, H.Y.; Kim, I.W.; Oh, J.M. Using real-world data for supporting regulatory decision making: Comparison of cardiovascular and safety outcomes of an empagliflozin randomized clinical trial versus real-world data. Front. Pharmacol. 2022, 13, 928121. [Google Scholar] [CrossRef]
- Cahn, A.; Melzer-Cohen, C.; Pollack, R.; Chodick, G.; Shalev, V. Acute renal outcomes with sodium-glucose co-transporter-2 inhibitors: Real-world data analysis. Diabetes Obes. Metab. 2019, 21, 340–348. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Karasik, A.; Thuresson, M.; Melzer-Cohen, C.; Chodick, G.; Khunti, K.; Wilding, J.P.H.; Garcia Rodriguez, L.A.; Cea-Soriano, L.; Kohsaka, S.; et al. Kidney outcomes associated with use of SGLT2 inhibitors in real-world clinical practice (CVD-REAL 3): A multinational observational cohort study. Lancet Diabetes Endocrinol. 2020, 8, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Koh, E.S.; Han, K.; Nam, Y.S.; Wittbrodt, E.T.; Fenici, P.; Kosiborod, M.N.; Heerspink, H.J.L.; Yoo, S.J.; Kwon, H.S. Renal outcomes and all-cause death associated with sodium-glucose co-transporter-2 inhibitors versus other glucose-lowering drugs (CVD-REAL 3 Korea). Diabetes Obes. Metab. 2021, 23, 455–466. [Google Scholar] [CrossRef] [PubMed]
- Nadkarni, G.N.; Ferrandino, R.; Chang, A.; Surapaneni, A.; Chauhan, K.; Poojary, P.; Saha, A.; Ferket, B.; Grams, M.E.; Coca, S.G. Acute Kidney Injury in Patients on SGLT2 Inhibitors: A Propensity-Matched Analysis. Diabetes Care 2017, 40, 1479–1485. [Google Scholar] [CrossRef] [PubMed]
- Toulis, K.A.; Bilezikian, J.P.; Thomas, G.N.; Hanif, W.; Kotsa, K.; Thayakaran, R.; Keerthy, D.; Tahrani, A.A.; Nirantharakumar, K. Initiation of dapagliflozin and treatment-emergent fractures. Diabetes Obes. Metab. 2018, 20, 1070–1074. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Sitagliptin n = 6170 | Empagliflozin n = 6170 | STD |
|---|---|---|---|
| Sex, male | 3534 (57.3) | 3464 (56.1) | −0.02 |
| Age, year | 50.8 ± 12.8 | 50.9 ± 12.1 | 0.01 |
| Normal | 5842 (94.7) | 5846 (94.8) | 0.004 |
| Medicaid | 307 (5) | 304 (4.9) | |
| No charge | 21 (0.3) | 20 (0.3) | |
| Number of inpatient visits | 0.5 ± 1.3 | 0.5 ± 1.3 | 0.003 |
| Number of outpatient visits | 29.0 ± 28.4 | 29.0 ± 28.4 | 0.002 |
| Index year | |||
| 2016 | 1545 (25) | 1564 (25.4) | 0.02 |
| 2017 | 3106 (50.3) | 3057 (49.6) | |
| 2018 | 1519 (24.6) | 1549 (25.1) | |
| Charlson comorbidity index | |||
| 0 | 2 (0) | 1 (0) | 0.02 |
| 1 | 416 (6.7) | 408 (6.6) | |
| 2 | 503 (8.2) | 523 (8.5) | |
| 3 | 5249 (85.1) | 5238 (84.9) | |
| CV risk factor | |||
| CAD | 1946 (31.5) | 2054 (33.3) | 0.04 |
| Multi vessel CAD | 1080 (17.5) | 1126 (18.3) | 0.02 |
| MI | 110 (1.8) | 95 (1.5) | −0.02 |
| CABG | 444 (7.2) | 430 (7) | −0.01 |
| Stroke | 190 (3.1) | 181 (2.9) | −0.01 |
| PAD | 170 (2.8) | 148 (2.4) | −0.02 |
| DM circulation | 1078 (17.5) | 1083 (17.6) | 0.002 |
| DM foot | 0 (0.0) | 0 (0.0) | 0 |
| DM nephropathy | 5789 (93.8) | 5828 (94.5) | 0.03 |
| DM neuropathy | 1111 (18) | 1089 (17.7) | −0.01 |
| DM other complications | 4101 (66.5) | 4085 (66.2) | −0.01 |
| Hyperglycemia | 126 (2) | 140 (2.3) | 0.02 |
| CV risk factor | |||
| Hypertension | 4312 (69.9) | 4330 (70.2) | 0.006 |
| Edema | 704 (11.4) | 696 (11.3) | −0.004 |
| Kidney stone | 120 (1.9) | 123 (2.0) | 0.004 |
| Osteoarthritis | 1832 (29.7) | 1808 (29.3) | −0.01 |
| Other arthritis | 1672 (27.1) | 1698 (27.5) | 0.01 |
| PUD | 1619 (26.2) | 1596 (25.9) | −0.01 |
| Pancreatitis | 126 (2) | 124 (2) | −0.002 |
| UC | 12 (0.2) | 9 (0.2) | −0.01 |
| Crohn | 3 (0.1) | 4 (0.1) | 0.000 |
| Asthma | 946 (15.3) | 899 (14.6) | −0.02 |
| COPD | 182 (3) | 164 (2.7) | −0.02 |
| Bladder stone | 2 (0) | 3 (0.1) | 0.01 |
| Dementia | 516 (8.4) | 525 (8.5) | 0.005 |
| Electrolyte imbalance | 576 (9.3) | 617 (10) | 0.02 |
| Glaucoma/cataract | 1775 (28.8) | 1766 (28.6) | −0.003 |
| HONK | 40 (0.7) | 44 (0.7) | 0.01 |
| HTN nephropathy | 354 (5.7) | 377 (6.1) | 0.02 |
| Hyperthyroid disease | 170 (2.8) | 175 (2.8) | 0.005 |
| Hypothyroid disease | 722 (11.7) | 685 (11.1) | −0.02 |
| Osteomyelitis | 32 (0.5) | 38 (0.6) | 0.01 |
| Pneumonia | 493 (8) | 457 (7.4) | −0.02 |
| Skin infection | 296 (4.8) | 290 (4.7) | −0.005 |
| Metformin | 4731 (76.7) | 4752 (77) | 0.008 |
| Insulins | 1575 (25.5) | 1620 (26.3) | 0.02 |
| SUs | 3154 (51.1) | 3178 (51.5) | 0.01 |
| Glitazones | 978 (15.9) | 954 (15.5) | −0.01 |
| GLP-1 agonists | 65 (1.1) | 78 (1.3) | 0.02 |
| AGIs | 225 (3.7) | 195 (3.2) | −0.03 |
| Meglitinides | 98 (1.6) | 113 (1.8) | 0.02 |
| Anticoagulants | 2837 (46) | 2825 (45.8) | 0.01 |
| Antiplatelets | 2783 (45.1) | 2768 (44.9) | −0.05 |
| Heparins | 190 (3.1) | 182 (3) | −0.01 |
| Thrombolytics | 3 (0.1) | 3 (0.1) | 0.01 |
| Statins | 4750 (77) | 4775 (77.4) | 0.01 |
| Other lipid lowerings | 1129 (18.3) | 1165 (18.9) | 0.01 |
| Nitrates | 451 (7.3) | 443 (7.2) | −0.005 |
| Digoxin | 392 (6.4) | 391 (6.3) | −0.001 |
| ACEIs | 255 (4.1) | 252 (4.1) | −0.002 |
| ARBs | 3752 (60.8) | 3723 (60.3) | −0.01 |
| Entresto | 0 (0) | 2 (0) | 0.03 |
| Other anti-HTNs | 3009 (48.8) | 2995 (48.5) | −0.005 |
| Loop diuretics | 638 (10.3) | 632 (10.2) | −0.003 |
| Other diuretics | 1509 (24.5) | 1469 (23.8) | −0.02 |
| Antianxieties | 2131 (34.5) | 2176 (35.3) | 0.02 |
| Antipsychotics | 163 (2.6) | 168 (2.7) | 0.005 |
| Antidepressants | 891 (14.4) | 893 (14.5) | 0.001 |
| Dementia | 516 (8.4) | 525 (8.5) | 0.005 |
| Antiparkinsons | 114 (1.9) | 117 (1.9) | 0.004 |
| Anticonvulsants | 90 (1.5) | 90 (1.5) | 0 |
| NSAIDs | 4828 (78.3) | 4779 (77.5) | −0.02 |
| Bisphosphonates | 140 (2.3) | 156 (2.5) | 0.02 |
| Opioids | 2610 (42.3) | 2639 (42.8) | 0.01 |
| Events | Person-Year | Hazard Ratio (95% CI) | ||
|---|---|---|---|---|
| Unadjusted | Adjusted | |||
| MACEs | ||||
| Sitagliptin | 470 | 16,824 | ||
| Empagliflozin | 342 | 16,945 | 0.72 (0.63, 0.83) * | 0.74 (0.64, 0.85) * |
| All-cause death | ||||
| Sitagliptin | 96 | 12,391 | ||
| Empagliflozin | 43 | 12,814 | 0.43 (0.30, 0.62) * | 0.47 (0.33, 0.68) * |
| Myocardial infarction | ||||
| Sitagliptin | 120 | 17,104 | ||
| Empagliflozin | 74 | 17,320 | 0.61 (0.46, 0.82) * | 0.60 (0.45, 0.81) * |
| Stroke | ||||
| Sitagliptin | 179 | 16,568 | ||
| Empagliflozin | 161 | 16,765 | 0.89 (0.71, 1.10) | 0.92 (0.74, 1.13) |
| Hospitalization for unstable angina | ||||
| Sitagliptin | 364 | 15,428 | ||
| Empagliflozin | 254 | 15,829 | 0.68 (0.58, 0.80) * | 0.67 (0.57, 0.79) * |
| Coronary revascularization | ||||
| Sitagliptin | 220 | 15,670 | ||
| Empagliflozin | 178 | 15,851 | 0.80 (0.65, 0.98) * | 0.79 (0.65, 0.97) * |
| Transient ischemic attack | ||||
| Sitagliptin | 143 | 16,422 | ||
| Empagliflozin | 131 | 16,552 | 0.91 (0.72, 1.15) | 0.92 (0.72, 1.17) |
| Hospitalization for heart failure | ||||
| Sitagliptin | 265 | 16,334 | ||
| Empagliflozin | 175 | 16,640 | 0.65 (0.54, 0.79) * | 0.66 (0.55, 0.80) * |
| Hypoglycemic adverse event | ||||
| Sitagliptin | 177 | 16,431 | ||
| Empagliflozin | 138 | 16,666 | 0.77 (0.62, 0.96) * | 0.78 (0.62, 0.97) * |
| Urinary tract infections | ||||
| Sitagliptin | 1112 | 9909 | ||
| Empagliflozin | 1032 | 10,231 | 0.90 (0.83, 0.98) * | 0.90 (0.82, 0.98) * |
| Genital infections | ||||
| Sitagliptin | 459 | 12,300 | ||
| Empagliflozin | 639 | 12,025 | 1.42 (1.26, 1.60) * | 1.43 (1.27, 1.61) * |
| Acute kidney injury | ||||
| Sitagliptin | 168 | 16,402 | ||
| Empagliflozin | 159 | 16,647 | 0.94 (0.75, 1.16) | 0.94 (0.76, 1.17) |
| Volume depletion | ||||
| Sitagliptin | 413 | 15,336 | ||
| Empagliflozin | 375 | 15,436 | 0.90 (0.78, 1.04) | 0.90 (0.78, 1.04) |
| Diabetic ketoacidosis | ||||
| Sitagliptin | 35 | 17,089 | ||
| Empagliflozin | 34 | 17,221 | 0.96 (0.60, 1.54) | 0.96 (0.60, 1.54) |
| Thromboembolic event | ||||
| Sitagliptin | 257 | 16,042 | ||
| Empagliflozin | 226 | 16,227 | 0.87 (0.73, 1.04) | 0.88 (0.73, 1.05) |
| Fracture | ||||
| Sitagliptin | 667 | 13,200 | ||
| Empagliflozin | 684 | 13,337 | 1.02 (0.91, 1.13) | 1.03 (0.92, 1.14) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, H.Y.; Kim, I.-W.; Oh, J.M. Comparative Safety Analysis of Empagliflozin in Type 2 Diabetes Mellitus Patients with Chronic Kidney Disease versus Normal Kidney Function: A Nationwide Cohort Study in Korea. Pharmaceutics 2023, 15, 2394. https://doi.org/10.3390/pharmaceutics15102394
Jang HY, Kim I-W, Oh JM. Comparative Safety Analysis of Empagliflozin in Type 2 Diabetes Mellitus Patients with Chronic Kidney Disease versus Normal Kidney Function: A Nationwide Cohort Study in Korea. Pharmaceutics. 2023; 15(10):2394. https://doi.org/10.3390/pharmaceutics15102394
Chicago/Turabian StyleJang, Ha Young, In-Wha Kim, and Jung Mi Oh. 2023. "Comparative Safety Analysis of Empagliflozin in Type 2 Diabetes Mellitus Patients with Chronic Kidney Disease versus Normal Kidney Function: A Nationwide Cohort Study in Korea" Pharmaceutics 15, no. 10: 2394. https://doi.org/10.3390/pharmaceutics15102394