

Association between Genetic Polymorphisms and Bleeding in Patients on Direct Oral Anticoagulants

Abstract
:1. Introduction
2. Methods
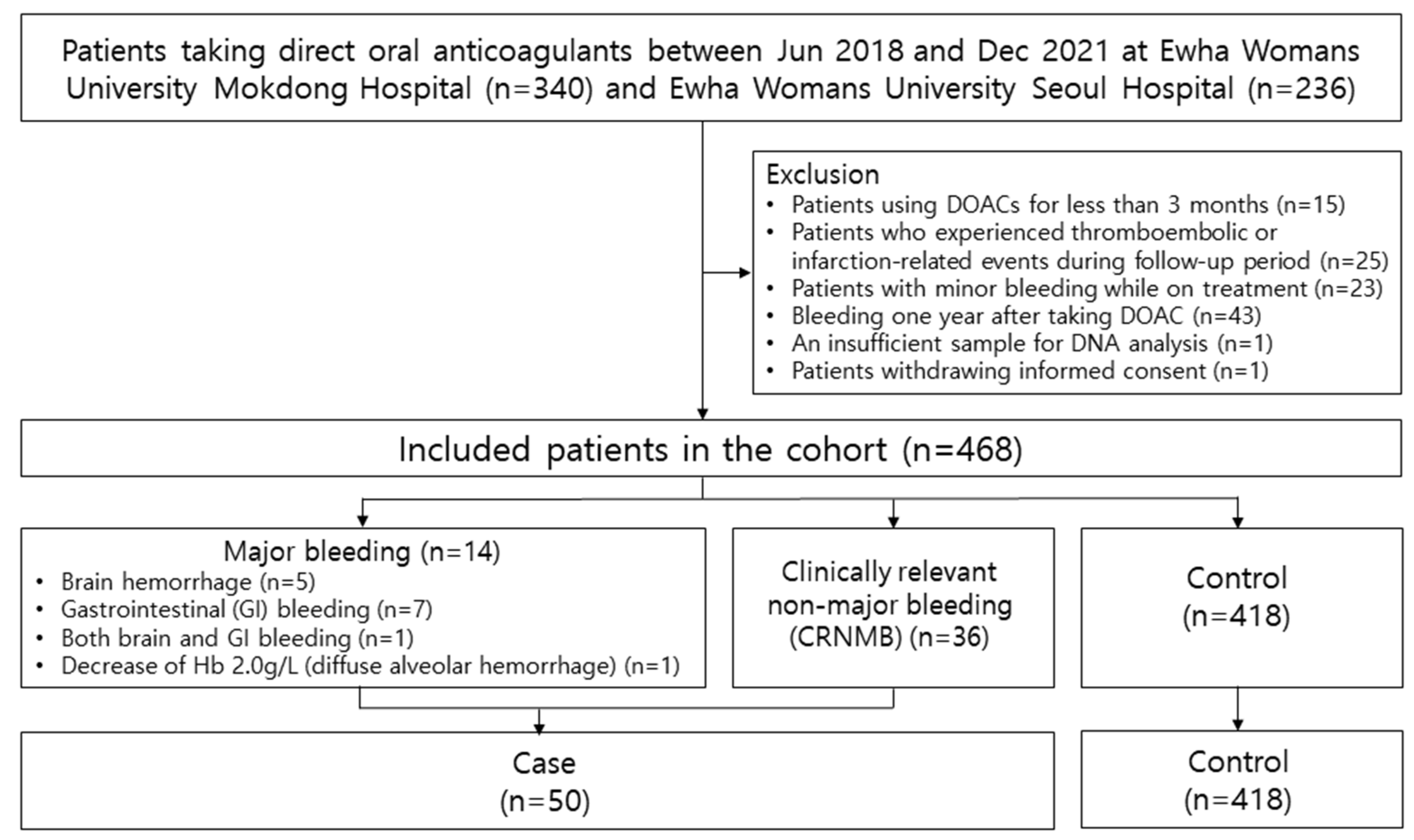
2.1. Study Patients and Data Collection
2.2. Selection of Single Nucleotide Polymorphisms (SNPs) and Genotyping
2.3. Statistical Analysis
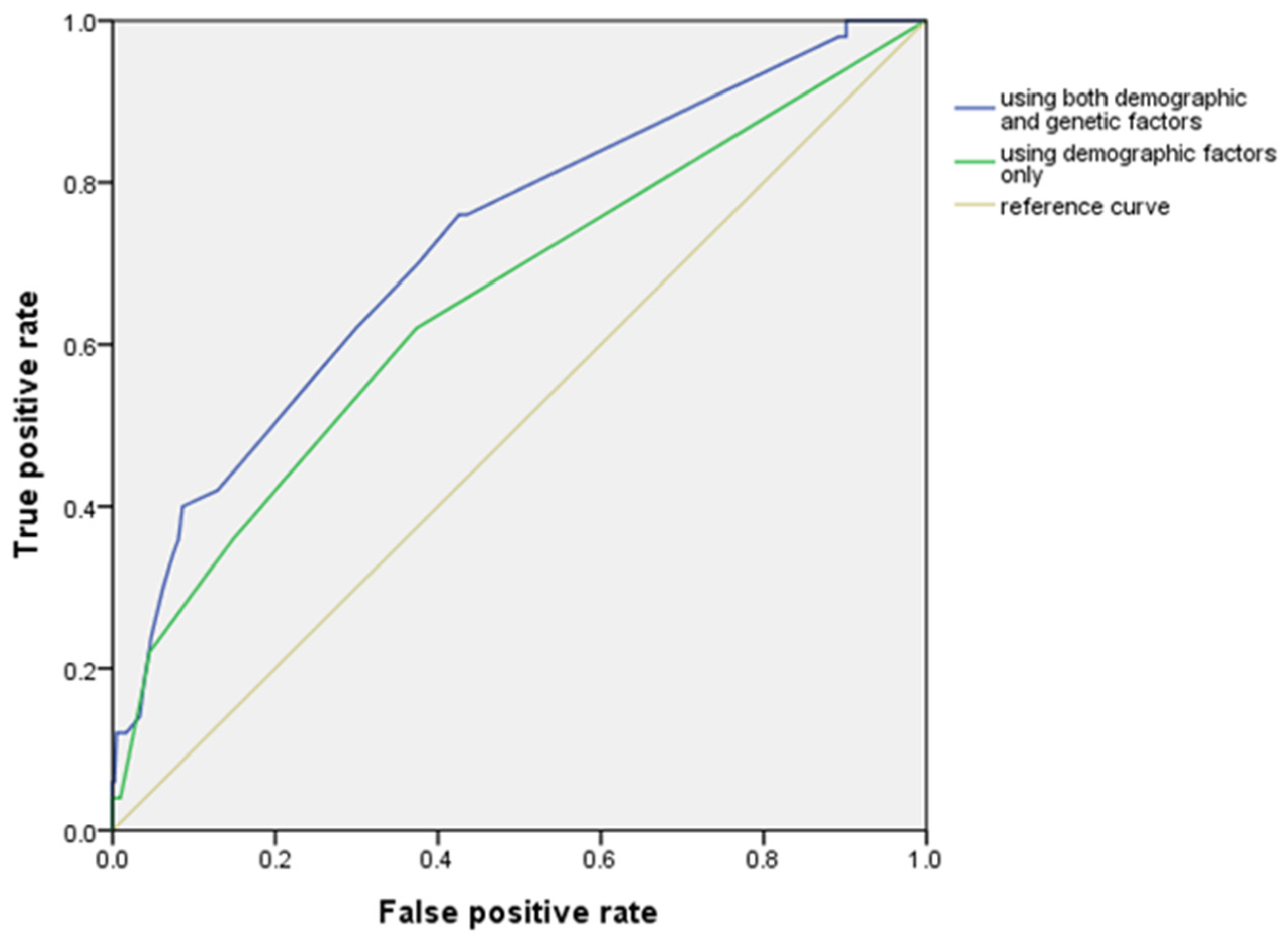
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deutsch, D.; Boustière, C.; Ferrari, E.; Albaladejo, P.; Morange, P.-E.; Benamouzig, R. Direct oral anticoagulants and digestive bleeding: Therapeutic management and preventive measures. Ther. Adv. Gastroenterol. 2017, 10, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Gong, I.Y.; Kim, R.B. Importance of Pharmacokinetic Profile and Variability as Determinants of Dose and Response to Dabigatran, Rivaroxaban, and Apixaban. Can. J. Cardiol. 2013, 29 (Suppl. 7), S24–S33. [Google Scholar] [CrossRef] [PubMed]
- Chan, N.; Sager, P.T.; Lawrence, J.; Ortel, T.; Reilly, P.; Berkowitz, S.; Kubitza, D.; Eikelboom, J.; Florian, J.; Stockbridge, N.; et al. Is there a role for pharmacokinetic/pharmacodynamic-guided dosing for novel oral anticoagulants? Am. Heart J. 2018, 199, 59–67. [Google Scholar] [CrossRef]
- Li, A.; Li, M.K.; Crowther, M.; Vazquez, S.R. Drug-drug interactions with direct oral anticoagulants associated with adverse events in the real world: A systematic review. Thromb. Res. 2020, 194, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Wanat, M.A. Novel Oral Anticoagulants: A Review of New Agents. Postgrad. Med. 2013, 125, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Raymond, J.; Imbert, L.; Cousin, T.; Duflot, T.; Varin, R.; Wils, J.; Lamoureux, F. Pharmacogenetics of Direct Oral Anticoagulants: A Systematic Review. J. Pers. Med. 2021, 11, 37. [Google Scholar] [CrossRef] [PubMed]
- Sennesael, A.-L.; Panin, N.; Vancraeynest, C.; Pochet, L.; Spinewine, A.; Haufroid, V.; Elens, L. Effect of ABCB1 genetic polymorphisms on the transport of rivaroxaban in HEK293 recombinant cell lines. Sci. Rep. 2018, 8, 10514. [Google Scholar] [CrossRef] [PubMed]
- Lorenzini, K.I.; Daali, Y.; Fontana, P.; Desmeules, J.; Samer, C. Rivaroxaban-Induced Hemorrhage Associated with ABCB1 Genetic Defect. Front. Pharmacol. 2016, 7, 494. [Google Scholar] [CrossRef]
- Dimatteo, C.; D’Andrea, G.; Vecchione, G.; Paoletti, O.; Tiscia, G.L.; Santacroce, R.; Correale, M.; Brunetti, N.; Grandone, E.; Testa, S.; et al. ABCB1 SNP rs4148738 modulation of apixaban interindividual variability. Thromb. Res. 2016, 145, 24–26. [Google Scholar] [CrossRef]
- Ueshima, S.; Hira, D.; Fujii, R.; Kimura, Y.; Tomitsuka, C.; Yamane, T.; Tabuchi, Y.; Ozawa, T.; Itoh, H.; Horie, M.; et al. Impact of ABCB1, ABCG2, and CYP3A5 polymorphisms on plasma trough concentrations of apixaban in Japanese patients with atrial fibrillation. Pharm. Genom. 2017, 27, 329–336. [Google Scholar] [CrossRef]
- Mehta, A.; Shapiro, M.D. Apolipoproteins in vascular biology and atherosclerotic disease. Nat. Rev. Cardiol. 2022, 19, 168–179. [Google Scholar] [CrossRef]
- Yee, J.; Kim, W.; Chang, B.C.; Chung, J.E.; Lee, K.E.; Gwak, H.S. APOB gene polymorphisms may affect the risk of minor or minimal bleeding complications in patients on warfarin maintaining therapeutic INR. Eur. J. Hum. Genet. 2019, 27, 1542–1549. [Google Scholar] [CrossRef]
- Riddell, D.R.; Graham, A.; Owen, J.S. Apolipoprotein E inhibits platelet aggregation through the L-arginine: Nitric oxide pathway. Implications for vascular disease. J. Biol. Chem. 1997, 272, 89–95. [Google Scholar] [CrossRef]
- Sudlow, C.; Martínez González, N.A.; Kim, J.; Clark, C. Does apolipoprotein E genotype influence the risk of ischemic stroke, intracerebral hemorrhage, or subarachnoid hemorrhage? Systematic review and meta-analyses of 31 studies among 5961 cases and 17,965 controls. Stroke 2006, 37, 364–370. [Google Scholar] [CrossRef]
- Svensson, E.H.; Abul-Kasim, K.; Engström, G.; Söderholm, M. Risk factors for intracerebral haemorrhage—Results from a prospective population-based study. Eur. Stroke J. 2020, 5, 278–285. [Google Scholar] [CrossRef]
- Gao, X.; Cai, X.; Yang, Y.; Zhou, Y.; Zhu, W. Diagnostic Accuracy of the HAS-BLED Bleeding Score in VKA- or DOAC-Treated Patients With Atrial Fibrillation: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2021, 8, 757087. [Google Scholar] [CrossRef]
- Tchen, S.; Ryba, N.; Patel, V.; Cavanaugh, J.; Sullivan, J.B. Validation of bleeding risk prediction scores for patients with major bleeding on direct oral anticoagulants. Ann. Pharmacother. 2020, 54, 1175–1184. [Google Scholar] [CrossRef]
- Apostolakis, S.; Lane, D.A.; Guo, Y.; Buller, H.; Lip, G.Y. Performance of the HEMORR2HAGES, ATRIA, and HAS-BLED bleeding risk-prediction scores in patients with atrial fibrillation undergoing anticoagulation: The AMADEUS (evaluating the use of SR34006 compared to warfarin or acenocoumarol in patients with atrial fibrillation) Study. J. Am. Coll. Cardiol. 2012, 60, 861–867. [Google Scholar]
- Schulman, S.; Kearon, C.; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef]
- Kaatz, S.; Ahmad, D.; Spyropoulos, A.C.; Schulman, S. Subcommittee on Control of Anticoagulation. Definition of clinically relevant non-major bleeding in studies of anticoagulants in atrial fibrillation and venous thromboembolic disease in non-surgical patients: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2015, 13, 2119–2126. [Google Scholar] [CrossRef]
- Lip, G.Y.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; de Vos, C.B.; Crijns, H.J.; Lip, G.Y. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: The Euro Heart Survey. Chest 2010, 138, 1093–1100. [Google Scholar] [CrossRef] [PubMed]
- Ward, L.D.; Kellis, M. HaploReg v4: Systematic mining of putative causal variants, cell types, regulators and target genes for human complex traits and disease. Nucleic Acids Res. 2016, 44, D877–D881. [Google Scholar] [CrossRef] [PubMed]
- Gow, J.M.; Hodges, L.M.; Chinn, L.W.; Kroetz, D.L. Substrate-dependent effects of human ABCB1 coding polymorphisms. J. Pharmacol. Exp. Ther. 2008, 325, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Cen, H.; Wen, Q.-W.; Zhang, H.-Q.; Yu, H.; Zeng, Z.; Jin, T.; Wang, T.-H.; Qin, W.; Huang, H.; Wu, X.-D. Associations Between Genetic Polymorphisms Within Transporter Genes and Clinical Response to Methotrexate in Chinese Rheumatoid Arthritis Patients: A Pilot Study. Pharm. Pers. Med. 2022, 15, 327–339. [Google Scholar] [CrossRef] [PubMed]
- Mukonzo, J.K.; Röshammar, D.; Waako, P.; Andersson, M.; Fukasawa, T.; Milani, L.; Svensson, J.O.; Ogwal-Okeng, J.; Gustafsson, L.L.; Aklillu, E. A novel polymorphism in ABCB1 gene, CYP2B6*6 and sex predict single-dose efavirenz population pharmacokinetics in Ugandans. Br. J. Clin. Pharmacol. 2009, 68, 690–699. [Google Scholar] [CrossRef] [PubMed]
- Xie, Q.; Xiang, Q.; Mu, G.; Ma, L.; Chen, S.; Zhou, S.; Hu, K.; Zhang, Z.; Cui, Y.; Jiang, J. Effect of ABCB1 Genotypes on the Pharmacokinetics and Clinical Outcomes of New Oral Anticoagulants: A Systematic Review and Meta-analysis. Curr. Pharm. Des. 2018, 24, 3558–3565. [Google Scholar] [CrossRef]
- Lähteenmäki, J.; Vuorinen, A.; Pajula, J.; Harno, K.; Lehto, M.; Niemi, M.; van Gils, M. Pharmacogenetics of Bleeding and Thromboembolic Events in Direct Oral Anticoagulant Users. Clin. Pharmacol. Ther. 2021, 110, 768–776. [Google Scholar] [CrossRef]
- Behbodikhah, J.; Ahmed, S.; Elyasi, A.; Kasselman, L.J.; De Leon, J.; Glass, A.D.; Reiss, A.B. Apolipoprotein B and Cardiovascular Disease: Biomarker and Potential Therapeutic Target. Metabolites 2021, 11, 690. [Google Scholar] [CrossRef]
- Zhou, Y.; Mägi, R.; Milani, L.; Lauschke, V.M. Global genetic diversity of human apolipoproteins and effects on cardiovascular disease risk. J. Lipid Res. 2018, 59, 1987–2000. [Google Scholar] [CrossRef]
- Li, D.; Luo, Z.-Y.; Chen, Y.; Zhu, H.; Song, G.-B.; Zhou, X.-M.; Yan, H.; Zhou, H.-H.; Zhang, W.; Li, X. LRP1 and APOA1 Polymorphisms: Impact on Warfarin International Normalized Ratio-Related Phenotypes. J. Cardiovasc. Pharmacol. 2020, 76, 71–76. [Google Scholar] [CrossRef]
- Niu, C.; Luo, Z.; Yu, L.; Yang, Y.; Chen, Y.; Luo, X.; Lai, F.; Song, Y. Associations of the APOB rs693 and rs17240441 polymorphisms with plasma APOB and lipid levels: A meta-analysis. Lipids Health Dis. 2017, 16, 166. [Google Scholar] [CrossRef]
- Zhu, H.; Yu, L.; Feng, L. Association of apolipoprotein B XbaI (rs693) polymorphism and gallstone disease risk based on a comprehensive analysis. Genes Environ. 2021, 43, 17. [Google Scholar] [CrossRef]
- Liu, X.; Wang, Y.; Qu, H.; Hou, M.; Cao, W.; Ma, Z.; Wang, H. Associations of polymorphisms of rs693 and rs1042031 in apolipoprotein B gene with risk of breast cancer in Chinese. Jpn. J. Clin. Oncol. 2013, 43, 362–368. [Google Scholar] [CrossRef]
- Wang, Y.-T.; Li, Y.; Ma, Y.-T.; Yang, Y.-N.; Ma, X.; Li, X.-M.; Liu, F.; Chen, B.-D. Association between apolipoprotein B genetic polymorphism and the risk of calcific aortic stenosis in Chinese subjects, in Xinjiang, China. Lipids Health Dis. 2018, 17, 40. [Google Scholar] [CrossRef]
- Starčević, J.N.; Letonja, M..; Pražnikar, Z.J.; Makuc, J.; Vujkovac, A.C.; Petrovič, D. Polymorphisms XbaI (rs693) and EcoRI (rs1042031) of the ApoB gene are associated with carotid plaques but not with carotid intima-media thickness in patients with diabetes mellitus type 2. Vasa 2014, 43, 171–180. [Google Scholar] [CrossRef]
- Yao, X.; Shah, N.D.; Sangaralingham, L.R.; Gersh, B.J.; Noseworthy, P.A. Non-Vitamin K Antagonist Oral Anticoagulant Dosing in Patients With Atrial Fibrillation and Renal Dysfunction. J. Am. Coll. Cardiol. 2017, 69, 2779–2790. [Google Scholar] [CrossRef]
- Gaikwad, T.; Ghosh, K.; Shetty, S. VKORC1 and CYP2C9 genotype distribution in Asian countries. Thromb. Res. 2014, 134, 537–544. [Google Scholar] [CrossRef]
- Liu, X.; Huang, M.; Ye, C.; Zeng, J.; Zeng, C.; Ma, J. The role of non-vitamin K antagonist oral anticoagulants in Asian patients with atrial fibrillation: A PRISMA-compliant article. Medicine 2020, 99, e21025.28. [Google Scholar] [CrossRef]
- Chao, T.-F.; Chen, S.-A.; Ruff, C.T.; Hamershock, R.A.; Mercuri, M.F.; Antman, E.M.; Braunwald, E.; Giugliano, R.P. Clinical outcomes, edoxaban concentration, and anti-factor Xa activity of Asian patients with atrial fibrillation compared with non-Asians in the ENGAGE AF-TIMI 48 trial. Eur. Heart J. 2019, 40, 1518–1527. [Google Scholar] [CrossRef]
- Wolfe, Z.; Nasir, F.; Subramanian, C.R.; Lash, B.; Khan, S.U. A systematic review and Bayesian network meta-analysis of risk of intracranial hemorrhage with direct oral anticoagulants. J. Thromb. Haemost. 2018, 16, 1296–1306. [Google Scholar] [CrossRef] [PubMed]
- Bensi, C.; Belli, S.; Paradiso, D.; Lomurno, G. Postoperative bleeding risk of direct oral anticoagulants after oral surgery procedures: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2018, 47, 923–932. [Google Scholar] [CrossRef] [PubMed]
- Aryal, M.R.; Gosain, R.; Donato, A.; Yu, H.; Katel, A.; Bhandari, Y.; Dhital, R.; Kouides, P.A. Systematic review and meta-analysis of the efficacy and safety of apixaban compared to rivaroxaban in acute VTE in the real world. Blood Adv. 2019, 3, 2381–2387. [Google Scholar] [CrossRef] [PubMed]
- Lobraico-Fernandez, J.; Baksh, S.; Nemec, E. Elderly Bleeding Risk of Direct Oral Anticoagulants in Nonvalvular Atrial Fibrillation: A Systematic Review and Meta-Analysis of Cohort Studies. Drugs R D 2019, 19, 235–245. [Google Scholar] [CrossRef]
- Westenbrink, B.D.; Alings, M.; Granger, C.B.; Alexander, J.H.; Lopes, R.D.; Hylek, E.M.; Thomas, L.; Wojdyla, D.M.; Hanna, M.; Keltai, M.; et al. Anemia is associated with bleeding and mortality, but not stroke, in patients with atrial fibrillation: Insights from the Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) trial. Am. Heart J. 2017, 185, 140–149. [Google Scholar] [CrossRef]
- Tu, S.J.; Hanna-Rivero, N.; Elliott, A.D.; Clarke, N.; Huang, S.; Pitman, B.M.; Gallagher, C.; Linz, D.; Mahajan, R.; Lau, D.H.; et al. Associations of anemia with stroke, bleeding, and mortality in atrial fibrillation: A systematic review and meta-analysis. J. Cardiovasc. Electrophysiol. 2021, 32, 686–694. [Google Scholar] [CrossRef]
- Whirl-Carrillo, M.; McDonagh, E.M.; Hebert, J.M.; Gong, L.; Sangkuhl, K.; Thorn, C.F.; Altman, R.B.; Klein, T.E. Pharmacogenomics knowledge for personalized medicine. Clin. Pharmacol. Ther. 2012, 92, 414–417. [Google Scholar] [CrossRef]
- Ruíz-Giménez, N.; Suárez, C.; González, R.; Nieto, J.A.; Todolí, J.A.; Samperiz, Á.L.; Monreal, M.; The RIETE Investigators Predictive variables for major bleeding events in patients presenting with documented acute venous thromboembolism. Findings from the RIETE Registry. Thromb. Haemost. 2008, 100, 26–31. [Google Scholar] [CrossRef]
- Yoshida, R.; Ishii, H.; Morishima, I.; Tanaka, A.; Morita, Y.; Takagi, K.; Yoshioka, N.; Hirayama, K.; Iwakawa, N.; Tashiro, H.; et al. Performance of HAS-BLED, ORBIT, PRECISE-DAPT, and PARIS risk score for predicting long-term bleeding events in patients taking an oral anticoagulant undergoing percutaneous coronary intervention. J. Cardiol. 2019, 73, 479–487. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Bleeding (n = 50) | No Bleeding (n = 418) | p |
|---|---|---|---|
| Sex | 0.93 | ||
| Female | 19 (38.0) | 156 (37.3) | |
| Male | 31 (62.0) | 262 (62.7) | |
| Age (years) | 69.32 ± 9.28 | 69.12 ± 0.50 | 0.90 |
| <65 | 16 (32.0) | 125 (29.9) | 0.76 |
| ≥65 | 34 (68.0) | 293 (70.1) | |
| BMI (kg/m2) | 25.48 ± 3.94 | 24.97 ± 3.38 | 0.34 |
| <25 | 22 (45.8) | 204 (51.1) | 0.49 |
| ≥25 | 26 (54.2) | 195 (48.9) | |
| Creatinine clearance (mL/min) | 68.04 ± 25.36 | 69.08 ± 24.70 | 0.78 |
| <30 | 5 (10.4) | 18 (4.5) | 0.09 |
| ≥30 | 43 (89.6) | 384 (95.5) | |
| AST (IU/L) | 0.92 | ||
| <40 | 42 (87.5) | 344 (88.0) | |
| ≥40 | 6 (12.5) | 7 (12.0) | |
| ALT (IU/L) | 0.39 | ||
| <40 | 43 (89.6) | 322 (84.9) | |
| ≥40 | 5 (7.8) | 59 (15.1) | |
| Types of DOACs | 0.04 | ||
| Apixaban | 13 (26.0) | 168 (40.2) | |
| Edoxaban | 18 (36.0) | 141 (33.7) | |
| Rivaroxaban | 16 (32.0) | 58 (13.9) | |
| Dabigatran | 3 (6.0) | 51 (12.2) | |
| Prescription dose a | 0.01 | ||
| Underdose | 18 (36.0) | 133 (31.8) | |
| Standard dose | 28 (56.0) | 278 (66.5) | |
| Overdose | 4 (8.0) | 7 (1.7) | |
| Co-medications | |||
| Antiplatelets | 3 (6.0) | 51 (12.2) | 0.20 |
| ACEI or ARBs | 19 (38.0) | 186 (44.5) | 0.38 |
| Beta-blockers | 38 (76.0) | 295 (70.6) | 0.42 |
| Calcium channel blockers | 13 (26.0) | 116 (27.8) | 0.79 |
| Diuretics | 11 (22.0) | 109 (26.1) | 0.53 |
| Statins | 28 (56.0) | 245 (58.6) | 0.72 |
| CYP inducers | 0 (0.0) | 1 (0.2) | 1.00 |
| CYP inhibitors | 7 (14.0) | 58 (13.9) | 0.99 |
| Previous myocardial infarction | 4 (8.0) | 36 (8.6) | 1.00 |
| Previous stroke/TIA/thromboembolism | 28 (56.0) | 179 (42.8) | 0.08 |
| Previous bleeding events | 4 (8.0) | 18 (4.3) | 0.28 |
| Comorbidities | |||
| Atrial fibrillation | 49 (98.0) | 398 (98.5) | 0.78 |
| Hypertension | 34 (68.0) | 282 (67.5) | 0.94 |
| Diabetes mellitus | 14 (28.0) | 119 (28.5) | 0.95 |
| Heart failure | 5 (10.0) | 78 (18.7) | 0.13 |
| Anemia | 22 (44.0) | 107 (25.6) | 0.01 |
| Smoking | 6 (12.0) | 57 (13.6) | 0.75 |
| Alcohol | 17 (34.0) | 134 (32.1) | 0.78 |
| CHA2DS2-VASc risk of stroke | 3.62 ± 1.69 | 3.47 ± 1.76 | 0.57 |
| Modified HAS-BLED | 2.00 ± 0.95 | 1.94 ± 1.04 | 0.70 |
| dbSNP rsID | Grouped Genotype | Bleeding (n = 50) | No Bleeding (n = 418) | p |
|---|---|---|---|---|
| ABCB1 | ||||
| rs3842 (T>C) | TT, CT | 40 (80.0) | 379 (90.7) | 0.02 |
| CC | 10 (20.0) | 39 (9.3) | ||
| rs1045642 (A>G) | AA | 7 (14.0) | 42 (10.1) | 0.39 |
| AG, GG | 43 (86.0) | 375 (89.9) | ||
| rs2032582 (A>C) | AA, AC | 37 (79.0) | 331 (79.6) | 0.36 |
| CC | 13 (26.0) | 85 (20.4) | ||
| rs1128503 (A>G) | AA, AG | 40 (80.0) | 339 (81.1) | 0.85 |
| GG | 10 (20.0) | 79 (18.9) | ||
| rs3213619 (A>G) | AA, AG | 50 (100.0) | 413 (99.5) | 1.00 |
| GG | 0 (0.0) | 2 (0.5) | ||
| rs3747802 (A>G) | AA | 43 (86.0) | 368 (88.2) | 0.64 |
| AG, GG | 7 (14.0) | 49 (11.8) | ||
| CYP3A5 | ||||
| rs776746 (C>T) | CC, CT | 46 (92.0) | 396 (95.7) | 0.28 |
| TT | 4 (8.0) | 18 (4.3) |
| dbSNP rsID | Grouped Genotype | Bleeding (n = 50) | No Bleeding (n = 418) | p |
|---|---|---|---|---|
| APOB | ||||
| rs1042034 (C>T) | CC | 34 (68.0) | 233 (55.9) | 0.10 |
| CT, TT | 16 (32.0) | 184 (44.1) | ||
| rs2163204 (T>G) | TT, GT | 50 (100.0) | 413 (99.0) | 0.49 |
| GG | 0 (0.0) | 4 (1.0) | ||
| rs693 (G>A) | GG | 49 (98.0) | 369 (88.3) | 0.04 |
| AG, AA | 1 (2.0) | 49 (11.7) | ||
| rs679899 (G>A) | GG, AG | 12 (24.0) | 119 (28.5) | 0.50 |
| AA | 38 (76.0) | 298 (71.5) | ||
| rs13306194 (G>A) | GG, AG | 49 (98.0) | 413 (98.8) | 0.49 |
| AA | 1 (2.0) | 5 (1.2) | ||
| rs13306198 (G>A) | GG | 37 (74.0) | 381 (91.1) | <0.01 |
| AG, AA | 13 (26.0) | 37 (8.9) | ||
| rs1367117 (G>A) | GG | 42 (84.0) | 324 (77.5) | 0.29 |
| AG, AA | 8 (16.0) | 94 (22.5) | ||
| APOE | ||||
| rs429358 (T>C) | TT | 43 (86.0) | 329 (79.5) | 0.27 |
| CT, CC | 7 (14.0) | 85 (20.5) | ||
| rs7412 (C>T) | CC | 42 (89.4) | 345 (85.2) | 0.44 |
| CT, TT | 5 (10.6) | 60 (14.8) |
| Predictors | Unadjusted OR (95% CIs) | Model I | Model II |
|---|---|---|---|
| Adjusted OR (95% CI) | Adjusted OR (95% CI) | ||
| Female | 1.03 (0.56–1.88) | ||
| Age (≥65) | 0.91 (0.48–1.70) | ||
| Overdose | 5.11 (1.44–18.10) | 4.02 (1.04–15.46) * | 4.21 (1.00–17.73) |
| Rivaroxaban | 2.92 (1.52–5.63) | 2.70 (1.37–5.33) * | 2.59 (1.26–5.30) * |
| Anemia | 2.28 (1.25–4.16) | 2.33 (1.26–4.31) ** | 2.61 (1.37–4.96) ** |
| ABCB1 rs3842 CC | 2.43 (1.13–5.23) | 2.44 (1.07–5.58) * | |
| APOB rs693 GG | 6.49 (0.88–47.62) | 6.85 (0.90–52.63) | |
| APOB rs13306198 AG, AA | 3.62 (1.77–7.41) | 3.00 (1.39–6.47) * |
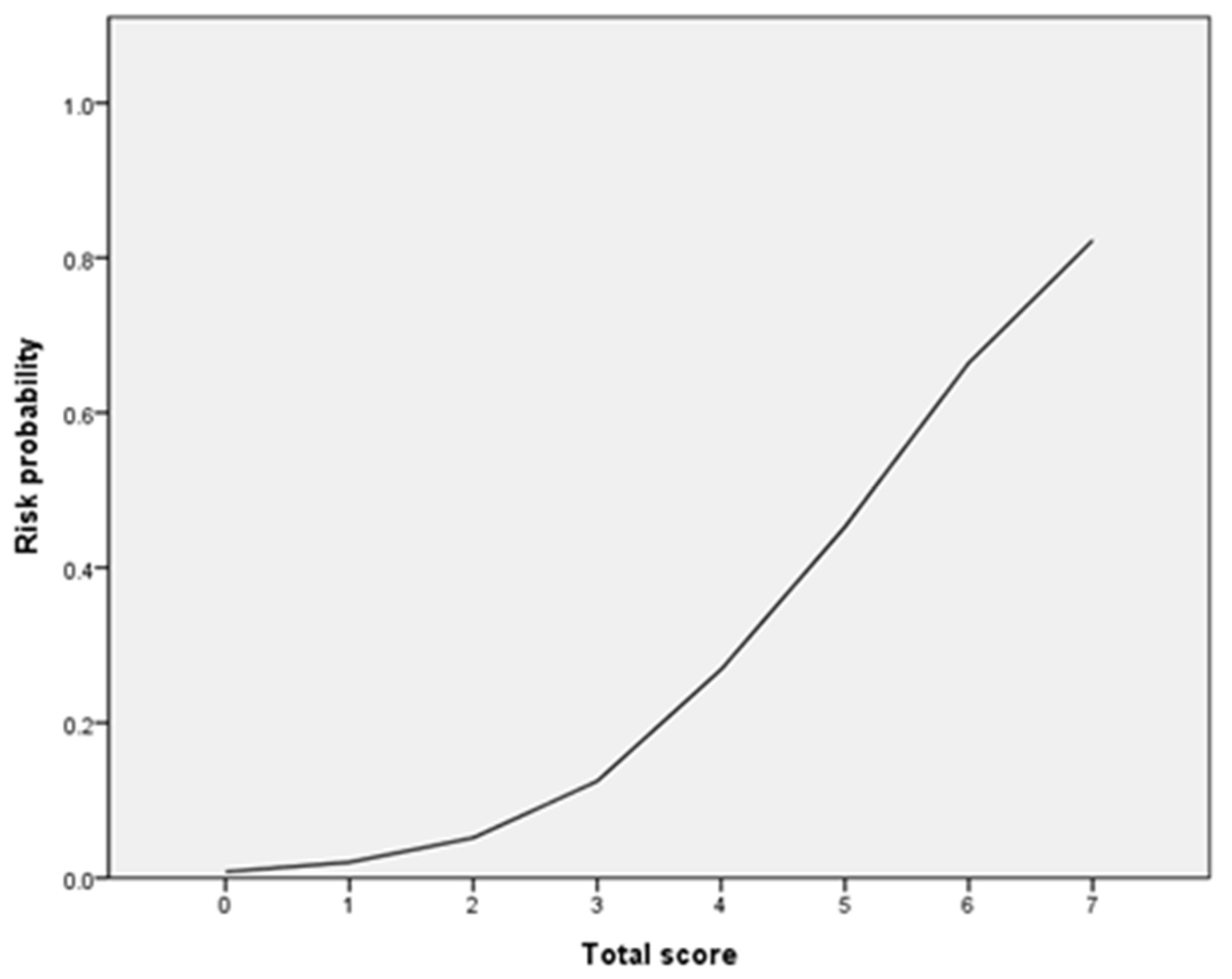
| Score | Bleeding | Total | Observed Bleeding Risk (%) | Predicted Bleeding Risk (%) |
|---|---|---|---|---|
| 0 | 0 | 25 | 0.00 | 0.79 |
| 1 | 1 | 17 | 5.88 | 2.02 |
| 2 | 0 | 7 | 0.00 | 5.41 |
| 3 | 11 | 203 | 5.42 | 5.18 |
| 4 | 18 | 160 | 11.25 | 12.51 |
| 5 | 14 | 43 | 32.56 | 26.90 |
| 6 | 3 | 9 | 33.33 | 47.00 |
| 7 | 2 | 3 | 66.67 | 64.27 |
| 8 | 1 | 1 | 100.00 | 82.25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, H.-Y.; Song, T.-J.; Yee, J.; Park, J.; Gwak, H.-S. Association between Genetic Polymorphisms and Bleeding in Patients on Direct Oral Anticoagulants. Pharmaceutics 2022, 14, 1889. https://doi.org/10.3390/pharmaceutics14091889
Yoon H-Y, Song T-J, Yee J, Park J, Gwak H-S. Association between Genetic Polymorphisms and Bleeding in Patients on Direct Oral Anticoagulants. Pharmaceutics. 2022; 14(9):1889. https://doi.org/10.3390/pharmaceutics14091889
Chicago/Turabian StyleYoon, Ha-Young, Tae-Jin Song, Jeong Yee, Junbeom Park, and Hye-Sun Gwak. 2022. "Association between Genetic Polymorphisms and Bleeding in Patients on Direct Oral Anticoagulants" Pharmaceutics 14, no. 9: 1889. https://doi.org/10.3390/pharmaceutics14091889