
Progress in 3D Bioprinting Technology for Osteochondral Regeneration

 , , , , and
, , , , and
Abstract
:1. Introduction
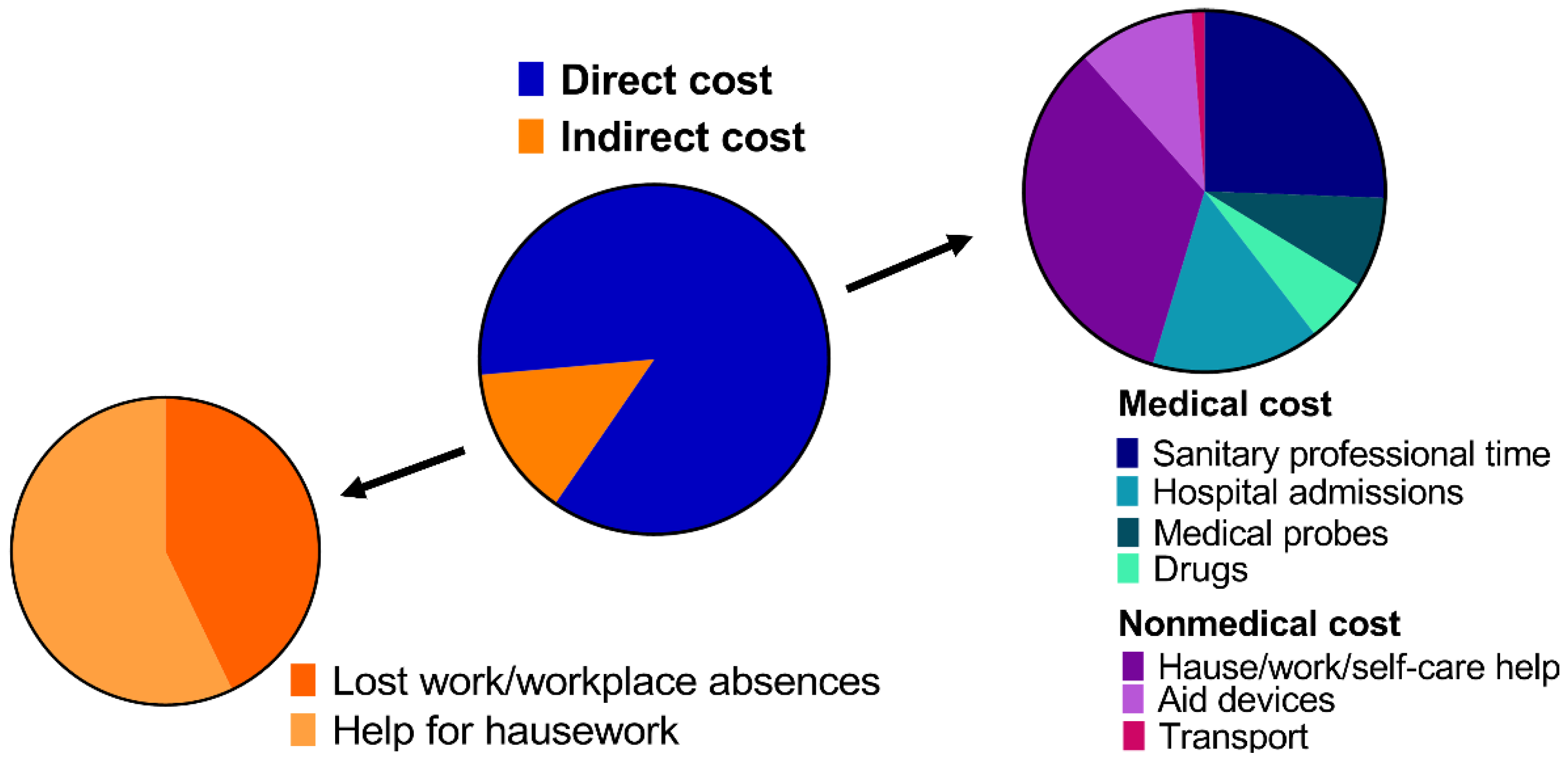
1.1. Prevalence and Economic Burden
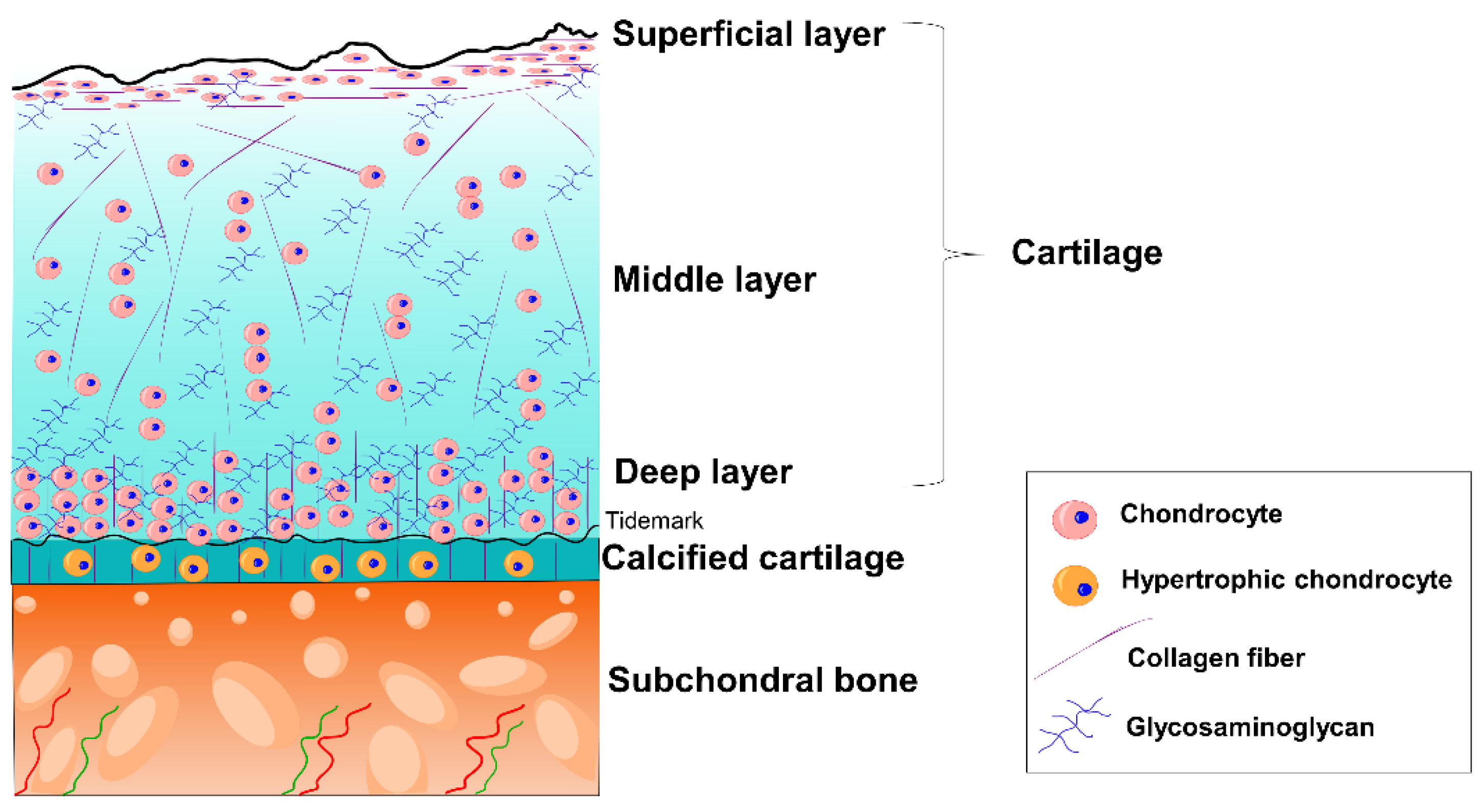
1.2. Joint Anatomy and Physiology
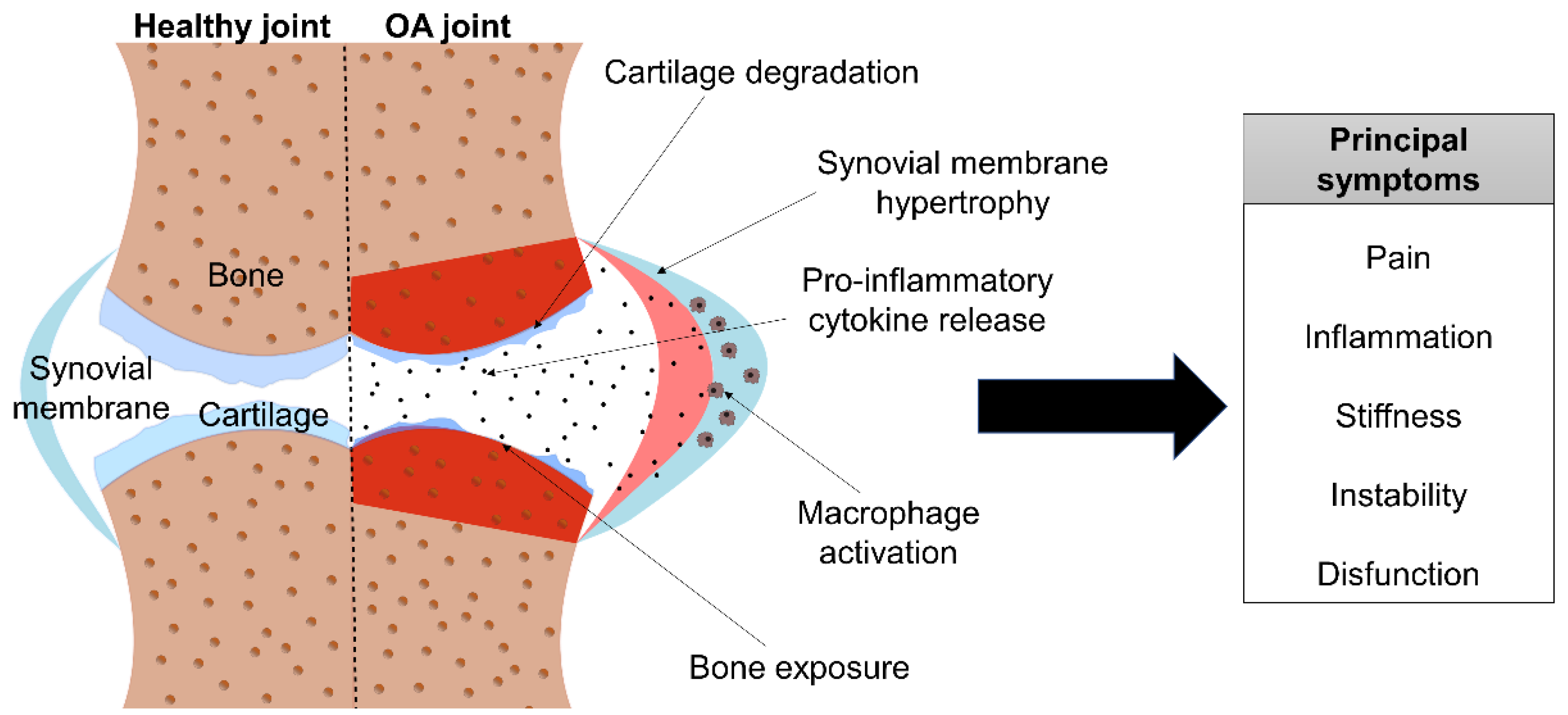
1.3. OA
Pathogenesis and Symptomatology
2. Current Treatments
2.1. Pharmacological Treatments
2.2. Surgery
2.3. Biological Therapies
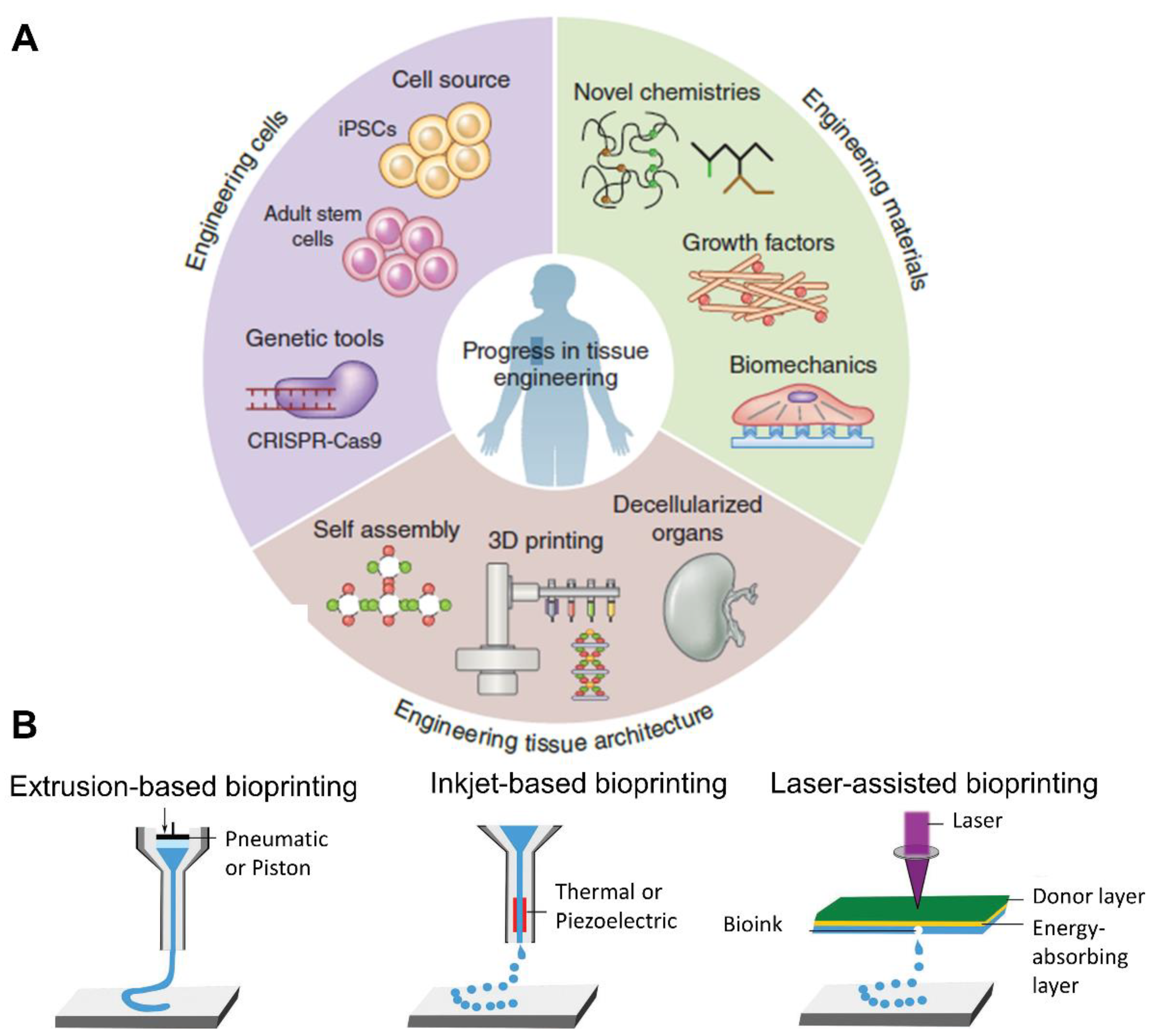
3. New Therapeutic Approaches: Tissue Engineering and 3D Bioprinting
3.1. 3D Bioprinting in Cartilage
3.2. 3D Bioprinting in Bone
3.3. 3D Bioprinting in Osteochondral Units
4. Current Limitations of 3D Bioprinting
5. Conclusions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Xu, J.; Ji, J.; Jiao, J.; Zheng, L.; Hong, Q.; Tang, H.; Zhang, S.; Qu, X.; Yue, B. 3D Printing for Bone-Cartilage Interface Regeneration. Front. Bioeng. Biotechnol. 2022, 10, 828921. [Google Scholar] [CrossRef] [PubMed]
- Poveda-Roda, R.; Bagán, J.V.; Sanchis, J.; Margaix, M. Pseudotumors and Tumors of the Temporomandibular Joint. A Review. Med. Oral Patol. Oral Cirugía Bucal 2013, 18, e392–e402. [Google Scholar] [CrossRef] [PubMed]
- García-Arias, M.; Balsa, A.; Mola, E.M. Septic Arthritis. Best practice & research. Clin. Rheumatol. 2011, 25, 407–421. [Google Scholar]
- Chau, M.M.; Klimstra, M.A.; Wise, K.L.; Ellermann, J.M.; Tóth, F.; Carlson, C.S.; Nelson, B.J.; Tompkins, M.A. Osteochondritis Dissecans. J. Bone Jt. Surg. 2021, 103, 1132. [Google Scholar] [CrossRef] [PubMed]
- Hawker, G.A. OA Serious Disease. Clin. Exp. Rheumatol. 2019, 37, 3. [Google Scholar]
- David, O.; Hunter, J.; Bierma-Zeinstra, S. Osteroarthritis. Lancet Semin. 2019, 393, 1745. [Google Scholar]
- Jorgensen, C.; Simon, M. In Vitro Human Joint Models Combining Advanced 3D Cell Culture and Cutting-Edge 3D Bioprinting Technologies. Cells 2021, 10, 596. [Google Scholar] [CrossRef]
- Daly, A.C.; Freeman, F.E.; Gonzalez-Fernandez, T.; Critchley, S.E.; Nulty, J.; Kelly, D.J. 3D Bioprinting for Cartilage and Osteochondral Tissue Engineering. Adv. Healthc. Mater. 2017, 6, 1700298. [Google Scholar] [CrossRef]
- Hunter, D.J.; March, L.; Chew, M. OA in 2020 and beyond. Lancet Comm. 2020, 396, 1711. [Google Scholar] [CrossRef]
- Hunter, D.J.; Schofield, D.; Callander, E. The Individual and Socioeconomic Impact of Osteoarthritis. Nat. Rev. Rheumatol. 2014, 10, 437–441. [Google Scholar] [CrossRef]
- Laires, P.A.; Canhão, H.; Rodrigues, A.M.; Eusébio, M.; Gouveia, M.; Branco, J.C. The Impact of Osteoarthritis on Early Exit from Work: Results from a Population-Based Study. BMC Public Health 2018, 18, 472. [Google Scholar] [CrossRef]
- Critchley, S.E.; Kelly, D.J. Bioinks for Bioprinting Functional Meniscus and Articular Cartilage. J. 3D Print. Med. 2017, 1, 269. [Google Scholar] [CrossRef]
- Puig-Junoy, J.; Ruiz Zamora, A. Socio-Economic Costs of Osteoarthritis: A Systematic Review of Cost-of-Illness Studies. Semin. Arthritis Rheum. 2014, 44, 531–541. [Google Scholar] [CrossRef]
- Loza, E.; Lopez-Gomez, J.M.; Abasolo, L.; Maese, J.; Carmona, L.; Batlle-Gualda, E. Economic Burden of Knee and Hip Osteoarthritis in Spain. Arthritis Rheum. 2009, 61, 158–165. [Google Scholar] [CrossRef]
- Ramos, T.; Moroni, L. Tissue Engineering and Regenerative Medicine 2019: The Role of Biofabrication—A Year in Review. Tissue Eng. Part C Methods 2020, 26, 91–106. [Google Scholar] [CrossRef]
- Derakhshanfar, S.; Mbeleck, R.; Xu, K.; Zhang, X.; Zhong, W.; Xing, M. 3D Bioprinting for Biomedical Devices and Tissue Engineering: A Review of Recent Trends and Advances. Bioact. Mater. 2018, 3, 144–156. [Google Scholar] [CrossRef]
- Bhat, A.; Janarthanan, M. Human Joint Anatomy and Physiology. In Pediatric Rheumatology; Springer: Berlin/Heidelberg, Germany, 2016; pp. 29–35. [Google Scholar]
- Nesic, D.; Whiteside, R.; Brittberg, M.; Wendt, D.; Martin, I.; Mainil-Varlet, P. Cartilage Tissue Engineering for Degenerative Joint Disease. Adv. Drug Deliv. Rev. 2006, 58, 300–322. [Google Scholar] [CrossRef]
- Daly, A.C.; Critchley, S.E.; Rencsok, E.M.; Kelly, D.J. A Comparison of Different Bioinks for 3D Bioprinting of Fibrocartilage and Hyaline Cartilage. Biofabrication 2016, 8, 045002. [Google Scholar] [CrossRef]
- Johnston, T.P. Anatomy and Physiology of the Oral Mucosa. In Oral Mucosal Drug Delivery and Therapy; Springer: Boston, MA, USA, 2015; pp. 1–15. [Google Scholar]
- Gadjanski, I.; Vunjak-Novakovic, G. Challenges in Engineering Osteochondral Tissue Grafts with Hierarchical Structures. Expert Opin. Biol. Ther. 2015, 15, 1583–1599. [Google Scholar] [CrossRef] [Green Version]
- Denoix, J.; Jeffcott, L.B.; McIlwraith, C.W.; van Weeren, P.R. A Review of Terminology for Equine Juvenile Osteochondral Conditions (JOCC) Based on Anatomical and Functional Considerations. Vet. J. 2013, 197, 29–35. [Google Scholar] [CrossRef]
- Li, G.; Yin, J.; Gao, J.; Cheng, T.S.; Pavlos, N.J.; Zhang, C.; Zheng, M.H. Subchondral Bone in Osteoarthritis: Insight into Risk Factors and Microstructural Changes. Arthritis Res. Ther. 2013, 15, 223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sophia Fox, A.J.; Bedi, A.; Rodeo, S.A. The Basic Science of Articular Cartilage: Structure, Composition, and Function. Sports Health 2009, 1, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, C.F.; Gasperini, L.; Marques, A.P.; Reis, R.L. The stiffness of living tissues and its implications for tissue engineering. Nat. Rev. Mater. 2020, 5, 351. [Google Scholar] [CrossRef]
- Schiphof, D.; Boers, M.; Bierma-Zeinstra, S.M.A. Differences in Descriptions of Kellgren and Lawrence Grades of Knee Osteoarthritis. Ann. Rheum. Dis. 2008, 67, 1034–1036. [Google Scholar] [CrossRef]
- Kohn, M.D.; Sassoon, A.A.; Fernando, N.D. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clin. Orthop. Relat. Res. 2016, 474, 1886–1893. [Google Scholar] [CrossRef] [Green Version]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol. 2020, 72, 220–233. [Google Scholar] [CrossRef]
- Grässel, S.; Muschter, D. Recent Advances in the Treatment of Osteoarthritis. F1000 Res. 2020, 9, 325. [Google Scholar] [CrossRef]
- Primorac, D.; Molnar, V.; Matišić, V.; Hudetz, D.; Jeleč, Ž.; Rod, E.; Čukelj, F.; Vidović, D.; Vrdoljak, T.; Dobričić, B.; et al. Comprehensive Review of Knee Osteoarthritis Pharmacological Treatment and the Latest Professional Societies’ Guidelines. Pharmaceuticals 2021, 14, 205. [Google Scholar] [CrossRef]
- Anandacoomarasamy, A.; March, L. Current Evidence for Osteoarthritis Treatments. Ther. Adv. Musculoskelet. Dis. 2010, 2, 17–28. [Google Scholar] [CrossRef]
- Trasolini, N.A.; McKnight, B.M.; Dorr, L.D. The Opioid Crisis and the Orthopedic Surgeon. J. Arthroplast. 2018, 33, 3379–3382.e1. [Google Scholar] [CrossRef]
- Bartha, L.; Vajda, A.; Duska, Z.; Rahmeh, H.; Hangody, L. Autologous Osteochondral Mosaicplasty Grafting. J. Orthop. Sports Phys. Ther. 2006, 36, 739–750. [Google Scholar] [CrossRef]
- Robinson, A.; Lindsay, A.; Vidal, A.; Frank, R.M. Osteochondral Autograft Transfer (OATS). Oper. Tech. Sports Med. 2020, 28, 150781. [Google Scholar] [CrossRef]
- Belk, J.W.; Kraeutler, M.J.; Houck, D.A.; Goodrich, J.A.; Dragoo, J.L.; McCarty, E.C. Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Am. J. Sports Med. 2021, 49, 249–260. [Google Scholar] [CrossRef]
- Everts, P.; Onishi, K.; Jayaram, P.; Lana, J.F.; Mautner, K. Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. Int. J. Mol. Sci. 2020, 21, 7794. [Google Scholar] [CrossRef]
- Hulme, C.H.; Perry, J.; McCarthy, H.S.; Wright, K.T.; Snow, M.; Mennan, C.; Roberts, S. Cell Therapy for Cartilage Repair. Emerg. Top. Life Sci. 2021, 5, 575–589. [Google Scholar] [CrossRef]
- Jevotovsky, D.S.; Alfonso, A.R.; Einhorn, T.A.; Chiu, E.S. Osteoarthritis and Stem Cell Therapy in Humans: A Systematic Review. Osteoarthr. Cartil. 2018, 26, 711–729. [Google Scholar] [CrossRef] [Green Version]
- Vilela, C.A.; Correia, C.; Da, A.; Morais, S.; Santos, C.; Gertrudes, A.C.; Moreira, E.S.; Frias, A.M.; Learmonth, D.A.; Oliveira, P.; et al. In Vitro and in Vivo Performance of Methacrylated Gellan Gum Hydrogel Formulations for Cartilage Repair. J. Biomed. Mater. Res. Part A 2018, 106, 1987–1996. [Google Scholar] [CrossRef] [Green Version]
- Delplace, V.; Boutet, M.; Le Visage, C.; Maugars, Y.; Guicheux, J.; Vinatier, C. Osteoarthritis: From Upcoming Treatments to Treatments Yet to Come. Joint, bone, spine. Rev. Rhum. 2021, 88, 105206. [Google Scholar]
- Manferdini, C.; Trucco, D.; Saleh, Y.; Gabusi, E.; Dolzani, P.; Lenzi, E.; Vannozzi, L.; Ricotti, L.; Lisignoli, G. RGD-Functionalized Hydrogel Supports the Chondrogenic Commitment of Adipose Mesenchymal Stromal Cells. Gels 2022, 8, 382. [Google Scholar] [CrossRef]
- Trucco, D.; Vannozzi, L.; Teblum, E.; Telkhozhayeva, M.; Gilbert, D.; Nessim, S.; Affatato, H.; Al-Haddad, G.; Lisignoli; Ricotti, L. Graphene Oxide-Doped Gellan Gum-PEGDA Bilayered Hydrogel Mimicking the Mechanical and Lubrication Properties of Articular Cartilage. Adv. Healthc. Mater. 2021, 10, 2001434. [Google Scholar] [CrossRef]
- Yao, H.; Kang, J.; Li, W.; Liu, J.; Xie, R.; Wang, Y.; Liu, S.; Wang, D.; Ren, L. Novel Β -TCP/PVA Bilayered Hydrogels with Considerable Physical and Bio-Functional Properties for Osteochondral Repair. Biomed. Mater. 2018, 13, 015012. [Google Scholar] [CrossRef] [PubMed]
- Roseti, L.; Desando, G.; Cavallo, C.; Petretta, M.; Grigolo, B. Articular Cartilage Regeneration in Osteoarthritis. Cells 2019, 8, 1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, W.; Ma, X.; Gou, M.; Mei, D.; Zhang, K.; Chen, S. 3D Printing of Functional Biomaterials for Tissue Engineering. Curr. Opin. Biotechnol. 2016, 40, 103–112. [Google Scholar] [CrossRef] [Green Version]
- Khademhosseini, A.; Langer, R. A Decade of Progress in Tissue Engineering. Nat. Protoc. 2016, 11, 1775. [Google Scholar] [CrossRef] [PubMed]
- Foyt, D.A.; Norman, M.D.A.; Yu, T.T.L.; Gentleman, E. Exploiting Advanced Hydrogel Technologies to Address Key Challenges in Regenerative Medicine. Adv. Healthc. Mater. 2018, 7, 1700939. [Google Scholar] [CrossRef] [PubMed]
- Hölzl, K.; Lin, S.; Tytgat, L.; Van Vlierberghe, S.; Gu, L.; Ovsianikov, A. Bioink Properties before, during and After 3D Bioprinting. Biofabrication 2016, 8, 032002. [Google Scholar] [CrossRef] [Green Version]
- Turnbull, G.; Clarke, J.; Picard, F.; Riches, P.; Jia, L.; Han, F.; Li, B.; Shu, W. 3D Bioactive Composite Scaffolds for Bone Tissue Engineering. Bioact. Mater. 2018, 3, 278–314. [Google Scholar] [CrossRef] [Green Version]
- Gungor-Ozkerim, P.S.; Inci, I.; Zhang, Y.S.; Khademhosseini, A.; Dokmeci, M.R. Bioinks for 3D Bioprinting: An Overview. Biomater. Sci. 2018, 6, 915–946. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Alonso, S.; Lafuente-Merchan, M.; Ciriza, J.; Saenz-del-Burgo, L.; Pedraz, J.L. Tendon Tissue Engineering: Cells, Growth Factors, Scaffolds and Production Techniques. JCR 2021, 333, 448–486. [Google Scholar] [CrossRef]
- Abdollahiyan, P.; Oroojalian, F.; Mokhtarzadeh, A.; Guardia, M. Hydrogel-Based 3D Bioprinting for Bone and Cartilage Tissue Engineering. Biotechnol. J. 2020, 15, 2000095. [Google Scholar] [CrossRef]
- Wu, Y.; Kennedy, P.; Bonazza, N.; Yu, Y.; Dhawan, A.; Ozbolat, I. Three-Dimensional Biopritning of Articular Cartilage: A systematic review. Cartilage 2021, 12, 76. [Google Scholar] [CrossRef]
- Ruiz-Alonso, S.; Villate-Beitia, I.; Gallego, I.; Lafuente-Merchan, M.; Puras, G.; Saenz-Del-Burgo, L.; Pedraz, J.L. Current Insights into 3D Bioprinting: An Advanced Approach for Eye Tissue Regeneration. Pharmaceutics 2021, 13, 308. [Google Scholar] [CrossRef]
- Cao, Y.; Cheng, P.; Sang, S.; Xiang, C.; An, Y.; Wei, X.; Shen, Z.; Zhang, Y.; Li, P. Mesenchymal Stem Cells Loaded on 3D-Printed Gradient Poly(Ε-Caprolactone)/Methacrylated Alginate Composite Scaffolds for Cartilage Tissue Engineering. Regen. Biomater. 2021, 8, rbab019. [Google Scholar] [CrossRef]
- Chen, W.; Xu, Y.; Liu, Y.; Wang, Z.; Li, Y.; Jiang, G.; Mo, X.; Zhou, G. Three-Dimensional Printed Electrospun Fiber-Based Scaffold for Cartilage Regeneration. Mater. Des. 2019, 179, 107886. [Google Scholar] [CrossRef]
- Beketov, E.E.; Isaeva, E.V.; Yakovleva, N.D.; Demyashkin, G.A.; Arguchinskaya, N.V.; Kisel, A.A.; Lagoda, T.S.; Malakhov, E.P.; Kharlov, V.I.; Osidak, E.O.; et al. Bioprinting of Cartilage with Bioink Based on High-Concentration Collagen and Chondrocytes. Int. J. Mol. Sci. 2021, 22, 11351. [Google Scholar] [CrossRef]
- Yang, X.; Lu, Z.; Wu, H.; Li, W.; Zheng, L.; Zhao, J. Collagen-Alginate as Bioink for Three-Dimensional (3D) Cell Printing Based Cartilage Tissue Engineering. Mater. Sci. Eng. C 2018, 83, 195–201. [Google Scholar] [CrossRef]
- Nguyen, D.; Hägg, D.A.; Forsman, A.; Ekholm, J.; Nimkingratana, P.; Brantsing, C.; Kalogeropoulos, T.; Zaunz, S.; Concaro, S.; Brittberg, M.; et al. Cartilage Tissue Engineering by the 3D Bioprinting of iPS Cells in a Nanocellulose/Alginate Bioink. Sci. Rep. 2017, 7, 658. [Google Scholar] [CrossRef]
- Rathan, S.; Dejob, L.; Schipani, R.; Haffner, B.; Möbius, M.E.; Kelly, D.J. Fiber Reinforced Cartilage ECM Functionalized Bioinks for Functional Cartilage Tissue Engineering. Adv. Healthc. Mater. 2019, 8, 1801501. [Google Scholar] [CrossRef]
- Visscher, D.O.; Lee, H.; van Zuijlen, P.P.M.; Helder, M.N.; Atala, A.; Yoo, J.J.; Lee, S.J. A Photo-Crosslinkable Cartilage-Derived Extracellular Matrix Bioink for Auricular Cartilage Tissue Engineering. Acta Biomater. 2021, 121, 193–203. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, Y.; Luo, C.; Zhai, C.; Li, Z.; Zhang, Y.; Yuan, T.; Dong, S.; Zhang, J.; Fan, W. Crosslinker-Free Silk/Decellularized Extracellular Matrix Porous Bioink for 3D Bioprinting-Based Cartilage Tissue Engineering. Mater. Sci. Eng. C. 2021, 118, 111388. [Google Scholar] [CrossRef]
- Li, Z.; Zhang, X.; Yuan, T.; Zhang, Y.; Luo, C.; Zhang, J.; Liu, Y.; Fan, W. Addition of Platelet-Rich Plasma to Silk Fibroin Hydrogel Bioprinting for Cartilage Regeneration. Tissue Eng. Part A 2020, 26, 886–895. [Google Scholar] [CrossRef]
- Singh, Y.P.; Bandyopadhyay, A.; Mandal, B.B. 3D Bioprinting using Cross-Linker-Free Silk–Gelatin Bioink for Cartilage Tissue Engineering. ACS Appl. Mater. Interfaces 2019, 11, 33684–33696. [Google Scholar] [CrossRef]
- Li, C.; Wang, K.; Zhou, X.; Li, T.; Xu, Y.; Qiang, L.; Peng, M.; Xu, Y.; Xie, L.; He, C.; et al. Controllable Fabrication of Hydroxybutyl Chitosan/Oxidized Chondroitin Sulfate Hydrogels by 3D Bioprinting Technique for Cartilage Tissue Engineering. Biomed. Mater. 2019, 14, 025006. [Google Scholar] [CrossRef]
- Galarraga, J.H.; Kwon, M.Y.; Burdick, J.A. 3D Bioprinting Via an in Situ Crosslinking Technique Towards Engineering Cartilage Tissue. Sci. Rep. 2019, 9, 19987. [Google Scholar] [CrossRef] [PubMed]
- Di Bella, C.; Duchi, S.; O’connell, C.D.; Blanchard, R.; Augustine, C.; Yue, Z.; Thompson, F.; Richards, C.; Beirne, S.; Onofrillo, C.; et al. In Situ Handheld Three-dimensional Bioprinting for Cartilage Regeneration. J. Tissue Eng. Regen. Med. 2017, 12, 611. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Cantu, L.; Gleadall, A.; Faris, C.; Segal, J.; Shakesheff, K.; Yang, J. Multi-Material 3D Bioprinting of Porous Constructs for Cartilage Regeneration. Mater. Sci. Eng. C. 2020, 109, 110578. [Google Scholar] [CrossRef] [PubMed]
- de Ruijter, M.; Ribeiro, A.; Dokter, I.; Castilho, M.; Malda, J. Simultaneous Micropatterning of Fibrous Meshes and Bioinks for the Fabrication of Living Tissue Constructs. Adv. Healthc. Mater. 2019, 8, 1800418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, W.; Cui, H.; Boualam, B.; Masood, F.; Flynn, E.; Rao, R.D.; Zhang, Z.; Zhang, L.G. 3D Bioprinting Mesenchymal Stem Cell-Laden Construct with Core–shell Nanospheres for Cartilage Tissue Engineering. Nanotechnology 2018, 29, 158101. [Google Scholar] [CrossRef]
- Wu, Y.; Ayan, B.; Moncal, K.K.; Kang, Y.; Dhawan, A.; Koduru, S.V.; Ravnic, D.J.; Kamal, F.; Ozbolat, I.T. Hybrid Bioprinting of Zonally Stratified Human Articular Cartilage using Scaffold-Free Tissue Strands as Building Blocks. Adv. Healthc. Mater. 2020, 9, 2001657. [Google Scholar] [CrossRef]
- Mouser, V.H.M.; Levato, R.; Mensinga, A.; Dhert, W.J.A.; Gawlitta, D.; Malda, J. Bio-Ink Development for Three-Dimensional Bioprinting of Hetero-Cellular Cartilage Constructs. J. Connect. Tissue Res. 2018, 61, 137. [Google Scholar] [CrossRef] [Green Version]
- Lafuente-merchan, M.; Ruiz-alonso, S.; Zabala, A.; Gálvez-martín, P.; Marchal, J.A.; Vázquez-lasa, B.; Gallego, I.; Saenz-del-burgo, L.; Pedraz, J.L. Chondroitin and Dermatan Sulfate Bioinks for 3D Bioprinting and Cartilage Regeneration. Macromol. Biosci. 2022, 22, e2100435. [Google Scholar] [CrossRef]
- O’connell, C.D.; Di Bella, C.; Thompson, F.; Augustine, C.; Beirne, S.; Cornock, R.; Richards, C.J.; Chung, J.; Gambhir, S.; Yue, Z.; et al. Development of the Biopen: A Handheld Device for Surgical Printing of Adipose Stem Cells at a Chondral Wound Site. Biofabrication 2016, 8, 015019. [Google Scholar] [CrossRef]
- Bhattacharjee, A.; Bose, S. 3D Printed Hydroxyapatite—Zn2+ Functionalized Starch Composite Bone Grafts for Orthopedic and Dental Applications. Mater. Des. 2022, 221, 110903. [Google Scholar] [CrossRef]
- Genova, T.; Roato, I.; Carossa, M.; Motta, C.; Cavagnetto, D.; Mussano, F. Advances on Bone Substitutes through 3D Bioprinting. Int. J. Mol. Sci. 2020, 21, 7012. [Google Scholar] [CrossRef]
- Bendtsen, S.T.; Quinnell, S.P.; Wei, M. Development of a Novel Alginate-polyvinyl Alcohol-hydroxyapatite Hydrogel for 3D Bioprinting Bone Tissue Engineered Scaffolds. J. Biomed. Mater. Res. 2017, 105, 1457. [Google Scholar] [CrossRef]
- Keriquel, V.; Oliveira, H.; Rémy, M.; Ziane, S.; Delmond, S.; Rousseau, B.; Rey, S.; Catros, S.; Amédée, J.; Guillemot, F.; et al. In Situ Printing of Mesenchymal Stromal Cells, by Laser-Assisted Bioprinting, for in Vivo Bone Regeneration Applications. Sci. Rep. 2017, 7, 1178. [Google Scholar] [CrossRef]
- Cunniffe, G.M.; Gonzalez-Fernandez, T.; Daly, A.; Sathy, B.N.; Jeon, O.; Alsberg, E.; Kelly, D.J. Three-Dimensional Bioprinting of Polycaprolactone Reinforced Gene Activated Bioinks for Bone Tissue Engineering. Tissue Eng. Part A 2017, 23, 891. [Google Scholar] [CrossRef]
- Freeman, F.E.; Pitacco, P.; van Dommelen, L.H.A.; Nulty, J.; Browe, D.C.; Shin, J.Y.; Alsberg, E.; Kelly, D.J. 3D Bioprinting Spatiotemporally Defined Patterns of Growth Factors to Tightly Control Tissue Regeneration. Sci. Adv. 2020, 6, eabb5093. [Google Scholar] [CrossRef]
- Kim, W.; Kim, G. Collagen/Bioceramic-Based Composite Bioink to Fabricate a Porous 3D hASCs-Laden Structure for Bone Tissue Regeneration. Biofabrication 2019, 12, 015007. [Google Scholar] [CrossRef]
- Kolan, K.C.R.; Semon, J.A.; Bromet, B.; Day, D.E.; Leu, M.C. Bioprinting with Human Stem Cells-Laden Alginate-Gelatin Bioink and Bioactive Glass for Tissue Engineering. Int. J. Bioprint. 2019, 5, 3. [Google Scholar] [CrossRef]
- Choe, G.; Oh, S.; Seok, J.M.; Park, S.A.; Lee, J.Y. Graphene Oxide/Alginate Composites as Novel Bioinks for Three-Dimensional Mesenchymal Stem Cell Printing and Bone Regeneration Applications. Nanoscale 2019, 11, 23275–23285. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Eyisoylu, H.; Qin, X.; Rubert, M.; Müller, R. 3D Bioprinting of Graphene Oxide-Incorporated Cell-Laden Bone Mimicking Scaffolds for Promoting Scaffold Fidelity, Osteogenic Differentiation and Mineralization. Acta Biomater. 2021, 121, 637–652. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Kargozar, S.; Baino, F.; Han, S.S. Additive Manufacturing Methods for Producing Hydroxyapatite and Hydroxyapatite-Based Composite Scaffolds: A Review. Front. Mater. 2019, 6, 313. [Google Scholar] [CrossRef]
- Raslan, A.; Saenz del Burgo, L.; Ciriza, J.; Pedraz, J.L. Graphene Oxide and Reduced Graphene Oxide-Based Scaffolds in Regenerative Medicine. Int. J. Pharm. 2020, 580, 119226. [Google Scholar] [CrossRef]
- Sun, Y.; You, Y.; Jiang, W.; Wang, B.; Wu, Q.; Dai, K. 3D Bioprinting Dual-Factor Releasing and Gradient-Structured Constructs Ready to Implant for Anisotropic Cartilage Regeneration. Sci. Adv. 2020, 6, 37. [Google Scholar] [CrossRef]
- Daly, A.C.; Kelly, D.J. Biofabrication of Spatially Organised Tissues by Directing the Growth of Cellular Spheroids within 3D Printed Polymeric Microchambers. Biomaterials 2019, 197, 194–206. [Google Scholar] [CrossRef]
- Burdis, R.; Chariyev-Prinz, F.; Kelly, D.J. Bioprinting of Biomimetic Self-Organised Cartilage with a Supporting Joint Fixation Device. Biofabrication 2021, 14, 015008. [Google Scholar] [CrossRef]
- Deng, C.; Yang, J.; He, H.; Ma, Z.; Wang, W.; Zhang, Y.; Li, T.; He, C.; Wang, J. 3D Bio-Printed Biphasic Scaffolds with Dual Modification of Silk Fibroin for the Integrated Repair of Osteochondral Defects. Biomater. Sci. 2021, 9, 4891–4903. [Google Scholar] [CrossRef]
- Kilian, D.; Ahlfeld, T.; Akkineni, A.R.; Bernhardt, A.; Gelinsky, M.; Lode, A. 3D Bioprinting of Osteochondral Tissue Substitutes—In Vitro-Chondrogenesis in Multi-Layered Mineralized Constructs. Sci. Rep. 2020, 10, 8277. [Google Scholar] [CrossRef]
- Kirillova, A.; Bushev, S.; Abubakirov, A.; Sukikh, G. Bioethical and Legal Issues in 3D Bioprinting. Int. J. Bioprint. 2020, 6, 272. [Google Scholar] [CrossRef]
- Gilbert, F.; O’Connell, C.D.; Mladenovska, T.; Dodds, S. Print Me an Organ? Ethical and Regulatory Issues Emerging from 3D Bioprinting in Medicine. Sci. Eng. Ethics 2017, 24, 73–91. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment | Positive Effects | Side Effects |
|---|---|---|
| Topical treatment |
|
|
| Acetaminophen or paracetamol |
|
|
| Oral NSAIDs |
|
|
| SYSADOA |
|
|
| Intra-articular injectable HA |
|
|
| Intra-articular injectable corticosteroids |
|
|
| Opiates |
|
|
| Surgery |
|
|
| PRP |
|
|
| Spherox™ |
|
|
| Bio-Ink | Cells | Technique | In Vivo | Results | Ref. |
|---|---|---|---|---|---|
| Type I COL | Rat chondrocytes | Extrusion-based bioprinting | Wistar Rats |
| [57] |
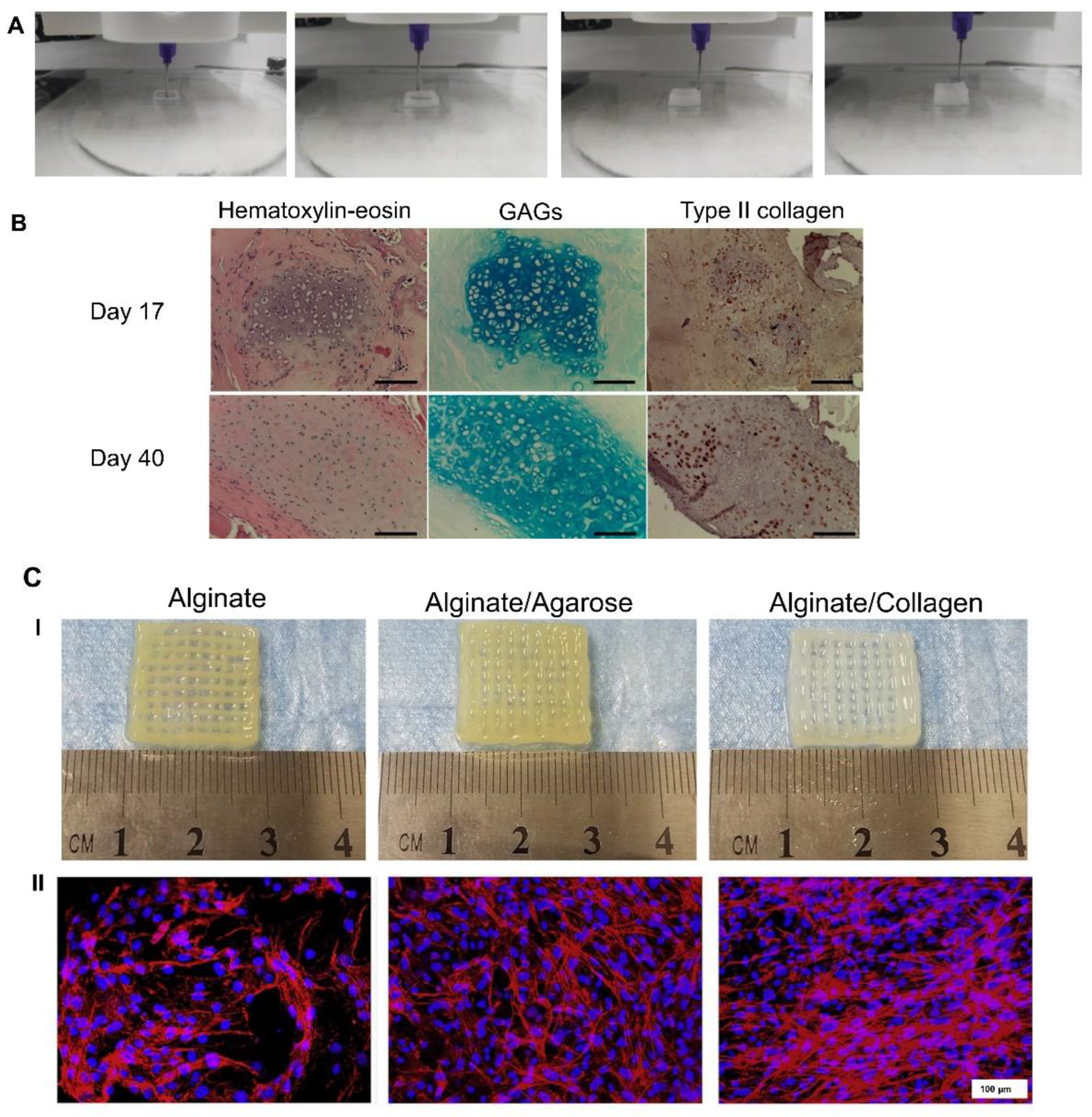
| ALG/COL ALG/agarose | Rat primary chondrocytes | Extrusion-based bioprinting | No |
| [58] |
| NFC/ALG NFC/ALG | HDiPSCs co-cultured with irradiated human chondrocytes | Extrusion-based bioprinting | No |
| [59] |
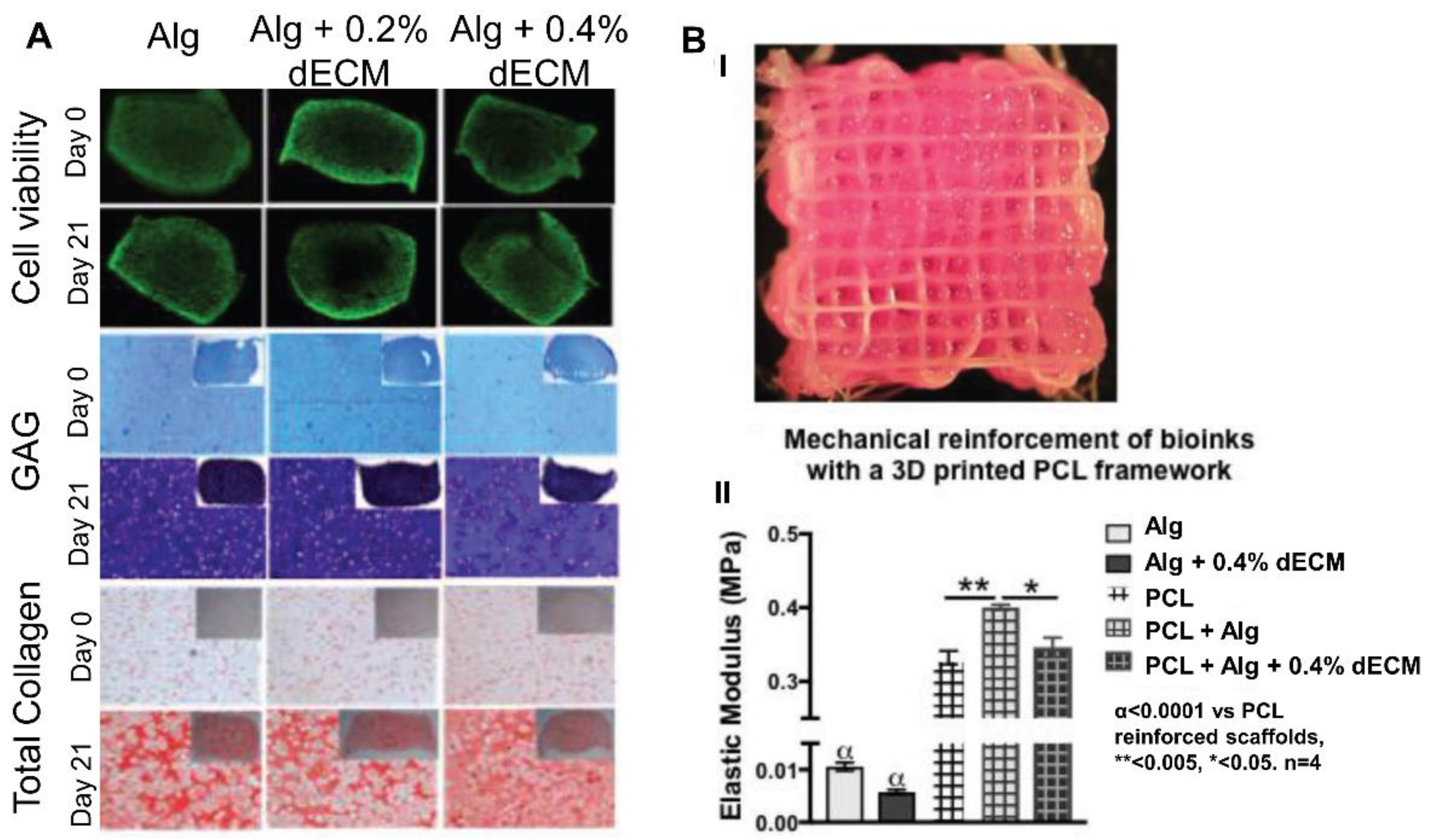
| ALG/pig dECM/TGF-β3 | Human BMSCs | Extrusion-based bioprinting | No |
| [60] |
| Pig cartilage derived dECM/Gel/HA/glycerol/DMEM | Rabbit chondrocytes | Extrusion-based bioprinting | No |
| [61] |
| SF/goat cartilage derived dECM/TGF-β3/PEG 400 | Rabbit BMSCs | Extrusion-based bioprinting | Nude mice |
| [62] |
| SF/rabbit PRP/PEG 400 | Rabbit chondrocytes | Extrusion-based bioprinting | No |
| [63] |
| SF/Gel | Porcine primary chondrocytes | Extrusion-based bioprinting | Swiss inbred mice |
| [64] |
| Hydroxybutyl CH/oxidized CS | Human ADMSCs | Extrusion-based bioprinting | C57BL/6 mice |
| [65] |
| Norbornene-modified HA | Bovine BMSC | In situ crosslinkable extrusion-based bioprinting | No |
| [66] |
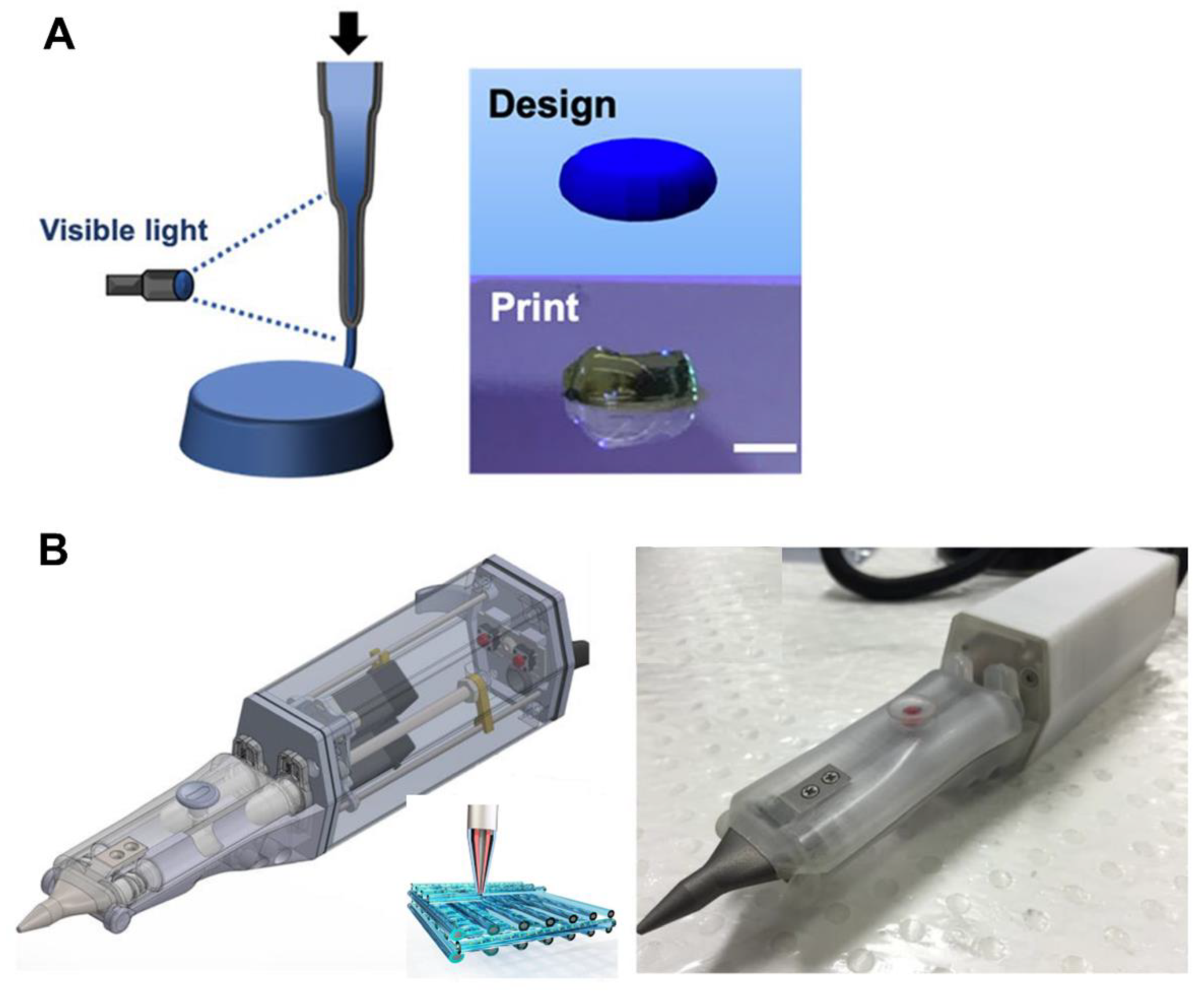
| HAMA/GelMA | Sheep ADMSCs | In situ handheld extrusion-based bioprinting “Biopen” | Chondral defect sheep |
| [67] |
| GelMA/PCL | Sheep chondrocytes | Extrusion-based bioprinting + PCL 3D printing | No |
| [68] |
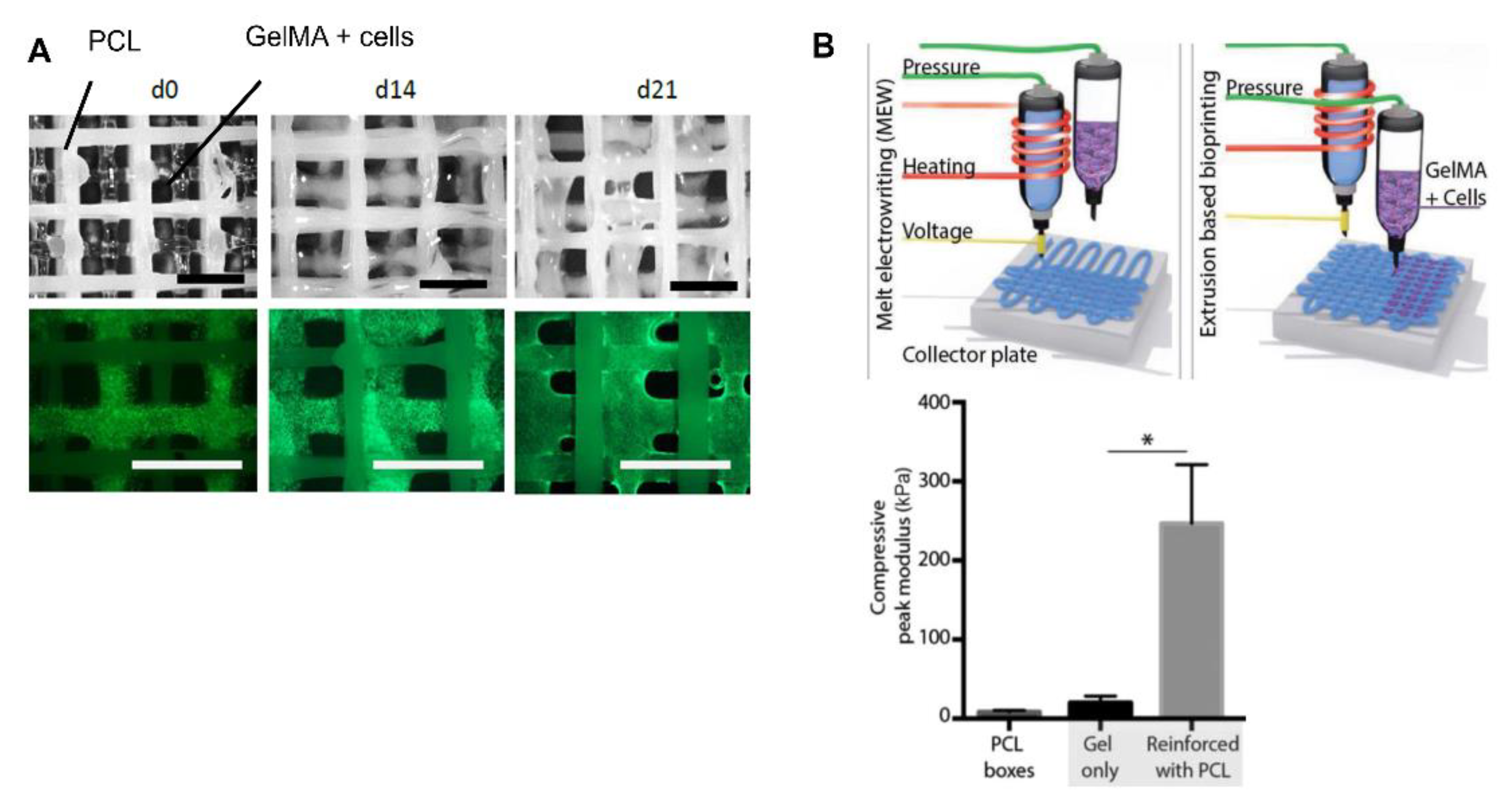
| GelMA/PCL | Equine MSCs | Extrusion-based bioprinting + PCL melt electrowriting | No |
| [69] |
| GelMa/PEGDA/TGF-β1-PLGA nanospheres | Human BMSCs | Stereolithography-based 3D bioprinting | No |
| [70] |
| ALG | Human ADMSCS | Extrusion-based bioprinting + aspiration-assisted bioprinting | No |
| [71] |
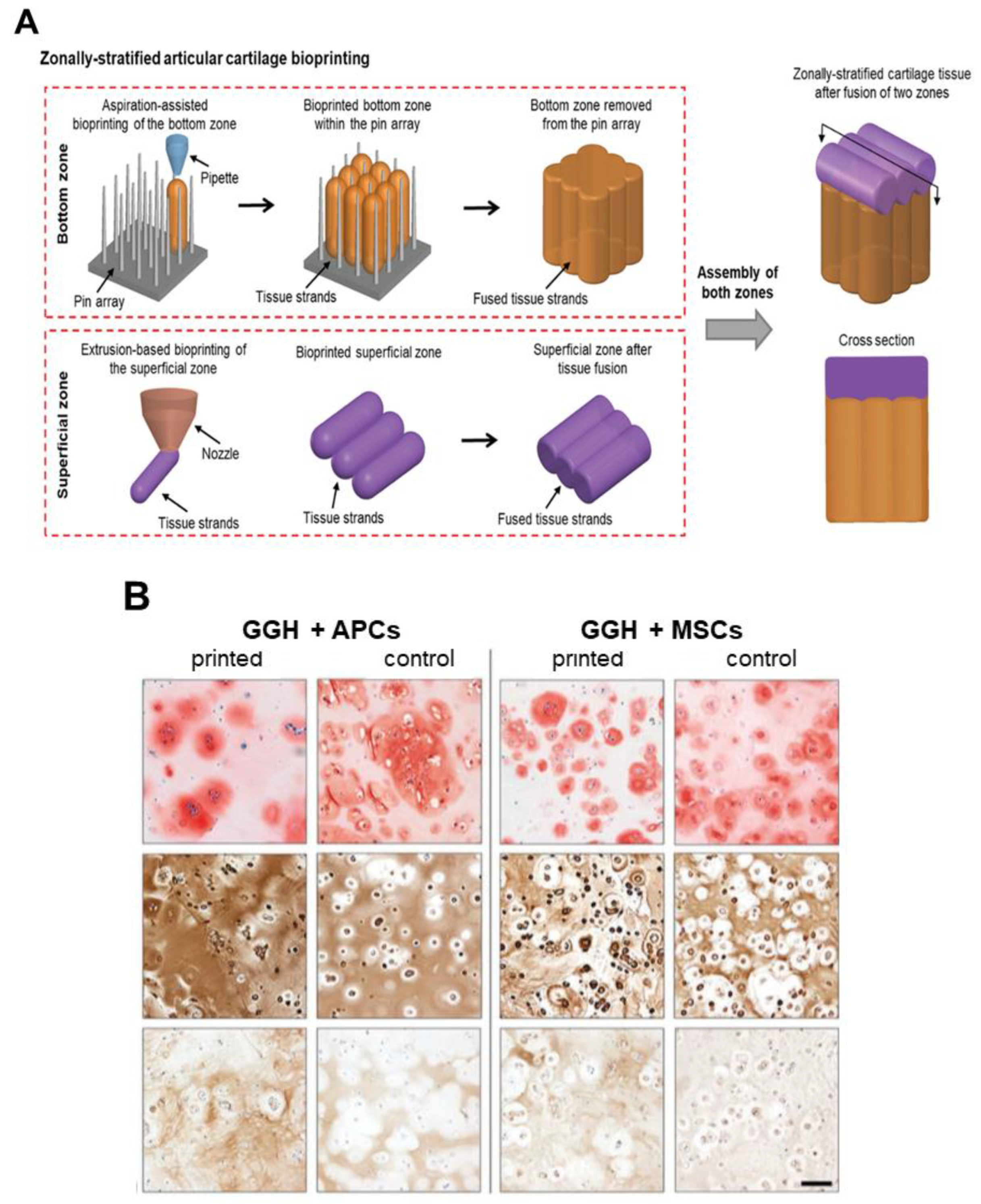
| GelMA/GG GelMA/GG/(HAMA) | Equine chondrocytes/MSCs/ACPCs | Extrusion-based bioprinting | No |
| [72] |
| Bio-ink | Cells | Technique | In Vivo | Results | Ref. |
|---|---|---|---|---|---|
| ALG/PVA/HAP | Murine calvaria 3T3-E1 cells | Extrusion-based bioprinting | No |
| [77] |
| Nano-HAP/type I COL | Murine D1-MSCs | Laser-based bioprinting | Calvaria defect rats |
| [78] |
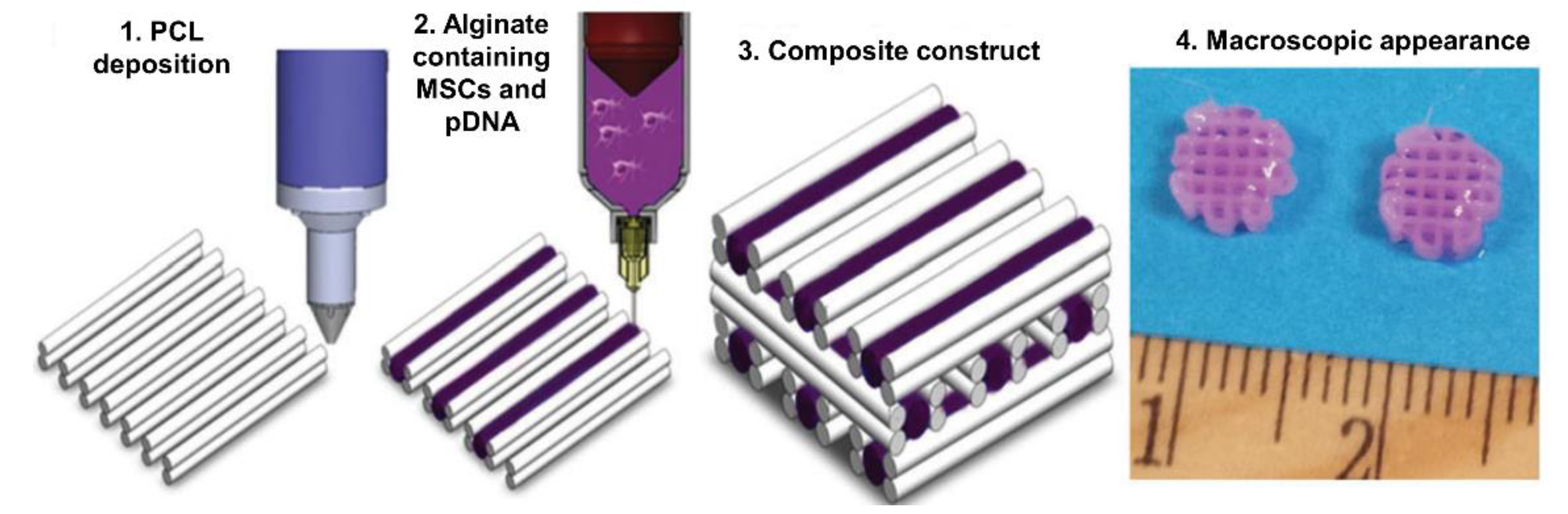
| RGD-γ-irradiated ALG/nano-HAP pDNA complexes encoding TGF-β3 and BMP-2 growth factors | Porcine BMSCs | Extrusion-based bioprinting + PCL 3D printing | Nude mice |
| [79] |
| Vascular bio-ink: RGD-γ-irradiated ALG/MC/nano-HAP nanoparticles loaded with VEGF Osteoinductive bio-ink: RGD-γ-irradiated ALG/MC/LAP/BMP-2 | Porcine BMSCs | Extrusion-based bioprinting + PCL 3D printing | Nude mice and femoral-defect rats |
| [80] |
| Type I COL/TCP | Preosteoblast cells (MC3T3-E1) And human ADMSCs | Extrusion-based bioprinting | No |
| [81] |
| ALG/GelMA/highly angiogenic borate bioactive glass (13-93B3) | Human ADMSCs | Extrusion-based bioprinting + PCL 3D printing | No |
| [82] |
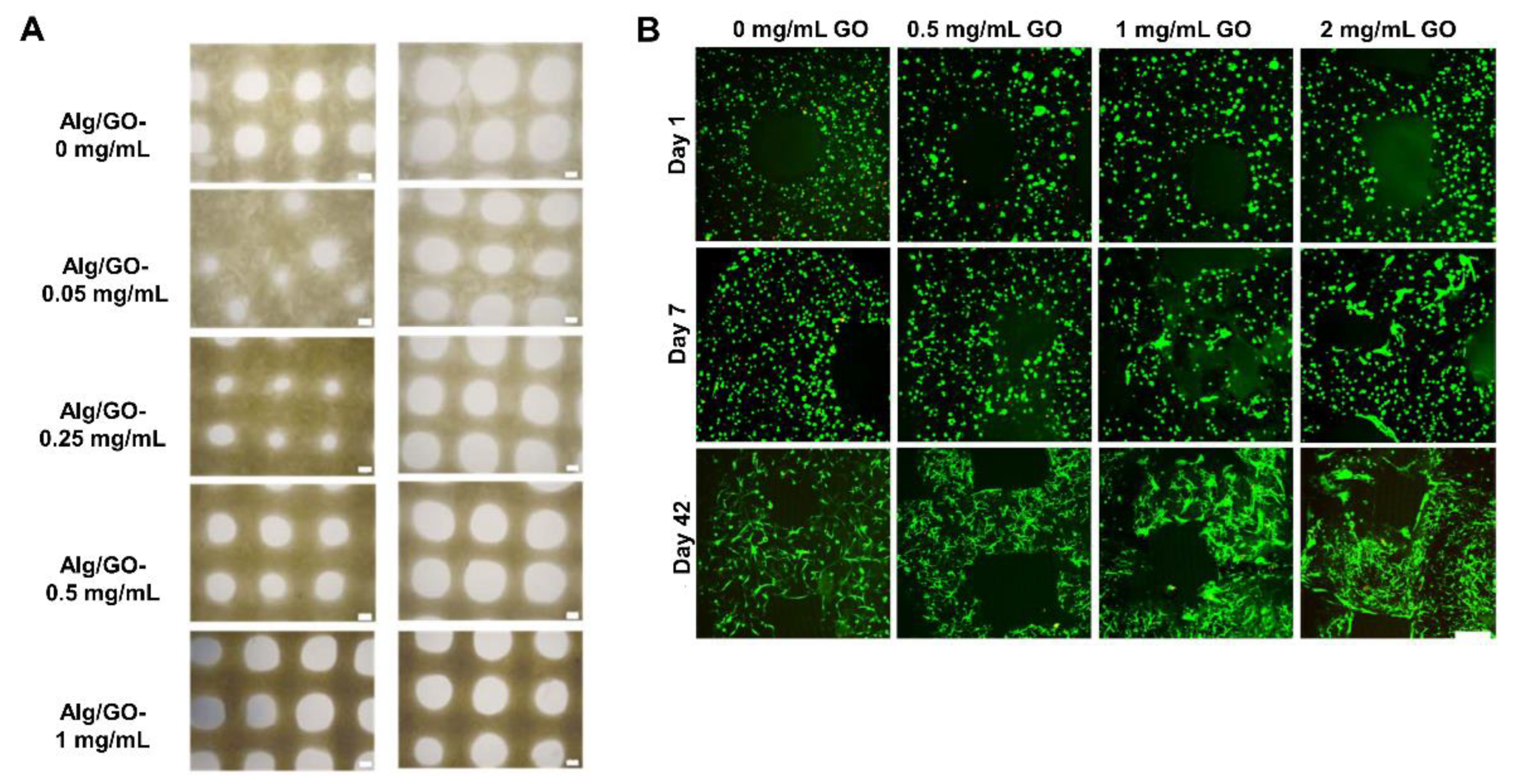
| ALG/GO | Human MSCs | Extrusion-based bioprinting | No |
| [83] |
| ALG/Gel/GO | Human BMSCs | Extrusion-based bioprinting | No |
| [84] |
| Bio-ink | Cells | Technique | In Vivo | Results | Ref. |
|---|---|---|---|---|---|
| Gel/FGN/HA/glycerol and PLGA microspheres loaded with TGF-β3 for superficial layers and BMP-4 for deeper layers. | Rabbit BMSC | Extrusion-based bioprinting + PCL 3D printing | Nude mice; rabbit knee defects |
| [87] |
| GelMA/pluronic | Porcine BMSCs co cultured with chondrocytes | Inkjet-based bioprinting + extrusion-based bioprinting + PCL 3D printing | No |
| [88] |
| Bio-ink free | Porcine BMSCs | Inkjet-based bioprinting + PCL 3D printing | No |
| [89] |
| Cartilage bio-ink: GelMA/SFMA/PTH Bone bio-ink: GelMA/SFMA | Rabbit chondrocytes Rabbit BMSCs | Extrusion-based bioprinting | Articular osteochondral defect rabbits |
| [90] |
| ALG/MC/CPC | Human chondrocytes | Extrusion-based bioprinting | No |
| [91] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lafuente-Merchan, M.; Ruiz-Alonso, S.; García-Villén, F.; Gallego, I.; Gálvez-Martín, P.; Saenz-del-Burgo, L.; Pedraz, J.L. Progress in 3D Bioprinting Technology for Osteochondral Regeneration. Pharmaceutics 2022, 14, 1578. https://doi.org/10.3390/pharmaceutics14081578
Lafuente-Merchan M, Ruiz-Alonso S, García-Villén F, Gallego I, Gálvez-Martín P, Saenz-del-Burgo L, Pedraz JL. Progress in 3D Bioprinting Technology for Osteochondral Regeneration. Pharmaceutics. 2022; 14(8):1578. https://doi.org/10.3390/pharmaceutics14081578
Chicago/Turabian StyleLafuente-Merchan, Markel, Sandra Ruiz-Alonso, Fátima García-Villén, Idoia Gallego, Patricia Gálvez-Martín, Laura Saenz-del-Burgo, and Jose Luis Pedraz. 2022. "Progress in 3D Bioprinting Technology for Osteochondral Regeneration" Pharmaceutics 14, no. 8: 1578. https://doi.org/10.3390/pharmaceutics14081578