
Optical Imaging Visualizes a Homogeneous and Horizontal Band-Like Biodistribution of Large- and Small-Size Hydrophilic Compounds Delivered by Ablative Fractional Laser


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setup
2.2. Skin Source
2.3. Molecule Preparation
2.4. Laser-Assisted Drug Delivery
2.5. Ex Vivo Confocal Microscopy
2.6. Optical Coherence Tomography
2.7. Image Analysis and Statistics
3. Results
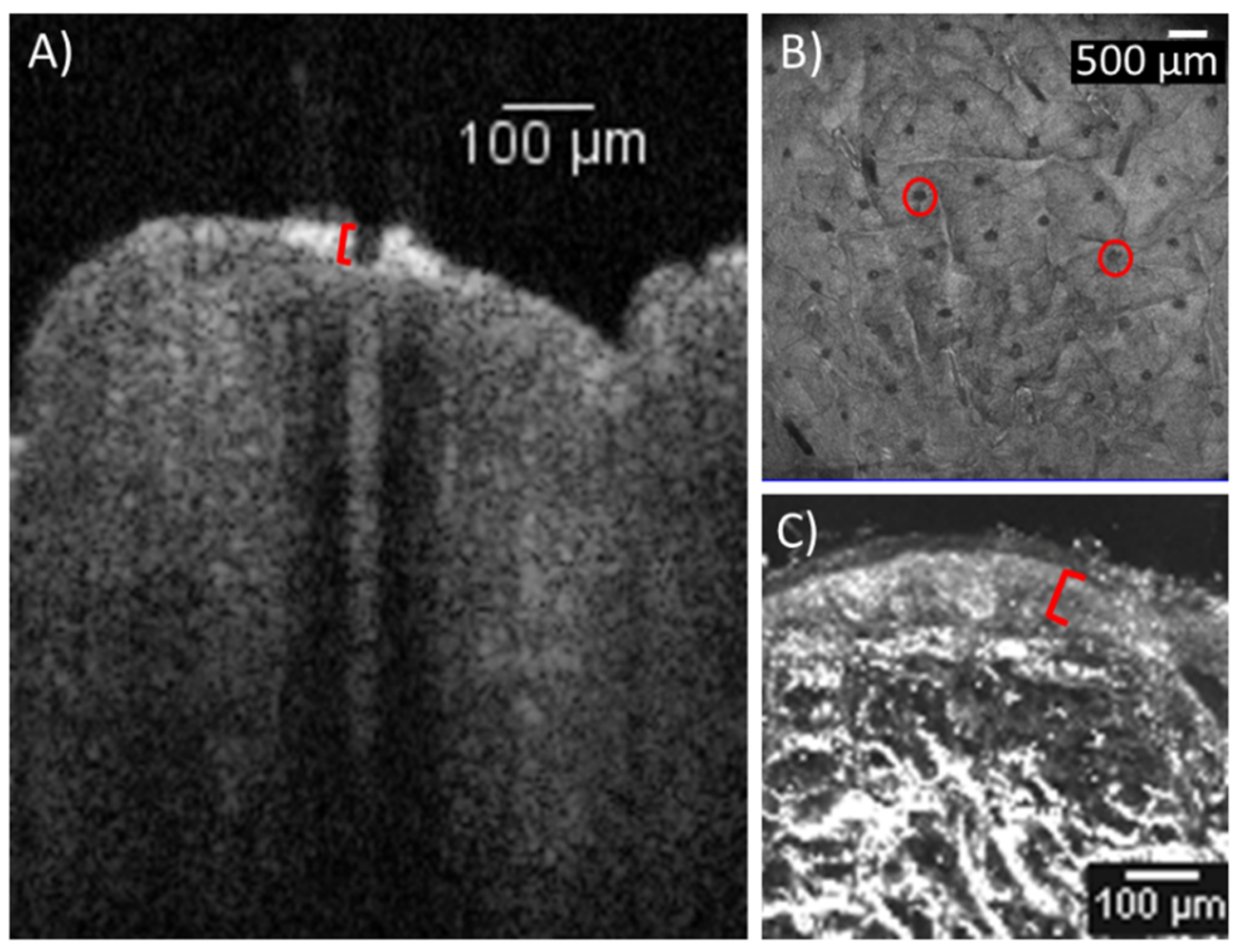
3.1. Laser-Tissue Interaction
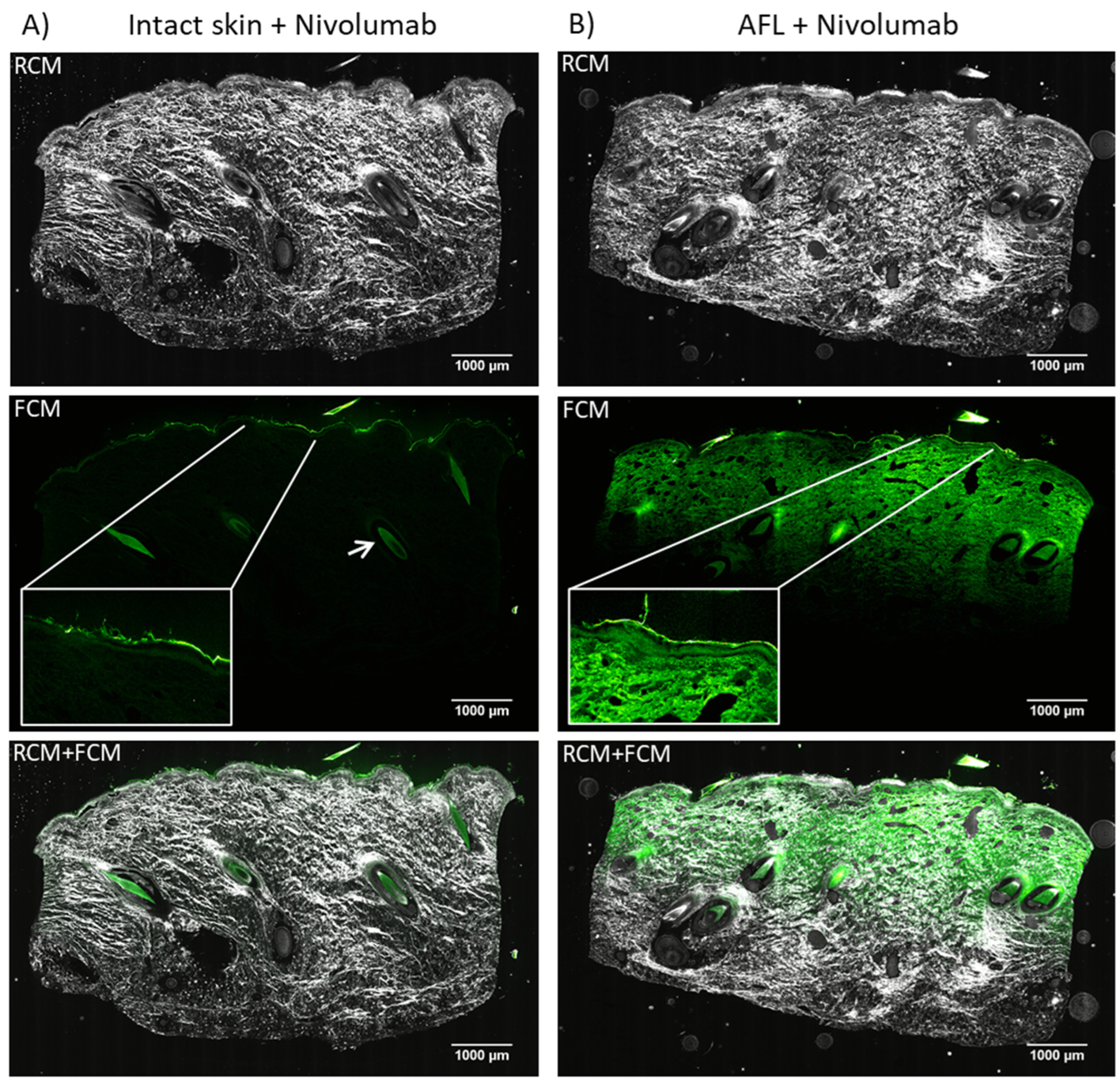
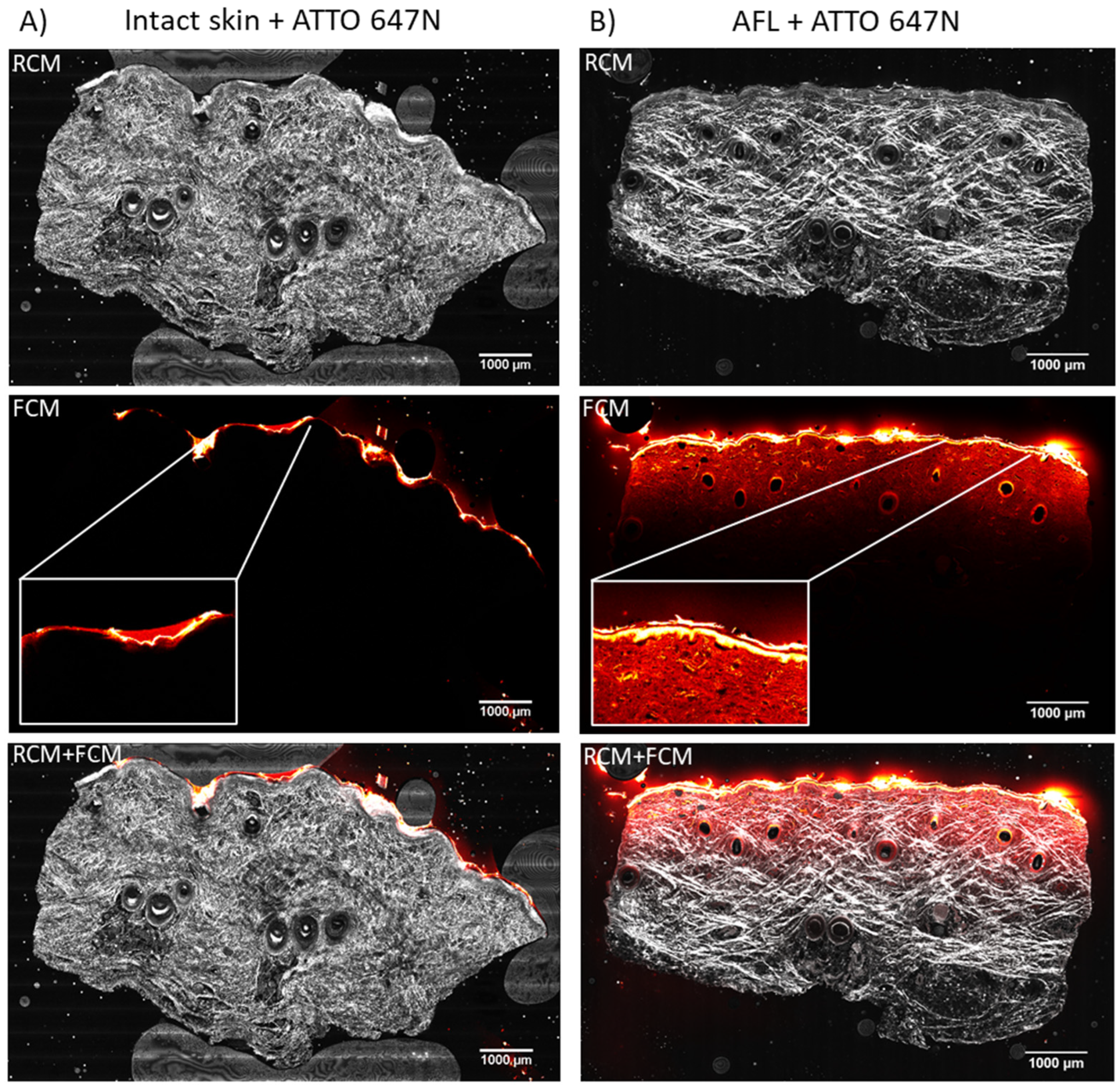
3.2. Cutaneous Biodistribution
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wenande, E.; Anderson, R.R.; Haedersdal, M. Fundamentals of fractional laser-assisted drug delivery: An in-depth guide to experimental methodology and data interpretation. Adv. Drug Deliv. Rev. 2020, 153, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Haedersdal, M.; Erlendsson, A.M.; Paasch, U.; Anderson, R.R. Translational medicine in the field of ablative fractional laser (AFXL)-assisted drug delivery: A critical review from basics to current clinical status. J. Am. Acad. Dermatol. 2016, 74, 981–1004. [Google Scholar] [CrossRef] [PubMed]
- Haak, C.S.; Bhayana, B.; Farinelli, W.A.; Anderson, R.R.; Haedersdal, M. The impact of treatment density and molecular weight for fractional laser-assisted drug delivery. J. Control. Release Off. J. Control. Release Soc. 2012, 163, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Bos, J.D.; Meinardi, M.M.H.M. The 500 Dalton rule for the skin penetration of chemical compounds and drugs. Exp. Dermatol. 2000, 9, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Hendel, K.K.; Bagger, C.; Olesen, U.H.; Janfelt, C.; Hansen, S.H.; Haedersdal, M.; Lerche, C.M. Fractional laser-assisted topical delivery of bleomycin quantified by LC-MS and visualized by MALDI mass spectrometry imaging. Drug Deliv. 2019, 26, 244–251. [Google Scholar] [CrossRef] [Green Version]
- Lapteva, M.; Del Río-Sancho, S.; Wu, E.; Carbonell, W.S.; Böhler, C.; Kalia, Y.N. Fractional laser ablation for the targeted cutaneous delivery of an anti-CD29 monoclonal antibody-OS2966. Sci. Rep. 2019, 9, 1030. [Google Scholar] [CrossRef] [Green Version]
- Wenande, E.; Olesen, U.H.; Nielsen, M.M.B.; Janfelt, C.; Hansen, S.H.; Anderson, R.R.; Haedersdal, M. Fractional laser-assisted topical delivery leads to enhanced, accelerated and deeper cutaneous 5-fluorouracil uptake. Expert Opin. Drug Deliv. 2017, 14, 307–317. [Google Scholar] [CrossRef]
- Olesen, U.H.; Clergeaud, G.; Hendel, K.K.; Yeung, K.; Lerche, C.M.; Andresen, T.L.; Haedersdal, M. Enhanced and Sustained Cutaneous Delivery of Vismodegib by Ablative Fractional Laser and Microemulsion Formulation. J. Investig. Dermatol. 2020, 140, 2051–2059. [Google Scholar] [CrossRef]
- Taudorf, E.H.; Lerche, C.M.; Erlendsson, A.M.; Philipsen, P.A.; Hansen, S.H.; Janfelt, C.; Paasch, U.; Anderson, R.R.; Haedersdal, M. Fractional laser-assisted drug delivery: Laser channel depth influences biodistribution and skin deposition of methotrexate. Lasers Surg. Med. 2016, 48, 519–529. [Google Scholar] [CrossRef]
- Cao, Y.; Kakar, P.; Hossen, M.N.; Wu, M.X.; Chen, X. Sustained epidermal powder drug delivery via skin microchannels. J. Control. Release Off. J. Control. Release Soc. 2017, 249, 94–102. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Kalaria, D.R.; Kalia, Y.N. Erbium:YAG fractional laser ablation for the percutaneous delivery of intact functional therapeutic antibodies. J. Control. Release 2011, 156, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Jiang, H.; Zhang, Y.; Ren, G.; Dong, L.; Zhu, J.; Tu, Y.; Tao, J.; Yang, L. Transdermal delivery of water-soluble fluorescent antibody mediated by fractional Er:YAG laser for the diagnosis of lupus erythematosus in mice. Lasers Surg. Med. 2019, 51, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Christensen, R.L.; Omland, S.H.; Persson, D.P.; Husted, S.; Haedersdal, M.; Olesen, U.H. Topical Delivery of Nivolumab, a Therapeutic Antibody, by Fractional Laser and Pneumatic Injection. Lasers Surg. Med. 2020, 53, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Christensen, R.L.; Hendel, K.K.; Persson, D.P.; Husted, S.; Olesen, U.H.; Haedersdal, M. Topical delivery of PD-1 inhibitors with laser-assisted passive diffusion and active intradermal injection: Investigation of cutaneous pharmacokinetics and biodistribution patterns. Lasers Surg. Med. 2021, 54, 170–181. [Google Scholar] [CrossRef]
- Wenande, E.; Olesen, U.H.; Boesen, M.R.; Persson, D.P.; Lerche, C.M.; Stürup, S.; Gammelgaard, B.; Husted, S.; Anderson, R.R.; Haedersdal, M. Laser-assisted delivery enhances topical uptake of the anticancer agent cisplatin. Drug Deliv. 2018, 25, 1877–1885. [Google Scholar] [CrossRef] [Green Version]
- Bağcı, I.S.; Aoki, R.; Vladimirova, G.; Sárdy, M.; Ruzicka, T.; French, L.E.; Hartmann, D. Simultaneous immunofluorescence and histology in pemphigus vulgaris using ex vivo confocal laser scanning microscopy. J. Biophotonics 2021, 14, e202000509. [Google Scholar] [CrossRef]
- Sattler, E.C.; Kästle, R.; Welzel, J. Optical coherence tomography in dermatology. J. Biomed. Opt. 2013, 18, 061224. [Google Scholar] [CrossRef]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji-an Open Source platform for biological image analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Banzhaf, C.A.; Ortner, V.K.; Philipsen, P.A.; Haedersdal, M. The ablative fractional coagulation zone influences skin fluorescence intensities of topically applied test molecules-An in vitro study with fluorescence microscopy and fluorescence confocal microscopy. Lasers Surg. Med. 2019, 51, 68–78. [Google Scholar] [CrossRef] [Green Version]
- Haak, C.S.; Hannibal, J.; Paasch, U.; Anderson, R.R.; Haedersdal, M. Laser-induced thermal coagulation enhances skin uptake of topically applied compounds. Lasers Surg. Med. 2017, 49, 582–591. [Google Scholar] [CrossRef]
- Paasch, U.; Haedersdal, M. Laser systems for ablative fractional resurfacing. Expert Rev. Med. Devices 2011, 8, 67–83. [Google Scholar] [CrossRef] [PubMed]
- Meesters, A.A.; Nieboer, M.J.; Almasian, M.; Georgiou, G.; de Rie, M.A.; Verdaasdonk, R.M.; Wolkerstorfer, A. Drug penetration enhancement techniques in ablative fractional laser assisted cutaneous delivery of indocyanine green. Lasers Surg. Med. 2019, 51, 709–719. [Google Scholar] [CrossRef]
- Chen, X.; Shah, D.; Kositratna, G.; Manstein, D.; Anderson, R.R.; Wu, M.X. Facilitation of transcutaneous drug delivery and vaccine immunization by a safe laser technology. J. Control. Release 2012, 159, 43–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieboer, M.J.; Meesters, A.A.; Almasian, M.; Georgiou, G.; de Rie, M.A.; Verdaasdonk, R.M.; Wolkerstorfer, A. Enhanced topical cutaneous delivery of indocyanine green after various pretreatment regimens: Comparison of fractional CO2 laser, fractional Er:YAG laser, microneedling, and radiofrequency. Lasers Med. Sci. 2020, 35, 1357–1365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenberg, L.K.; Bagger, C.; Janfelt, C.; Haedersdal, M.; Olesen, U.H.; Lerche, C.M. A Comparison of Human and Porcine Skin in Laser-Assisted Drug Delivery of Chemotherapeutics. Lasers Surg. Med. 2021, 53, 162–170. [Google Scholar] [CrossRef]
- Kositratna, G.; Hibert, M.L.; Jaspan, M.; Welford, D.; Manstein, D. Effects of deviation from focal plane on lesion geometry for ablative fractional photothermolysis. Lasers Surg. Med. 2016, 48, 555–561. [Google Scholar] [CrossRef]
- Olesen, U.H.; Clergeaud, G.; Lerche, C.M.; Andresen, T.L.; Haedersdal, M. Topical delivery of vismodegib using ablative fractional laser and micro-emulsion formulation in vitro: Topical vismodegib and laser in vitro. Lasers Surg. Med. 2019, 51, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Haak, C.S.; Christiansen, K.; Erlendsson, A.M.; Taudorf, E.H.; Thaysen-Petersen, D.; Wulf, H.C.; Haedersdal, M. Ablative fractional laser enhances MAL-induced PpIX accumulation: Impact of laser channel density, incubation time and drug concentration. J. Photochem. Photobiol. B 2016, 159, 42–48. [Google Scholar] [CrossRef]
- Zorec, B.; Škrabelj, D.; Marinček, M.; Miklavčič, D.; Pavšelj, N. The effect of pulse duration, power and energy of fractional Er:YAG laser for transdermal delivery of differently sized FITC dextrans. Int. J. Pharm. 2017, 516, 204–213. [Google Scholar] [CrossRef]
- Ryzhkov, A.; Raikher, Y. Size-Dependent Properties of Magnetosensitive Polymersomes: Computer Modelling. Sensors 2019, 19, 5266. [Google Scholar] [CrossRef] [Green Version]
- Kurlyandskaya, G.V.; Blyakhman, F.A.; Makarova, E.B.; Buznikov, N.A.; Safronov, A.P.; Fadeyev, F.A.; Shcherbinin, S.V.; Chlenova, A.A. Functional magnetic ferrogels: From biosensors to regenerative medicine. AIP Adv. 2020, 10, 125128. [Google Scholar] [CrossRef]
- Kennedy, S.; Roco, C.; Déléris, A.; Spoerri, P.; Cezar, C.; Weaver, J.; Vandenburgh, H.; Mooney, D. Improved magnetic regulation of delivery profiles from ferrogels. Biomaterials 2018, 161, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Gambin, B.; Kruglenko, E.; Tymkiewicz, R.; Litniewski, J. Ultrasound assessment of the conversion of sound energy into heat in tissue phantoms enriched with magnetic micro- and nanoparticles. Med. Phys. 2019, 46, 4361–4370. [Google Scholar] [CrossRef]
- Patra, J.K.; Das, G.; Fraceto, L.F.; Campos, E.V.R.; Rodriguez-Torres, M.d.P.; Acosta-Torres, L.S.; Diaz-Torres, L.A.; Grillo, R.; Swamy, M.K.; Sharma, S.; et al. Nano based drug delivery systems: Recent developments and future prospects. J. Nanobiotechnology 2018, 16, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Intervention | n | Median MFI (IQR, AU) | p-Value |
|---|---|---|---|
| Intact skin + nivolumab | 3 | 1731 (1715/1765) | 0.100 |
| AFL + nivolumab | 3 | 2783 (2544/2838) | |
| Intact skin + ATTO 647N | 4 | 1911 (1811/2048) | 0.029 |
| AFL + ATTO 647N | 4 | 2727 (2436/3076) | |
| Total median | 14 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Christensen, R.L.; Ortner, V.K.; Haedersdal, M.; Olesen, U.H. Optical Imaging Visualizes a Homogeneous and Horizontal Band-Like Biodistribution of Large- and Small-Size Hydrophilic Compounds Delivered by Ablative Fractional Laser. Pharmaceutics 2022, 14, 1537. https://doi.org/10.3390/pharmaceutics14081537
Christensen RL, Ortner VK, Haedersdal M, Olesen UH. Optical Imaging Visualizes a Homogeneous and Horizontal Band-Like Biodistribution of Large- and Small-Size Hydrophilic Compounds Delivered by Ablative Fractional Laser. Pharmaceutics. 2022; 14(8):1537. https://doi.org/10.3390/pharmaceutics14081537
Chicago/Turabian StyleChristensen, Rikke Louise, Vinzent Kevin Ortner, Merete Haedersdal, and Uffe Høgh Olesen. 2022. "Optical Imaging Visualizes a Homogeneous and Horizontal Band-Like Biodistribution of Large- and Small-Size Hydrophilic Compounds Delivered by Ablative Fractional Laser" Pharmaceutics 14, no. 8: 1537. https://doi.org/10.3390/pharmaceutics14081537